
Abstract
Abstract
Objectives
To investigate previous treatment and clinical characteristics in migraine and tension-type headache patients at their first visit to a tertiary headache center.
Methods
This was a cross-sectional study using data obtained from electronic questionnaires and medical charts. Migraine and tension-type headache patients were investigated at their first visit to the Danish Headache Center.
Results
Out of 382 patients the main diagnoses of primary headaches were: 36% with episodic migraine, 43% with chronic migraine, 3% with episodic tension-type headache and 17% with chronic tension-type headache. The majority had attempted non-pharmacological treatment options such as physiotherapy (episodic migraine: 53%, chronic migraine: 68%, episodic tension-type headache: 50%, chronic tension-type headache: 65%) and acupuncture: (episodic migraine: 45%, chronic migraine: 62%, episodic tension-type headache: 17%, chronic tension-type headache: 51%). The majority of migraine patients had tried no more than one triptan (episodic migraine: 71%, chronic migraine: 66%). In total, 35% of episodic migraine and 19% of chronic migraine patients as well as 50% of episodic tension-type headache and 41% of chronic tension-type headache patients had never tried preventive medication. The headache under-response to treatment (HURT) questionnaire score was higher in chronic migraine (score 15) and chronic tension-type headache (score 16) patients than the episodic forms (P < 0.004).
Conclusions
Headache patients had attempted several non-pharmacological treatments prior to their first visit at a tertiary headache center in Denmark. The limited use of acute and preventive treatment before the first visit demonstrates a need for better treatment at the primary and secondary care level.
Keywords
Introduction
Headache disorders are the second leading cause of years lived with disability worldwide (1). This is despite the fact that effective acute and preventive treatments exist for the most frequent primary headache disorders such as migraine and tension-type headache (TTH) (2,3). The Danish healthcare system, which is comparable to other high-income countries, diagnose and manage headaches at three levels. The first level is primary care conducted by general practitioners; the second level is private practicing neurologists or general neurology departments in hospitals. Tertiary care is conducted at specialized headache centers, where medical professionals are trained and specialize in headache disorders (4). In Denmark, diagnosis and treatment of headaches are performed at three levels. At the first level, there are approximately 3,300 general practitioners in Denmark with 5.8 million citizens. At the second level, diagnosis and treatment are handled by the private practicing specialists of neurology or other related professionals with interest and experience in pain conditions or by local neurological departments. There are 44 practicing neurologists in Denmark and 14 neurological departments. The tertiary level consists of headache centers, where medical specialists and interdisciplinary staff specializing in headache conditions are responsible for diagnosis and treatment at the highest national level. There are currently eight headache centers with varying capacity. The largest (The Danish Headache Center) has eight neurologists attending the headache center 1–4 days per week. Headache is the most common neurological symptom presenting at the primary care level (5). It is estimated that in 90% of patients relevant headache treatment can be initiated and maintained at the primary care level (6,7). The level of headache care at the primary and secondary treatment levels is likely reflected by checking how thorough treatment has been prior to the first visit to a tertiary headache center. However, headache patients treatment prior to the first visit at a tertiary headache center has only been elucidated in a few studies so far (8 –11).
The present study is a cross-sectional investigation of patients with migraine and/or TTH referred to the tertiary specialized Danish Headache Center (DHC) at Rigshospitalet-Glostrup, Copenhagen, Denmark. We investigated previous non-pharmacological and pharmacological headache treatment and clinical characteristics in episodic and chronic migraine and TTH patients.
Methods
Study design
This was an observational, cross-sectional study conducted on patients at their first visit to the DHC between May 2020 and March 2021. All patients 18 years or older who had completed an electronic questionnaire and were diagnosed with migraine or TTH were included in the study. Data was collected through an electronic questionnaire sent to the patients prior to the visit as part of routine care and through review of the medical charts from the first visit. In total 748 migraine and tension-type headache patients received the electronic questionnaire of which 348 (47%) responded. A trained medical student (SAM) reviewed medical charts of the first visit to obtain the diagnoses, headache frequency as well as previous pharmacological treatments as this was considered the most reliable information source. Patients diagnosed with both episodic migraine (EM) and episodic TTH (ETTH) were registered as EM. Patients with both EM and chronic TTH (CTTH) were registered as CTTH patients. Only the main headache diagnosis was applied, although they may have been classified with other headache diagnoses. The headache diagnosis was made by the attending doctor supervised by one of the permanent neurologists at the headache center. Over the last 5 years the DHC has seen on average 5,775 consulted patients per year. On average 35% of consulted patients per year have migraine and 23% of consulted patients per year have TTH.
Semi-structured questionnaire
A semi-structured questionnaire was sent electronically to headache patients prior to their first visit at the DHC. The questionnaire contained questions on patients’ headache history, sociodemographic information, clinical history, and previous non-pharmacological treatment. Furthermore, three standardized questionnaires were included: The Headache Under-Response to Treatment (HURT index), Insomnia Severity Index (ISI) and Hospital Anxiety and Depression scale (HADS). The HURT questionnaire is a set of eight questions designed to assess headache burden in terms of frequency, disability, medication use and effect, patients' perceptions of headache “control” and their understanding of their diagnoses (12). HURT-8 is the total score, which ranges from 0–24 with a high score indicating a high headache burden (12). The ISI questionnaire consists of seven questions related to the patients sleep pattern within the last two weeks (13). It ranges from 0–28 points. Points are interpreted as followed: 0–7 (absence of insomnia), 8–14 (sub-threshold insomnia), 15–21 (moderate insomnia), and 22–28 points (severe insomnia) (13). HADS is a self-assessment questionnaire that sets to identify possible cases of depression and anxiety disorder among patients in medical clinics. It contains two subscales: an anxiety scale (HADS-A) and a depression scale (HADS-D), each with seven questions (14). Total score ranges from 0–21 points and are interpreted as followed: 0–7 (normal case), 8–10 (borderline abnormal), 11–21 (abnormal case) (14).
Statistics
Data were presented as either: number with percentage, mean with standard deviation (SD) or median with interquartile range (IQR). Statistical tests were performed on clinical characteristics. Numeric data were compared with Mann-Whitney Test and dichotomous data were assessed using Chi-Square test. A P value <0.05 was considered significant. We did not correct for multiple testing. EXCEL for Office and IBM SPSS Statistics Version 27 were used for descriptive data and statistical analysis.
Ethical approval
The cross-sectional study was approved by the Regional Ethical Committee of the Capital Region (H-18008942) and Rigshospitalet-Glostrup as being a quality control project that did not require patient consent nor formal ethical approval according to Danish law.
Results
Study cohort characteristics
The total sample size consisted of 382 migraine and TTH patients (Table 1). In total, 36% (n = 139) were diagnosed with EM, 43% (n = 166) with CM, 3% (n = 12) with ETTH and 17% (n = 65) with CTTH (Table 1). Most of both EM and CM patients were women (EM: 75%; CM: 91%), mean age was 42 ± 13 and 45 ± 13, respectively. The majority of ETTH and CTTH patients were also women (ETTH: 75%; CTTH: 82%), mean age was 46 ± 16 and 38 ± 16, respectively.
Demographics and clinical characteristics for migraine and tension-type headache patients.

*A: P-value comparing episodic migraine and chronic migraine. *B: P-value comparing episodic and chronic tension type headache (TTH). NA: not applicable; SD: standard deviation.
Clinical characteristics
EM and CM patients had suffered from headaches for two decades (19 ± 14 and 21 ± 14 years) (Table 1). Patients with CTTH had suffered for headache longer than patients with ETTH (11 ± 12 vs. 4 ± 4 years, P = 0.025). CM and CTTH patients reported more days of absenteeism per month than episodic headache patients (CM: 9 vs EM: 4, P < 0.001) and (CTTH: 8 vs ETTH: 2, P = 0.029). Medication overuse headache (MOH) was found in 33% of CM patients and 12% of CTTH patients (Table 1).
Chronic headache patients had a higher HURT-8 score than episodic patients (CM: 15 vs. EM: 12, P < 0.001) and (CTTH: 16 vs. ETTH: 12, P = 0.003) (Table 2). CM patients scored higher on ISI compared to EM patients (median (IQR); CM: 13 (10) vs. EM: 10 (11); P < 0.001), whereas there was no such significant difference between CTTH and ETTH patients (median (IQR); CTTH: 14 (9) vs ETTH: 13 (11); P = 0.508). The median of all patient groups indicated sub-threshold insomnia, defined as an ISI score between 8–14. CTTH patients were more likely than ETTH patients to have symptoms of anxiety. HADS-A score > 8 points were found in 46% CTTH compared to 8% ETTH patients (P = 0.014), while HADS-A score was >8 points in 31% CM compared to 25% EM patients (P = 0.236). Patients with CM were more likely to have symptoms of depression. HADS-D score > 8 points were found in 18% CM vs 9% EM patients (P < 0.001). However, TTH patients differed numerically, but not statistically, in reported HADS-D score (HADS-D > 8 points; CTTH:23% vs ETTH: 0%; P = 0.064). Chronic headache patients were more likely to rate their health as being “rather poor or poor” compared to episodic patients (CM: 46% vs EM: 24%; P < 0.001) (CTTH 43% vs. ETTH 25%; P = 0.241).
Clinical characteristics based on standardized questionnaires.

*A: P-value comparing episodic migraine with chronic migraine. *B: P-value comparing episodic with chronic tension type headache (TTH). **HADS: >8 points in a total subscale score indicates a possible risk of having symptoms of anxiety or depression. ***Low level of physical activity: primarily sedentary activities or light exercise at least 4 hours a week.
HADS: Hospital Anxiety and Depression scale; HURT: The Headache Under-Response to Treatment; IQR: interquartile range.
Previous non-pharmacological treatment
The three main types of non-medical treatments patients had received were physiotherapy, acupuncture, and chiropractic treatment, with the most frequent being physiotherapy (Table 3). In total, 53% EM patients and 68% CM patients had been treated by a physiotherapist. The corresponding numbers for ETTH and CTTH were 50% and 65%, respectively. Acupuncture was attempted by 45% of EM and 62% of CM patients, as well as by 17% ETTH and 51% CTTH patients. In total, 36% EM and 44% CM patients had tried chiropractic treatment as non-medical treatment for their headache, as well as 17% ETTH and 34% CTTH patients. On average, the number of non-pharmacological treatment types among patients who had tried it was 2.9 for EM, 3.3 for CM, 1.8 for ETTH and 2.9 for CTTH. It was only 22% of EM, 21% of CM, 25% of ETTH and 20% of CTTH, who had never tried non-pharmacological treatment options. We did not identify a patient, who had never tried non-pharmacological or pharmacological treatment of any kind.
Previous non-pharmacological treatment.

TTH: tension-type headache.
Previous pharmacological treatment
The majority of migraine patients had tried no more than one type of triptan (EM: 71%; CM: 66%), while 17% EM and 11% CM patients had never tried a triptan (Table 4). Furthermore, only 8% EM and 17% CM patients had tried at least three different triptans prior to their first visit at the DHC.
Previous acute medication.
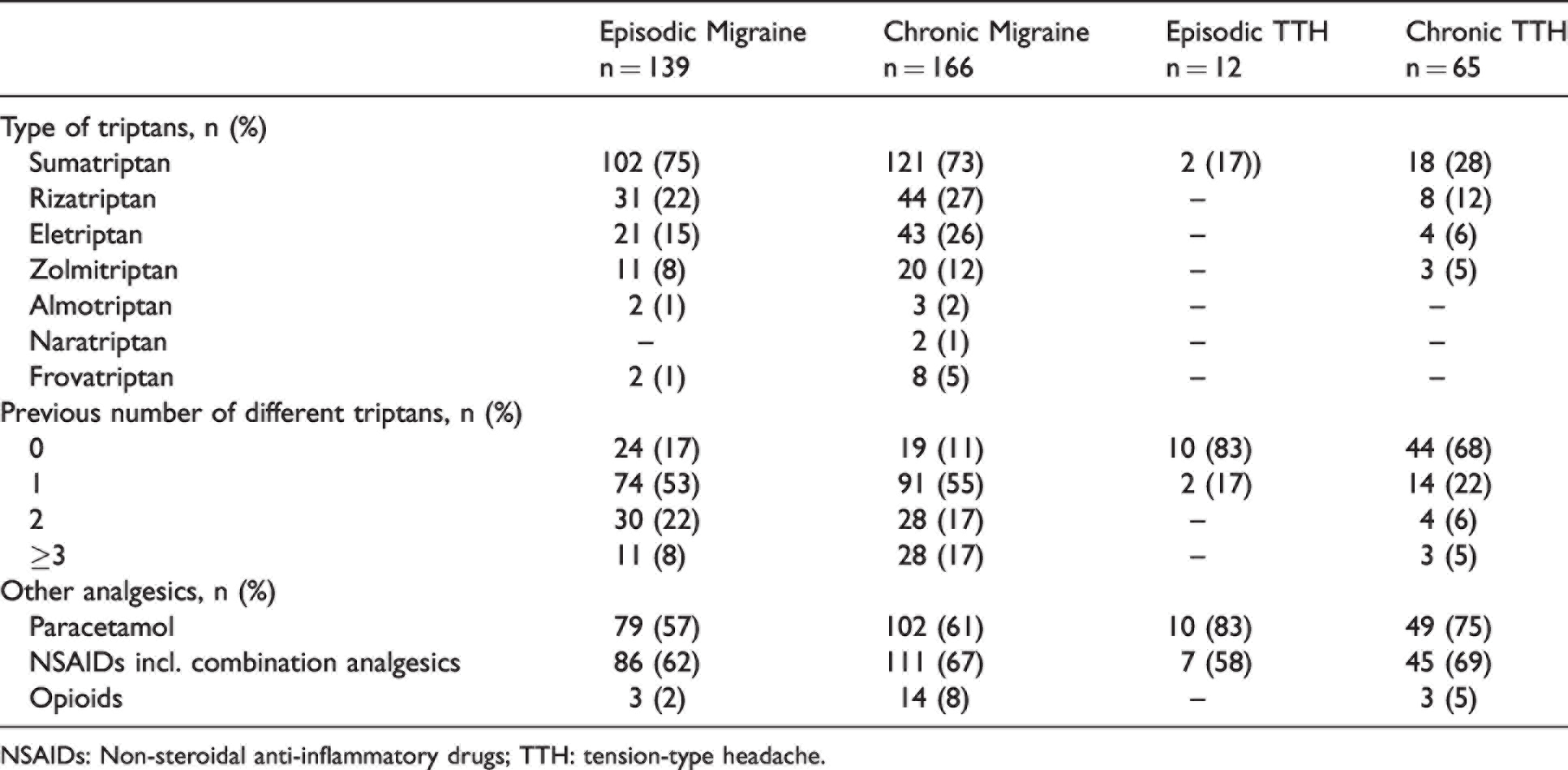
NSAIDs: Non-steroidal anti-inflammatory drugs; TTH: tension-type headache.
A total of 35% of EM and 19% of CM patients had never used preventatives (Table 5). In total, 50% of ETTH and 41% of CTTH patients had also never tried preventatives. Antihypertensives were the most frequently used preventatives by migraine patients (EM: 59%; CM: 73%), while antidepressants were the most frequently used preventatives by TTH patients (ETTH:17%; CTTH:40%) (Table 5).
Previous preventative medication.
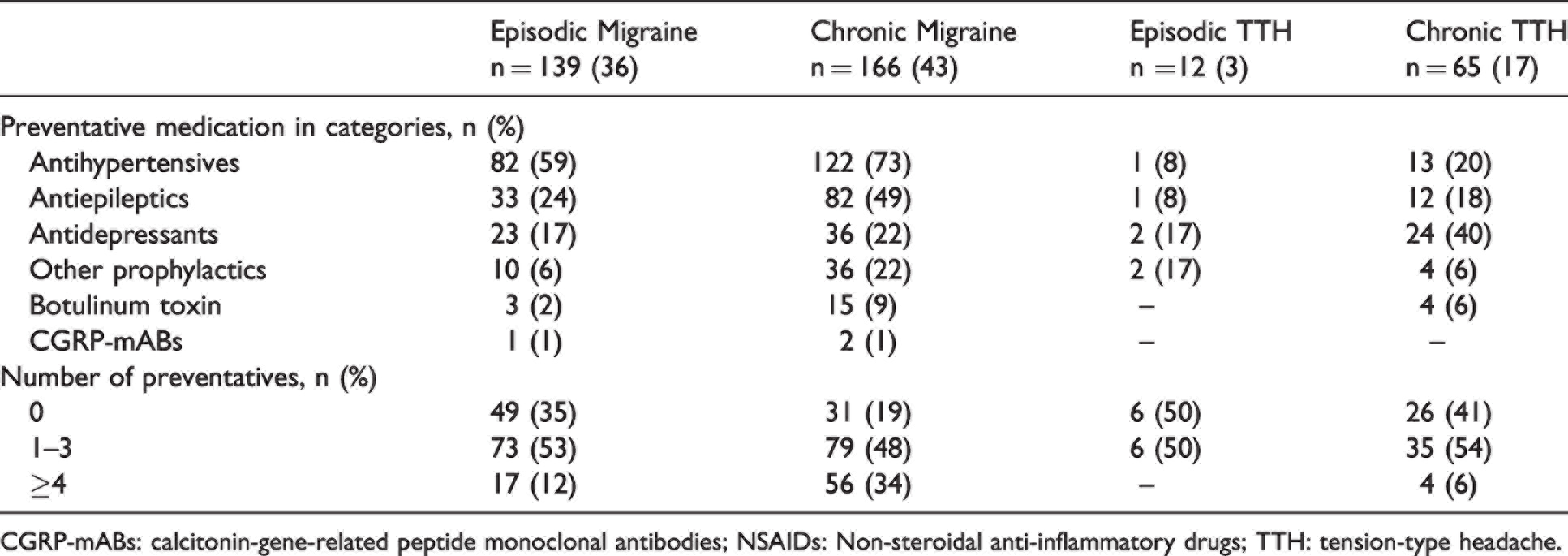
CGRP-mABs: calcitonin-gene-related peptide monoclonal antibodies; NSAIDs: Non-steroidal anti-inflammatory drugs; TTH: tension-type headache.
Discussion
The major findings of this study are that most migraine and TTH patients have attempted approximately three non-pharmacological treatment options before the first visit to a tertiary headache center in Denmark. Only one out of three migraine patients had tried more than one triptan and only one out of six CM patients had tried at least three different types of triptans. One out of three EM and one out of five CM patients had never tried preventive medication prior to their first visit. The headache burden was very high for both migraine and TTH patients and most pronounced in the chronic forms.
Previous non-pharmacological treatments
Patients may seek non-pharmacological treatment to avoid medicine in general or to avoid side effects. In the present study, we found that more than 75% of migraine and TTH patients had pursued non-pharmacological therapies prior to their first visit at the DHC. Physiotherapy, acupuncture, and chiropractic treatment were the most sought out approaches, and more than half of patients in all four categories had tried physiotherapy. This reflects the patients need and desire to find treatment, even though the evidence of effect of, for example, physiotherapy alone is very sparse in both migraine (15,16) and TTH (17). The findings are in contrast to the low proportion of previous pharmacological treatment attempts, which highlight a potential for optimizing headache treatment at the primary and secondary care level.
Previous pharmacological therapy
We found that only 8% of EM and 17% of CM patients had tried at least three triptans. This is surprising for a 30-year-old acute migraine drug class, which is effective and recommended in all current clinical migraine treatment guidelines (4,18 –20). These findings are in line with several studies conducted on migraine patients showing inadequate use of migraine medication prior to their first visit at a tertiary headache center (8,9,21 –23). A study conducted in ten headache centers in Italy found that 54% of migraine patients had never used triptans and only 27% had received a migraine diagnosis (9). An Austrian study showed that 73% of migraineurs had never used triptans prior to their first visit at a tertiary headache center (21). Our findings also appear to coincide with a Danish study that analyzed the trends in triptan use on nationwide data over a 25-year period (24). The study showed that only 12% of the migraine population in Denmark had purchased a triptan between 2014-2019 and that 43% of new triptan users had not repurchased triptans within 5 years (24). Still, our findings are surprising considering that most triptans are currently inexpensive, the Danish population receives free healthcare including free GP visits, free neurological consultations, and reimbursements for part of their medical expenses. Furthermore, there is a strong tradition for headache research in Denmark and big efforts have been made to teach optimal headache care at primary and secondary treatment levels for decades. Thus, the low number of migraine patients that had tried at least three triptans may be due to other factors that needs further exploration. In the current study, we found that our patients relied heavily on paracetamol and NSAIDs including combination analgesics for acute treatment of headache. In a population study published 30 years ago, half of migraine patients and 83% of TTH patients in the previous year had managed with at least one type of drug in the current year, where acetylsalicylic acid preparations and paracetamol were at that time the most commonly used analgesics (25). In Denmark, triptans are prescription drugs, whereas paracetamol and certain NSAIDs such as ibuprofen are over-the-counter drugs. Patients might prefer to self-manage their headaches with analgesics due to its easier accessibility or they might lack awareness of headache disorders and the existing options for treatment. According to guidelines from the Danish Headache Society migraine patients should try at least three different triptans for a minimum of three migraine attacks before the effect of a triptan is ruled out (4). However, the guidelines have not had an optimal effect on Danish medical practice. Furthermore, we found that more attention to preventative treatment is needed in treatment of both migraine and TTH patients. Preventive treatment is indicated for patients with CTTH, when non-pharmacological approaches or analgesics have insufficient outcome, and for migraine patients when attack medications have shown poor efficacy. In our study 41% of CTTH patients had never tried preventatives. For migraineurs, 35% of EM and 19% of CM patients had never used preventatives. In comparison, Rasmussen et al. (25) reported in a population-based study that only 7% out of 119 migraine patients had used preventives over the last year. Furthermore, headache-related consultation rates increased in Demark from 1989–2001, with acute headache medication increased moderately, whereas preventive medication use remained stable (26). A Danish nationwide cohort study found that adherence to preventative migraine treatment is lacking (27), which may be due to insufficient information from health care professionals, lack of patient compliance, ineffectiveness of said treatment or side effects. The improper medical treatment of headache may lead to a significant risk of MOH especially in migraine patients (28). Indeed, a recent national cross-sectional survey of residents in neurology in Denmark showed that overall knowledge of neurology residents on headache disorders do not meet the expectations set out by both national and international recommendations (29). The study identified several deficiencies and barriers in headache management amongst residents particularly related to diagnosis. Even though there are eight tertiary headache centers in Denmark today and more pharmacological options than 30 years ago, there is obviously a need for improved headache care in Denmark. Structured education in headache and other strategic initiatives at all treatment levels should be prioritized by both regional and national stakeholders (29). Headache care is possible to improve in Denmark through education and awareness. As an example, a recent public campaign in Denmark on MOH targeted the general public, general practitioners, and pharmacists (30). The campaign resulted in increase in the percentage of the public who knew about MOH (30). This has also been shown in relation to cluster headache in which diagnostic delay was significantly reduced for each decade of cluster headache onset from 1950-2010 (31).
Clinical characteristics of headache patients at the DHC
In comparing episodic headache patients to their respective chronic patient group, we found that patients in all groups suffered from headache for many years before visiting a tertiary headache center. Both EM and CM patients suffered on average for twenty years with a headache, while CTTH suffered longer than ETTH patients with an average of 11 and 4 years respectively. The long history of headache and relatively sparse use of pharmacological treatment emphasize the need for an early and effective treatment plan for migraine and TTH patients.
In the first epidemiological headache study in Denmark, 20% of the total absenteeism was due to headache (32). We found that on average, our CM and CTTH patients were absent from work for respectively 9 and 8 days a month due to headache. These numbers are quite high and reflect that these chronic headache patients from a clinical population are severely affected. In comparison, a previous Danish population-based study found that 43% of employed migraineurs had missed one or more days off work in the preceding year due to headache (32). Nonetheless, our study further underlines the significant socioeconomic burden on both headache patients and society as a whole. Our findings also emphasize the importance of preventing the transition of episodic to chronic headache in patients, especially when considering the significant differences in missing workdays and overall burden that we found between episodic and chronic headache patients.
The total HURT scores in this study were high and similar to previous studies (12), which is expected among patients referred to tertiary headache centers. HURT scores were larger in CM and CTTH compared to the episodic forms, which is likely driven by higher headache frequency and MOH. The HURT questionnaire can be used for the first assessment but can also assess responsiveness in treatment at follow-up visits to increase the possibility of an effective treatment outcome (12). A large proportion of both migraine and TTH patients showed low self-reported health. These findings are similar to other studies (33 –35) and reflect a considerable impact on the quality of life of these patients, which highlight the need for relevant treatment.
According to previous studies, insomnia, anxiety and depression are more common in individuals with migraine (36) and TTH (3) compared to people without headache. Data from all four patient groups in our sample suggests subthreshold insomnia, with CM scoring higher than EM patients. This is in line with insomnia having been identified as a trigger for both migraine (37) and TTH (38), making it important to recognize in headache patients when aiming to improve quality of life of these patients. Furthermore, our study found that most patients did not show considerable symptoms of anxiety or depression, except for CTTH patients where 46% showed possible risk of anxiety. Nevertheless, screening for and treatment of psychiatric comorbidities may improve prognosis for the individual patient (39).
Distribution of migraine and TTH-patients referred to the DHC
Despite TTH being the most common headache disorder in the general population, migraine appears to be diagnosed more frequently in tertiary care (40), which we also found in our study. There are several factors that could explain this. TTH has received less scientific attention with fewer treatment options compared to migraine and other headache disorders, despite being the most prevalent form of primary headache disorder worldwide (3,41,42). Furthermore, 94% of migraine patients also suffer from coexisting TTH (43), but usually only the migraine diagnosis is registered. It has previously been shown in a Danish population study that while 56% of migraine patients had consulted a GP, the corresponding proportion was only 16% for TTH patients (32). TTH may also be perceived by sufferers as less debilitating due to the mild to moderate pain intensity. However, CTTH significantly affects daily functioning as demonstrated by the higher degree of absenteeism to the same degree as in CM (8 days per month vs 9 days per month) and compared to ETTH patients (eight days per month vs two days per month) (32).
Study strengths and limitations
This study is a real-life study from a tertiary clinic illustrating the significant burden on our patients. The instruments used are validated and easily applied in clinical as well as in population studies making comparisons possible. Data such as diagnosis, headache frequency, MOH and previous pharmacological treatment were extracted from medical charts, which is reliant on the quality of registration by the medial professional. Nevertheless, the responses in the questionnaires and medical charts could be affected by recall bias, and whether the patients fully understood the questions being asked.
Conclusion
Migraine and TTH patients have tried several non-pharmacological treatment options before the first visit to a tertiary headache center. This is in contrast to only one out of six chronic migraine patients having tried at least three triptans. The average headache patient referred to a tertiary headache center had suffered from headache for at least a decade and was severely burdened by headache. There continues to be a need for better education and adherence to clinical guidelines in acute and preventative treatment of both migraine and TTH to shorten the personal and societal burden of headache.
Clinical implications
Before the first visit to a tertiary headache center migraine and tension-type headache patients have tried several non-pharmacological treatments. Before the first visit to a tertiary headache center migraine and tension-type headache patients have tried few acute and preventive treatments. There is a need for better treatment at the primary and secondary care level.
Footnotes
Acknowledgement
The authors greatly acknowledge headache research laboratory technician Merete Bak Bertelsen and headache nurse Janne Jensen for their meticulous work in handling and controlling data from questionnaires and medical charts.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SAM has nothing to declare. LNC has given lectures for Allergan, Lundbeck and Teva, served on scientific advisory board for Lundbeck and received research funding from Rigshospitalet and Helsefonden. RHJ has given lectures for Pfizer, Eli-Lilly, Merck, TEVA, Novartis, Lundbeck and Allergan. Investigator in clinical trials with Eli-Lilly, Novartis and Lundbeck. Director of Danish Headache Center, Lifting the Global Burden of Headache and Founder of Master of Headache Disorders at the University of Copenhagen. Recived research funding from University of Copenhagen, Rigshospitalet, Lundbeck Foundation, The Medical Society in Copenhagen, NovoNordisk Foundation and Tryg Foundation. LB has given lectures and served on the scientific advisory board for Novartis, Allergan, Teva, Lundbeck and Eli Lilly and has received a research grant from Novartis. HWS has given lecturers and received consultation fees from for Lilly, Novartis, Allergan, Lundbeck and TEVA. HWS has received a research grant from Novartis.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.