
Abstract
Objective
To identify the most frequent causes of secondary pseudotumor cerebri syndrome and compare phenotype, clinical presentation, and symptoms of secondary pseudotumor cerebri syndrome to the primary form of pseudotumor cerebri syndrome, idiopathic intracranial hypertension.
Methods
The study was a prospective cohort study including patients with new-onset pseudotumor cerebri syndrome. Diagnostic work up was standardized. Patients were diagnosed with secondary pseudotumor cerebri syndrome or idiopathic intracranial hypertension according to the revised Friedman criteria. Secondary pseudotumor cerebri syndrome patients were categorized into five causes: medication, systemic causes, sleep apnea, cerebrovascular causes, and several competing causes. Phenotype, clinical presentation, symptoms and neuroimaging were compared between groups.
Results
Out of 278 cases, 28 secondary pseudotumor cerebri syndrome and 120 idiopathic intracranial hypertension patients were included. The most frequent causes of secondary pseudotumor cerebri syndrome were medication (n = 8, 28.6%) and systemic causes (n = 8, 28.6%), followed by sleep apnea (n = 5, 17.9%), cerebrovascular causes (n = 4, 14.3%) and several competing causes (n = 3, 10.7%). Secondary pseudotumor cerebri syndrome and idiopathic intracranial hypertension patients were phenotypically alike and predominately female, premenopausal, and obese. Symptoms and objective findings at disease onset were similar between groups.
Conclusion
Secondary pseudotumor cerebri syndrome should be considered in all patients with suspected pseudotumor cerebri syndrome as secondary pseudotumor cerebri syndrome and idiopathic intracranial hypertension patients are phenotypically and clinically alike. A thorough diagnostic workup is needed as treatment of idiopathic intracranial hypertension and secondary pseudotumor cerebri syndrome is markedly different.
Introduction
Pseudotumor cerebri syndrome (PTCS) is the overarching term for a neuro-ophthalmological disorder characterized by elevated intracranial pressure (ICP) and papilledema in the absence of hydrocephalus or structural cerebral lesions and with normal composition of the cerebrospinal fluid (CSF) (1). Symptoms include headaches, pulsatile tinnitus and visual disturbances (2,3). PTCS can occur in a primary form with unknown etiology, also known as idiopathic intracranial hypertension (IIH), or secondary to other identifiable causes (sPTCS). PTCS is diagnosed according to the revised Friedman criteria, and while papilledema is typically found, the condition can also occur without papilledema (1). IIH is closely related to female sex, obesity, and pre-menopausal age. Diagnosis of IIH can be difficult due to a heterogeneous clinical presentation and 40% of patients referred to tertiary care centers with a primary diagnosis of IIH have been reported to be misdiagnosed (4). Secondary causes of PTCS include a very broad spectrum ranging from cerebral venous abnormalities, hypercoagulative states, sleep apnea and anemia to rare side effects of medical drugs e.g. retinoids, tetracycline class antibiotics, corticosteroids or lithium (5–12). Important differential diagnoses of PTCS include cerebrovascular venous sinus thrombosis (CVST), optic neuritis and cerebral infections (1,13,14). Thus, the phenotype of sPTCS is most likely highly variable. The management of IIH and sPTCS is markedly different, and therefore, early and correct differentiation is crucial (1).
Patients with sPTCS and patients with IIH may have an identical clinical presentation such as headache and visual disturbances (2,15–17). According to the current consensus guidelines (13) sPTCS should primarily be suspected in patients with an atypical phenotype e.g. males, post-menopausal females or BMI <30. Previous studies investigating sPTCS have primarily been case studies or retrospective studies and only one recent literature review has reviewed various causes of sPTCS (18). Interestingly this study found that among sPTCS cases, 70.9% were female and 40.4% had a BMI >25 (18). This begs the question whether clinicians should consider sPTCS in patients who display the typical IIH phenotype or whether this should primarily be a concern in atypical patients. In this prospective cohort study, our primary aim was to identify the most frequent causes of sPTCS. Secondary aims were to compare phenotype, clinical presentation and presenting symptoms of sPTCS patients and IIH patients. We hypothesized that the most frequent cause of sPTCS would be treatment with certain medications and that sPTCS patients would have a different phenotype from IIH patients.
Methods
Inclusion of participants
This study is a prospective cohort study. A total of 278 patients with clinically suspected new-onset PTCS were included from two highly specialized centers with multi-disciplinary expertise in PTCS (the Department of Neurology, Odense University Hospital, and the Danish Headache Center, Rigshospitalet-Glostrup) between January 2018 to July 2021. Inclusion criteria for patients were clinically suspected new-onset PTCS (1), and above 18 years of age. Exclusion criteria were missing data, not fulfilling the revised Friedman criteria (identified as non-PTCS), relapse of PTCS, pregnancy or breastfeeding. All patients had a baseline interdisciplinary diagnostic workup. This included a structured medical interview, somatic, neurological, and neuro-ophthalmological examination, routine blood collection, lumbar puncture including opening pressure (OP) and CSF status (protein, glucose, and cell count), cerebral MRI, and cerebral venography (CT or MRI). OP was measured using a standard issue manometer (cm CSF), with the relaxed patient placed in the left lateral decubitus position with neck and legs extended. The neuro-ophthalmological examination included visual acuity, visual fields, optical coherence tomography and ophthalmoscopy by a senior neuro-ophthalmologist. Papilledema was graded according to the Frisén scale (19). The worst eye was used as the study eye. As part of the medical interview all patients were asked if they had experienced symptoms of sleep apnea e.g. daytime sleepiness, nightly snoring etc. If a suspicion of sleep apnea was raised from the medical interview, patients were offered to undergo polysomnography.
Neuroimaging was assessed by a neuro-radiologist to identify any space occupying lesions, thrombosis, or signs of elevated ICP. Supplemental diagnostic procedures were added if the patient was suspected to suffer from sPTCS and the cause was unclear: polysomnography, genetic evaluation, supplementary specialized blood samples (e.g. antibodies, specialized hematology, rheumatology and endocrinology) and bone marrow investigations (13).
A brief version of the revised Friedman criteria is provided in Table 1 (1). After the diagnostic work-up patients diagnosed with PTCS (including definite PTCS, probable PTCS, suggested PTCS without papilledema (WOP) or PTCS-WOP) were divided into two groups (1): one group included patients with IIH and the other group included patients with sPTCS. Patients were diagnosed by consultants with expertise in PTCS (DB, RHJ and JJK) according to the revised Friedman criteria (1). sPTCS was suspected in patients with conditions, clinical findings or medications associated with sPTCS as described by the consensus guidelines (13) and the revised Friedman criteria (1). In this group we also included CVST as sPTCS in line with recent consensus guidelines and the current diagnostic criteria (1,13).
Diagnostic criteria for Pseudotumor Cerebri Syndrome (Revised Friedman Criteria [1]).a
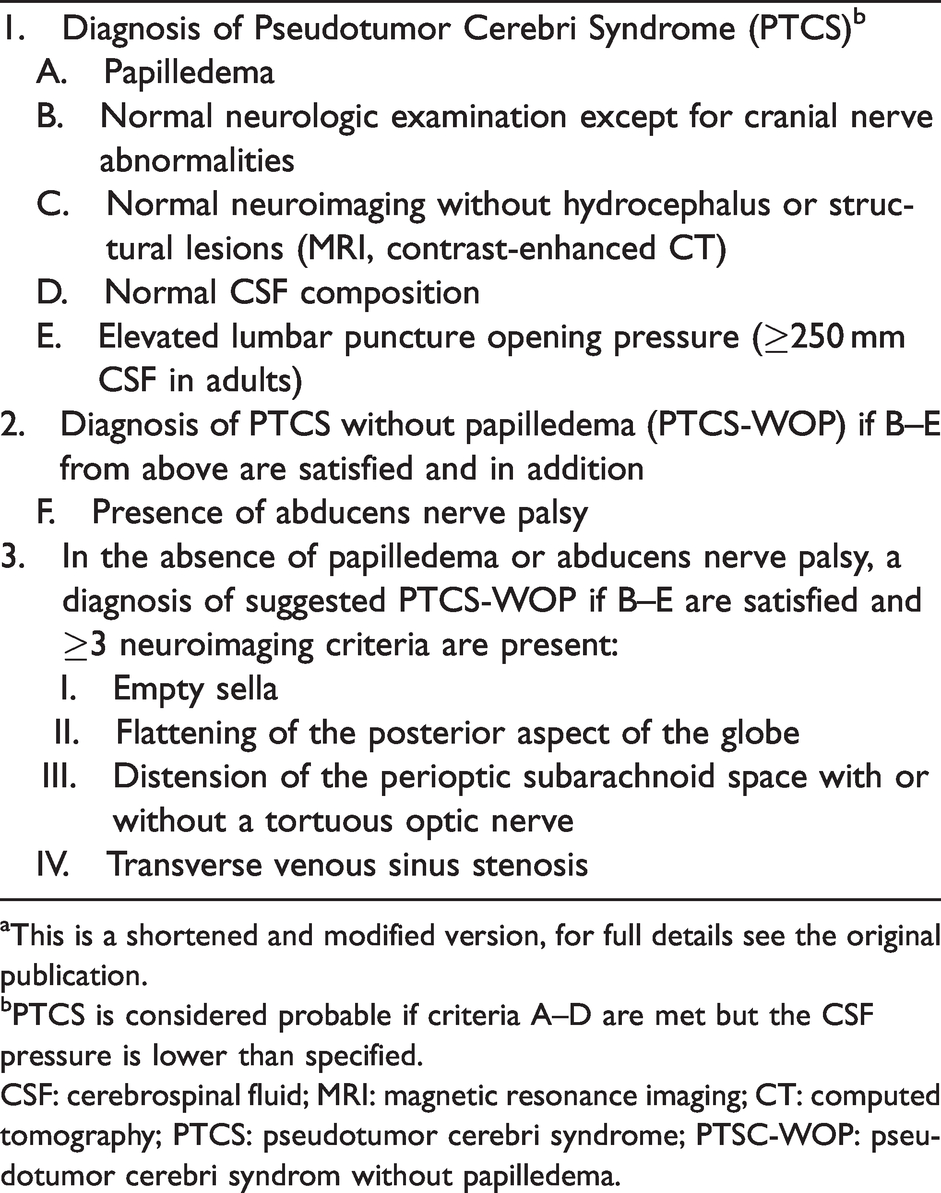
aThis is a shortened and modified version, for full details see the original publication.
bPTCS is considered probable if criteria A–D are met but the CSF pressure is lower than specified.
CSF: cerebrospinal fluid; MRI: magnetic resonance imaging; CT: computed tomography; PTCS: pseudotumor cerebri syndrome; PTSC-WOP: pseudotumor cerebri syndrom without papilledema.
We categorized patients with sPTCS into 5 categories: medication, systemic causes, sleep apnea, cerebrovascular causes, and several competing causes known to cause sPTCS. Patients with medication induced sPTCS were included if the drug has been well established as a potential cause of sPTCS by previous studies (1,12), and symptoms occurred within a reasonable time after drug exposure, defined as within five half-lives of the drug (20). The systemic causes category included patients with conditions described by the consensus guidelines (13) to cause sPTCS. One patient had an atypical presentation of CHARGE-syndrome (acronym for Coloboma, Heart defects, choanal Atresia, Retardation, Genitourinary malformation and Ear abnormalities) with no hydrocephalus and underwent thorough neurologic and genetic evaluation, that concluded CHARGE syndrome to be the cause of sPTCS (the patient had genetic variants in the CHD7-gene and a clinical presentation compatible with CHARGE-syndrome except for hydrocephalus) (21,22). Patients with obstructive sleep apnea (OSA) or upper airway resistance syndrome (UARS) were identified as sPTCS if treatment (CPAP) was recommended. This is in accordance with previous studies where only OSA or UARS requiring treatment, are considered serious enough to cause elevated ICP (8,23). Cerebrovascular causes included CVST and one case of antiphospholipid syndrome (APS) with substantial clinical and radiological suspicion of venous thrombosis in the left internal jugular vein.
Evaluation of neuroimaging
All included patients had a cerebral MRI and CT or MRI venography evaluated by a neuroradiologist as part of the diagnostic workup unless contraindications were present. Furthermore, a subset of the scans (96 IIH patients, 80% and 26 sPTCS patients, 92.9%, p = 0.2) were subsequently evaluated for research purposes by a neuroradiologist (LH), who was blinded to patient identity and results of the diagnostic work up. LH was instructed to describe the specific signs of elevated ICP as described in the revised Friedman criteria: Empty sella or partial empty sella, flattening of the posterior aspect of the globe, distention of the perioptic subarachnoid space and transverse venous sinus stenosis (1). Pituitary morphology associated with PTCS was described according to Yuh et al. (24) in which the cut-off point is grade III (partial empty sella). The more extensive version of this, empty sella (grade V) (1,24) was also included. Distention of the perioptic subarachnoid space and flattening of the posterior aspect of the globe was considered positive, if present either uni- or bilaterally. Transverse venous sinus stenosis was graded 1–4 on each side according to Carvalho et al. (25). The two grades were multiplied to a score (ITSS) and a value of ≥4 was considered pathological (25).
Statistical analysis
The R software was used. As several causes of sPTCS are rare, e.g. systemic lupus erythematosus (SLE), we aimed to include at least 100 patients with PTCS. To describe categorical variables, frequencies and percentages were used. To describe continuous variables, means and standard deviations or interquartile range (IQR) were used depending on the normality of the data. The Welch t test, Wilcoxon rank sum test and Fisher’s exact test were used as appropriate. Patients with missing answers were excluded from the given analysis. We considered p < 0.05 to be statistically significant. The upper limit of a standard issue manometer is 50 cm CSF, 28 patients had an OP equal to or above this. We evaluated these patients to the highest measurable OP for the statistical analysis. OP may therefore be underestimated in this study.
Standard protocol approvals, registrations, and patient consents
The study was approved by the local ethical committee (Region of Southern Denmark, project ID: S-20170058) and followed Danish data regulations. All participants provided written informed consent.
Data availability
De-identified participant data can be shared upon request from qualified researchers who provide a methodologically sound proposal. Legal requirements state that a data processing agreement is signed and approved by the data protection office in the Region of Southern Denmark. Data is available two years after publication. Requests should be directed at the corresponding author.
Results
Of the initial 278 patients evaluated for the study, a total of 148 patients were included in the study, 120 (81.1%) IIH patients and 28 (18.9%) sPTCS patients. The remaining 130 patients were excluded based on: non-PTCS (n = 95), relapse of PTCS (n = 12), pregnancy (n = 3) and missing data (n = 20) (Figure 1). The alternative diagnoses in the non-PTCS group were as follows: 58.9% (n = 56) another primary headache disorder (tension-type headache and/or migraine and new daily persistent headache), 12.6% (n = 12) a secondary headache or facial pain disorder (posttraumatic headache, trigeminus neuralgia etc.), 8.4% (n = 8) an ophthalmological disorder (anterior ischemic optic neuropathy (AION), non-arteritic AION, diabetic papillopathy, inflammatory optic neuritis or glaucoma) or pseudopapilledema, or 20% (n = 19) other headache disorders.

Inclusion of patients.
Management and causes of sPTCS
The most frequent causes of sPTCS were medication (n = 8, 28.6%) and systemic causes (n = 8, 28.6%). Thirty-two (21.6%) of the included patients underwent polysomnography and five patients had sPTCS related to sleep apnea (17.9%). Four patients had cerebrovascular causes (14.3%) including CVST, stenosis after previous CVST, and APS with substantial clinical and radiological, but not confirmed, suspicion of thrombosis. Three patients (10.7%) had several competing causes known to cause sPTCS (cerebrovascular, renal and medication). The group with medication induced sPTCS included tetracycline (n = 2), lithium (n = 2), prednisolone (n = 1), retinoids (n = 1), tacrolimus (n = 1), and ustekinumab (n = 1). Patients in the systemic causes group had severe anemia (hemoglobin level ≤5 mmol/L, n = 3), SLE (n = 2) and other medical conditions (n = 3; polycythemia vera, CHARGE syndrome and severe kidney disease). Results are presented in Figure 2.

Secondary pseudotumor cerebri syndrome divided in categories.
Patient characteristics
Patient characteristics were compared between the sPTCS-group and the IIH-group. Patients in both groups were predominantly female (92.9% for sPTCS versus 96.7% for IIH, p = 0.3) and obese (BMI 35.6 versus 36.4 respectively, p = 0.6). In both groups mean age was within the pre-menopausal age range but sPTCS patients were significantly older than IIH patients (age 33.9 versus 28.9 years, p = 0.003) (Table 2). Presenting symptoms were similar between the two groups and included chronic headache (>15 headache days per month, 65.4% versus 61.1%, p = 0.8), dizziness (57.7% versus 43.3%, p = 0.2), transient visual obscurations (29.6% versus 39.2%, p = 0.4), blurry vision (55.6% versus 60.8%, p = 0.4), photopsia (14.8% versus 17.5%, p = 1) and double vision (16% versus 30.7%, p = 0.2). IIH patients were significantly more likely to have pulsatile tinnitus than sPTCS patients (30.8% versus 56.1%, p = 0.03) (Table 3).
Management of patients and patient characteristics.

a Structured medical interview, somatic, neurological, and ophthalmological examination performed by a consultant with expertise in IIH, routine blood collection, lumbar puncture including opening pressure and routine CSF status, cerebral MRI, and cerebral venography (CT or MRI).
b Different/additional treatment included: Anticoagulants, thrombectomy, CPAP, correction of anemia, withdrawal from medications and treatment with immunosuppressants.
c Missing data excluded: Degree of papilledema (IIH, n = 3 and sPTCS, n = 1), abducens nerve palsy (IIH, n = 2 and sPTCS, n = 3), opening pressure (sPTCS, n = 1).
d Surgery included: Optical nerve fenestration (uni- or bilateral), ventriculoperitoneal shunt, or ventriculoatrial shunt.
e In case of immeasurably high ICP the highest assessable value was used (IIH, n = 24 and sPTCS, n = 4).
CSF: cerebrospinal fluid; IIH: idiopathic intracranial hypertension; IQR: interquartile range; SD, standard derivation; sPCTS: secondary pseudotumor cerebri syndrome.
Symptoms.

a Missing data excluded: Headache days (IIH, n = 7 and sPTCS, n = 2), transient visual obscurations (sPTCS = 1), blurry vision (sPTCS = 1), photopsia (sPTCS = 1), double vision (IIH, n = 6 and sPTCS, n = 3), dizziness (IIH, n = 16 and sPTCS, n = 2), pulsatile tinnitus (IIH, n = 6 and sPTCS, n = 2).
IIH: idiopathic intracranial hypertension; sPCTS: secondary pseudotumor cerebri syndrome.
There was no significant difference in mean OP (36.9 cm CSF versus 40.1 cm CSF, p = 0.1) or abducens nerve palsy (8% versus 8.5%, p = 1) between the two groups. We found no difference in severity of papilledema between the groups but patients with sPTCS were more likely to have suggested PTCS-WOP or PTCS-WOP compared to patients with IIH (18.5% versus 5.1%, p = 0.04). Furthermore, there was no difference in presentation with vision threatening papilledema in need of surgical intervention between the two groups (3.6% versus 5.8%, p = 1) (Table 2).
The secondary causes of PTCS became evident in test results from our standard diagnostic workup in 16 (57.1%) of the patients determined to have sPTCS. For the remaining 12 (42.9%) patients a suspicion of a secondary cause of elevated ICP was raised through the initial, structured medical interview, but additional diagnostic tests were needed to confirm the diagnosis, e.g. polysomnography, specialized blood analyses, or genetic evaluation. We found that specific treatment efforts, which were not part of our standard of care for IIH but were aimed directly at correcting the secondary cause of elevated ICP, were needed in 23 (82.1%) of the patients with sPTCS (Table 2).
Interestingly we had a patient in our cohort, who debuted with initial sPTCS due to CVST, had complete remission after treatment, and subsequently relapsed without any triggering factor except recent weight gain. Furthermore, one patient was excluded from the study due to previous sPTCS caused by tetracycline. This patient was evaluated due to suspected relapse. At evaluation she had been in complete remission for 10 years after withdrawal from tetracycline, and had no other triggering factors for her relapse, other than a recent weight gain. Both patients had a BMI >30, were female and premenopausal, and experienced relapse only related to weight gain after previous successful treatment of sPTCS.
Neuroimaging
All patients had a cerebral MRI and CT or MRI venography was available in 27 (96.4%) patients with sPTCS and in 120 (100%) patients with IIH (p = 0.2). A blinded evaluation of cerebral MRI was available in 26 (92.9%) patients with sPTCS and 96 (80%) patients with IIH (p = 1). We found no significant difference in any of the neuroimaging findings associated with elevated ICP between the two groups. Results are presented in Table 4.
Neuroimaging.

a A subset of patients were evaluated by a blinded neuroradiologist for research purposes in addition to the clinical evaluation.
b Missing data excluded: Empty sella (grade V) (IIH, n = 27 and sPTCS, n = 5), partial empty sella or empty sella (grade III or more) (IIH, n = 25 and sPTCS, n = 5), distension of the perioptic subarachnoid space (IIH, n = 36 and sPTCS, n = 10), flattening of the posterior aspect of the globe (IIH, n = 43 and sPTCS, n = 11), transverse sinus stenosis (ITTS ≥4) (IIH, n = 30 and sPTCS, n = 5), ≥3 neuroimaging signs (IIH, n = 36 and sPTCS, n = 10).
c Defined according to Yuh et al. (24) into five grades depending on the degree of suprasellar herniation of CSF into the sella. In this study ‘empty sella’ or ‘partial empty sella’ was defined as grade III-moderate suprasellar herniation or more.
d Transverse venous sinus stenosis was graded 1–4 on each side according to Carvalho et al. (25): 1 ≤33% stenosis, 2 = 33–66% stenosis, 3 ≥66% stenosis and 4 = hypoplasia or agenesia. The two grades were multiplied to a score (ITSS) and a value of ≥4 was considered pathological (25).
IIH: idiopathic intracranial hypertension; ITSS: index of transverse sinus stenosis; MRI: Magnetic Resonance Imaging; sPCTS: secondary pseudotumor cerebri syndrome.
Discussion
sPTCS is very important to distinguish from IIH as management is widely different. Few studies have investigated the most frequent causes of sPTCS or any phenotypical differences between sPTCS and IIH patients. The majority of the existing studies have been retrospective and/or case studies (5–11,26–28), and no previous studies have prospectively evaluated the most common causes of sPTCS. Here, we present a prospective cohort study investigating various causes of sPTCS in a population of patients with clinically suspected new-onset PTCS. Nineteen percent of included patients with PTCS had sPTCS. We categorized patients with sPTCS into five categories and found that the most frequent causes of sPTCS were medication and systemic causes, followed by sleep apnea, cerebrovascular causes and several competing causes known to cause PTCS (Online Supplemental Table 1).
Interestingly, the phenotype of sPTCS and IIH patients was similar regarding sex and BMI. sPTCS patients were significantly older than IIH patients. However, this difference, while statistically significant, is not useful for clinicians to distinguish IIH from sPTCS as both means fall well within the typical pre-menopausal age of patients with IIH. IIH patients were significantly more likely to have pulsatile tinnitus but otherwise there were no differences between the two groups regarding presenting symptoms, CSF OP, abducens nerve palsy or neuroimaging findings. We found that sPTCS patients were more likely to fulfill the criteria for PTCS-WOP than patients with IIH, but other than this, there was no difference in grade of papilledema. This finding may indicate that patients with PTCS-WOP might be more likely to have a secondary cause of elevated ICP and should undergo further work-up. Nevertheless, our results demonstrate that clinicians should be very cautious to exclude secondary causes of PTCS in any patient presenting with PTCS. This point is especially important as we show that 82.1% of our patients with sPTCS needed additional treatment, which is not part of the standard of care for PTCS. However, our results also show that with a standardized, comprehensive diagnostic work-up and a thorough medical history, it is possible to identify sPTCS patients early in the diagnostic process. We have provided a checklist for clinicians to identify sPTCS and aid the diagnostic work up of patients with suspected PTCS (Table 5).
Diagnostic workup for patients with suspected PTCS.a

aOur suggestions for additional diagnostic workup for sPTCS should be adjusted according to the individual patient and additional work up other than listed here might be necessary.
bCombined with obesity an increased risk of cerebral sinus venous thrombosis.
CSF: cerebrospinal fluid; PTCS: pseudotumor cerebri syndrome; OP: opening pressure; OSA: obstructive sleep apnea; sPCTS: secondary pseudotumor cerebri syndrome; UARS: upper airway resistance syndrome; CT: computed tomography; MRI: magnetic resonance imaging.
Eight (28.6%) patients had medication induced sPTCS. Medications included tetracycline, lithium, prednisolone, retinoids, tacrolimus and ustekinumab. In a systematic review tetracycline class antibiotics and retinoids had the highest number of reported cases of medication induced sPTCS with ≥20 cases (12). Prednisolone has mostly been associated with sPTCS in children in previous studies (12,18). For two patients categorized as ‘several competing causes known to cause sPTCS’ debut of sPTCS was associated with both prednisolone treatment and renal failure. These cases illustrate that a combination of several risk factors e.g. prednisolone treatment and renal failure (29) is possible.
The systemic causes category included patients with severe anemia, SLE and other systemic causes. An association between elevated ICP and anemia has been reported in various case reports (10,11). In two case series improvement of symptoms and ophthalmologic signs was seen with correction of anemia without any other medical treatment in 13 out of 14 patients with anemia and sPTCS (10,11), stating the importance of identifying these patients. In our cohort 2 patients had sPTCS caused by SLE. Although a rare association, one study found 10 patients with SLE and elevated ICP among 651 hospitalized SLE patients (27). Six out of the 10 patients with SLE and elevated ICP had elevated antibodies for APS and two patients met the criteria for definite APS, whereas the prevalence of APS was only 13% in the general SLE cohort (27). Both patients with SLE associated sPTCS in our cohort had APS and thromboembolic complications, suggesting that elevated ICP in SLE patients could be associated with hypercoagulability.
Five patients (17.9%) had sPTCS related to OSA or UARS. Prior studies have found, that OSA is related to elevated ICP possibly due to hypoxia and hypercapnia during apnea periods causing cerebral vasodilation (30). Obesity is associated with OSA, and it has been suggested that OSA is involved in the pathogenesis of PTCS. A recent study found that 47% of IIH patients with BMI ≥35 kg/m2 had OSA (8) and there was a significant association between improvement of apnea-hypopnea index (AHI) and resolution of papilledema, despite adjustment for BMI (8). We identified five patients with sPTCS related to OSA or UARS and our results suggest, in accordance with previous studies (6–8,23,30), that OSA should be suspected in all PTCS patients.
Cerebrovascular causes of sPTCS included CVST, sequelae due to previous CVST and APS. Similar to PTCS, CVST is related to female sex and obesity (31). CVST is a serious condition and early diagnosis is crucial. MRI in combination with cerebral venography should be standard in all patients with suspected PTCS. Symptoms and signs mimic those of PTCS (31,32). One study found that 10 (9.4%) out of 106 patients with suspected PTCS proved to have CVST (9). We found a much lower incidence of CVST in our cohort as only four patients (2.7%) were identified as having cerebrovascular associated sPTCS. This finding could reflect referral bias, as patients with obvious CVST might not be referred to our centers.
PTCS is a complex mix of diseases that affect ICP-regulation and the exact pathophysiological mechanisms remain largely unknown. We found that sPTCS and IIH were both linked to female sex, childbearing age, and obesity, suggesting a common pathological mechanism of the two conditions. Two patients in our cohort debuted with initial sPTCS and developed IIH subsequently. We speculate that some patients with sPTCS may share common pathological risk factors for development of PTCS as IIH patients. We suggest that sPTCS may be a multifactorial disease, and some of the causes of sPTCS stated in this study might act as trigger factors in pre-disposed individuals, rather than as direct causes.
Strengths and limitations
An important strength of this study is the prospective design and the structured, diagnostic work-up. Patients had a detailed medical interview and a multidisciplinary work-up. Furthermore, in most patients, neuroimaging signs associated with elevated ICP were validated by a blinded neuroradiologist. Patients were not screened with a standardized questionnaire for OSA and only 21.6% of our included PTCS patients had a diagnostic workup for OSA. Furthermore, only patients that required treatment for OSA or UARS were included as sPTCS, therefore OSA might be underestimated in our study. Another limitation was that patients were included at two highly specialized centers. It is possible that patients with mild headache or self-limiting illness were not referred to our centers. Additionally, patients with obvious secondary causes of PTCS, for example CVST, may not be referred to our centers, but treated locally, thus, the true phenotypical difference between sPTCS and IIH patients might be greater than stated in this study.
Conclusion
sPTCS is a challenging diagnosis for clinicians. We have provided the first prospective cohort study investigating known causes of sPTCS. Out of 148 PTCS patients from two highly specialized centers we identified 19% with sPTCS. Almost 30% of the cases in our study were due to medication and systemic causes respectively. Our results show that female sex, childbearing age, and obesity is intricately linked to both IIH and sPTCS, and the clinical presentation is similar, complicating correct diagnosis for clinicians. Importantly, in our study patients with an atypical phenotype (male, high age, normal BMI) are rare also in sPTCS and here differential diagnoses should be further considered. Our results indicate that sPTCS should be considered in all patients with clinically suspected PTCS – regardless of patient phenotype or clinical presentation. The majority of sPTCS patients (82.1%) received a different treatment than standard treatment for PTCS, stating the importance of identifying these patients. Based on our findings we suggest a diagnostic workup plan for clinicians.
Key findings
Non-idiopathic pseudotumor cerebri (sPTCS) is a challenging diagnosis, but not uncommon as 19% of included patients with pseudotumor cerebri syndrome (PTCS) had sPTCS. The two most common causes of sPTCS were medication side effects and systemic causes. Patients with sPTCS and patients with idiopathic intracranial hypertension were phenotypically and clinically alike.
Supplemental Material
sj-pdf-1-cep-10.1177_03331024221120073 - Supplemental material for Phenotyping non-idiopathic pseudotumor cerebri syndrome – A prospective cohort study
Supplemental material, sj-pdf-1-cep-10.1177_03331024221120073 for Phenotyping non-idiopathic pseudotumor cerebri syndrome – A prospective cohort study by Katrine Svart, Rigmor Højland Jensen, Lisbeth Høgedal, Vlasta Vukovic-Cvetkovic, Dagmar Beier and Johanne Juhl Korsbæk in Cephalalgia
Footnotes
Declaration of conflicting interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KS: No conflicts of interest to disclose. RHJ: Gave lectures for Pfizer, Eli-Lilly, ATI, Merck, TEVA, Novartis, Lundbeck and Allergan. Investigator in clinical trials with ATI, Eli-Lilly, Novartis and Lundbeck. Director of Danish Headache Center, Lifting The Global Burden of Headache and Founder of Master of Headache Disorders at University of Copenhagen. Received research funding from University of Copenhagen, Rigshospitalet, ATI, Lundbeck Foundation, The Medical Society in Copenhagen, NovoNordisk Foundation and Tryg Foundation. LH: No conflicts of interest to disclose. VVC: No conflicts of interest to disclose. DB: No conflicts of interest to disclose. JJK: Received funding from the Lundbeck Foundation and Candys Foundation.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Lundbeck Foundation [R-276-2018-403-4], Candys Foundation [grant number 2015-146], Rigshospitalet and Odense University Hospital. Foundation between Rigshospitalet and Odense University Hospital 2016 [R25 A1320], 2019 [69-A3346] and 2021 [123-A5083].
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.