
Abstract
Introduction
The pathophysiology of migraine is based on cyclic changes within the central nervous system, associated with a cascade of events provoking a heightened sensitivity of the trigeminal nervous system and associated symptoms such as phono- and photophobia, nausea and vomiting (1,2). The most frequently associated symptom is neck pain (3,4) and an increasing body of evidence reports on musculoskeletal findings, including trigger points in neck and face muscles, joint hypomobility, posture or range of motion changes of the cervical spine, which are significantly more prevalent in patients with migraine than in control participants (5–9). While some authors explain such findings as the consequence of repeated migraine attacks influencing the musculoskeletal system, others hypothesize that the nociceptive input originating from the cervical muscles and joints would influence the attack frequency and thereby potentially contribute to the transition to chronic migraine (10,11). Indeed, more severe migraine presentations are associated with more musculoskeletal findings but the difference between chronic and episodic migraine is less pronounced than between migraine patients and healthy participants (10,12). Head pain referral during manual palpation of upper cervical structures (13–15) points towards a connection between the occipital, upper cervical and trigeminal nerves, indicating a convergence of afferences at brainstem level within the trigeminocervical complex (16,17). A reciprocal connection can be inferred from preliminary data indicating a reduced headache frequency after physiotherapy focusing on cervical musculoskeletal structures (18,19), but there is currently no evidence from methodologically rigorous randomized controlled trials.
Although migraine is a condition with alternating painful and pain-free intervals, it can also be understood as a chronic pain disease (20,21). The term “chronic” is somewhat misleading because the international headache classification describes chronic migraine based on the frequency of attacks (22) rather than on the duration of the disease or underlying central nervous system changes, as defined by the International Association for the Study of Pain for other chronic pain conditions (23). In contrast to episodic migraine, chronic migraine is associated with a greater sensitization and can exhibit pain features of other primary headaches, such as chronic tension type headache (24,25). However, both migraine forms share features of chronic pain by showing characteristic sensory alterations (26,27), altered endogenous pain modulation (28) and by associated psychophysical features such as impaired sleep and the influence of stress (29,30). Similar to other chronic pain conditions, migraine is also characterized by altered central nervous system processing (31).
Guideline-recommended treatment for chronic pain conditions is mainly exercise-based and includes multimodal cognitive behavioral treatment (32). A dominant feature of such programs is pain neurophysiology education (PNE), which is a structured approach to teach patients the physiological processes underlying ongoing pain (33–35). The mechanism of action of this established cognitive-behavioral intervention for adults with chronic pain is based on changing maladaptive illness beliefs and subsequently altering behavior. PNE takes into account the individual behavioral, psychological, and environmental factors that may contribute to a patient’s pain persistence.
Although education in general has been shown to be an important component of migraine management (36), the effectiveness of PNE has not been evaluated in migraine populations. Only recently, a scoping review highlighted that there is a lack of PNE studies in migraine populations (37).
The aim of this study was therefore to evaluate the additional effect of PNE, adapted to the pathophysiology of migraine, on headache frequency, migraine frequency and headache associated disability, when provided as an add-on to physiotherapy. Our hypothesis is that adding PNE to usual physiotherapy treatment would lead to additional improvements in headache frequency, disability, neck pain and psychosomatic outcomes.
Methods
Study design
This randomized controlled trial featured two intervention arms, physiotherapy plus pain neuroscience education (PT + PNE) or physiotherapy alone (PT). Effects were compared within and between groups. The study was stopped after recruitment goals were met. Ethical consent was granted from the ethics committee of the University of Luebeck (process number 19-362) and all participants provided written consent before enrollment. The reporting follows the recommendations of the CONSORT Statement for the Standardized Reporting of Randomized Clinical Trials (38).
Participants
Participants aged between 18–66 years diagnosed with migraine (migraine on >4 days per month) with or without neck pain were included in the study. Migraine was diagnosed according to the current diagnostic criteria of the International Classification of Headache Disorders (22). Patients with additional psychiatric or neurological diseases or concomitant other headache types (except for episodic tension-type headache) were excluded. Participants were instructed to continue with ongoing prophylactic therapies without any changes, and to not start any further therapy such as physiotherapy during participation in the study. Participants were consecutively recruited by placing information brochures at local neurology and primary care clinics in the region, advertising at local support groups (Migraine League) and physical therapy practices, and on the local University of Applied Health Sciences website, as well as through advertisements in daily newspapers and social media.
Interventions
Physiotherapy and PNE were provided by one physiotherapist (RM) experienced in the treatment of headache patients (>10 years) and with additional training in manual therapy (OMPT). Interventions were conducted at the University of Applied Health Sciences in Bochum, Germany, and at two local physical therapy clinics. Following a thorough physical examination, based on an international consensus procedure (39) and previously evaluated for the use in migraine populations (12), all patients received six sessions (30 minutes each) of tailored physiotherapy consisting of strengthening exercises for the neck and shoulder girdle muscles, mobilization of the cervical and thoracic spine, coordination and posture exercises and soft-tissue mobilization. The choice and combination of interventions was based on the findings from the physical examination. In addition, home exercises were provided to both groups in order to complement the intervention and to support self-efficacy.
In this study we used a simple, unrestricted randomization and the allocation of treatment was randomized without constraints. Each participant could choose one of two sealed, opaque envelopes after the baseline assessment. Thus, with two treatments, the equivalent to a coin toss for each patient, without regard to balance, each participant had an equal chance of receiving each of the treatments. The randomization ratio was 1: 1, based on two study arms.
An allocation order as well as an assignment of the participants was not needed, as the participants chose and opened one of the two closed envelopes themselves. After reviewing the inclusion criteria, providing informed consent and obtaining written consent, enrollment in the study was performed by the treating therapist.
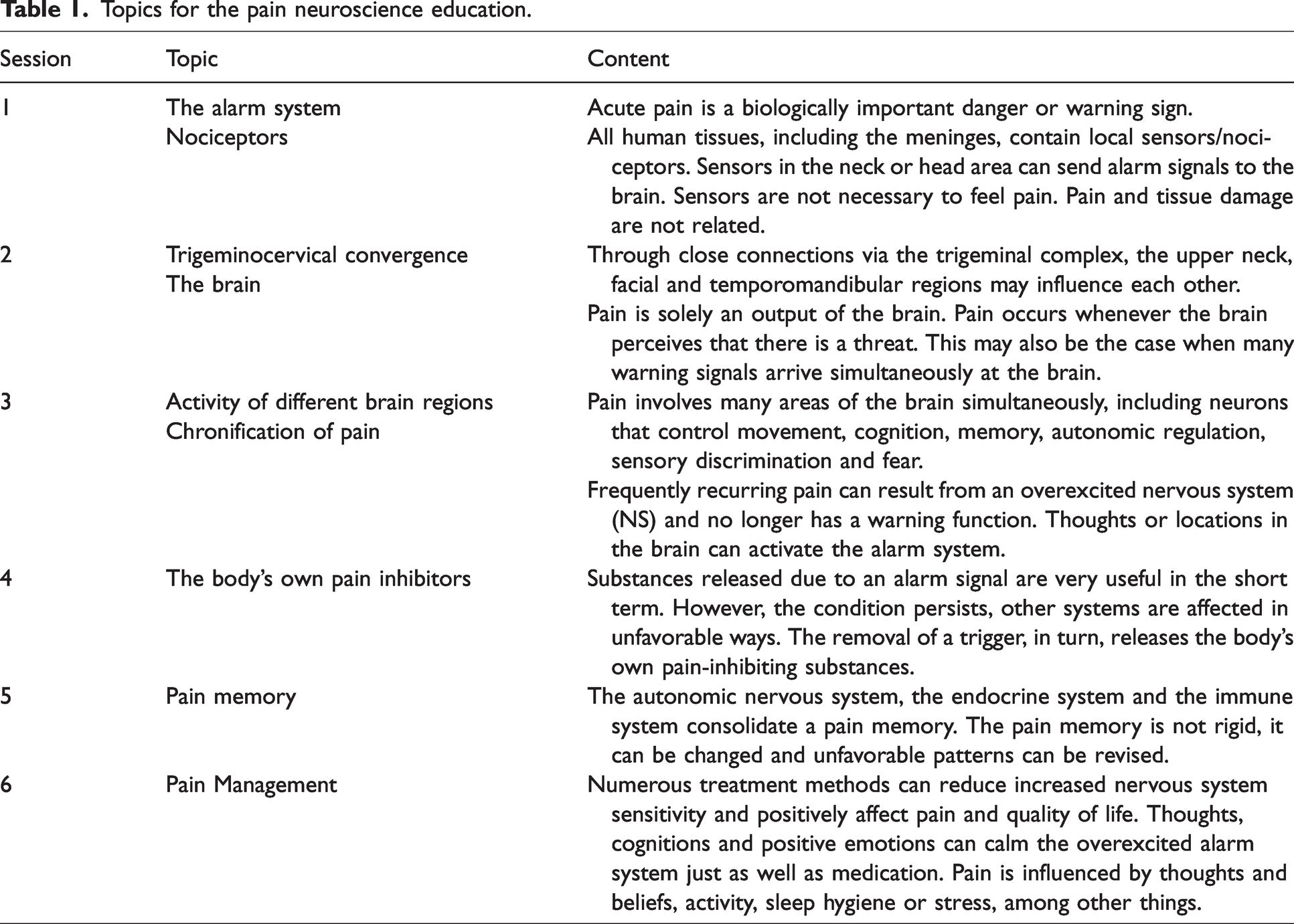
Patients randomized to the PT + PNE group additionally received approximately 15 minutes of theory classes after each physiotherapy session. Contents of the PNE were based on the PNE literature for chronic pain (33,40–43), supplemented and adapted to the specific aspects of migraine. As the study was conducted in Germany, PNE was provided in German. The education included nine topical areas (provided in six sessions) which are summarized in Table 1. Neither the therapist nor patients were blinded towards group allocation.
Topics for the pain neuroscience education.
Outcome measures
Primary outcome measures were headache frequency (days/month), migraine frequency (headache days with exclusively migraine features), both measured by a diary, and migraine associated disability score (MIDAS) (44–46). Headache frequency includes headache days with and without migraine features in the last month.
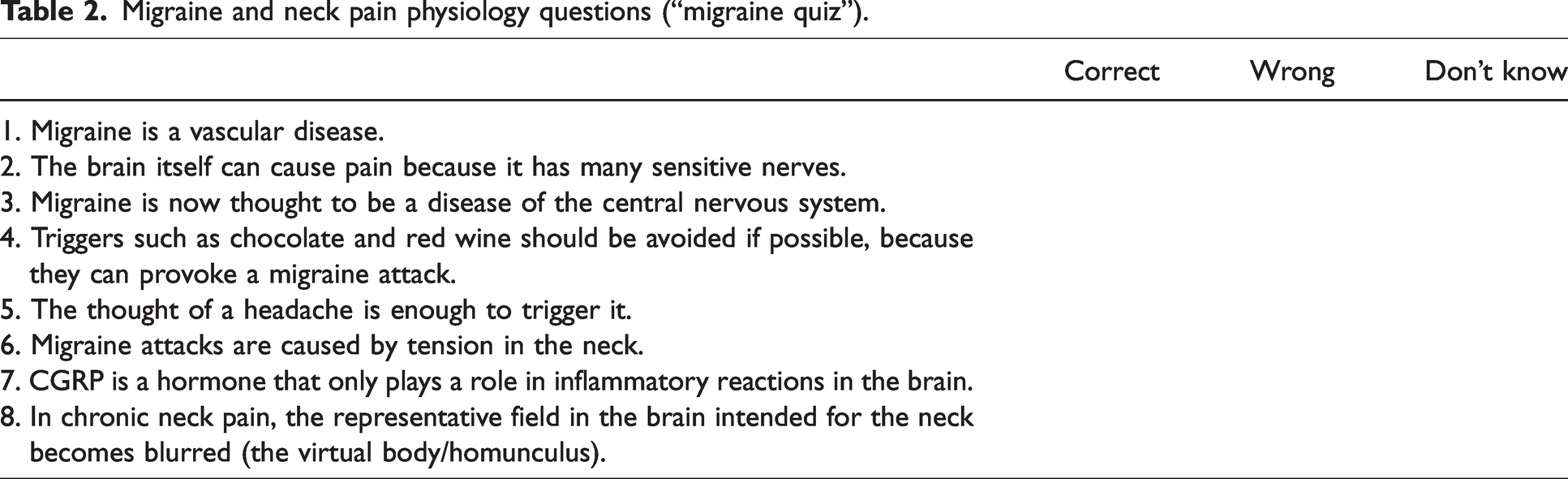
Secondary outcome measures included migraine-specific quality of life (MSQoL) (47), depression symptoms (Patient Health Questionnaire-9 [PHQ-9]) (48), neck pain associated disability (NDI) (49), cutaneous allodynia (ASC-12) (50), as well as the acquired knowledge on the neurophysiology of pain, measured through the Neurophysiology of Pain Questionnaire (NPQ) (51–53). Eight additional questions were formulated in order to assess the acquired specific knowledge about neck and migraine (“migraine quiz”) (Table 2). Patients additionally filled out a questionnaire on demographic data.
Migraine and neck pain physiology questions (“migraine quiz”).
Headache and neck pain frequency (days/month) and medication intake (number/month) were documented in a diary during a prolonged baseline period (T0) three months before the beginning of the intervention in order to provide more reliable pre-post estimations for the effect of physiotherapy. All measurements were taken at baseline (T1), post-treatment (T2) (immediately after the sixth intervention) and at a follow-up three months after treatment (T3). Thus, the primary outcome headache frequency was recorded four times (always referring to the previous month). All secondary outcomes were assessed three times, except for the MIDAS that has a recall time of three months. Therefore, it was analyzed just at T1 and T3 due to the overlap at T2. All variables, including baseline physical examination, were collected before randomization. At the following time points, the participants and the investigator were not blinded to the group.
At T2 and T3, patients were additionally asked to fill out the global rating of change scale (GROC) (54) to assess their subjective perception of improvement regarding three different aspects: headache days, neck pain days and quality of life. The 15-point GROC scale ranged from −7 (very much worse) to +7 (maximally improved).
Statistical methods
An a priori sample size calculation was performed for the primary outcome measure headache days, based on existing clinical studies in migraine (55,56), assuming a difference in the headache frequency between groups with an effect size of d = 0.25, a power of 80% and an alpha level of 0.05. The total required sample size was 74 patients. After accounting for 10% expected dropouts, 82 patients were recruited.
The descriptive statistics consisted of patients’ characteristics at baseline, which were presented as means and SD or frequencies and percentages for each group. Differences between groups at baseline were compared by independent samples t‐test and x2 or Fisher exact test, according to the nature of the variable.
To assess if PNE has a positive influence on migraine, a two-tailed repeated measures analysis of variance (ANOVA) was used to assess between- and within-subjects factors (within: three time points, between: two intervention groups) and interactions. The achieved effect size was calculated using the F-value of the analyses of variance (57). In cases of sphericity violation (Mauchly’s test p < 0.05), values were corrected by using the Greenhouse-Geisser estimates. For the variables that exhibited baseline significant differences between the two intervention groups, baseline values were used as covariates in the model. Post-hoc pairwise comparisons were Bonferroni-corrected for multiple testing. Results were described using mean, mean difference and 95% Confidence Intervals (95%CI).
The Mann-Whitney test was used to compare groups regarding the perceived improvement of headache, neck pain and quality of life measured with the GROC scales at the timepoints T2 and T3.
Pearson’s correlations were calculated to assess the association between change in the primary outcomes and neuroscience and migraine quiz scores.
Intention to treat was employed in the analysis (all randomized subjects were analyzed) and the five missing values at post-treatment and follow-up timepoints were replaced by simple imputation.
All statistical analyses were performed at a significance level of 5% using IBM SPSS Statistics, version 26.0, by a researcher (GFC) blinded to the group allocation.
Results
Between March 2020 and August 2021, 84 subjects were recruited. Two persons were excluded before randomization, since they did not fulfil the migraine criteria defined by the ICHD-III (23). Figure 1 shows the progression of study participants within the RCT. The unequal group size arose by chance, since no block randomization was performed. Each participant selected one of two sealed envelopes.

CONSORT flow diagram: progression of study participants within this RCT (enrollment, intervention assignment, follow-up, and evaluation) (38) and measurement timepoints.
Patient characteristics
Most participants (45 +/− 12 years, 94% female) reported severe impairment due to headaches accompanied by mild to moderate depressive symptoms and had neck pain on nearly half of the days per month, with mostly moderate neck associated disability (Table 3). Headache frequency, migraine frequency and neck pain intensity differed between groups at baseline. Comparison between T0 and T1 showed no changes over time for either group in terms of headaches, migraine days and medication intake. The frequency of neck pain increased in both groups from T0 to T1, however no between-group difference was observed (Table 4).
Baseline demographic and clinical characteristics measured at baseline (T1).
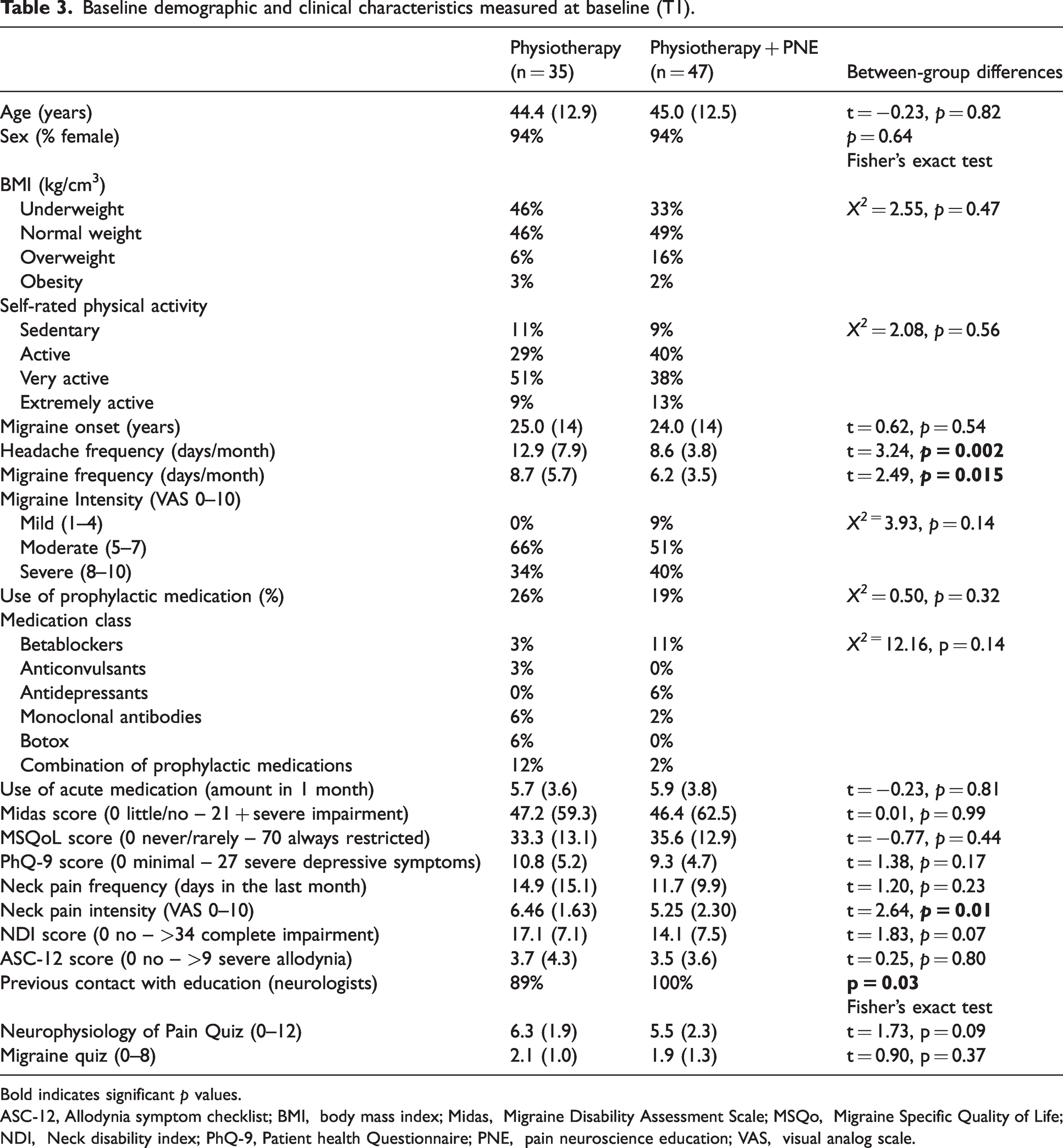
Bold indicates significant p values.ASC-12, Allodynia symptom checklist; BMI, body mass index; Midas, Migraine Disability Assessment Scale; MSQo, Migraine Specific Quality of Life; NDI, Neck disability index; PhQ-9, Patient health Questionnaire; PNE, pain neuroscience education; VAS, visual analog scale.
Extended baseline comparisons of the outcomes which are measured three month and directly before the beginning of the interventions including within and between-group differences.
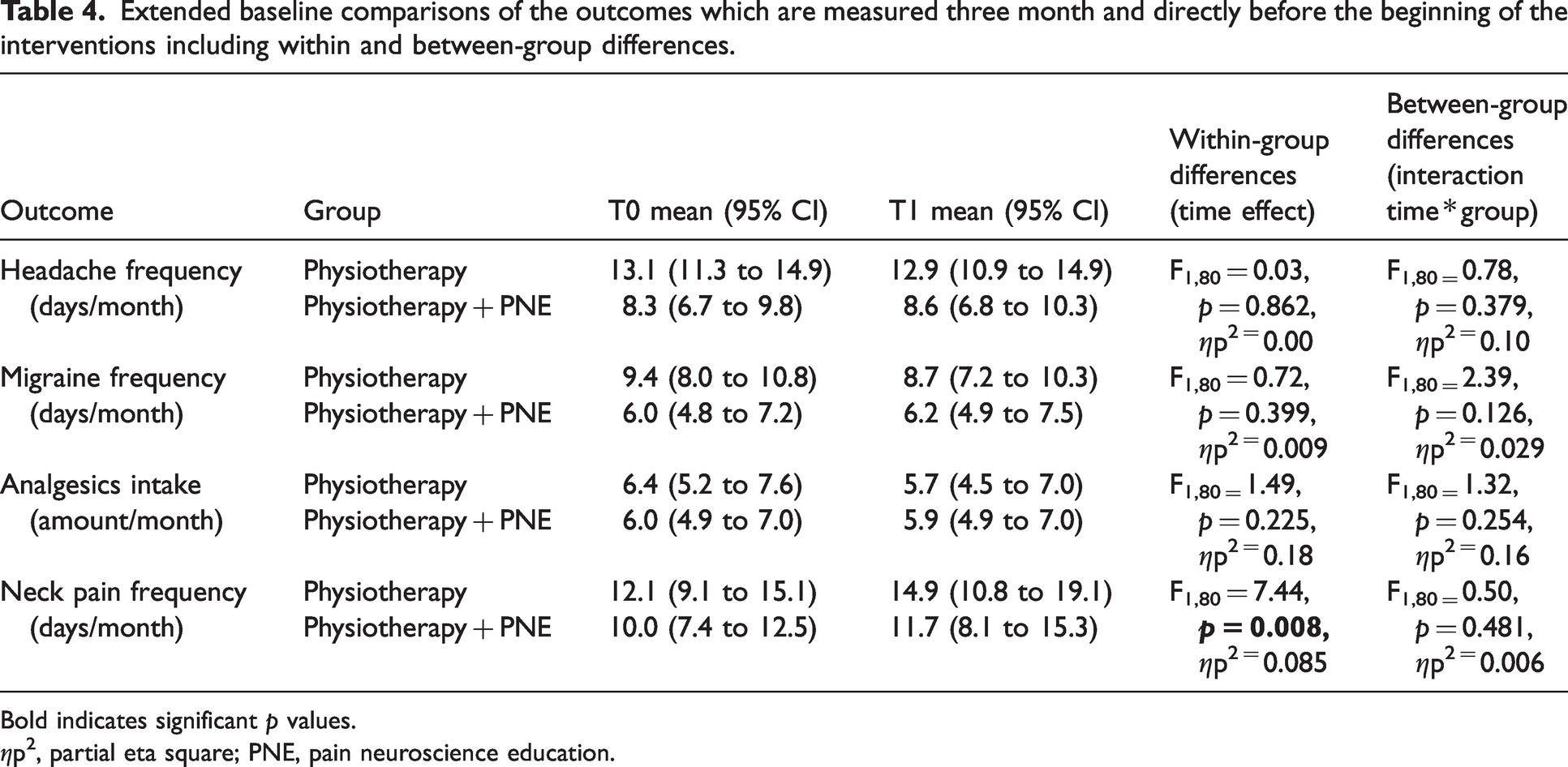
Bold indicates significant p values.ηp2, partial eta square; PNE, pain neuroscience education.
Primary outcomes
Headache days significantly decreased at post-treatment and at follow-up in the total sample (F2,158 = 4.12, p = 0.02) as compared to the prolonged baseline T0 as well as baseline T1 with a small effect size (d = 0.46). Headache days in the PT group significantly decreased by 1.93 days (95%CI: 0.07 to 3.78, p = 0.039) at follow-up but not at post-treatment (mean difference: 0.77, 95%CI: −0.75 to 2.29, p = 0.664). The PT + PNE group also showed a significant reduction of 3.48 days (95%CI: 1.89 to 5.06) at follow-up, but not at post-treatment (mean difference: 1.25, 95%CI: −0.05 to 2.55, p = 0.039). No interaction between group and time was observed for headache frequency (F2,158 = 1.35, p = 0.26, d = 0.26).
When exclusively assessing migraine days per month, there was also an effect of time within both groups (F2,158 = 4.79, p = 0.01) with a medium effect size (d = 0.5). A significant interaction between group*time was observed (F2,158 = 5.04, p = 0.008), with the PT + PNE group showing a larger reduction of migraine frequency (mean effect size d = 0.51). Compared to baseline migraine days within the PT group did not present a significant reduction neither at post-treatment (mean difference: 0.16, 95%CI: −0.93 to 1.26, p = 1.00) nor at follow-up (mean difference: 0.99, 95%CI: −0.25 to 2.24, p = 0.163). The PT + PNE group presented a reduction of 1.28 migraine days (95%CI: 0.34 to 2.22, p = 0.004) at post-treatment and 3.05 days (95%CI: 1.98 to 5.06, p < 0.0001) at follow-up, in contrast to baseline (Table 5, Figure 2). In comparison to the PT group, the PT + PNE presented a significant reduction of 2.06 migraine days at follow-up (95%CI: 0.70 to 3.42, p = 0.003), but not at post-treatment (mean difference: 1.12, 95%CI: −0.07 to 2.31, p = 0.066).
Means (95% CIs) at baseline, post-treatment, and follow-up for all outcomes and interactions of group and time including effect sizes (d).

Bold indicates significant results.Mean values of all outcomes at three time points. Superiority of the combination of PT + PNE is shown for migraine days and the neurophysiology of pain quiz. *p < 0.05, Physiotherapy versus Physiotherapy + PNE. †p < 0.01 within-group differences versus baseline. Effect size d = <0.2 no effect; 0.2–0.4 small effect; 0.5–0.7 medium effect; >0.8 large effect.
ASC-12, Allodynia symptom checklist; Midas, Migraine Disability Assessment Scale; MSQoL, Migraine Specific Quality of Life; NDI, Neck disability index; PhQ-9, Patient health Questionnaire; PNE, pain neuroscience education; VAS, visual analog scale.

Mean and 95% confidence intervals of headache frequency and migraine frequency among groups at baseline, post-treatment and 3-month follow-up. Both groups improved over time and a significant difference between groups was found with the PT+PNE group showing a larger reduction of migraine frequency (†p < 0.01 within-group differences versus baseline. *Between-group differences p = 0.008. **Estimated values adjusted by the baseline).
Migraine-related disability (MIDAS) significantly decreased at follow-up in the total sample (F1,80 = 24.08, p < 0.001) as compared to baseline T1 with a large effect size (d = 1.15). The MIDAS in the PT group significantly decreased 28.0 points (95% CI: 16.4 to 39.6) at follow-up, the MIDAS in PT + PNE group significantly decreased 22.4 points (95% CI: 12.3 to 32.4)). No interaction between group and time was observed for MIDAS scores (F1,80 = 0.30, p = 0.583, d = 0.13).
Secondary outcomes
Results of secondary outcomes (medication intake [number/month], neck pain intensity [VAS], neck pain frequency, Neck disability index [NDI], Allodynia symptom checklist [ASC-12], Patient health Questionnaire [PHQ-9], Migraine Specific Quality of Life [MSQoL]), demonstrated a significant effect of time for each of these outcomes, with no interaction between time and group (Table 5).
A moderate and significant correlation was observed between the reduction of headache days at post-treatment and changes in the “migraine quiz” (r = 0.52, p < 0.0001). Weak and non-significant correlations were observed between the changes in NPQ and reduction of headache days at post-treatment (r = 0.10, p = 0.36), reduction of migraine frequency post-treatment (r = 0.10, p = 0.372), and changes in the “migraine quiz” (r = 0.03, p = 0.79). Both groups rated the GROC questions on headache, neck pain and quality of life similarly. Mean improvements ranged between +2.0 and +3.0 points post treatment and at three-month follow-up (Table 6).
Patients’ perception of change post treatment and at three-month follow-up according to GROC scales.

GROC, Global rating of change.
No harmful or adverse events were observed during the study.
Discussion
This study is the first to investigate additional effects of PNE to physiotherapy in patients with migraine. While the interaction of time and group was not statistically significant for the reduction of headache frequency and MIDAS, there was a trend towards better outcomes in favor of PNE for the primary endpoints just mentioned, especially at follow-up. The MIDAS showed in both groups high scores at baseline. A score >21 is considered a severe impairment. The ANOVA showed a significant effect of time at three-month follow-up for both groups (within-group differences p = 0.001) but a between groups difference for MIDAS scores was not observed evaluating the interaction of time and group. A change of 4.5 points or more in four weeks (for three months = 13.5 points) represents a clinically significant change for patients with frequent episodic and chronic migraine (58). Improvement values at follow-up were far above this minimally important change cut-off in both groups with a strong effect size (d = 1.15). An improvement of more than 50% was only measured in the PT + PNE group (Table 5).
The analysis further showed that combining physiotherapy with PNE was superior to physiotherapy alone, by significantly decreasing migraine days by about three per month. A similar but not significant direction was seen in the secondary outcomes and in patients' perceptions of change; in five of six categories, patients in the PT + PNE group reported a greater positive change. Specifically, the variable “migraine days/month” is addressed by the PNE and the neurophysiology of chronic pain. Therefore, we attribute the results to the additional intervention. It is certainly worth discussing that the PT + PNE group received more therapy overall and the combination of two different treatment approaches can generally lead to better results, but the additional treatment should otherwise have affected the other variables as well. Furthermore, we aimed to specifically investigate if adding an intervention that is standard care for other chronic pain conditions, would provide an additional benefit for migraine patients.
Learning the underlying neurophysiology of pain seemed to have effectively enhanced the patients’ understanding of their disease, as shown by the improvement in the neurophysiology of pain and migraine quiz. Furthermore, the correlation between the migraine quiz results and headache frequency improvement might be explained by reduced migraine-related fear and modified pain cognitions. In other pain conditions, this has been reported to evoke a “desensitization of overactive alarm systems” and brain areas involved in pain (43,59) and positively influenced emotions and thoughts (37). The one-to-one setting used in this current study allowed to take into account the individual behavioral, psychological, and environmental factors that may contribute to a specific patient’s pain experience and persistence.
Interestingly, almost 100% of the participants stated that they had already received education on migraine, which consisted of information about the disease. However, none of the patients had received any information about the neurophysiology of pain, which is specifically addressed in the pain neuroscience education intervention, applied in this current study. Previous research on the influence of education on migraine focused on lifestyle factors such as sleep and eating behavior, stress reduction, relaxation, trigger management and medication use (36,60). A result of 60% correct answers in the Neurophysiology of Pain Quiz is deemed to indicate successful participation in PNE (52). As expected, only the PT + PNE group (79% correct answers vs 55% in the PT group) improved their knowledge on the neurophysiology of pain.
Some concepts within the classical PNE – primarily designed for patients with low back pain or osteoarthritis – cannot be intuitively transferred to migraine, therefore contents had to be adapted. A moderate and significant correlation was found between the reduction of headache days after treatment and migraine-specific knowledge, mapped in the migraine quiz. The current data provides first evidence that comprehensive information on migraine as a chronic pain disease may help desensitize the “overactive alarm systems” in this population. Migraine patients reported fear of attacks as an important indicator of improvement after non-pharmacological interventions (45). A better understanding of the disease and its underlying pathophysiology may facilitate a reduction of this fear of the next attack.
Significant superiority of the PT + PNE combination was shown in the analysis of migraine days per month, which is in line with results for combined PNE and physiotherapy in other pain syndromes (61,62), also shown to be effective to reduce chronic neck pain (63). Considering that up to 80% of migraine patients complain about neck pain (3) and that neck dysfunctions were detected in almost all migraine patients (12), an examination of the neck and a treatment approach addressing identified neck dysfunctions or even chronic neck pain, should be a routine procedure in migraine management.
Previous research highlighted the added value of combining PT with PNE (37,64,65), therefore this approach was chosen for the current study. The reasoning behind this combination was to modify pain “bottom-up” (by reducing nociceptive afferents) as well as “top-down” through PNE (activating endogenous pain modulation) (66).
The PT + PNE group had a reduction in neck pain days at follow-up which was not observed in the PT group. This indicates that understanding the pathophysiology strengthens self-efficacy (41), an effect previously demonstrated for other chronic pain conditions following PNE (37,65).
Limitations
A limitation of this study is the absence of a control group that did not receive an intervention to more specifically assess the effect of physical therapy. We used an extended baseline in order to provide more reliable pre-post estimations for the effect of physiotherapy. Taking into consideration the three months of baseline data, the current study allows us to estimate the effect of physiotherapy in migraine. However, this needs to be confirmed by future studies in a randomized controlled design.
Secondary outcome measures indicated that physiotherapy can reduce acute medication intake, neck pain intensity and neck associated disability as well as allodynia, depression, migraine associated disability and that it improved the disease-related quality of life. However, the study design without a control or placebo group did not allow reasoned recommendation regarding the efficacy of additional PNE rather than for the efficacy of physiotherapy alone. Furthermore, the combination of two different treatment approaches can generally lead to better results. In this way we recommend that future studies consider the addition of a "sham-PNE" intervention, which would complement the findings of the current study.
The effect of the intervention was only assessed at a three-month follow-up, thus future studies are necessary to study long-term effects. Previous research on PNE showed that effects stabilized or even increased over time (63).
Conclusion
This study is the first to describe and apply a structured PNE curriculum in a migraine population. Both groups, physiotherapy or physiotherapy + PNE, showed improvement of primary and secondary outcomes data over time. Physiotherapy in combination with PNE was superior to physiotherapy alone regarding the reduction of migraine frequency. More stringent RCTs are needed to improve the strength of the evidence. Physiotherapy should be considered for the treatment of migraine patients and accompanied by education on the neurophysiology of pain.
Article highlights
Migraine patients receiving either physiotherapy or physiotherapy + pain neuroscience education showed improvements in the primary and secondary outcomes after the intervention. Physiotherapy combined with pain neuroscience education was more effective than physiotherapy alone to reduce migraine frequency. Physiotherapy also accompanied by pain neuroscience education can be considered for the treatment of migraine.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: A funding source by the Friedrich-Ebert-Stiftung, doctoral funding, Godesberger Allee 149, 53175 Bonn was received by the corresponding author RM.
Other information
The trial is registered at the German Clinical Trials Register (Deutsches Register Klinischer Studien) (DRKS00020804), accessible at: https://www.drks.de/drks_web/navigate.do?navigationId=trial.HTML&TRIAL_ID=DRKS00020804 All the datasets used and analyzed during the current study are available from the corresponding author on reasonable request.