
Abstract
Background
Erenumab is a monoclonal antibody against calcitonin gene-related peptide receptors, which showed efficacy in migraine attack prevention. The aims of the present pilot study were to i) evaluate the effect of single dose of Erenumab 70 mg on laser evoked potentials from trigeminal and brachial stimulation in a cohort of migraine patients; ii) correlate the neurophysiological changes with clinical outcome after 3 months’ treatment.
Methods
Laser evoked potentials were recorded by 61 electroencephalogram channels before (T0), 1 h (T1) and 7 days after (T2) Erenumab 70 mg injection, stimulating the left and right forehead and the right hand. Laser evoked potential control 1 h after the injection served as placebo session.
Results
Seventeen migraine patients were evaluated. The N1 and N2 component obtained from the right and left trigeminal stimulation diminished in amplitude at T2, compared to T0 and T1 conditions. N2 habituation reduction slightly recovered at T2. Laser evoked potential changes did not correlate with clinical improvement after 3 months of Erenumab treatment.
Conclusions
A single dose of Erenumab has a mild inhibitory effect on cortical responses evoked from trigeminal cutaneous a-delta fibers. Though this phenomenon was not predictive of the clinical outcome, it confirms a wide representation of calcitonin gene-related peptide receptors on trigeminal afferents.
Introduction
Recent studies have highlighted the role of calcitonin gene-related peptide (CGRP) in migraine pathogenesis (1). Monoclonal antibodies against CGRP or CGRP receptors, as well as direct CGRP receptor antagonists, have opened a new era in the migraine scenario (2).
Pivotal studies ascertained that CGRP is the prevalent peptide in sterile inflammation (3) and that efficacy of symptomatic drugs such as triptans is also due to the inhibiting action on CGRP release (4,5). In fact, whatever the migraine initiating event, the activated meningeal unmyelinated fibers produce CGRP, which acts on its receptors and on neighboring terminals of trigeminal afferent myelinated Aδ fibres, leading to sensitisation of these sensory neurons and the following cascade of neurovascular events (1).
Erenumab is a monoclonal antibody against CGRP receptors, which showed efficacy in migraine attacks prevention (6). Recently, it was approved by FDA and Italian AIFA for the preventive treatment of drug-resistant migraine. It acts at peripheral level, inhibiting the a-delta fibres’ CGRP receptors (2). In fact, the action of CGRP monoclonal antibodies seems highly selective for the a-delta peripheral receptors, as they seem not to exert any action on wide dynamic range neurons, largely activated by C and a-beta fibres (6). The CGRP receptors predominate in sensory nerves with cell bodies in the dorsal root ganglion (DRG) and trigeminal ganglion (TG), with a relevant role in peripheral and central sensitisation phenomena (7).
At the moment, further confirmation is needed regarding the effect of CGRP monoclonal antibodies on somatic and trigeminal sensory afferents and how it could impact clinical efficacy.
Laser evoked potentials are a reliable method to explore the function of thin myelinated fibres in the skin. They generate from SII, insula and anterior cingulate (8,9). In migraine, the phenomenon of reduced habituation, which is observed in evoked and reflex responses, involves LEPs recorded during the intercritical and acute phase (10). The late component from the anterior cingulate increases in amplitude during attack, indicating an over-activity of trigeminal nociceptive system (11). Symptomatic drugs and preventive treatments modulate LEP amplitude and habituation (12,13) along with their clinical effect, confirming that the mode of activation of a-delta trigeminal afferents plays a crucial role in migraine pathogenesis. Onabotulinumtoxin-A did not show a direct inhibition of trigeminal LEP, but it restored the pattern of reduced habituation in parallel with the efficacy on migraine frequency (14), confirming the lack of action on a-delta afferents and a modulation of mechanisms of central sensitisation via c-fibre inhibition.
The aims of the present study are i) to evaluate the effect of a single dose of Erenumab 70 mg on laser evoked potentials obtained from trigeminal and brachial stimulation in a group of migraine patients; ii) to correlate the neurophysiological changes with headache frequency, intensity and allodynia after 3 months Erenumab treatment.
Methods
Subjects
The present pilot evaluation was realised within an observational real-life longitudinal multi-centre study on the effects of Erenumab on main migraine features. Migraine patients were selected at the tertiary Headache Center of Applied Neurophysiology and Pain Unit of Bari Policlinico General Hospital from December 2019 to February 2020. According to Italian rules for CGRP monoclonal antibody prescription, selection criteria for Erenumab treatment were: Migraine diagnosis, according to current criteria (migraine with aura, without aura or chronic migraine) (15), more than 4 days with migraine/month in the last 3 months, and demonstrated resistance to at least three preventive drugs, including botulinum toxin, for chronic migraine. The in-course preventive treatment was thus suspended for inefficacy at the time of Erenumab prescription. All the selected chronic migraine patients were taking symptomatic drugs – triptans and NSAIDs – for more than 10 days/month at the time of study inclusion. There were no specific exclusion criteria for Erenumab prescription. The demographic and clinical data of selected patients are detailed in Table 1.
Demographic and clinical data of migraine subjects under monthly erenumab treatment at Month 0 (M0) and Month 3 (M3).
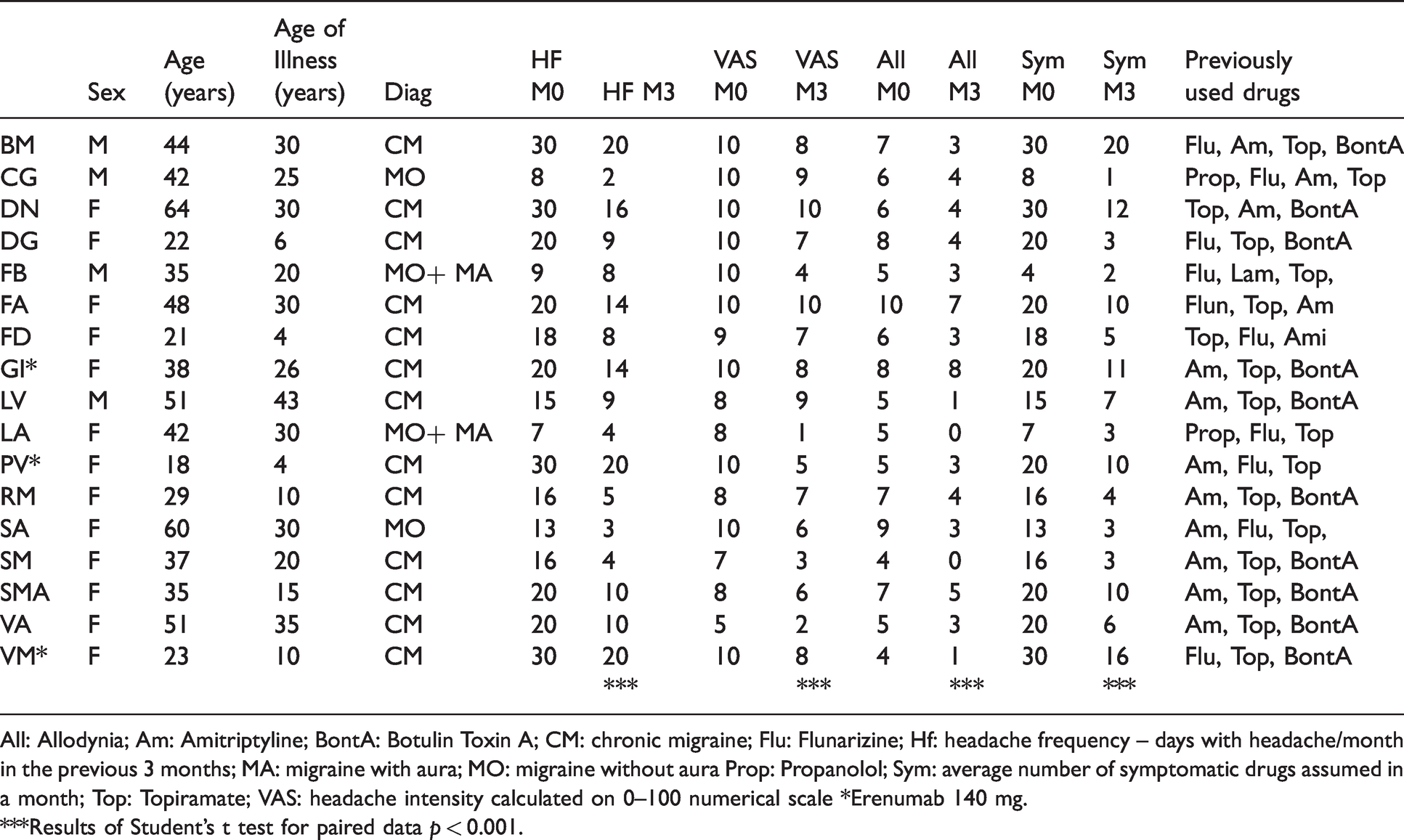
All: Allodynia; Am: Amitriptyline; BontA: Botulin Toxin A; CM: chronic migraine; Flu: Flunarizine; Hf: headache frequency – days with headache/month in the previous 3 months; MA: migraine with aura; MO: migraine without aura Prop: Propanolol; Sym: average number of symptomatic drugs assumed in a month; Top: Topiramate; VAS: headache intensity calculated on 0–100 numerical scale *Erenumab 140 mg.
***Results of Student’s t test for paired data p < 0.001.
All patients filled headache diaries, reporting days with headache, intensity of headache, and presence of allodynia symptoms, as detailed in previous studies (16). Briefly, allodynia was measured using the allodynia questionnaires, including 12 items; intensity of headache was evaluated through a numerical rating scale from 0–10; frequency of headache was the average number of days with headache in a month, calculated over 3 months (16).
Laser evoked potentials
Recording: LEPs were recorded by 61 scalp electrodes. Patients lay on a couch in a warm, semi-darkened room. The recording electrodes were placed on the scalp, referred to the nasion, according to the International 10–20 System. The recording system was a MICROMED EEG apparatus (Micromed Brain Quick, Mogliano Veneto, Italy). Two additional electrodes were positioned above the eyebrows for the electrooculogram. The impedance was kept below 4 KΩ. During the recording sessions, we applied digital filters in the 0.1–70 Hz range and a notch 50 Hz filter to allow signal inspection.
Stimulation: For LEP stimulation, cutaneous heat stimuli were delivered by a CO2 laser (wavelength, 10.6 mm; beam diameter, 2 mm ELEN, Florence, Italy) on the right and left supraorbital zones and right-hand dorsum. The duration of the stimulus was 30 ms. The laser pain threshold (Pth) was established by delivering a series of stimuli at increasing and decreasing intensities using 0.5-W steps. The pain threshold was the lowest intensity that enabled at least 50% of the stimuli to be perceived as a painful pinprick. The laser intensity was two 0.5-W steps over the Pth. We asked all patients to rate the laser pain on a visual analogue scale after each trial of stimulation. In the 0–100 visual analogue scale, the white colour corresponding to 0 indicates no pain sensation and the intense red corresponding to 100 indicates the worst pain conceivable. For each stimulation site and each condition, we delivered one series of 30 laser stimuli, with an inter-series interval of 2 min and an inter-stimulus interval of 10 sec. To avoid damage to the skin, fatigue, or sensitisation of nociceptors, we shifted the irradiated spot after each stimulus.
LEPs analysis: LEP examiners were blinded for the study phases (T0, T1, T2). Preprocessing was performed in MATLAB using the EEGLAB 14_1_1 tool. The data were first high-pass filtered at 1 Hz to remove slow drifts. Next, a notch filter at 50 Hz (L: 48, H: 52) was applied to remove power line noise artifacts. Bad channels were identified by a semi-automatic method based on visual detection and channel statistics. To precompute channel measures, spherical interpolation of missing channels and deletion of Independent Component Analysis (ICA) artifact components related to the electro-oculogram (EOG) was performed. Channels presenting distributions of potential values further away from the Gaussian distribution were also removed. The laser-evoked potentials (LEPs) were precomputed in the time interval of 1000 ms post stimuli using a 70 Hz low-pass filter, removing the baseline and considering the 100 ms preceding the laser stimulus. We used the Letswave tool, version 7. For the computation of habituation, we considered the ratio between the average of the last and the first series of 10 consecutive responses, according to previous studies (third/first) (17).
After single-track visual analysis, the main LEP waves were identified in predetermined time intervals, according to previous studies of our laboratory (N1 face: 100–140 msec; hand: 160–200 msec; N2 face: 170–210 msec; hand: 210–250 msec; P2 face: 290–340 msec; hand: 310–360 msec) (17).
LEP wave amplitudes were thus considered as the average value in the predetermined interval. The N1 was identified on T3 and T4 channels, referred to Fz, the N2 and P2 on Cz channel, referred to the nasion. For LEP latencies, the maximal peak in the predetermined interval was considered.
Experimental procedure
LEPs were recorded before, 1 h and 7 days after Erenumab 70 mg injection (Figure 1). Patients were advised that the action on CGRP receptors could happen soon after drug administration, so LEP control 1 h after the injection served as the placebo session (Figure 1). The original pilot protocol included the LEP control after 3 months’ treatment, but the COVID-19 emergency did not enable this to be accomplished. The local Ethics Committee of Bari Policlinico General Hospital approved the study, and all patients signed an informed consent about the LEPs procedure. After 3 months’ treatment, patients were allowed to come to the Center only for clinical assessment.

Study design.
Statistical analysis
LEPs: The N1, N2 and P2 components’ latency, amplitudes and habituation were compared between the different conditions (T0 before Erenumab, T1 after 1 h and T2 after 7 days from drug administration) using the repeated measures ANOVA included in the SPSS software, version 21.
We also evaluated possible differences between chronic and episodic migraine patients, introducing diagnosis as factor analysis.
To evaluate the possible correlation of neurophysiological changes with clinical outcome, the percent ratio of change of headache frequency, VAS and allodynia after 3 months’ treatment were introduced as covariates in the ANOVA analysis.
For the statistical probability maps (SPMs) of the main LEP waves, we used the statistical analysis included in the Letswave version 7 program, performing a point-by-point ANOVA analysis at 256 Hz resolution, with condition T0 versus T1 versus T2 as within factor. The ANOVA model is corrected for multiple comparisons by Bonferroni test.
Single comparisons between conditions were performed by the same software, using a paired sample two-way t-test, with 0.05 alpha level.
Giving the amount of data of statistical analyses, only the relevant results are reported in detail.
Results
At T0, T1 and T2, all patients were free from migraine for at least 24 h. In two cases, the T2 control was deferred by 1 day, due to the inability of patients to come during critical phase. No patient was lost to clinical follow-up.
Laser evoked potentials
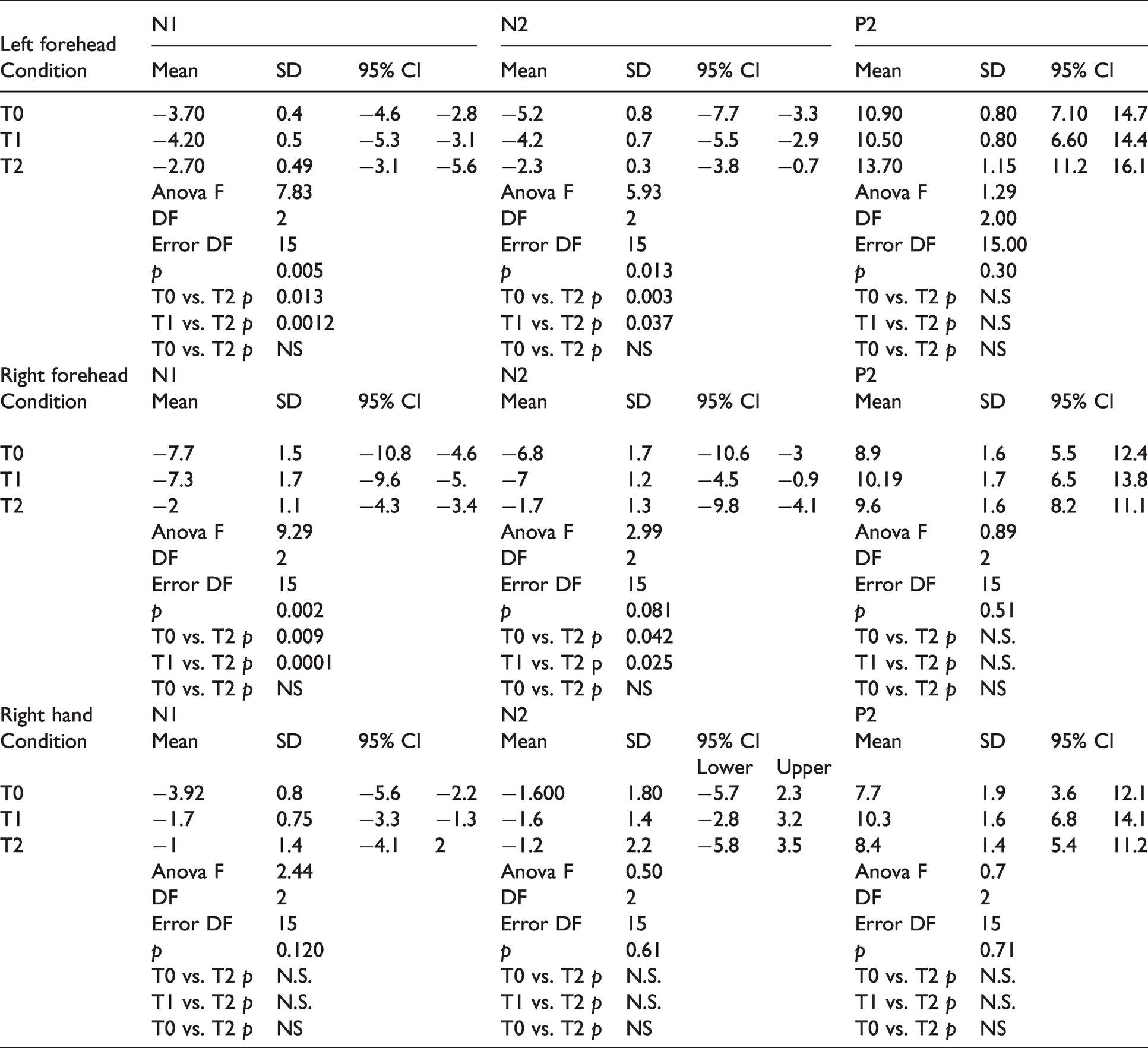
Left forehead: Latency of N1, N2 and P2 components were similar for T0, T1, and T2, as well as subjective perception of laser pain. The amplitude of N1 and N2 waves were significantly smaller in T2, compared to T0 and T1 conditions (Table 2; Figure 2).
Mean, standard errors and 95% confidence interval values of LEP waves amplitude. Data are expressed in microvolts. Results of repeated measures ANOVA with condition as factor and repetitive contrasts are reported.
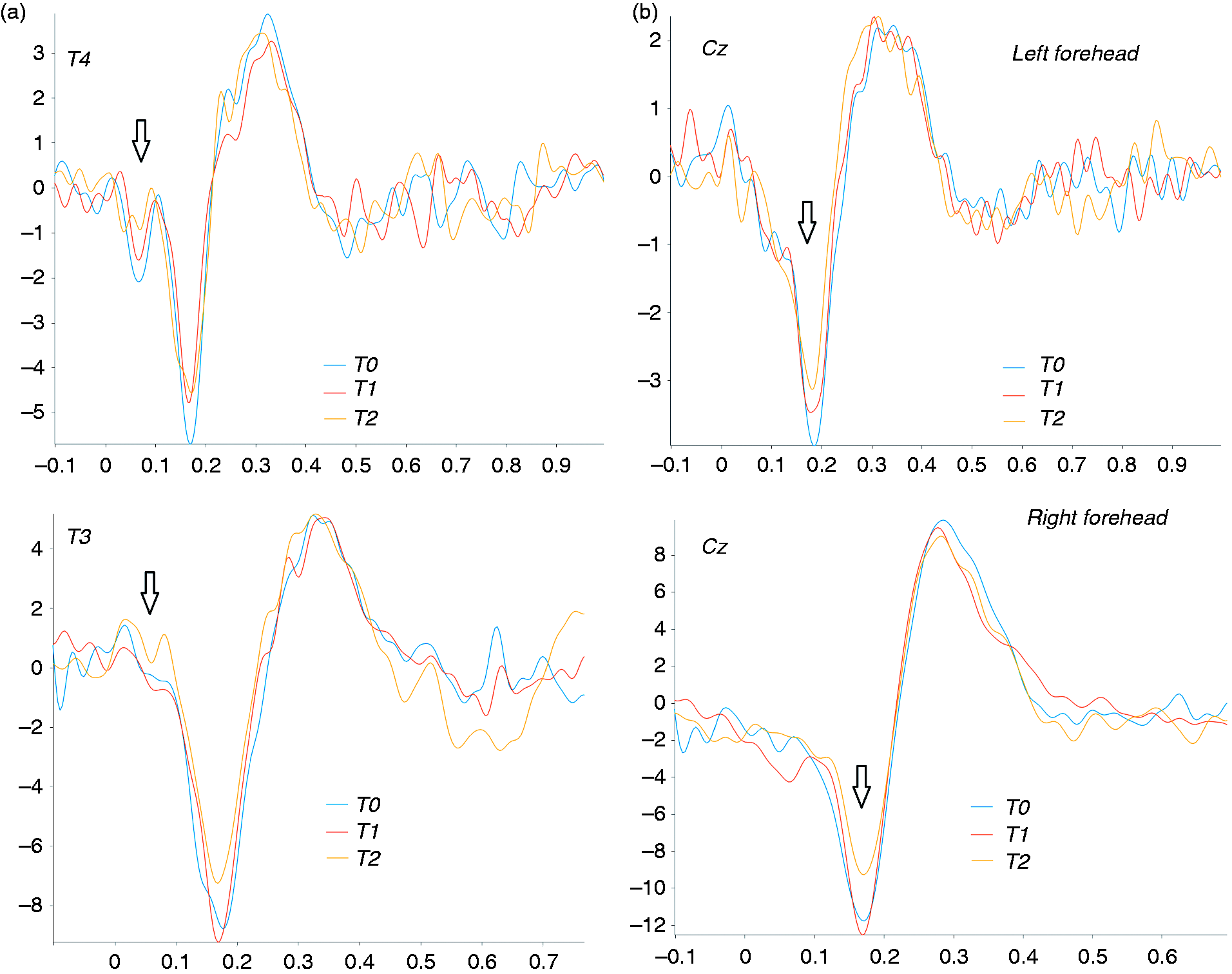
Grand average of laser evoked potentials in 17 migraine patients under Erenumab treatment. (a) N1 responses on temporal electrodes; (b) N2 and P2 responses on central electrodes. Arrows show the relevant amplitude changes.
We did not observe that results differed between chronic and episodic migraine patients (ANOVA with diagnosis as factor: Left N2 F 0.66; p 0.52; left N1 F 1.52; p 0.25)
The P2 wave did not show significant changes between the different conditions (Table 2; Figure 2)
The statistical probability maps reporting results of ANOVA with conditions as factor showed a reduction of N2 scalp representation prevalent over the left temporal and bilateral frontal regions, and of N1 wave over the left central-frontal regions (Figure 3). The t test confirmed a significant amplitude reduction in the T2 condition for the N1 and N2 waves, compared to the basal T0 condition and T1 placebo session (Figure 4, Figure 5). In the T1 condition, a slight increase in the N2 wave emerged in the prefrontal regions (Figure 4).
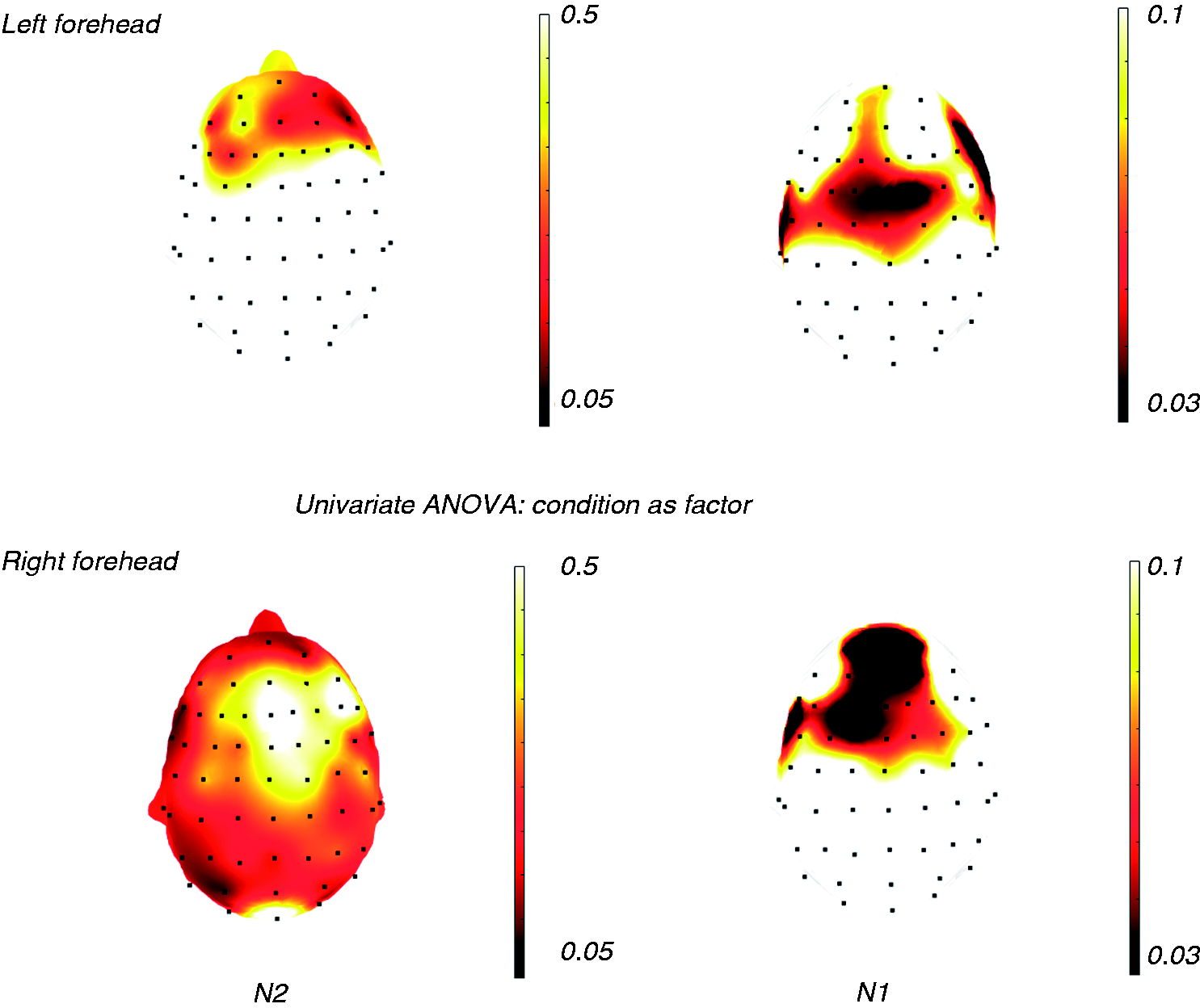
Statistical probability maps (SPMs) reporting p-values obtained from the repeated measures ANOVA between T0, T1 and T2 conditions for the N1 and N2 amplitudes in 17 migraine patients. Black expresses the topographical distribution of statistically significant comparison among the three conditions.
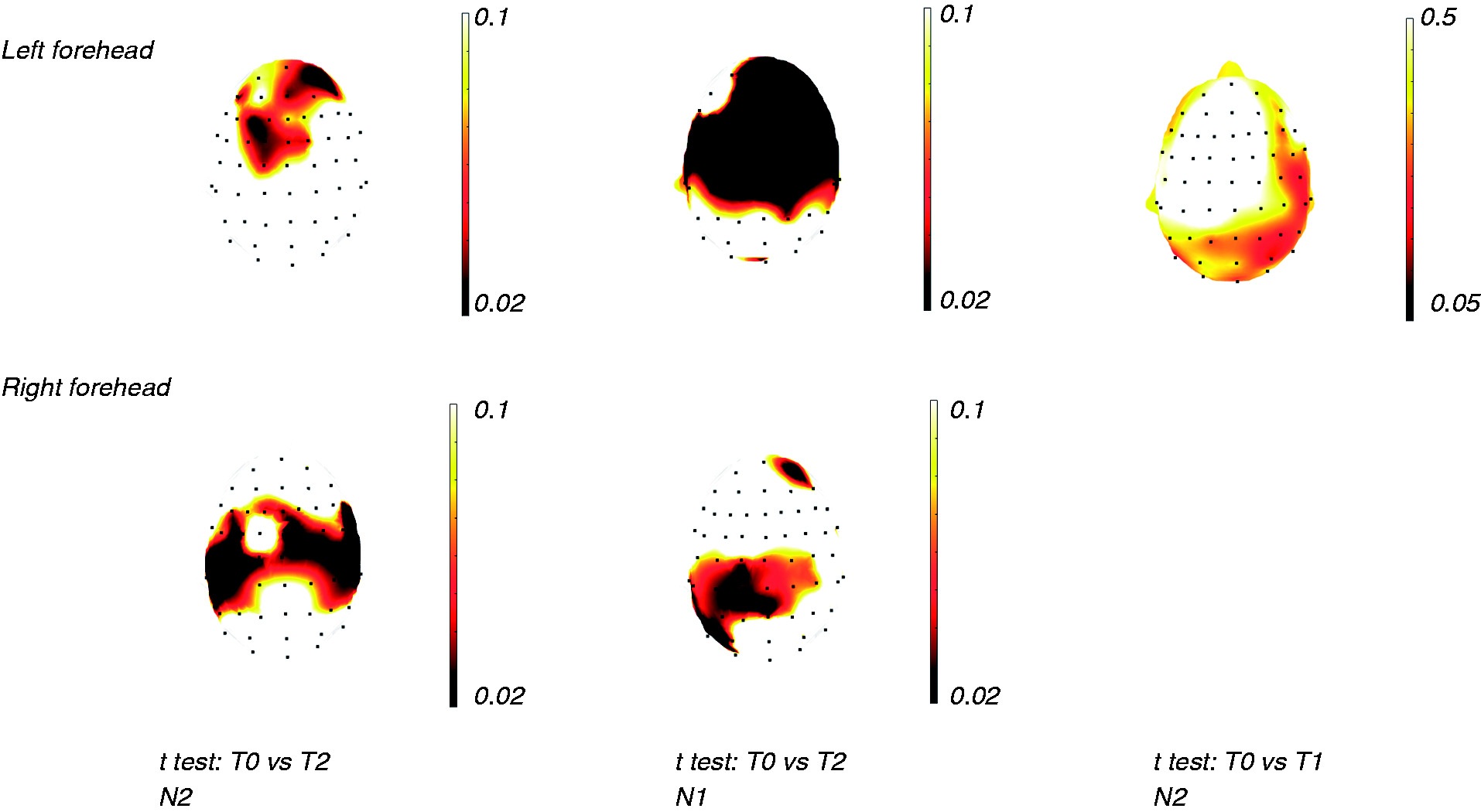
Statistical probability maps (SPMs) reporting p-values obtained from the Student’s t test between T0 and T1 and T2 conditions for the N1 and N2 amplitudes in 17 migraine patients. Black expresses topographical distribution of statistically significant comparison between the conditions.

Statistical probability maps (SPMs) reporting p-values obtained from the Student’s t test between T1 and T2 conditions for the N1 and N2 amplitudes in 17 migraine patients. Black expresses topographical distribution of statistically significant comparison between the conditions.
The N1 Habituation index slightly decreased (e.g. habituation increased) in the T2 condition, compared to the T0 and T1 conditions. The N2 habituation index decreased in the T2 condition, compared to the T0 and T1 conditions (Table 3).
Mean, standard errors (SD) and 95% confidence intervals (CI) of habituation index (the ratio between the average of the first and last series of 10 consecutive responses, 3rd/1st). Higher habituation index corresponded to reduced habituation. Results of repeated measures ANOVA with condition as factor and repetitive contrasts are reported.

Right forehead: Latencies of N1, N2 and P2 components were similar for T0, T1, and T2. The VAS values, expressing subjective pain by laser stimulation, were not significantly different in T0, T1 and T2 conditions. The amplitude of the N1 component diminished at T2, compared to T0 and T1 conditions. For the N2 amplitude, the repeated measures ANOVA approached statistical significance, while the repeated contrasts indicated a significant amplitude reduction at T2 compared to T0 and T1 conditions.
The comparison between chronic and episodic migraine patients was not significant (ANOVA with diagnosis as factor right N2: F 0.68; p 0.52; right N1: F 0.37; p 0.69)
The P2 wave was similar for the different conditions (Table 2; Figure 2)
The SPMs showed a significant decrease of the N1 wave on the left temporal and central frontal regions, and N2 wave on bilateral temporo-parietal regions (Figure 3). The t test confirmed a significant amplitude reduction in the T2 condition for the N1 and N2 waves, compared to the T0 and T1 conditions (Figure 4, Figure 5).
There was a slight decrease of habituation index in the T2 condition for the N1 and N2 waves, which did not reach statistical significance (Table 3).
Right hand: Subjective perception of laser pain, latency, and amplitude of LEPs were similar for all conditions (Table 2). Accordingly, the statistical probability maps did not show relevant changes for different conditions. The habituation index did not change in a relevant way in the different conditions.
Correlation between neurophysiological data and clinical outcomes
In three cases we prescribed Erenumab 140 mg after the first month of treatment, for inefficacy of the 70 mg dose. After 3 months of Erenumab treatment, patients showed a significant improvement in headache frequency, intensity, use of symptomatic drugs, and allodynia (Table 1).
The ANOVA for repeated measures did not show a statistically relevant association between neurophysiological changes and clinical outcome, comparing the N1 and N2 amplitude in T0 and T2 with the percent ratio of change of headache frequency, intensity and allodynia as covariates (Supplementary Table).
Discussion
Results of the present study showed that Erenumab could partially inhibit cortical responses obtained by the stimulation of cutaneous a-delta fibres in migraine patients. This effect is present at trigeminal but not at somatic level and it relates to the first N1 and N2 components; it was not correlated to the clinical efficacy of Erenumab after 3 months’ therapy.
Effects of Erenumab on LEPs
In detail, Erenumab reduced the N1 and N2 components obtained by the stimulation of trigeminal cutaneous a-delta fibres. There is evidence about the representation of CGRP receptors on meningeal and perivascular a-delta terminals (18).
CGRP is localised within the primary afferent terminals, and this distribution is consistent with the role of CGRP as a primary afferent transmitter. Calcitonin gene-related peptide is also found in peripheral fibres innervating the heart, coronary arteries, vascular beds, and myenteric system.[18]
Present results could confirm the presence of CGRP receptors on cutaneous a-delta afferents. In fact, the N1 and N2 waves express the activation of the SII and insular regions, which are the first stations of painful stimuli receptions (8,9,19). The inhibitory effect was partial, as the waves were only reduced in amplitude but not suppressed. The control session was performed after 7–8 days from the drug administration in all cases, according to the drug pharmacokinetics (20), though the maximal response could have inter-individual differences (20). Moreover, the short-term control 1 h after Erenumab administration, which we used as a sham recording session, has no real effect on CGRP receptors (20). The P2 component, which originates from the anterior cingulate, remained substantially unchanged after a single dose of Erenumab. The late positive component expresses the cognitive response toward the salience of painful stimulation (21). In previous studies, we found that this late positive wave increases during a migraine attack (22) and diminishes after acute pharmacological and non-pharmacological treatments, including those without direct action on cutaneous a-delta fibres (10,12,14). We can thus suppose that a single 70 mg dose of Erenumab exerted only a mild inhibitory effect on trigeminal cutaneous a-delta fibres by CGRP receptor blocking. This is reasonable, considering the rich ionic channels and TRP receptor representation on cutaneous thin myelinated afferents (23).
In line with this partial inhibition, the subjective perception of laser pain did not change after 7 days from Erenumab injection.
As described in previous studies, reduced habituation of cortical response to laser stimuli characterises migraine patients (10). Preventive treatments such as topiramate and botulinum toxin A modulate LEPs habituation, though they have no direct inhibitory effect on a-delta fibres (13,14). Erenumab had a mild restorative effect on reduced habituation, with a significant result for the N2 component. The long-term effect of preventive treatments could globally modulate the cortical networks devoted to pain processing. The single dose of Erenumab could have a mild direct inhibitory action on cutaneous afferents, with a minor effect on the dishabituation pattern. The COVID-19 emergency did not permit LEPs to be controlled 3 months after treatment and observe a possible long-term modulation of cortical areas elaborating pain, with a restoration of habituation pattern.
Moreover, the study design lacks a control session in normal subjects. Most patients were affected by chronic migraine, which is characterised by changes in cortical processing of pain and persistent phenomena of peripheral and central sensitisation (24). This can partly explain the mild inhibitory effect on LEP waves and dishabituation phenomena.
The partial inhibitory effect we observed on facial LEPs was absent at somatic level, confirming that Erenumab could preferentially act on cortical responses evoked by trigeminal stimulation. The neuropeptide CGRP is abundant in trigeminal ganglion neurons, and is released from the peripheral nerve and central nerve terminals as well as being secreted within the trigeminal ganglion (18). Present results confirm that the cutaneous a-delta fibres innervating the facial regions could be more furnished with CGRP receptors than those innervating somatic sites (18).
Correlation between neurophysiological and clinical findings
Patients included in the study had a global positive effect on migraine after 3 months’ treatment, though only half could be considered responders for a 50% reduction of headache frequency. The lack of correlation between clinical outcome and LEPs changes after a single dose of Erenumab suggests that the individual sensitivity of cutaneous a-delta fibres’ CGRP receptors is not predictive of the clinical result.
Allodynia, which expresses the sensitisation of trigeminal second-order nociceptive neurons under mechanical and tactile stimulation, improved in almost all patients 3 months after treatment. This effect was not related to the mild inhibition of cutaneous a-delta fibres obtained by Erenumab, which in any case is not directly involved in the allodynia mechanism (25). Further LEPs control 3 months after treatment could clarify if a long-term modulation of CGRP receptors at a cutaneous level may contribute to modulate the firing of caudal nuclei nociceptive neurons and reduce symptoms of central sensitisation.
Study limitations
This was a pilot study realised within the routine clinical examination of patients submitted to Erenumab treatment, so it lacks a control group and placebo randomisation. The low sample size and the heterogeneity of patients was another serious limitation of the study. In fact, the comparison between chronic and episodic migraine was affected by the low patient numbers. In addition, we did not realise the scheduled LEP control after 3 months’ treatment, due to the partial closure of our Center for the Covid-19 emergency. This could be useful to show a long-term modulation of CGRP receptors and cortical responses from cutaneous a-delta fibre stimulation.
Other problems were the inclusion of episodic and chronic migraine patients, and the small case series, both due to the limited availability of the drug at the time of study design.
Conclusions
We found that a single dose of Erenumab has a mild inhibitory effect on cortical responses evoked from trigeminal cutaneous a-delta fibres. Though this phenomenon was not predictive of the clinical outcome, it confirms a wide representation of CGRP receptors on trigeminal afferents. The possible relevance of long-term modulation exerted by monoclonal antibodies on cutaneous afferents may be worthy of further exploration.
Clinical implications
Erenumab inhibited cortical responses evoked by cutaneous a-delta fibre stimulation in migraine patients. This mild inhibition was present only in the trigeminal district. The short term modulation of cutaneous a-delta fibers did not correlate with clinical efficacy.
Supplemental Material
sj-pdf-1-cep-10.1177_0333102421996345 - Supplemental material for Effect of single dose Erenumab on cortical responses evoked by cutaneous a-delta fibers: A pilot study in migraine patients
Supplemental material, sj-pdf-1-cep-10.1177_0333102421996345 for Effect of single dose Erenumab on cortical responses evoked by cutaneous a-delta fibers: A pilot study in migraine patients by Marina de Tommaso, Marianna Delussi, Eleonora Gentile, Katia Ricci, Silvia Giovanna Quitadamo and Giuseppe Libro in Cephalalgia
Footnotes
Author contributions
MDT: study design and coordination, manuscript preparation; MD: patient assessment, manuscript editing; EG: patient assessment, data analysis; KR: LEP recording and analysis; SGQ: patient assessment, LEP recording and analysis; GL: study coordination, clinical assessment.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.