
Abstract
Objective
The current study explored whether the chances of having migraine are influenced by a youth’s friendship with a migraineur.
Methods
The study was centered on a community-based non-referral cohort of eighth graders from two middle schools in Taiwan. Among the 642 recruited adolescent students, 610 (95%) (mean age 14.1 years, male ratio 51.2%) nominated three good friends and completed a validated headache questionnaire for migraine diagnosis at the follow-up survey 1 year later. To explore social influences on incident migraine, we used longitudinal statistical models to examine whether the development of migraine in one adolescent during the 1-year observational period was associated with that in his/her friends.
Results
Overall, 1700 social ties were established in the social network based on the reported lists of good friends. Randomization test for the homophily effect demonstrated that the students with migraine tended to cluster together in the social network even when those with incident migraine were also considered (p = 0.003). Besides, when friendship choices were mutual, the relative risk of an adolescent becoming a migraineur was 3.26 (95% CI: 1.25–8.47, p = 0.015) if his/her friend became a migraineur (induction) during the 1-year observational period.
Conclusion
To the best of our knowledge, this is the first study to demonstrate that migraine may spread through social networks in young adolescents. Both homophily and induction effects are possibly contributory.
Introduction
Amidst a backdrop of decreasing premature childhood death, aggregate disability increased to a total of 145 million years lived with disability (YLDs) globally among children and adolescents in 2017. Overall health improvements were slowest in adolescents (1). Among the top 10 causes of YLDs in children and adolescents, primary headache disorder, particularly migraine, stands out because this highly debilitating disease – now recognized as the second highest cause of disability worldwide and the first cause in those under 50 years of age (2) – has its root in adolescence, and comparatively little is understood about modifiable risk factors and effective prevention programs.
Existing literature has suggested that a single mechanism mediating the underlying neurophysiology of migraine symptoms is unlikely (3). Social causation of migraine is one of the hypothesized mechanisms (4), assuming that social factors, such as the socioeconomic status (SES) and social networks, may exert an effect on the level and severity of migraine. A higher prevalence of migraine among low-income or low-education groups has been reported (5–13). Additionally, migraine initiation appears to be the dominant mediator of the observed higher prevalence in these disadvantaged groups (4). This finding suggests that the etiology of migraine can be associated with exogenous factors because SES itself can be a surrogate for various social, psychological, and physical exposures. Besides, evidence has revealed a potential association between societal transformation and changes in the prevalence of migraine over time. From 1974 to 1992, an alarming threefold increase in the prevalence of migraine was reported in two independent cohorts of 7-year-old children in Finland (14). Similarly, in the sampled populations of Taiwanese adolescents, we found that the 1-year prevalence of migraine increased by 42% from 5.2% in 1999 to 7.4% in 2001 (15). Despite the influences on prevalence of migraine from increased awareness and diagnosis over time, the previously reported prevalence of migraine might likely seem to be increasing, with societal changes or modernization being a potential factor influencing the development or maintenance of the disease.
Although many behaviors and affective states, including smoking (16), drinking (17), obesity (18), depression (19), and suicide (20), have been shown to spread through social networks over time, evidence of the effect of social networks on the emergence of migraine remains lacking. A higher occurrence of menstrual migraine was observed among university students who lived together than among students who lived alone, but no social causes of the association were specified (21). By contrast, evidence from another discipline, animal research, implicated the possibility of communication of pain through social contacts. The presence of a mouse in pain housed for several weeks in a cage can have a physiological and behavioral effect on another mouse housed in the same cage through social cues (22). A more recent study showed that “bystander” mice housed and tested in the same room as mice subjected to inflammatory pain developed corresponding hyperalgesia (23). Considering that migraine may have its social etiology, it is interesting to examine whether and how social contacts or social relationships between individuals may influence the occurrence of this highly disabling pain disorder.
In this social network study, we explored whether and how migraine might spread through social networks. By using a longitudinal network of adolescent students, we analyzed the role of social networks in the onset and presence of migraine, focusing on the following: a) whether clusters of migraineurs existed within the social network; b) whether an adolescent’s migraine status was associated with that of his/her social contacts; and c) the extent to which such associations depended on the nature or type of friendship.
Methods
Data source
The current study was part of the Taitung County Headache Survey, a population-based, longitudinal, observational cohort study that was initiated in 2005 to prospectively investigate relationships between headache and a set of mood, sleep, and behavioral problems in adolescent students (24–26). Taitung County is less developed compared with other regions of Taiwan, and most of its population belongs to the middle or lower socioeconomic class. To obtain representative data, this survey selected three public middle schools, including Shin-Sheng and Tung-Hai middle schools, both located in urban areas, and Chih-Pen middle school, located in a rural area. In the first wave recruitment, we aimed to recruit all the seventh and eighth graders from Tung-Hai and Chih-Pen middle schools and all the seventh graders from Shin-Sheng middle school in 2005. We continued to recruit all the seventh graders at Tung-Hai and Chih-Pen middle schools in 2006 (second wave recruitment) and 2007 (third wave recruitment). Besides, we annually followed up the recruited adolescents from 2006 to 2009 (first to fourth follow-up surveys) while they were at school. Because students spend 3 years in middle schools in Taiwan, we could perform one or two annual follow-ups when they were in middle schools (grades 7–9) (Figure 1). The Institutional Review Board of the Kaohsiung Medical University of Taiwan reviewed the medical ethics of the study (KMUH-IRB-950090).

Flowchart of the recruitment and follow-up survey from 2005 through 2009.
Sampling method and survey
The sample population of the first wave recruitment comprised all the seventh and eighth graders from Tung-Hai and Chih-Pen middle schools and all the seventh graders from Shin-Sheng middle school in 2005. In the second and third waves, all the seventh graders at Tung-Hai and Chih-Pen middle schools were recruited in 2006 and 2007, respectively. The sample could be considered a community-based sample, accounting for around 46% of adolescents aged 13–14 years in Taitung County who attended middle schools at that time. Official letters describing the study objectives and methodology were initially mailed to the Education Department of Taitung County Government and school principals of these three schools for their approval. With help from teachers and school nurses, the participating students answered the survey questionnaires by themselves in class both at baseline recruitment and follow-ups.
Questionnaires
The self-administered questionnaires consisted of four parts. 1. Sociodemographic data included age, sex, grade, living arrangements, parental education levels, parental occupations, self-reported household economic status, academic performance, family dynamics, and stressful life events, which were adapted from questionnaires employed in the Taiwan Youth Project (27). 2. A validated headache questionnaire for adolescents was used for headache diagnoses (28) with some modifications based on the International Classification of Headache Disorders, Second Edition (ICHD-2) (29). This questionnaire assessed the headache profile during the past 3 months, including headache severity, duration, frequency, locations, characteristics, accompanying symptoms, painkiller usage, and school absence due to headache or other causes. Aura symptoms before headache and their duration were also explored, including visual, sensory, and language disturbances. 3. A validated depression questionnaire for adolescents, the Adolescent Depression Inventory (ADI), was used to survey symptoms of depression with the time frame of the past month. This 31-item questionnaire has a high internal consistency of 0.86 and a test–retest reliability of 0.76. It has also been shown to be highly correlated with the Chidren’s Depression Inventory (0.79), a widely recognized measurement for depression in youths, in the original validation study (30). Adolescent students in the present study were asked to report their experience of each symptom in a ‘yes’ or ‘no’ manner and we calculated ADI scores as an index of depression severity (score range 0–31). ADI was used as a main measurement in our previous studies on the associations between child-parent relationship, depression, migraine and presence of suicidal ideation in adolescents (24–26). 4. A validated Chinese version of the Pediatric Migraine Disability Assessment (31,32) was used to assess headache disability during the previous 3 months. All four questionnaires were administered at each recruitment and follow-up survey. The adolescents were required to provide additional information on friendship only at the third follow-up survey in 2008; they were asked to provide a list of three good friends, either in their school or outside the school. Accordingly, we analyzed the current data of social networks based on the reported lists of good friends.
Validation of headache diagnosis and suicide ideation item of ADI
A parallel study to evaluate the validity of this questionnaire-based diagnosis for migraine with and without aura was conducted. The board-certified neurologists, who were blind to the questionnaire results, performed a neurologic examination and conducted a semi-structured headache interview of randomly selected subjects. Headache diagnoses made by the neurologists according to the ICHD-2 criteria (29) were used as the gold standard. Besides, 65 subjects (46 girls and 19 boys; mean age 14.5 ± 0.7 years) with chronic daily headache finished the ADI and were interviewed using the Mini-International Neuropsychiatric Interview for Children and Adolescents (MINI-Kid, version 1.01) by a board-certified psychiatrist to assess psychiatric comorbidity, including depression and anxiety. Compared to the MINI-Kid results, the sensitivity of the single question of suicidal ideation in the ADI was 75%, and the specificity was 88.7% (24).
Analytical methods
A separate data set was created that linked adolescents through self-described social ties (based on the reported lists of good friends). Through these self-described social ties, we developed network links from one participating adolescent to other adolescents. Each link between two adolescents might be identified by either party identifying the other as good friend; for example, we identified this link either when A nominated B as a friend or when B nominated A as a friend. This directionality was methodologically important, and accordingly, friends were classified as nonmutual (ipsilateral); that is, ego perceived or alter perceived, in which “ego” denoted the adolescent of interest and “alter” denoted the other adolescent in this social tie, and mutual (bidirectional). We analyzed the effect of social influence on ego’s migraine status by type of friendship.
To examine whether clusters of migraineurs existed within the observed social network, we used a randomization procedure to test the autocorrelation of social ties for students with and without migraine (33,34). The observed social network was compared with 10,000 randomly permutated networks by preserving the network topology and the overall prevalence of migraine but randomly shuffling the assignment of the relationship between nodes. Accordingly, if clustering of migraine in the social network existed, the autocorrelation was higher within the migraine group than between groups.
Furthermore, to explore the association between an ego’s social network and his/her migraine status, various factors were included in our models, including the prospective effect of an alter’s migraine status and social network variables, such as an ego’s number of first-degree friends and his/her eigenvector centrality. An ego’s migraine status at the 2009 follow-up survey was regressed on ego’s sex, depression score, and migraine status in the prior year as well as an alter’s migraine status in the prior year and that in the year of interest (2009). The ego’s migraine status in the prior year was included to eliminate serial correlation in errors and control the ego’s genetic endowment and any intrinsic, stable tendency to develop migraine. The alter’s migraine status in the prior year was included to control for the “homophily” effect by which individuals might tend to bond with other similar individuals. The key coefficient in the model used to measure the effect of “induction” was the variable for contemporaneous alter migraine status; that is, the alter’s migraine status in the year of interest (2009). Generalized estimating equations (GEEs) were used to account for multiple observations of the same ego across ego–alter pairings, and an independent working correlation structure was assumed for the clusters (35,36). GEE regression models provided parameter estimates in the form of beta-coefficients, whereas the results reported in tables are in the form of relative risks.
To assess the possibility of omitted variables or contemporaneous events explaining the associations, we used longitudinal models and examined how the type or direction of the friendship between an ego and alter affected the association between them. If unobserved factors drove the association between the ego and alter, then the directionality of friendship should not be relevant and migraine in an ego and alter would increase and decrease together in response to unobserved factors. In this study, we tested the potential existence of effects of the migraine status of an alter on the migraine status of an ego by their type of friendship (i.e. any type of friend, nonmutual friend, and mutual friend).
Results
Among the 642 grade 8 adolescents surveyed in 2008, 610 (95%) nominated three good friends and received a follow-up survey in 2009. The mean age of this study cohort (n = 610) was 14.1 years. Among them, 51.2% were male adolescents. Approximately 10% of the adolescents (n = 61) had migraine at baseline (2008), whereas the other 26 developed migraine in the subsequent year (2009) when they became ninth graders (incidence rate: 4.7%). The average scores for depressive symptoms among the eighth-grade students was 6.7 in 2008. A total of 1700 social ties among the 610 adolescent students constituted a connected but fragmented network, as revealed in Figure 2. The mean number of reported friends for each student was 2.4 (average degree: 2.4), and the average social distance between any two students was 10.9, meaning that these students usually had two to three close friends and it took more than 10 steps for the students to reach one another. Most students clustered together as small-group friends, and the whole network exhibited 195 strongly connected groups (Figure 2). The results of randomization tests for the homophily effect demonstrated that the students with migraine tended to cluster together in the social network in 2008 (p = .032) as well in 2009 when those with incident migraine were also considered (p = .003). Additionally, the majority (69.2%, 18 of 26) of the incident migraineurs in the 2009 network were found within the existing migraineur clusters, as illustrated in Figure 2.

Social network and migraine status of the study cohort of adolescent students from two middle schools in Taitung, Taiwan (n = 610, 2008–2009). Each circle (node) represents one student and there are 610 students in the observed network. The ties (lines) between the nodes indicate friendship between them. The interior color of the circle indicates the student’s migraine status: Yellow denotes a student who had existing migraine since the prior year; red denotes a student who newly developed migraine, while gray denotes a student without migraine. Students with migraine (yellow color) formed multiple small clusters in the social network initially (a), and one year later, the initial migraine clusters expanded, and some of the students tied to friends with existing migraine developed migraine (red color) (b).
For any type of friendship, the induction effect of a contemporaneous alter’s migraine status on an ego’s migraine status at the 2009 survey was not significant in the GEE model. An ego’s migraine status in the prior year, alter’s migraine status in the prior year, and ego’s depressive symptom score significantly contributed to the ego’s migraine status in the year of interest (2009) regardless of whether network variables were controlled for in the models (Table 1). Network variables included in the model were an ego’s number of first-degree friends and “eigenvector centrality,” which indicated how central a person was in the whole network. The larger this value was, the better connected an adolescent was to all others in the network either directly via friends or indirectly via the friends of their friends. The model showed that network centrality did not contribute to the likelihood of an ego’s migraine.
Prospective influence of an alter’s migraine on an ego’s migraine status in the subsequent year of interest (for any type of friend).
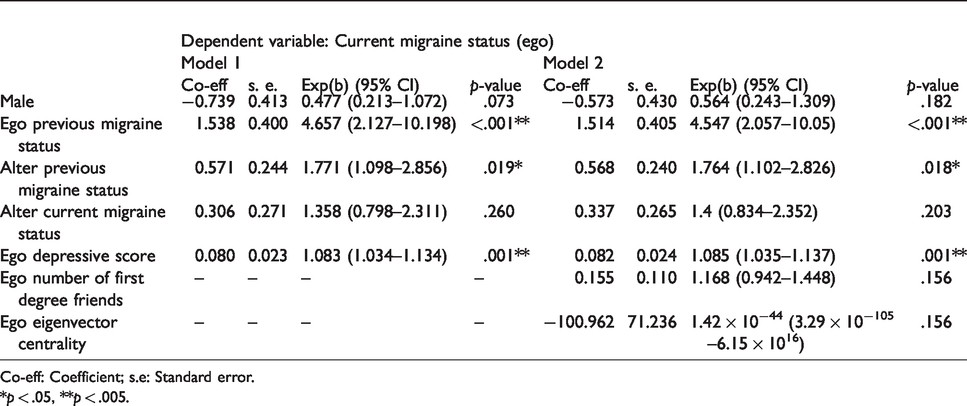
Co-eff: Coefficient; s.e: Standard error.*p < .05, **p < .005.
To further clarify the effect of type of friendship, Table 2 shows that the adolescents were at an over threefold risk (RR = 3.26 [95% CI: 1.25–8.47]) of becoming migraineurs if a mutual friend became a migraineur during the 1-year observational period. This held true irrespective of whether we included network variables in the models. Additional measurements that influenced an ego’s migraine status among mutual friends included the ego’s previous migraine status (RR = 4.66 [95% CI: 1.82–11.95]) and depression score (RR = 1.09 [95% CI: 1.03–1.15]). Besides, Table 3 and Figure 3 show that in subgroup analyses, the induction effect of a contemporaneous alter’s migraine status on an ego’s migraine status at the 2009 survey was significant only for mutual friends (RR = 3.38 [95% CI: 1.34–8.55]) and for alter-perceived friends (RR = 1.95 [95% CI: 1.03–3.69]) but not for ego-perceived friends.
Prospective influence of an alter’s migraine on an ego’s migraine status in the subsequent year of interest (for mutual friend).

Co-eff: Coefficient; s.e: Standard error*p < .05, **p < .005.
Association between a friend’s migraine and ego’s migraine, by type of friendship.
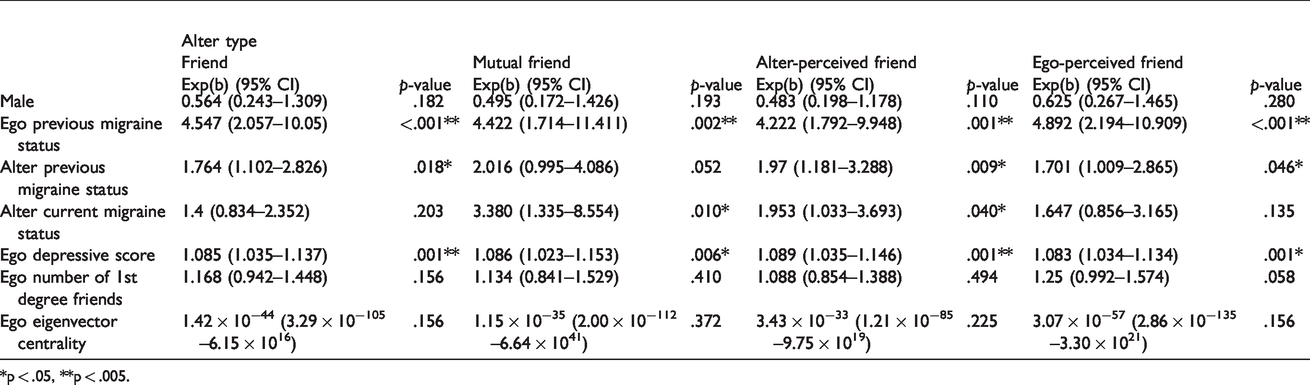
*p < .05, **p < .005.

Alter type and migraine in the social network.
Discussion
The current study evidenced the potential existence of “homophily” and “induction” effects on the presence of migraine in young adolescents. In the observed social network, adolescents with migraine tended to cluster, and the clustering of migraineurs might be partly attributable to the “homophily” effect by which adolescents selected friends with similar traits or friends who resembled themselves. Additionally, our findings on the association between the type of friendship and social influence on an ego’s migraine status suggested the existence of an “induction” effect (contagion), which was more prominent between mutual friends by which migraine was observed to travel along social networks over time.
Although the induction effect of migraine has never been fully explored, the existing literature suggested the possibility of influences of another individual’s pain status on an observer’s related neurocircuits. Numerous studies have demonstrated that empathy for pain activates neural structures involved in the direct experience of pain, such as the anterior insula and medial/anterior cingulate cortex (37,38), which are part of the so-called pain neuromatrix (39). A meta-analytic study provided robust evidence that these neural structures constitute a core network for pain empathy, and this activation pattern holds true across studies performed in different countries, on different MRI scanners, and using different types of paradigms. The overlap of this empathic network with the neural network involved in the direct experience of pain supports theoretical accounts that place shared neural representations at the root of our ability to understand others by at least partially processing them with our own systems (40).
In the current study, we found that induction of migraine occurred only through certain friendship ties, such as mutual friends, but did not hold true for analyses among any type of friendship. In accordance, the existing literature suggested that empathy for pain may vary by type of social relationships. For instance, people are shown to recruit the dorsal anterior cingulate cortex and insula for both the physical pain of close others (41) and strangers (42); however, an fMRI study showed that while observing a friend’s exclusion (social pain) activated affective pain regions associated with the direct experience of exclusion, observing a stranger’s exclusion (social pain) activated different regions associated with thinking about the traits, mental states, and intentions of others (43). Such a finding supports the hypothesis that pain empathy differs with the nature of social relationships. In this sense, the current study agreed with the hypothesis in reporting that the induction effect of migraine might occur only through close friendship ties such as mutual friends.
Migraine usually begins in adolescence or early adult life (44). Prior studies showed that factors including low age at onset, female gender, depression, and having cutaneous allodynia were significantly associated with number of migraine days at follow-up, with lifetime depression being probably the most significant risk factor (45). Similarly, we found in this study that the adolescent’s depressive symptom predicted his/her migraine risk significantly in every model irrespective of whether we included network variables in the models. By contrast, we did not find any significant effect of gender in this social network study. Given that adolescents are frequently embedded in complex social networks and may be vulnerable to peer effects, it is understandable that within a hypothetical framework of “social causation (4)”, migraine may be capable of spreading among adolescents in this social network. Although speculative, the underlying mechanism may involve pain empathy because observing a close friend’s pain tends to trigger at least part of an adolescent’s own pain neurocircuits. However, pain empathy cannot solely explain the influence of social network on the occurrence of migraine. Beyond head pain, a migraine attack is often accompanied by nausea, vomiting, or sensitivity to light and sound. Therefore, future research is warranted to further elucidate mechanisms underlying the social transmission of not only pain but also the constellations of the associated migraine presentations.
We speculate that repeated activations of pain neurocircuits while observing a close friend’s migraine can alter the plasticity of central nociceptive pathways and reduce the threshold of developing migraine (46). Apart from the potential existence of this “induction” effect, the “homophily” effect can also play a role, by which people’s friends may not only have similar traits but actually resemble each other on a genotypic level, even at specific allele and nucleotide levels (47). In this sense, the repeated activations of neurocircuits during pain empathy might probably trigger the emergence of migraine considering the similar genotypic constellations between friends. Other supporting evidence might be drawn from animal research that demonstrated that exposure to olfactory cues from mice experiencing hyperalgesia could trigger hyperalgesia in mice housed and tested in the same environment that were not exposed to injury or noxious stimulation (bystanders) (23). Similar to this socially transferred hyperalgesia in mice, the socially transferred migraine among the adolescents, as demonstrated in the current social network study, suggested a possibility of the contagion of pain through social contacts.
Strengths and limitations
The strengths of this study include the rarely available cohort of young adolescents, the community-based nonreferral sample, and the longitudinal follow-up design. However, a few limitations should be discussed. The study did not randomize individuals into social networks, thus exposing the possibility that these results may partly reflect homophily-driven selection bias due to unobserved phenotypes that influence the development and transmission of migraine over time. It is also possible that precursor symptoms of migraine may contribute to the selection of friends due to understanding, empathy, and sharing of similar experiences. Moreover, friends of a migraineur may be more aware of migraine symptoms. It seems reasonable that adolescents might be more likely to report migraine symptoms if their friends had migraines earlier. Because the students were asked to report three good friends, our data set captured only a limited number of close friendship ties, and we could not extend our analyses to broader social networks. Despite not requiring the students to report good friends from their own schools, most of them reported good friends in the same school. In addition, the current data were collected at the time when the usage of social media was not popular; therefore, our results might not be directly generalizable to interactions through social media. Owing to the sample size of social ties, we were unable to thoroughly examine associations between social networks and migraine among second- or third-degree friends.
In conclusion, our results are important because we first demonstrated the effect of interpersonal relationships on the development of migraine in young adolescents. Both homophily and induction effects may have influenced the occurrence of migraine by the youth’s friendship with a migraineur. Future efforts to further reveal the underlying mechanisms are warranted.
Article highlights
Adolescents with migraine tended to cluster in the observed social network, and the clustering of migraineurs might be partly attributable to the “homophily” effect by which adolescents selected friends of similar traits or friends who resembled themselves. The relative risk of an adolescent becoming a migraineur was 3.26 (95% CI: 1.25--8.47; p = .015) if his/her mutual friend became a migraineur (i.e. the induction [contagion] effect). Migraine might spread from person to person in adolescent social networks.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by grants from Ministry of Science and Technology of Taiwan [MOST 107-2321-B-010-001-; MOST 106-2321-B-010-009-; MOST 104-2314-B-418-003-] and Brain Research Center, National Yang-Ming University, from the Featured Areas Research Center Program within the framework of the Higher Education Sprout Project by the Ministry of Education in Taiwan. The funding bodies played no role in the study design, analysis, or interpretation of data in this paper.
ORCID iDs
Shih-Pin Chen https://orcid.org/0000-0003-3492-9902 Shuu-Jiun Wang ![]()