
Abstract
Background
Only limited data are available regarding the treatment status and response to cluster headache in an Asian population. Therefore, this study aimed to provide a real-world treatment pattern of cluster headache and the response rate of each treatment in an Asian population.
Methods
Patients with cluster headache were recruited between September 2016 and January 2019 from 16 hospitals in Korea. At the baseline visit, we surveyed the patients about their previous experience of cluster headache treatment, and acute and/or preventive treatments were prescribed at the physician’s discretion. Treatment response was prospectively evaluated using a structured case-report form at 2 ± 2 weeks after baseline visit and reassessed after three months.
Results
Among 295 recruited patients, 262 experiencing active bouts were included. Only one-third of patients reported a previous experience of evidence-based treatment. At the baseline visit, oral triptans (73.4%), verapamil (68.3%), and systemic steroids (55.6%) were the three most common treatments prescribed by the investigators. Most treatments were given as combination. For acute treatment, oral triptans and oxygen were effective in 90.1% and 86.8% of the patients, respectively; for preventive treatment, evidence-based treatments, i.e. monotherapy or different combinations of verapamil, lithium, systemic steroids, and suboccipital steroid injection, helped 75.0% to 91.8% of patients.
Conclusion
Our data provide the first prospective analysis of treatment responses in an Asian population with cluster headache. The patients responded well to treatment despite the limited availability of treatment options, and this might be attributed at least in part by combination of medications. Most patients were previously undertreated, suggesting a need to raise awareness of cluster headache among primary physicians.
Introduction
Cluster headache (CH) is a primary headache disorder that manifests as extremely severe headache, autonomic symptoms, and/or agitation. As CH is a devastating disorder, its treatment is an important issue for both physicians and patients. There are two evidence-based guidelines for the treatment of CH mostly from Europe and United States (1,2). However, a standard treatment for CH has not been established, and different treatment strategies are used in real-world settings in different countries.
Although the disease burden of CH is significant in Asia (3–6), CH in Asians may have a different disease profile than those reported in European and American countries. Comparing the literature on CH characteristics published in Asian, European, and North American countries, Asians seem to have a relatively mild disease load in terms of attack frequency, bout duration, and bout frequency (7). Moreover, many guideline-recommended treatments and novel neuromodulation techniques are unavailable, not reimbursed by the national insurance program, or are off-label in Asian countries. These factors, i.e. milder clinical characteristics and the issue of limited resources, might have affected the prescription pattern of Asian physicians treating CH. However, there is limited knowledge regarding the current treatment pattern and treatment response of CH in Asian regions (7). With particular regards to preventive treatment, a limited number of studies are available (8).
In this study, we prospectively collected data on patient experience, prescription pattern, and treatment response to acute and preventive CH treatments with a pre-designed, structured follow-up program in a multicenter setting. This study aimed to provide a real-world treatment pattern of CH and the response rate of each treatment in an Asian population.
Methods
Study design
This study was part of the Korean Cluster Headache Registry (KCHR) Study, which is a prospective, longitudinal, multicenter, observational study that enrolled consecutive patients with CH from 16 hospitals (14 university hospitals, including eight tertiary and five secondary referral hospitals, and two general hospitals) in Korea. CH symptoms, manifestations, and comorbidities were also assessed. Patients with CH who visited the participating hospitals of the KCHR were recruited between September 2016 and January 2019. CH was diagnosed by KCHR investigators (experienced neurologists experienced in headache disorders) based on the most updated criteria from the International Classification of Headache Disorder at the time of enrollment (i.e., 3rd edition beta version, or 3rd edition). The study protocol was approved by the institutional review board of each participating hospital, and written informed consent was obtained from all patients prior to recruitment. The details of the KCHR study are published in our previous studies (4,5).
Baseline evaluation
At the baseline visit, the patients were asked about their treatment experience before visiting the study site. As this was based on retrospective recall, the questions were simply about the experience of each treatment (oxygen, over-the-counter painkiller, prescribed painkiller, migraine-specific drugs such as triptans or ergots, lidocaine spray, oral steroid, suboccipital injection, oral preventive medications) and the subjective response determined by the patients themselves. Patients were also requested to identify the best acute and preventive treatment they had previously tried.
At the baseline visit, investigators prescribed acute and/or preventive treatments to the patients according to their clinical decisions. The treatments were not specifically controlled in this study. During the study period, acute treatments available in Korea included oxygen (although it cannot be reimbursed), nonsteroidal anti-inflammatory drugs (NSAIDs), combination analgesics, triptans, intranasal lidocaine, and available preventive treatments, including oral steroids, occipital nerve block (mostly using steroids), verapamil, and lithium. Other drugs were also prescribed if clinically deemed necessary and were recorded prospectively.
Treatment response
Patients were prospectively followed-up, and the treatment responses were recorded by the investigators. According to the study design, patients were to be followed up at 2 ± 2 weeks (visit 2) and again at three months after baseline. However, we allowed flexibility, and the visit 2 follow-up time was decided based on the estimation of the remaining bout duration in each patient. Remission was determined at visit 2, and the date of remission was recorded. Patients underwent another follow-up at three months after initial visit to ensure the exact remission date. Compliance with preventive medications was categorized as 100%, 50–99%, 1–49%, and 0%, and the date of the last intake was recorded. For oral preventive medications, treatment response was assessed only in patients with ≥50% compliance to minimize the possibility of natural remission, because patients who judge that their current bout is going to end soon have a tendency of not taking the prescribed preventive medications. In terms of occipital nerve blockade, compliance was not considered when determining treatment response. Oral medications were further stratified into monotherapy and combination therapies for subgroup analyses of treatment response.
Treatment response was assessed based on the attack frequency during preventive treatment and the maximal headache intensity when acute treatment was administered. The response to acute treatment was defined as a 50% or more reduction in the maximal headache intensity within shorter time than the anticipated attack duration. Preventive treatments were assessed by each investigator as a 50% or more reduction in attack frequency, which was not considered a result of the patients’ natural course.
Statistical analysis
A descriptive analysis was performed in this study. Categorical data were presented as numbers (percentages), and continuous variables were summarized as mean (SD) or median (interquartile range) according to the data distribution. Group comparisons were made using the chi-square or Fisher’s exact tests. Data from patients who did not complete the visit 2 evaluation were considered missing. Individual missing data was excluded pairwise. As this was a descriptive study, we did not adjust for multiple comparisons. Statistical analyses were performed using the Stata 15.0 software (StataCorp LLC, College Station, TX, USA). Statistical significance was set at a two-tailed p-value <0.05.
Results
Patients
During the study period, 295 patients with CH were recruited. Among these, 262 within the active bouts were included in this study. The patient demographics and CH characteristics are presented in Table 1. The mean age of patients was 37.8 ± 10.74 years, and 221 (84.4%) were males. Only 13 (5.3%) patients had chronic cluster headache.
Patient demographics and characteristics of the current bout.

Data are presented as the mean ± SD, median (interquartile range), or number (percentage).
CH, cluster headache; NRS, numeric rating scale.
*Applicable to patients who had experienced a sufficient number of attacks or bouts to provide adequate information regarding circadian or seasonal propensity for attacks.
Previous treatment experience and recalled response.

Previous treatment experience reported by patients
A total of 171 patients completed the survey regarding their experience with CH treatment before enrollment in the study. Patients who received a certain treatment answered a corresponding survey regarding its response. As this survey was based on subjective recall, there were missing data when patients could not correctly recall the responses to previous treatments.
With regard to acute treatment (Table 2), over-the-counter painkillers (33.3%) were the most frequently experienced, followed by prescribed painkillers (77.2%), and migraine-specific drugs (65.5%). Lidocaine spray was used in nine (5.3%) patients. The response rate to oxygen was the highest (78.9%), followed by those to migraine-specific drugs (60.2%), prescribed painkillers (51.2%), lidocaine spray (22.2%), and over-the-counter painkillers (21.2%).
Overall, preventive treatments were infrequently applied (Table 2). Less than one-third of the patients reported a prior experience with steroids, occipital nerve injection, and oral preventive medications (29.5%, 12.9%, and 31.6%, respectively). Among these treatments, systemic steroids were reportedly effective in 35 (76.1%) of 46 previous users. Responses to oral preventive medications and occipital nerve injection were reported in 49 (65.3%) out of 54 and 10 (45.5%) out of 22 previous users, respectively.
Prospective evaluation of treatment response
Among the 262 patients, 27 (10.3%) were lost to follow-up at visit 2. Of the 235 patients who underwent evaluations at visit 2 (191 by clinic visit and 42 by phone), 234 (99.6%) completed the interview regarding the treatment response after a median of 20 days (IQR 14–34) after baseline evaluation. Treatment response and outcomes were confirmed at the three-month follow-up in all 234 patients.
Acute treatment
Prescriptions for acute treatment are shown in Figure 1. Triptans (73.1%) were the most frequently prescribed, followed by NSAIDs (42.1%) and oxygen (16.8%). The prescription of combination analgesics and intranasal lidocaine was uncommon (5.6% and 1.7%, respectively).

Prescription rate of acute CH treatment.
Patients who actually received or underwent acute treatment were assessed in terms of treatment response (Table 3). The overall response rates were as follows: oxygen (87.2%), NSAIDs (82.6%), combination analgesics (75.0%), triptans (90.3%), and lidocaine spray (100.0%).
Response rates of acute treatment.

*Only patients who actually received or underwent acute treatment were included.
Data are presented as median (interquartile range) or number (percentage).
NSAIDs, nonsteroidal anti-inflammatory drugs.
Preventive treatment
Prescriptions for preventive treatment are shown in Figure 2. Verapamil (67.5%, median dose 180mg/d [IQR 180–240 mg/d]) and oral steroids (54.7%, mostly prednisolone 60 mg/d [IQR 50–60 mg/d] with tapering courses) were the most frequently prescribed, followed by lithium (19.2%, median dose 300 mg [IQR 300–300 mg/d]) and suboccipital steroids (16.2%, betamethasone [n = 9], dexamethasone [n = 9], methylprednisolone [n = 8], and triamcinolone [n = 6], with a median dexamethasone equivalent dose of 15 mg [IQR 11.3–20 mg]).

Prescription rate of preventive CH treatment.
Table 4 shows the response rate for each preventive treatment. Only patients with >50% compliance with preventive treatment were assessed. The patients showed an excellent response to systemic steroids (93.5%), verapamil (90.8%), suboccipital steroids (84.4%), and lithium (81.6%).
Response rates from preventive treatment.
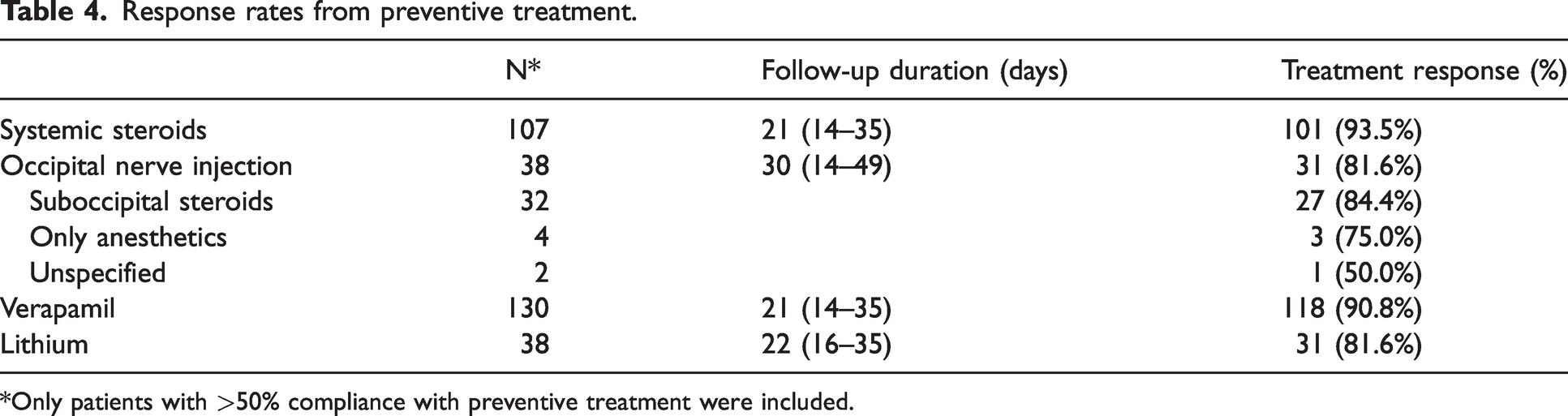
*Only patients with >50% compliance with preventive treatment were included.
Subgroup analysis
When oral medications were stratified into monotherapy and combination therapy, no differences were noted in terms of the efficacy of acute and preventive medications. Table 5 summarizes the responses to monotherapy and combination therapy for each acute medication class.
Comparison of response rates between monotherapy vs. combination therapy.
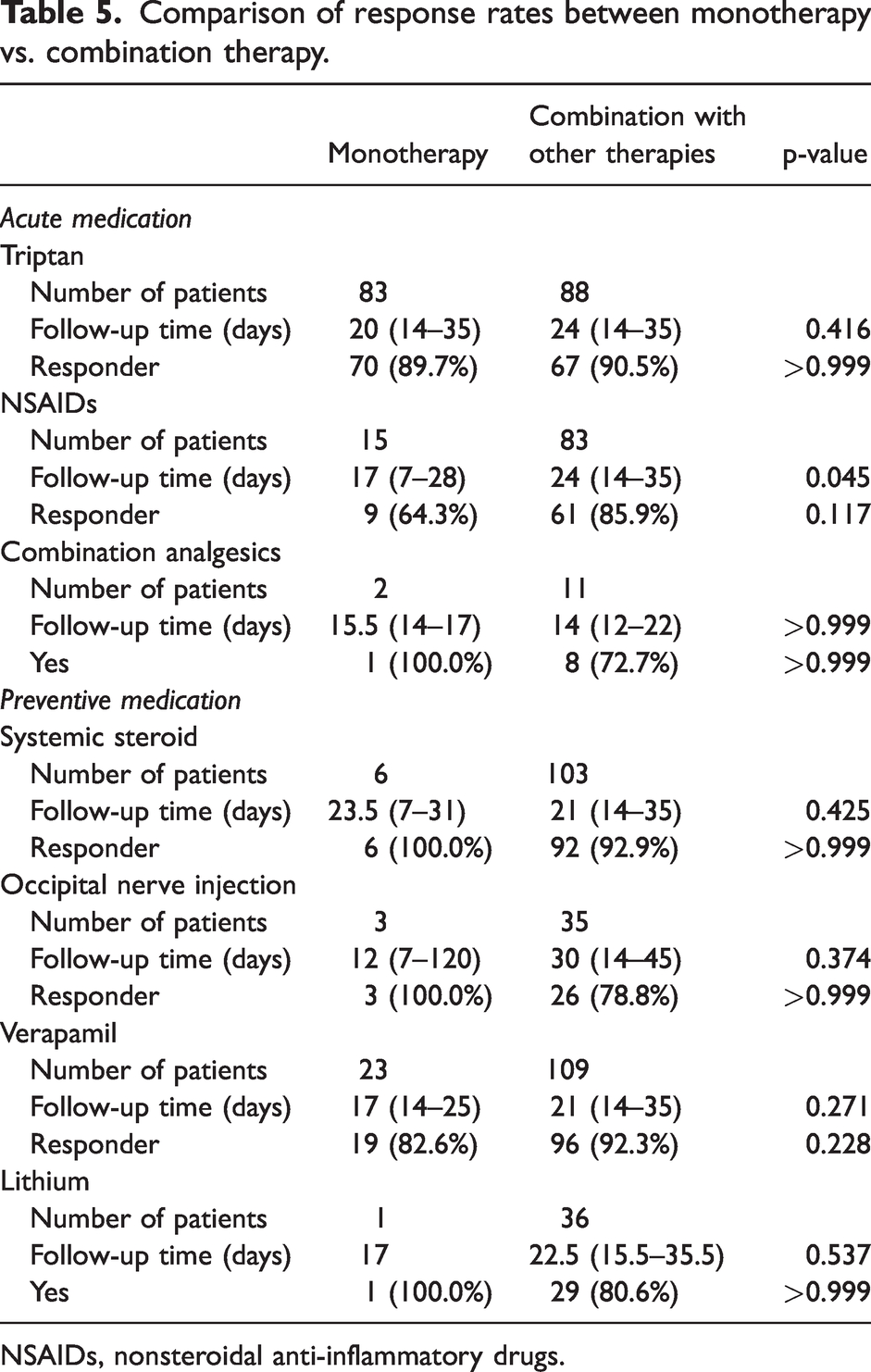
NSAIDs, nonsteroidal anti-inflammatory drugs.
There was an imbalance in the number of patients in each group (monotherapy vs. combination therapy; Table 5). Triptans were administered either as monotherapy or in combination with other therapies, but these two strategies did not yield a statistically significant difference (response rates 89.7% vs. 90.5%, p > 0.999; Table 5). NSAIDs or combination analgesics were mostly administered in combination with other therapies, and the response rate of NSAIDs differed numerically between monotherapy (64.3%) and combination therapy (85.8%), but the difference was not statistically significant (p = 0.117) and the follow-up time significantly differed (p = 0.045), thus those two strategies were incomparable (Table 5).
Preventive medications were mostly administered in combination with other therapies. Thus, the number of patients receiving monotherapy was small for all preventive medications. No preventive treatment modality showed a significant difference in response rates between monotherapy and combination therapy: systemic steroids (100.0% vs. 92.9%, p > 0.999); occipital nerve injections (100.0% vs. 78.8%, p > 0.999); verapamil (82.6% vs. 92.3%, p = 0.228); and lithium (100.0% vs. 80.6%, p > 0.999) (Table 5).
When the medications were stratified into preventative (verapamil and lithium) and transitional (systemic or local steroids) treatments, 171 (73.1%) and 148 (63.2%) patients received preventive and transitional treatment, respectively, and the combination of both was used in 132 (56.4%). Thirty-nine (16.7%) patients received only preventive medications (verapamil in 30; lithium in one; and the combination of verapamil and lithium in eight), and 16 (6.8%) had only transitional treatments (systemic steroids in 10; suboccipital steroids in three; and both systemic and suboccipital steroids in three). The combination regimens and numbers of patients receiving each regimen are listed in Table 6.
Combinations used in this study.

Discussion
Our study provides real-world treatment patterns and outcomes for Korean patients with CH. The major findings of this study are as follows: 1) only a small proportion of patients had received evidence-based treatments before they visited the KCHR investigators, 2) evidence-based treatments yielded high response rates even though the treatment options were limited, and 3) combination therapy was the common for both acute and preventive treatments of CH in Korea.
Despite increasing awareness of CH with innumerous efforts from physicians and patients in some regions around the globe, CH is still underdiagnosed and undertreated (9–11). A significant delay in CH diagnosis has been confirmed in several studies (10–16). Such diagnostic delays inevitably lead to mistreatment and under-treatment. Mistreatment such as tooth extraction or sinus surgery prior to CH diagnosis has been reported in studies in Europe (10,13,15,16). However, the use of guideline-adherent treatment and its efficacy have rarely been studied (16), and to our knowledge, no such study has been published in Asia. Our study revealed poor treatment experience prior to patients presenting to headache specialists among Korean patients with CH. Most patients used over-the-counter painkillers for acute abortive treatment, and the proportion of patients who received preventive treatments was low. Along with diagnostic delay, guideline-adherent treatment should also be promoted among physicians.
When the best acute treatments available in Korea were administered, patients exhibited a high response rate. Due to the limited availability of acute treatment options, such as injectable triptans, oral triptans (mostly zolmitriptan but sometimes other triptans in cases where zolmitriptan was unavailable) were most commonly prescribed by the KCHR investigators and showed a response rate of approximately 90% (89.7% as monotherapy and 90.5% in combination with other medications). Oxygen also yielded a high response rate of nearly 90%, although it was only used in less than one-fifth of patients, as the oxygen prescription for CH is not reimbursed in Korea. NSAIDs and combination analgesics are commonly used as substrates in combination therapy. NSAIDs monotherapy yielded a less prominent response (64.3%) than when used in combination with other agents (mostly oral triptans) (85.9%), although the difference was not statistically significant, probably because of the small sample size. The prescription of lidocaine spray was uncommon, although it yielded a 100% response rate.
Verapamil and systemic steroids are the most commonly used preventive treatment. The overall response rates were high (>80%) with evidence-based treatments, particularly with systemic steroids and verapamil. Along with the low prevalence of chronic CH in our cohort (about 5%), the high response rate of CH preventive treatments in our multicenter KCHR cohorts may explain why chronic CH is rare in Asians while it affects a major subgroup in Europe and the United States (7). A German study showed that guideline-adherent prophylactic treatment was successful in 92.8% of patients with episodic CH, whereas patients with chronic CH only showed a 70.9% response rate (17). Cumulatively, our results strongly encourage the use of evidence-based treatments for the prevention of CH in Asian patients. The response rates were higher in our study than in a recent real-life study from Denmark (18). This difference can be attributed to: 1) most of patients had episodic CH in our study while a substantial proportion of Danish patients had chronic CH; 2) transitional treatment and combination therapies are commonly used in our study and; 3) bout duration of episodic cluster headache is much less in our patients than in European cohorts (18). Whether this could be a genetic influence should be determined in further studies using pharmacogenomic methodologies.
In our study, most preventive treatments were a combination of systemic steroids or occipital nerve injections as a bridge therapy with oral preventives. This approach yielded a high response rate of 80–100%. In a smaller proportion of patients who received monotherapy, treatment response was also high, with no statistically significant difference in response rates between monotherapy and combination therapy. However, this may be attributable to the small sample size, and the use of combination therapy might have been selected based on previous inefficacy of monotherapy in these patients. Therefore, our study could not conclude that combination therapy monotherapy and combination therapy have similar efficacy. Rather, a combination treatment strategy would have led to a high response rate despite limited treatment options.
The strengths of our study are as follows. First, to our knowledge, our study is the first Asian report on patient experience, prescription pattern, and treatment response to CH treatments with a pre-designed, structured follow-up program in a multicenter setting. Second, due to the multicenter setting and uncontrolled study design, we could observe a variety of real-world treatment patterns and their responses. However, our study had some limitations. As the study setting of KCHR was descriptive and rather hypothesis-generating than hypothesis-testing, no sample size estimations were conducted based on a specific hypothesis. In addition, as most of our participants had episodic CH, which is a self-limiting disorder that converts to an inactive “between-bouts” period, treatment responses from preventive treatment can be influenced by the natural remission. Although the investigators attempted to discriminate the treatment response from the natural disease course, the possibility of bias remains unless a placebo arm is implemented. Short initial follow-up duration can be considered a limitation, but we followed up patients after three months to ensure the treatment response. Another limitation was that the treatment was uncontrolled; thus, the treatment response could have been a result of physicians’ comprehensive and careful selection of medications, which might have led to better outcomes than those expected from a single drug trial. A last limitation is a possibility of selection bias as we only analyzed the treatment response in patients who took 50% or more preventive medications. It was to minimize the possibility of natural remission, but some unmeasured issues (e.g. side effects, preference, or previous treatment experience) would have affected the compliance and caused some selection bias.
Clinical implications
From this multicenter study of CH conducted in Korea, Korean patients exhibited high response rates to evidence-based acute and preventive treatments of CH. Previous treatment experience and response rates were poor, suggesting the need for better identification of the disease and implementation of evidence-based treatments for patients with CH. Combination treatment strategy is commonly used for both acute and preventive treatment of CH in Korea.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.