
Abstract
Background
Hypertension and headache disorders are major contributors to public ill health, linked by a long-standing but questionable belief that hypertension is a conspicuous cause of headache. In Nepal, where hypertension is common and often untreated, we assessed the substance of this belief, hypothesising that, should hypertension be a significant cause of headache, a clear positive association between these disorders would exist.
Methods
In a cross-sectional, nationwide study, trained health workers conducted face-to-face structured interviews, during unannounced home visits, with a representative sample of the Nepalese adult population (18–65 years). They applied standard diagnostic criteria for headache disorders and measured blood pressure digitally. Hypertension was defined as systolic pressure ≥140 and/or diastolic ≥90 mm Hg.
Results
Of 2,100 participants (59.0% female, mean age 36.4 ± 12.8 years), 317 (15.1%) had hypertension (41.0% female) and 1,794 (85.4%) had headache (61.6% female; 728 migraine, 863 tension-type headache, 161 headache on ≥15 days/month [mutually exclusive diagnoses]; 42 unclassified headaches).
All headache collectively was less prevalent among hypertension cases (78.9%) than non-cases (86.6%; p = 0.001). A negative association between hypertension and all headache was demonstrated in bivariate analysis (odds ratio: 0.6 [95% Confidence interval: 0.4–0.8]; p < 0.001), but did not maintain significance in multivariate regression analysis (adjusted odds ratio: 0.8 [95% Confidence interval: 0.5–1.1]; p = 0.09). The findings were reflected, without significance, in each headache type.
Conclusions
If any association exists between hypertension and headache disorders, it is negative. From the public-health perspective, headache disorders and hypertension are unrelated entities: they need distinct policies and programs for prevention, control and management.
Background
Hypertension (HTN) and headache disorders are both recognized as major public-health concerns all over the world, no less so in low- and middle-income (LAMI) countries, where both are less likely to be treated (1–3). HTN is an important risk factor for stroke and cardiovascular diseases (4). The Global Burden of Disease study 2017 (GBD2017) estimated that high systolic blood pressure (SBP) was responsible for 10.4 million deaths globally (95% uncertainty interval [UI]: 9.39–11.5 million) and 218 million disability-adjusted life years (DALYs) (95% UI: 198–237 million) (5). Active headache disorders affect around half of the world’s adult population (6). In GBD2017, headache disorders were ranked the second leading cause of disability worldwide (7). GBD2015 had earlier noted that tension-type headache (TTH) was the second and migraine the fifth most prevalent disorders worldwide (8). GBD2019 reported migraine as the second highest cause of disability among specific disorders and, most importantly, first highest in adults aged under 50 years, the most economically active group (9,10).
There has been a persistent belief, commonly expressed in countries where HTN is poorly diagnosed and treated, that HTN is an important cause of headache. This belief is questionable. Evidence behind it is somewhat conflicting (11–13): several population-based epidemiological studies have found no correlation (14–17) or even negative associations between these two disorders (18,19).
Nepal is in the South-East Asia Region (SEAR), with a population of approximately 30 million. About one quarter live below the international poverty line (20), establishing it as one of the poorest countries in this Region. In two nationwide epidemiological studies conducted in the same year, the prevalence of HTN and of uncontrolled HTN (treated or untreated) were 26.0% (21) and 15.1% (22) respectively, findings that clearly demonstrated not only the size of the problem in Nepal but also the unmet need for treatment (more than half of cases). Our population-based study in this country found the 1-year prevalence of migraine was exceptionally high (34.1%), while of TTH (41.5%) it was close to the global mean (6). The group of headache disorders characterized by headache on ≥15 days/month (d/m) were also common (7.4%) (23). Headache-attributed burden was accordingly high (24), but coverage and quality of headache-care services were very poor (25).
The objective of this study was to assess the associations in Nepal between HTN and headache disorders (any headache, migraine, TTH and headache occurring on ≥15 d/m), using data on each from the same survey. The primary purpose, having global relevance, was to contribute to the debate regarding HTN as a putative cause of headache. For this purpose we hypothesised that, should HTN be a significant cause of headache, a clear positive association between these disorders would necessarily exist and be demonstrable. A secondary but important purpose was to provide evidence for decision makers and health-care providers for formulation of public-health policy in relation to the prevention, control and management of HTN and of headache disorders in Nepal.
The study was a project within the Global Campaign against Headache.
Methods
Ethics
Nepal Health Research Council, the Institutional Review Committee of Kathmandu University School of Medical Sciences, Dhulikhel Hospital, and the Regional Committee for Health and Research Ethics in Central Norway approved the study protocol.
We informed all participants of the nature, procedures and purposes of the study. All participants gave consent.
Study design, sampling and data collection
We conducted a nationwide epidemiological survey in Nepal during May 2013, the methods of which have been published in detail elsewhere (26,27). In brief, it was a cross-sectional, population-based study employing multistage random cluster sampling to select individual households. To ensure national representativeness, 15 of the 75 districts in the country were sampled, one from each of the three physiographic divisions (Mountain, Hill and Terai) in each of the five development regions (Far-Western, Mid-Western, Western, Central and Eastern) of Nepal (26). Trained health workers made unannounced visits to each of these households, listing the eligible occupants (adults aged 18–65 years), randomly selecting one and conducting a face-to-face structured interview with that person (returning by appointment if he or she was not initially present) (26).
Instrument
Interviewers used the Headache-Attributed Restriction, Disability, Social Handicap and Impaired Participation (HARDSHIP) modular structured questionnaire developed by Lifting The Burden (LTB) for population-based studies (28). This was culturally adapted, and translated into Nepali language according to LTB’s translation protocol for hybrid documents (29). The questionnaire begins with demographic enquiry, followed by a neutral headache screening question (“Have you had a headache during the last 12 months?”), addressed to all participants. Those who answered the screening question positively were asked diagnostic questions based on the International Classification of Headache Disorders (ICHD) (30), which focused on the subjectively most bothersome headache type in those reporting more than one type.
Headache diagnosis
Diagnoses of the different headache disorders were mutually exclusive. The diagnostic method has been described previously (23). Participants reporting headache on ≥15 d/m were first separated; for the purposes of this study, they were not further diagnosed. For those reporting headache on <15 d/m, we used the HARDSHIP algorithm (28) based on modified ICHD-3 beta criteria (30) in the following sequence: definite migraine, definite TTH, probable migraine and probable TTH. Definite and probable migraine were combined, and likewise definite and probable TTH, for further analyses. The few remaining cases were unclassifiable.
Blood pressure (BP) measurement and definition of hypertension caseness
Interviewers took two BP readings from the right arm of each participant, with a rest in between, using a digital device (Microlife 3BM1-3, Microlife Corporation, Taipei, Taiwan). Since chairs were not available in most of the households, for consistency of measurement we took all readings from participants seated on the floor. When either reading was ≥140/90 mm Hg, the measurement was repeated after a further two minutes of rest.
The average of these measurements was calculated: SBP ≥140 and/or diastolic BP (DBP) ≥90 mm Hg were considered to indicate HTN caseness; readings below were considered normotensive (HTN non-caseness) (31).
Data analysis
We estimated 1-year prevalences with 95% confidence intervals (CIs) of any headache, headache occurring on ≥15 d/m, migraine and TTH among participants with and without HTN (cases and non-cases). Since household altitude and gender were associated with headache (23,32), and gender with HTN (22), we further analysed headache prevalences among HTN cases and non-cases by household altitude (categorized into two groups: <1,000 m and ≥1,000 m) and by gender.
We used chi-squared to test differences in headache prevalences between HTN cases and non-cases. We used bivariate and multivariate logistic regressions to evaluate associations between headache disorders and HTN, calculating odds ratios (ORs) and adjusted ORs (AORs) respectively, each with 95% CIs. We took HTN as the independent variable in regression analyses and headache disorders (any headache, headache on ≥15 d/m, migraine or TTH) as dependent variables. We entered the following, previously found to have actual or potential influence on the prevalence of headache or HTN (22,23,32), as covariates in the multivariate logistic regression analyses: demographic variables (age in years [continuous variable], gender [male or female], habitation [urban or rural], household consumption [in USD/year (at the time of the study, 1 USD ≈ NPR 100) categorized into poorest (<USD 950), poor (USD 950–1,200) and intermediate or above (>USD 1,200)] and household altitude [categorized as above]), and also the Eysenck personality questionnaire revised short form-Neuroticism (EPQRS–N) and hospital anxiety and depression scale (HADS) scores (continuous variables).
We analysed all data using Statistical Package for Social Sciences (SPSS) 21.0 software (IBM Corp, Armonk, NY, USA). We considered p < 0.05 to be statistically significant.
Results
Of 2,109 selected respondents, nine (0.4%) refused and 2,100 completed the survey (male: 861 [41.0%]; female: 1,239 [59.0%]; mean age: 36.4 ± 12.8 years). More than half (1,100: 52.9%) were from households at altitudes ≥1000 m.
Of the participants, 317 (15.1%) were HTN cases (male: 187 [59.0%]; female: 130 [41.0%]; mean age 44.1±12.9 years). Again, more than half of these (180: 56.8%) were from households at ≥1,000 m. The remaining 1,783 (84.9%) were HTN non-cases (male: 674 [37.8%]; female: 1,109 [62.2%]; mean age 35.1±12.2 years; 920 [51.6%] from households at ≥1000 m).
There were 1,794 participants (85.4%) with any headache (male: 689 [38.4%]; female: 1,105 [61.6%]). Of these, 728 had migraine, 863 had TTH and 161 reported headache on ≥15 d/m. The 42 unclassifiable cases were included among those with any headache but not further analysed.
Headache prevalences by hypertension caseness
The estimated 1-year prevalences of any headache, headache on ≥15 d/m, migraine and TTH in participants with and without HTN are presented in Table 1 and Figure 1. Participants with HTN appeared less likely to have any headache and each type of headache, although the difference was significant only for any headache (p = 0.001).
One-year headache prevalences by hypertension (HTN) caseness.

CI: confidence interval; p*: chi-squared test; † including 42 unclassifiable.

One-year headache prevalences by hypertension (HTN) caseness (proportions, with 95% confidence intervals).
In the stratified analyses by gender and altitude, headache prevalences in most groups were lower among HTN cases than among non-cases (Table 2). However, in a few, prevalences were numerically slightly higher among cases (migraine in females, and at altitude <1,000 m, TTH at <1,000 m and headache on ≥15 d/m in females). None of these differences were significant (95% CIs overlapping) (Table 2).
One-year headache prevalences by hypertension (HTN) caseness, age and household altitude.

CI: confidence interval; * including 42 unclassifiable.
Associations between headache disorders and hypertension
We found a negative association between HTN and any headache in bivariate analysis (OR 0.6 [95% CI: 0.4–0.8]; p < 0.001). This did not quite survive in multivariate logistic regression analyses adjusting for variables that might be influential (particularly altitude and gender, both associated with headache (23,32) and with HTN (22)) (AOR: 0.8 [95% CI: 0.5–1.1]; p = 0.09; Table 3). No associations were found between HTN and any specific headache type (Table 3).
Associations between headache by type and hypertension (HTN).
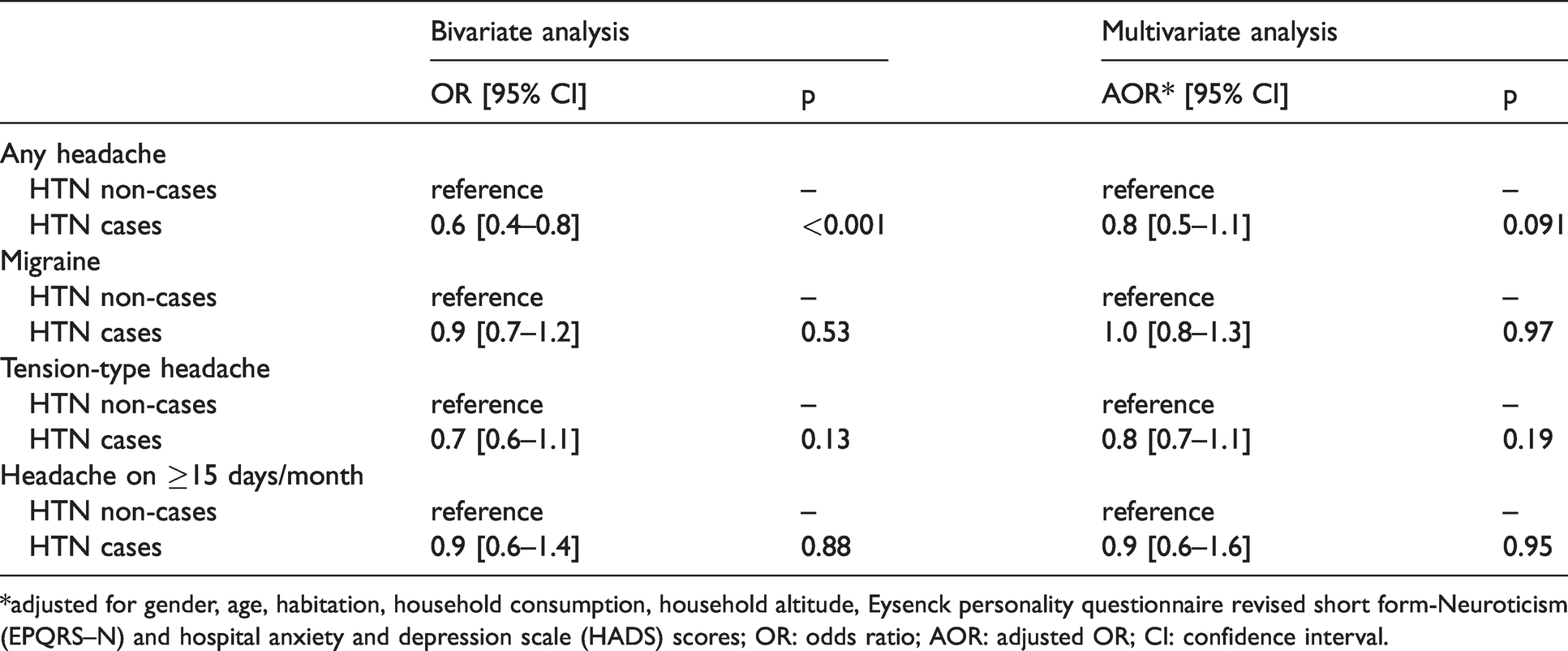
*adjusted for gender, age, habitation, household consumption, household altitude, Eysenck personality questionnaire revised short form-Neuroticism (EPQRS–N) and hospital anxiety and depression scale (HADS) scores; OR: odds ratio; AOR: adjusted OR; CI: confidence interval.
Discussion
As we noted earlier, HTN and headache disorders are both highly prevalent and burdensome in Nepal, but undertreated (22,23). The additional analyses here focus on the associations between them. We found that all headache collectively was less prevalent among HTN cases than non-cases (p = 0.001). This was reflected in each headache type, but without significance. An inverse association between HTN and any headache in bivariate analyses was not confirmed in the multivariate analyses adjusting, especially, for gender.
Earlier findings on associations between HTN and primary headache disorders, from clinical and population-based studies, are conflicting and inconclusive (11–19,33–36). The findings of our study contrast with those of several that have found mostly positive associations between HTN and headache prevalence (11,33–36). Variations in methodology have certainly influenced findings, making comparisons difficult (37). Most of these previous studies were performed in clinical settings, and some drew conclusions without using multivariate analyses to control possible confounders (33,35). We need, therefore, to interpret the findings of these with care and circumspection. Studies based on patient samples are highly subject to selection bias (so-called Berkson’s bias (38,39)). As noted, both headache and HTN are highly prevalent diseases, but far from all patients with either one of them seek hospital treatment; they are rather more likely to do so if they have both (34). Associations appearing in clinic-based studies, therefore, may well be spurious. A study in an emergency department, while finding an association between HTN and headache, also noted that improvement in headache was not associated with improvement in BP, and vice versa (36). There is a common consensus within the Classification Committee of the International Headache Society (IHS) that chronic arterial HTN of mild to moderate degree does not cause headache. This might not be true of severe HTN (30,40); indeed, ICHD criteria for headache attributed to arterial hypertension require pressures of at least 180 (systolic) or 120 mmHg (diastolic). We did not investigate this.
In our view, the association between HTN and headache disorders can be confirmed only if observed systematically in a well-designed population-based study. Findings of our study are consistent with those of other such epidemiological studies (14–19). Most of these demonstrated no positive association between HTN and headache disorders (14–17), while a few found HTN cases were less likely to have headache, especially non-migraine headache, than HTN non-cases (18,19). A negative relationship could be explained by the higher probability of receiving headache treatment among HTN cases than non-cases, because of greater likelihood of contact with health-care services. In Nepal, where most HTN is untreated (25), this is an improbable explanation. In Norway, where statistically negative associations between HTN and any headache and between HTN and TTH have been documented both in cross-sectional and in prospective longitudinal population-based studies (18,19), this explanation seems improbable for the opposite reason: HTN and headache are rather well treated in available and affordable health-care services. Rather, the Norwegian authors invoked the well-known phenomenon of hypertension-associated hypalgesia (41). The HUNT studies in Norway have shown inverse relationships between BP and most other bodily pains (42), while, for headache, the inverse relationship was not only evident with BPs well within the normal range (i.e., not indicative of HTN) but also demonstrable among adolescents (43).
Whether or not the proposition of a negative association is true, our findings taken with those of other studies (14–17) establish clearly the lack of a positive association, even when HTN is largely untreated. This should put to rest the long-standing but always questionable belief that HTN is among the important causes of headache, since if it were so then a clear and positive association would necessarily exist. This has implications of consequence for public health and health policy in many countries other than Nepal. Where this mistaken belief persists, as it does in many LAMI countries, likely consequences are that headache is misdiagnosed, appropriate and generally effective treatments are not initiated, resources are misdirected (and potentially wasted) and remediable headache-attributed burden remains unmitigated. On the other hand, it is no bad thing if a complaint of troublesome headache encourages screening for HTN (as it should for anxiety, which is highly comorbid (44)), since HTN is often undetected but should not be.
Strengths and limitations
This was the first nationwide population-based study in any country of SEAR to enquire into any association between HTN and headache disorders. The epidemiological study on which the enquiry was based included a large and representative sample of the general adult population of Nepal, with a very high participation proportion (>99%) effectively excluding participation bias (22–26). The careful face-to-face interviews ensured there were no missing data. The use of the standard HARDSHIP questionnaire, already validated in many countries and cultures (28), enhanced the validity of results. These were considerable strengths.
Measurement of BP at least twice by trained health workers following a standard protocol was a careful approach, constrained by practicality, to recognising HTN caseness. It did not comply with the many standard guidelines on diagnosing HTN, which require multiple measurements on different occasions, but it was not our purpose to identify need for treatment. While we noted whether HTN was treated or not, we could not collect data on the antihypertensive drugs being used (22). Therefore, no judgement was possible of treatment appropriateness, but this was not an important limitation with regard to our purpose.
It is a well-recognized limitation of cross-sectional studies that no inferences can be drawn as to causation should a positive association be found. The inverse is not true. If no association is demonstrated, or any association tends towards the negative, which was the essence of our findings, there is nothing upon which a proposition of causation can be mounted.
Conclusions
If any association exists between HTN and headache disorders (any headache, headache on ≥15 d/m, migraine or TTH), it is negative.
Public health relevance
No evidence exists that hypertension (even untreated) is a significant cause of headache; health-care policy and provision should not be misled by belief to the contrary. Headache disorders and hypertension are unrelated entities requiring distinct policies for prevention, control and management. This does not, and should not, exclude horizontal integration of services, since both disorders should be managed mostly in primary care.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: TJS is a Director and Trustee of Lifting The Burden. Otherwise, all authors declare no competing interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research project was financed by grants from Samarbeidsorganet, the Liaison Committee between the Central Norway Regional Health Authority and the Norwegian University of Science and Technology.
It was conducted within the Global Campaign against Headache, led by the nongovernmental organization Lifting The Burden in official relations with the World Health Organization, and with the support of Dhulikhel Hospital, Kathmandu University Hospital, Dhulikhel, Kavre, Nepal.
Authors’ contributions
All authors contributed to conception and design of the study and to acquisition of data. KM and TJS analysed and interpreted the data. KM drafted the manuscript. All other authors revised it critically for intellectual content, and approved the version submitted.
Data availability
The data are held on file at Norwegian University of Science and Technology (NTNU). Once analysis and publications are completed, they will be freely available for non-commercial purposes to any person requesting access in accordance with the general policy of the Global Campaign against Headache.