
Abstract
Aim
The aim of the present study was to establish annual prevalence of primary headaches, migraine, and tension-type headache among adults in a post-conflict area of Serbia.
Methods
The data for this cross-sectional study was obtained via face-to-face interviews using questionnaires specifically designed for this purpose, in line with the available guidelines. The study sample included adults aged 18–65 years whose native language is Serbian with residence in six predominantly Serbian communities in Kosovo and Metohija. Relevant diagnoses were established according to the diagnostic criteria of the International Classification of Headache Disorders, 3rd edition.
Results
The study included 1062 adults. Analyses indicated 47.7% prevalence of primary headaches. The 1-year prevalence of migraine (with aura and without aura) and tension-type headache was established at 15.2% (3.3% and 11.9%), and 32.2%, respectively. One-year prevalence of chronic headache was calculated at 3.5%, while the prevalence of medication overuse headache was slightly lower at 2.9%. Primary headaches were more prevalent among women, participants residing south of the river Ibar, married or cohabiting individuals, as well as among interviewees (persons) who reported feeling unsafe in Kosovo and Metohija. This is the first study of the prevalence of primary headache disorders in Serbia. The obtained data is comparable to the data available for other countries, especially those in the Balkan region.
Introduction
The majority of extant studies exploring primary headache prevalence have been conducted in Europe. The cumulative lifetime primary headache prevalence in Europe is estimated at 77%, with migraine affecting 16% of the population, 20% of women and 11% of men, and tension-type headache (TTH) reported by 62.6% of individuals, with a somewhat higher prevalence among women (1).
Average 1-year migraine prevalence in adults is estimated at 14.7% (8% for males and 17.6% for females), whereas episodic TTH affects about 42% of adults (2). When interpreting these findings, however, it is important to consider that the majority of pertinent studies included only individuals with a definitive migraine diagnosis. Thus, some authors estimate that the rates would likely double if all individuals in whom migraine is indicated by the presence of all but one diagnostic criterion of the International Classification of Headache Disorders, 3rd edition (ICHD-3) (3) were included. Meta-analysis of European studies aiming to ascertain primary headache prevalence indicates that 4% of European population is affected by chronic headaches (1). In such cases, excessive use of pain relief medication is common, affecting 1–2% of the population, and is more frequent among women of low socioeconomic status (4,5).
Counter to the findings yielded by studies conducted in Europe, those pertaining to Asian countries indicate much greater variability in primary headache prevalence. Thus, a prevalence of primary headaches of 23.8% was reported from China (6) and of 80% for some headache forms in adults from Nepal (7). Less pronounced variations are noted among African countries, with the lowest prevalence, of 44.9%, recorded in Ethiopia (8) and the highest, of 61.6%, in Zambia (9). Some authors postulate that such wide variations in primary headache prevalence are due to genetic factors, while others ascribe them to etiological or cultural influences (10). Although living conditions have improved for most individuals across the globe, stress levels have also increased, while pain medication has become more readily accessible and awareness of preventative factors has improved (2). This prompts the question of whether, and how, the interplay of all these influences affects primary headache prevalence. The available evidence indicates that despite a slight increase in migraine frequency, headache prevalence in the adult population has remained relatively stable (11). Given the specific living conditions in the Autonomous Province of Kosovo and Metohija in terms of political and security factors, the present study was guided by the hypothesis that these unique characteristics would influence the primary headache prevalence in areas predominantly inhabited by ethnic Serbs in this region.
This is indeed the first study examining primary headache prevalence among adults in Serbia.
Aim
The aim of the study was to estimate the annual prevalence of primary headaches, migraine and TTH, diagnosed in accordance with the ICHD-3 criteria, among adults in a post-conflict area of Serbia.
Methods
This cross-sectional study involved a representative sample of participants that took part in face-to-face interviews guided by a questionnaire specifically designed for this purpose. The inclusion criteria were: age in the 18–65 range, Serbian mother tongue, and residence in the areas of Kosovo and Metohija predominantly inhabited by ethnic Serbs. Sample size was established considering headache prevalence, population size, statistical significance (alpha = 5%) and a power of 80%. The study included six municipalities, namely Severna Kosovska Mitrovica, Zubin Potok and Leposavić, located north of the Ibar river, as well as Gračanica, Štrpce and Ranilug, representing central municipalities of three geographically distinct regions inhabited by predominantly Serbian residents, located south of the Ibar river (Figure 1). It is estimated that 65,000 individuals of Serbian nationality reside in the region covered by the present study. The survey included all boroughs in all aforementioned municipalities, starting with the main street and then selecting every other one thereafter. In each chosen street, the first house or flat in the building on the right hand side was visited first, after which every other dwelling was chosen. Once the household representative provided information on the number of adults residing in each dwelling, one person that met the study inclusion criteria was chosen for the interview. If this individual was not at home at the time, two additional visits were made before eliminating them from the sample. Study participation was voluntary and all included individuals were provided with a detailed explanation of the study aims and procedures, which they confirmed by signing an informed consent. Individuals with a history of stroke, multiple sclerosis, meningitis, encephalopathy, epilepsy, dementia, and head trauma were excluded from the sample.

Serb population of Kosovo in 2011.
Prior to commencing the participant recruitment process, the study was approved by the Ethics Committee of the Medical Faculty, University of Pristina-Kosovska Mitrovica.
A structured questionnaire was developed for the study, in line with the recommendations for headache epidemiological studies (12), for which the HARDSHIP questionnaire served as a guideline (13). The adopted survey items were translated to the Serbian language using the “Lifting the burden” translation protocol (14). The first part of the data collection instrument comprised questions aiming to elicit demographic and socioeconomic information and was completed by all respondents. The final item in this section prompted the participant to indicate if, in the preceding 12 months, they had experienced headaches unrelated to cold, fever or head injury. The individuals that gave an affirmative response to this question proceeded to the second part of the interview, guided by questions pertaining to headache characteristics: Headache frequency and duration; pain localisation, intensity and quality; presence and duration of symptoms preceding pain; presence of associated symptoms and signs, such as nausea, vomiting, photo/phonophobia; headache influence on everyday activities; and any links between physical exertion and pain exacerbation.
Recruitment and data collection in the field encompassed the period from March 2017 to June 2017. The interviews were conducted by medical doctors or students in the final year of a medical degree, all of whom were trained for the purpose of the present study. Training incorporated clinical aspects of headaches, study design, and interview aims and procedures, and all interviewers were tested on their acquired knowledge upon completion of training. To establish the diagnostic sensitivity and specificity of the questionnaire used during the interviews, a pilot study involving 70 individuals that subsequently underwent neurological assessment was conducted (NM and JZT). High sensitivity (95.6%) and specificity for migraine (88.1%) and TTH (86.5%) was noted. A definitive migraine or TTH diagnosis was established if all ICHD-3 criteria were met, whereas a diagnosis of probable TTH/migraine was noted if all but one criterion was met. Headache was diagnosed independently by two neurologists (JZT and NM) based on the questionnaire responses. If the examinee had ≥15 attacks during the month for more than 3 months, a diagnosis of chronic headache, migraine or TTH was made, depending on which criteria were met. If there was also frequent use of analgesics (≥15 days/month for more than 3 months or combined analgesics, opioids, ergotamine or triptans) (≥10 days/month for more than 3 months), a diagnosis of headache with excessive use of medication was made.
One-year prevalence, as well as the prevalence specific for gender, age group and headache type, were calculated as the ratio of positive cases to the relevant population size, adopting a 95% confidence interval (CI). All statistical analyses were performed using SPSS Statistics (Statistical Package for Social Sciences) for Windows, version 17. For continuous variables, mean and standard deviation was reported, while categorical variables were presented as numbers and percentages. Continuous variable comparisons were performed via Student’s t-test, while the chi squared (χ2) test was employed for the comparison of categorical variables across subgroups. Statistical significance was indicated by p < 0.05.
Results
The previously described participant recruitment process yielded 1200 adults aged 18–65 years that met the study inclusion criteria, 1062 (53.8% females and 46.2% males) of whom agreed to take part in the interviews. Response rate was 88.5%. In the 12-month period preceding the study, 503 respondents experienced headaches, indicating a 47.4% 1-year prevalence.
Headaches affected a greater percentage of women (58.3%) relative to men (34.6%) (p < 0.001). The average age in the subsample affected by headaches was 40.14 ± 12.1 years, while that among individuals that were headache free was 37.7 ± 14.1 years (p = 0.004). Headache was most frequently reported by those aged between 36 and 55 years, while being least common among the youngest participants. Socio-demographic characteristics of the study participants are reported in Table 1.
Sociodemographic characteristics of participants with and without headache.

Note: Values in bold denote statistical significance.
Analyses further revealed that headaches predominantly affected married or cohabiting individuals. More frequent headaches were reported by employed and unemployed respondents relative to students and the retired, as well as by individuals who reported feeling unsafe in Kosovo and Metohija (Table 1).
While 1-year prevalence migraine prevalence in the study sample was 15.2%, a statistically significant gender difference was noted, whereby 22.2% of women were affected compared to only 6.9% of men (p < 0.001). Migraine without aura was noted in 11.9% of the sample (17% and 5.9% for women and men, respectively) (p < 0.001), while migraine with aura affected 3.3% of the sample (5.3% of women, 1% of men; p < 0.001). In the 12 months preceding the study, 32.2% of the respondents suffered from TTH, which was once again more prevalent among women (36.1% vs. 27.7% for men) (p = 0.004). Socio-demographic characteristics of the study participants affected by migraine and TTH are reported in Table 2.
Sociodemographic characteristics of participants with migraine and TTH.
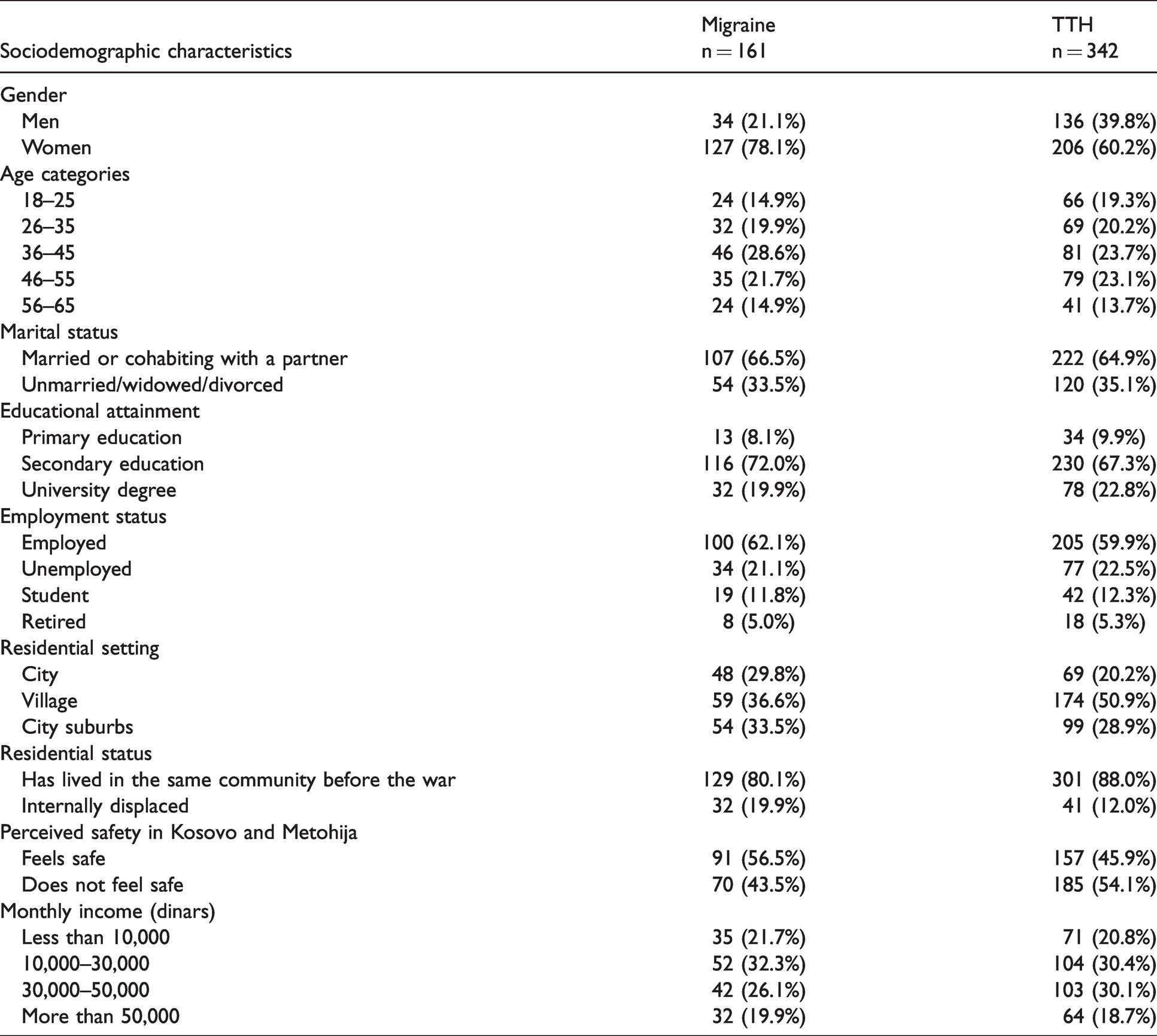
Migraine was more frequently reported by participants in the 36–45 and 46–55 age groups (19.7% and 16.8%, respectively), while being least prevalent among those aged 18–25 years (9.2%), as shown by Table 2. While no statistically significant differences in migraine prevalence were noted among men in different age categories, migraine was statically significantly more frequent among women aged 36–45 years (28.7%) relative to other age groups (p = 0.011). Married and cohabiting participants were also more likely to report migraines (17.1%) compared to unmarried, divorced, and widowed individuals (12.4%) (p = 0.003). Migraine was also more prevalent among city (19.4%) and suburban residents (15.9%) relative to those living in rural areas (12.4%) (p = 0.044). Finally, internally displaced persons reported migraines more frequently (23.5%) relative to those that had resided in the current community prior to the war of 1999 (13.9%) (p = 0.004). TTH prevalence was highest among those aged 46–55 (38%) and lowest for the youngest respondents (25.3%). Counter to the findings reported for migraine, TTH was highest among rural residents (36.7%), followed by those living in city suburbs (29.1%) and finally cities (27.8%). On the other hand, the findings related to marital status coincided with those obtained for migraine, as TTH was more prevalent among married or cohabiting respondents (35.5%) than among those that were unmarried, divorced, or widowed (27.5%).
Finally, a statistically significantly higher number of participants that feel unsafe in Kosovo and Metohija reported having TTH (37.9%) compared to those that felt safe in their community (27.4%) (p < 0.001). While 3.5% of the respondents were diagnosed with chronic headache, the difference among women (5.4%) and men (1.2%) was statistically significant (p < 0.001). Similarly, medication overuse headache (2.9%) was statistically significantly higher among women (4.2%) compared to men (1.4%) (p = 0.007). No statistically significant differences in the chronic headache prevalence or rate of pain medication overuse among those suffering from migraine and TTH was noted, at 3% versus 4.4% and 2.4% versus 3.6%, respectively. Finally, in 4.9% of respondents suffering from migraine, this condition was diagnosed as chronic. The prevalence of chronic migraine and excessive medication use by age category is provided in Table 3.
Distribution of participants with chronic headache and medication overuse by age category.

Discussion
This is the first population study aiming to establish primary headache prevalence in Serbia. The sample for this investigation was drawn from predominantly Serb communities in the Autonomous Province of Kosovo and Metohija and, based on the interview responses, the 1-year primary headache prevalence was determined. According to the Serbian Statute, Kosovo and Metohija remains an autonomous province within the Serbian territory following the war in 1999. The region has been under temporary UN administration (UNMIK) and since 2008 independent governance has been supported by European Union Rule of Law Mission in Kosovo. Since 1999, ethnic Serbs in the Kosovo and Metohija territory have been residing mostly north of the Ibar River, in municipalities where the majority of the population is of Serbian nationality, forming a unified geographic region directly adjacent to Central Serbia. However, some of the ethnic Serbs still live south of the Ibar River, far from the remaining Serbian territory, in isolated and geographically dispersed communities (enclaves) surrounded by a predominantly Albanian population. This unique situation imposes vastly different political and security conditions for those living north and south of the Ibar River, which is why the present study included three municipalities from each of these regions.
The 1-year prevalence of primary headache for the entire study sample was calculated at 47.4%. In pertinent literature, there is a wide variation in the reported prevalence, ranging from 21.6% to 84.9% (6–10,15–24). Our findings are comparable to those obtained in neighbouring Croatia (39.9%) (19). More recently, higher prevalence rates are increasingly being reported, with 61% noted for Kuwait (23), 62.9% for Russia (16), 63.9% for India (24), 76.6% for Pakistan (10) and 84.9% for Nepal (7). In line with most earlier research on this topic (22–24), our findings indicate that primary headache is more prevalent among women, which is attributed to biological factors, as well as socio-cultural influences (25,26). Nonetheless, other authors have reported similar primary headache prevalence for men and women (10). In accordance with the results obtained for the Croatian population (19), in our sample, headaches became more frequent in middle age, and primarily affected married and cohabiting individuals, while no link between educational level and residential setting was noted. Other authors have also reported variations in headache prevalence across municipalities and regions within this territory (19). Our findings further reveal that those that reported feeling unsafe in Kosovo and Metohija were more likely to suffer from headaches.
One-year migraine prevalence of 15.2% was measured for the entire sample, with a significant difference between women (22.2%) and men (6.9%), which is in line with the 14.7% yielded by the Global Burden of Disease Study 2010 (27). Women are not only more likely than men to suffer from migraine, but the highest prevalence was noted for those in the 36–45 age group. On the other hand, no link between age and migraine prevalence was noted for male respondents, in line with the findings reported by other authors (7,9,10,16,19,22). Migraine was also more frequently reported by married or cohabiting individuals, those living in cities or suburbs, and internally displaced persons (after the war of 1999). The results obtained in this investigation most closely coincide with those based on European surveys, as 15% was reported for Croatia [19], 16.4% for Turkey (17) and 18% for Norway (28). In other parts of the world, variations in migraine prevalence are more pronounced, ranging from 6.1% in South Korea (21) and 9.3% in China (6) to 23.1% in Kuwait (23), 25.2% in Pakistan (10) and 34.1% in Nepal (7).
Limited empirical evidence, however, exists for prevalence of migraine subtypes. Based on the available data, 1-year prevalence of migraine with aura in specific Russian subpopulations is 2.4% (29), while 2.3% was reported for Australia (30) and 2.6% for Ethiopia (31), which is slightly lower than the 3.3% obtained in our study (5.3% for women, and 1% for men). A more recent Norwegian study revealed a much higher 1-year prevalence of migraine with aura in this country, at 6.9%, with a significant difference between women (8.6%) and men (3.8%) (22).
Our investigation yielded a 1-year prevalence for TTH of 32.2%, which was once again greater for women (36.1%) relative to men (27.7%). Similar findings (28.6%) were reported for Italy (32), while 29% was cited for Kuwait (23) and 37.3% for Georgia (18), while somewhat higher prevalence (41.7%) was recorded in Pakistan (26), Norway (43.1%) (22), and Nepal (44.1%) (7). In our sample, TTH prevalence was highest in the southernmost municipality of Štrpce, and was lowest in the northernmost municipality of Leposavić, which is geographically linked to Central Serbia. Overall, higher TTH prevalence was noted for the respondents residing south of the Ibar river. The continued uncertainty imposed by the unstable political and security conditions since the war of 1999 has likely increased the tension for ethnic Serbs living in this territory. Indeed, it is noteworthy that the perceived sense of safety decreases with the distance from the Central Serbia boundary, as the southernmost parts of Kosovo and Metohija are predominantly populated by ethnic Albanians. Thus, it can be assumed that these conditions have contributed to the much greater TTH prevalence among participants that reported feeling unsafe in their communities.
Chronic headache was diagnosed in 3.5% of the study sample. In current literature, chronic headache prevalence varies, with 1.0% reported for China (6), 4.4% for Kuwait (23), 7.4% for Nepal (7), 7.6% for Georgia (18), 8.1% for Pakistan (10), and 10.3% for Russia (16). Our findings are in line with those pertaining to the neighbouring countries, such as Croatia (33), where 2.4% prevalence was reported, and Norway (34), where an earlier study yielded 2.9% chronic headache prevalence. Authors that have conducted a population study in Brazil have reported a 6.9% 1-year chronic headache prevalence, indicating that it primarily affects women, the unemployed, higher earners, and sedentary individuals (35). We have also noted a greater prevalence among women, especially those aged 36–45, 6.8% of whom were diagnosed with chronic headache. Based on the available data, prevalence of medication-overuse headache (MOH) ranges from 0.9% in Georgia (18) to 2% in Germany (36). In a more recent Norwegian study (22), the authors found a very high (3.0%) MOH prevalence, based on 1.2% recorded for men and 3.9% for women. It is interesting to note that in Pakistan, chronic headache prevalence is high (8.1%) but MOH is rare, at 0.7% (10). Our investigation indicated that in the 12 months preceding the study, 2.9% of the respondents overused pain relief medication for countering headache symptoms. Moreover, MOH was most common among younger and middle-aged individuals (5.1%) and women (4.2%). In the recently published study from Serbia, it was shown that headaches have not only medical but also great socioeconomic significance. The authors evaluated the impact of individual headache types on work and work efficiency and demonstrated that monthly absence from work was mostly represented by migraine sufferers (7.1%), significantly more than sufferers with TTH (2.23%) and other headache types (2.15%). Additionally, lower efficiency was significantly more frequent with migraine sufferers. This study showed that headaches, especially migraines, significantly affect the work and work efficiency of headache sufferers by reducing their productivity (37).
Study limitations
War and persecution of the Serbian population in the Kosovo and Metohija territory have resulted in extensive internal displacement, whereby the majority of ethnic Serbs have left their homes and now reside elsewhere in the region, or have migrated away from Kosovo and Metohija. Thus, to ensure impartiality, a large sample was recruited for the present study. For most Serbs still living in the Kosovo and Metohija territory, fear of conflict breaking out and potential forced displacement dominates their everyday life. Stressful events are a frequently reported trigger for primary headache disorders; therefore, the obtained results may overestimate the prevalence of headache. However, it is common for various diseases, especially those that are not life-threatening conditions, to be ascribed to stress. Hence, it is likely that the results reported here underestimate the true headache prevalence, as the respondents have neglected or overlooked its signs and symptoms. Another limitation stems from restricting the study sample to native Serbian speakers due to the language barrier. It would thus be beneficial to replicate this investigation by including Albanians that have for centuries lived on this territory alongside Serbs. It is likely that wide variations would emerge in headache prevalence, reflecting genetic differences, as well as effects of cultural, and political and security factors. In the future, such multi-ethnic studies should be considered to increase our understanding of the factors contributing to headache development. A special problem in statistical analysis of this study was the lack of census data, which consequently made assessment of regional differences impossible.
Conclusion
Primary headache prevalence among adults in a post-conflict area of Serbia is similar to those reported for other countries, especially those in the Balkan region. Primary headaches are more prevalent among women, participants residing south of the Ibar river, married or cohabiting individuals, as well as among those who reported feeling unsafe in KiM.
Clinical implications
Primary headache prevalence in the ethnic Serb population residing in the Kosovo and Metohija territory is similar to that reported for other countries, especially those in the Balkan region. Primary headaches are more prevalent among women, participants residing south of the river Ibar, married or cohabiting individuals, as well as among persons who reported feeling unsafe in KiM.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.