
Abstract
Background
Preparations for the Global Campaign Against Headache done jointly with WHO started almost 25 years ago. It was officially incorporated 18 years ago. It is the story of a few dedicated individuals who, together with the World Health Organization, generated epidemiological data all over the world and made use of these data to gradually increase the position of headache disorders, until migraine became number two among all causes of years lost to disability. It is also the story of impressive development of scientific tools, their validation and use in low-income countries.
Methods
Models of care for headache patients were developed that are adaptable and hence can be implemented in future throughout the world.
Results
The last phase of the campaign shall use the impressive data set generated to cause real improvement in the healthcare for people with headache throughout the world. The recent World Health Organization initiative: Intersectoral Global Action Plan on Epilepsy and Other Neurological Disorders invites international organizations to collaborate, and headache is mentioned.
Conclusion
This calls for the International Headache Society and all its national members and all other organizations involved in headache to work together with Lifting the Burden, the organization in charge of the Global Campaign Against Headache.
Introduction
Most readers of Cephalalgia have written a scientific paper recently and many have written grant applications. Likely you have argued that migraine and other headaches are worthwhile research areas because they are very prevalent and disabling. You have probably specified that migraine affects one billion persons worldwide and that it is the second biggest cause of years lost to disability. The fact that such strong statements can be made is the best way of proactively avoid prejudice against headache from reviewers of scientific manuscripts and grant applications, but what is the history behind these statements? How did it come about that today migraine and other headaches cannot be disregarded by editors, reviewers, granting bodies and decision makers in health care? This is the story of the Global Campaign Against Headache (GCH), conducted under the auspices of the independent organization Lifting The Burden (LTB) (1).
The idea of the Global Campaign Against Headache and its formation
The idea of the Global Campaign Against Headache (GCH) originated after a long meeting at the World Health Organization (WHO). At this and previous meetings information was given about the Global Campaign Against Epilepsy (2). The success of this campaign made it clear that collaboration with WHO about the prevalence, burden and care of headache diseases would be immensely beneficial. The WHO could not allocate resources to such an initiative, but it had useful experience with the Global Campaign Against Epilepsy and other health campaigns, it had offices in all regions of the world, and it had direct access to World ministries of health. The International Headache Congresses are held every other year on uneven years, but Timothy Steiner and others planned a special additional congress: The Millennium Meeting on Headache (Headache World 2000) in London. This was still the heydays of triptans, and it could be expected that such a meeting would generate a considerable surplus. Steiner gained support from many quarters that the surplus from the Headache World 2000 should be used to promote a Global Campaign Against Headache. The meeting fulfilled expectations and a financial basis for the future campaign was established. Then there was a long struggle to get the campaign accepted by WHO. It involved collection of all available epidemiological information and delivery of this information to the Global Burden of Disease (GBD) study of the WHO. As a result of persistent advocacy this information was included in the GBD 2000 Study and in the World Health Report (3). For the first time migraine was accepted and rated number 19 amongst all diseases causing disability. The GCH was endorsed by the International Headache Society (IHS), European Headache Federation (EHF), British Association for the Study of Headache (BASH) and World Headache Alliance (WHA). Together with WHO they signed a memorandum of understanding in 2003. Thus, the WHO was a full and formal partner in the initiative.
Early years of the campaign
The creation of the campaign, its acceptance by WHO and sponsorship by all major non-governmental organizations were major feats. The only other disease with such a campaign was epilepsy with its powerful support from the International League Against Epilepsy (2). Information about the GCH had to be spread widely to those studying headache and those caring for headache patients. The first papers describing the initiative were published in 2004 (4) and 2005 (5). In accordance with other initiatives of the WHO, the campaign was conceived in three stages (Table 1).
The 3 stages of the Global Campaign Against Headache as originally conceived (reproduced from Steiner et al. (1) with permission). The first 2 stages are virtually complete by now, but the third stage requires considerable effort to be successful. It requires close collaboration with IHS and other headache organizations.
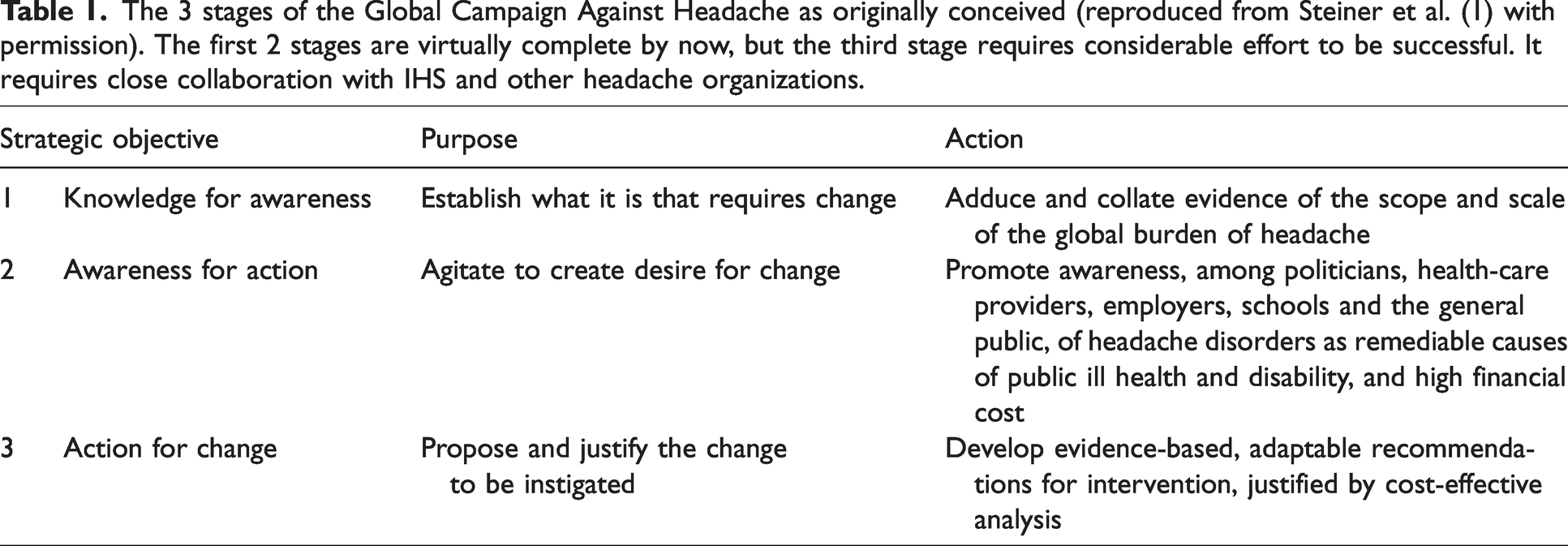
The first stage was “Knowledge for Awareness” meaning generating epidemiological evidence. The general belief that headache is a health problem of industrialized high-income countries had to be disproven. The next stage was “Awareness for Action” meaning that the evidence collected during the first stage should be used to enlighten ministries of health, hospital directors, chairpeople of foundations, colleagues and the general public about the size of the problem and the possibilities for its treatment. The last stage of the campaign would focus on “Action for Change” using all the evidence collected and the awareness created in the second phase to cause real action in terms of better education in headache, more research and better care for headache patients worldwide. These were extremely ambitious plans requiring major effort. Epidemiological methodology had to be developed with standard protocols to be followed all over the world. They were field tested, later refined and put to world-wide use (6,7). A simple model of headache care including a main emphasis on primary care was promoted (8) (Figure 1).

A simple model of headache care with 3 levels which also includes an estimated caseload at the different levels. Reproduced with permission from Steiner et al. (8).
At the same time work started on the second phase using the significant amounts of data already available and new data as they were pouring in. Many publications resulted from collaboration with the WHO. They described the epidemiology, burden, and insufficient care of headache diseases. They had WHO's official stamp with the implication that national health authorities had to take them seriously.
Although the campaign at this point was extremely successful it ran into organizational problems. It was necessary to create an independent international organization called Lifting the Burden (LTB) incorporated under English law to partner with WHO. In 2011 LTB gained official relation with WHO, something that is very difficult and often takes many years (9).
Knowledge for awareness
Knowledge about the prevalence and impact of headache disorders was absent for at least half of the world's population before the global campaign amended this (10,11). Incredible effort went into developing the methodology for epidemiological studies in low income countries (6) and to complete around 60 such studies. Thus, data became available from every region of the world. All these studies have been recently summarized (1). Here we shall just mention that studies have been completed in Ethiopia, Zambia, Benin, Cameroon, Mali, Malawi, Brazil, Peru, Pakistan, Saudi-Arabia, Morocco, Georgia, Lithuania, Russia, India, South Nepal, India North, China (six studies) and Mongolia. Together with the Eurolight project studies have been conducted in eight countries of western Europe (12). Studies in children and adolescents began later with the development and testing of new methodologies (13). So far data collection has been completed in Austria, Ethiopia, Lithuania, Turkey, Benin, Iran, Mongolia, Serbia and Zambia and many more are planned or have already commenced. The results are of immense importance because these studies have provided the data behind recent GBD studies. Thus, in GBD 2019 migraine is number two out of all diseases causing disability, and tension-type headache is also high on the list (14). These are the data that we all cite in our papers and grant applications. The epidemiological studies have also had another positive effect. They have involved neurologists in many countries where little neurological research was previously conducted at an international level. Doctors in many countries have learned from using the technology developed by the global campaign in their epidemiological studies.
Awareness for action
All disease related organizations advocate for “their” disease. The public scene is bombarded with data claiming that this and that disease is extremely important. How and why was the global campaign successful in getting its huge epidemiological data sets accepted by decision makers? The answer is of course the high quality of the data and the close collaboration with WHO and in later years with the GBD study conducted by the Institute for Health Metrics and Evaluation (IHME) at the University of Washington, Seattle, USA.
Some activities relating to Awareness for Action have already been described above because the global campaign decided to use all new data as soon as they became available to influence decision makers. The main activity has been joint initiatives with the WHO such at the Atlas of Headache Disorders (15). The continued presentation of new data to the organization behind the GBD studies (IHME) is another important activity. Medication overuse headache was for example included in GBD 2013 as the 18th highest cause of disability (16). Later it was decided to include MOH as a sequela of migraine (73%) and TTH (27%). Its considerable burden is thus still included in GBD publications but under migraine and tension-type headache. WHO distributed information directly to the world's ministries of health about headache as a major cause of public ill health and pointed out inadequacies in its management throughout the world. Finally, the many epidemiological studies have made it clear to leading neurologists throughout the world that headache disorders are of immense importance and the size of the unfulfilled need for treatment is enormous. Such professional understanding spreads to many decision makers, particularly in low- and middle-income countries. An updated version of the Headache Atlas is urgently needed and there is a big need for continued use of the already produced evidence in advocacy in every country. Here support from the professional headache societies would be very helpful.
Action for change
With all necessary epidemiological data secured and having already influenced WHO, IHME and many governments in a positive direction, the global campaign presently wants to improve healthcare for people with headache throughout the world. GCH developed a model of structured headache services based on primary healthcare but including a second tier at specialist level as well as a highly specialized tier of tertiary headache referral centers (Figure 2).This would be impossible for the IHS to do because it receives support from the pharma industry while LTB does not.

The most recent model of care for headache patients which is the one to be promoted in the third stage of the Global Campaign Against Headache. It includes educational initiatives and service structure and organization. It can be adapted to the situation in the many different countries of the world. It does not include research activities, but these are a natural element to be promoted by the campaign. Reproduced with permission from Steiner et al. (1).
The model can be adapted to fit all countries in the world using sufficient simplification in countries with low income. It is now crucial to show cost-effectiveness of organized headache care. Some studies have already been conducted but much more needs to be done. These studies are, however, costly, and long-lasting and funding is difficult. This would be an obvious project for headache organizations to take on in collaboration with LTB.
The Global Campaign has calculated the necessary manpower to be allocated to headache care at the three different tiers (Table 2). At first glance these requested resources per million inhabitants are very modest compared to the resources spent in high-income countries like Denmark, but due to the enormous prevalence of headache diseases the combined requirement for healthcare according to the table is considerable and unfulfilled in most countries.
Estimated service requirements to meet headache-related health-care demand in a population of 1 million (based on assumptions in Steiner et al. (8). Structured headache services as the solution to the ill-health burden of headache: 1. Rationale and description.
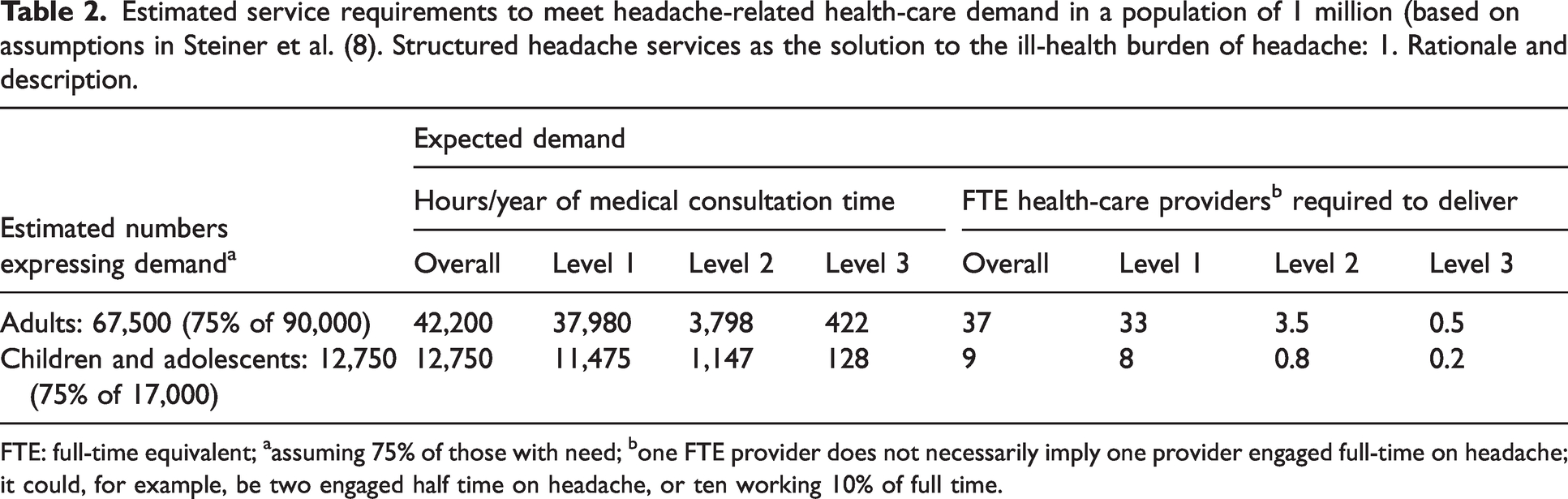
FTE: full-time equivalent; aassuming 75% of those with need; bone FTE provider does not necessarily imply one provider engaged full-time on headache; it could, for example, be two engaged half time on headache, or ten working 10% of full time.
The future
The global campaign has managed the first two stages of its activities rather independently, but the campaign will not be able to successfully complete the third stage without strong support from the IHS and other organizations. If everybody gets together supporting the campaign and participating actively and financially, then a successful outcome seems within reach. All the data on epidemiology and health care resources are ready for use but forceful advocacy is needed. Recently the World Health Assembly adopted the Intersectoral Action Plan on Epilepsy and Other Neurological Disorders (IGAP). The GCH has worked with WHO in developing the document and headache is mentioned. The idea is that for the next 10 years neurological disorders must be a priority for WHO and world governments. The headache field, thanks to GCH, is well prepared for this initiative, but it needs a strong commitment from IHS and other headache organizations to harvest sufficient results. Education in headache care at pre- as well as post-graduate level, funding for headache research, and first and foremost, care facilities for headache patients must all be greatly improved. That should be the common goal for GCH, IHS and all other headache organizations during the next 10 years.