
Abstract
Background
Effects of emotion suppression on physical health might be contingent on culture. Existing research on emotion regulation has mainly included western participants. Herewith the question arises, whether this gained expertise is transferable to an Asian culture.
Objectives
This cross-sectional study evaluated to what extent the regulation of emotions is related to migraine and if the relation between emotion regulation and migraine complaints differs between a Western and an Asian population. Therefore, the main characteristics and symptoms of patients with migraine from both Germany and Japan are compared.
Methods
261 Japanese and 347 German headache patients participated in this online study and completed self-report measures of emotion regulation (suppression and reappraisal) and headache complaints.
Results
Cultural groups did not differ regarding their demographic data, intake of medication and number of days with headache. German participants showed significantly higher levels of anxiety and lower levels of emotion suppression compared to Japanese patients. Emotion regulation is not correlated with headache complaints either in the Japanese or in the German patient group.
Conclusion
Although group differences were found with respect to anxiety and emotion suppression, subsequent regression analysis revealed these differences were unrelated to headache complaints. As our baseline analysis focused on group means, approaches that examine individual reaction patterns to stress and accompanying sensory stimulus processing may prove to be more fruitful and illuminating.
Introduction
Emotions are powerful signals that allow us to respond to our environment. The term “emotion regulation” defines the process by which individuals try to control or change their behavior due to prevailing emotions (1). Reappraisal is the interpretation of potentially negative stimuli in unemotional terms. Emotion suppression is defined as a conscious inhibition of expressive behavior (2). Several studies have shown that using reappraisal strategies is related to less negative emotional experience and can hence contribute to a healthier mental and physical state of being (2,3). In contrast to these findings, exerting suppression is associated with cognitive, physical and social costs such as rebound effects, poor memory, increased physical stress, including increased sympathetic activation of the cardiovascular system and heightened activation of the sympathetic nervous system (4–11). Overall one might suspect that the aforementioned outcomes of emotion regulation are universal to every individual. However, existing research on emotion regulation has mainly included Western participants, implying that these findings can only be interpreted with consideration of the Western value system (12). In some studies, Asian participants show attenuation or even complete absence of negative outcomes after emotion suppression (13). It was observed that expressing emotions led to lower blood pressure within European-American dyads. Reversed outcomes were present in Asian-American dyads, in which expressing emotions led to higher blood pressure (14). Even though the outcomes of emotion regulation considering different disorders have been addressed in recent research, the outcomes for headache disorders, and especially for migraine, have received only little attention.
The present study aims to compare the main characteristics and symptoms of patients with migraine from both Western (i.e. Germany) and Asian (i.e. Japanese) cultures. This includes frequency and severity of migraine symptoms and associated psychological complaints such as anxiety and depression, health-disturbing anxiety, emotion regulation, additional bodily symptoms and quality of life. Second, the study investigates the relation between emotion regulation and migraine complaints and explores the moderating role of cultural aspects therein.
Methods
Participants and recruiting
Data for clinical patients in Japan were collected in the Tominaga Headache Center of Tominaga Hospital, Osaka. Data for clinical patients in Germany were collected in the Headache and Migraine Clinic, Königstein. Additionally, non-clinical participants in Japan and Germany were recruited using social media and flyers. The study was approved by the Ethics Review Committee Psychology and Neuroscience of Maastricht University (reference number: 177_31_03_2017) and by the Institutional Review Board, Japan (reference number: 120046).
Male and female participants aged 18–65 years were eligible for participation in the study. Self- reported presence of acute, severe psychiatric comorbidities (major depression, anxiety disorders, eating disorders) served as exclusion criteria for study participation. Patients were asked if they currently experience acute psychiatric disturbances by means of a dichotomous response format within the online questionnaire. Patients who answered with “yes” were not able to proceed with the survey and were automatically excluded. Furthermore, sufficient understanding of German or Japanese was a prerequisite for participation. All participants had to have a history of migraine. In order to achieve a broad range of scores and, to avoid selection errors, both groups of participants included migraine patients who were already in treatment (either in a headache clinic or a subclinical setting) and participants who were not in treatment.
Assessments
The score of the Emotion Regulation Questionnaire (ERQ) assesses emotion suppression (15). It is designed to measure the participants’ tendency to use two types of emotion regulation: Cognitive reappraisal and expressive suppression. The ERQ contains six items for suppression (such as “When I am feeling negative emotions, I make sure not to express them”) and four items for reappraisal (such as “When I want to feel less negative emotion, I change the way I am thinking about the situation”). Each item is rated on a seven-point Likert scale, ranging from 1 (strongly disagree) to 7 (strongly agree). The final score is the average of all scores, which results in a final score between 1 and 7. A higher score represents greater use of the specific emotion regulatory strategy. The ERQ shows a high internal consistency (r = .79 for the reappraisal scale and r = .73 for the suppression scale) and a three-month test-retest reliability of r = .69 for both scales (15,3). The Japanese and German versions showed a good internal consistency for both the reappraisal and the suppression scale (16,17).
The Hospital Anxiety and Depression Scale (HADS) measures the affective and cognitive aspects of anxiety (HADS-A) and depression (HADS-D) whereby each sub-scale includes seven items. The items of the HADS-D focus on the symptoms of anhedonia (the inability to experience joy), which is a main feature of major depression. The HADS-A focuses on items such as restlessness, fear and worry. Items of both scales are rated on a four-point severity scale, indicating how the participant has felt in the last two weeks prior to testing (18). Each item is scored from 0–3, resulting in a maximum score of 21 for each participant. The cut-off scores for each scale range between 8–10 for mild cases, 11–15 for moderate cases and 16 and above for severe cases (18). The Short Health Anxiety Inventory (SHAI) measures the level of concern and the fear of negative consequences related to an illness on a continuum with 14 items with four response options each. Participants select the response that represents their mood over the last six months (19). The German version shows an excellent reliability (α ≥ .95) (20). The Japanese version shows a good reliability (α = .84) (21).
For our questionnaire, we used the first factor of the SHAI, which includes health anxiety (four items). For the scale of health anxiety, there is a cut-off score of >15 for participants with an elevated level of health anxiety and >18 for hypochondria (22).
Answers are scored on an ordinal scale ranging from 0 (low health anxiety) to 3 (high health anxiety). The total scale of the sum score ranges from 0–42.
Headache-related disability is evaluated by the Headache Impact Test (HIT-6), which evaluates headache-related disability in migraine patients and consists of six items (23–25). The burden of somatic symptoms is measured by means of the Somatic Symptom Scale (SSS-8) using eight items (26). Participants rate to what extent they have experienced common somatic symptoms such as stomach problems, dizziness, trouble with sleeping or back pain within the last 7 days. The SSS-8 allows an interpretation of bodily symptoms that may be caused by emotional distress and derogation from migraine disorders. Each item has five response options, which are scored form 0–4 (0 = not at all, 5 = very much). The total range of scores is from 0–32. The somatic burden is categorized in five severity levels ranging from none to minimal (0–3 points), low (4–7 points), medium (8–11), high (12–15 points) and very high (16–32 points) (26). The Japanese version shows a good reliability (α = .86) (27). The German version shows good reliability as well (α = .81) (26).
Procedure
Data were collected by means of the online survey platform Qualtrics (Qualtrics, Provo, UT), version of March 2017. Participants were not provided with the goal of the study beforehand to prevent experimenter demand effects. More specifically, they were informed that we were interested in individual differences in headache complaints. In the debriefing afterwards, they received detailed information about the goal of the study. Participants were not compensated for their participation in the study. Informed consent was obtained from all participants. Participants who agreed to these terms and conditions, who had no current existing psychiatric comorbidities and who met the International Classification of Headache Disorders diagnostic criteria for a migraine disorder were eligible for the survey. The diagnosis of migraine was checked via self-check by the ICHD-3 beta criteria of migraine (28). The patients were qualified to take part in the study and to proceed with the online survey if they confirmed at least five headache attacks fulfilling the following criteria: a) headache attack lasting 4–72 hours; b) pulsating quality; c) moderate or severe pain intensity; d) aggravation by or causing avoidance of routine physical activity; e) nausea/vomiting or photophobia/ phonophobia. Gender and age were also assessed by self-report within the survey. Moreover, the number of days with migraine within the last month, age at onset of migraine and intake of prophylactic or acute medication was asked for.
Statistical analyses
Data was analyzed using IBM Statistical Package for the Social Science (SPSS) version 24.0. Sample characteristics were analyzed using standard methods of descriptive statistics. The first analysis was a cultural comparison using t-test for independent samples for the different constructs, checking for differences of mean values for the cultural groups Japan and Germany. The second analysis checked the strength of the relationship between the dependent and independent variables within the groups for Japan and Germany, assessed by Pearson correlation. All tests of significance were conducted at the level of significance α = .05 (two tailed).
Based on a multiple linear regression, a moderator analysis was conducted using the affiliation to the cultural group as moderator. The interaction term was formed by multiplying both scales (suppression and reappraisal) with the affiliation to the group. Moderator variables were tested as well by using a partial correlation. The first model tested whether the affiliation to a cultural group (Japan and Germany, respectively) had any influence on the correlation between emotion regulation and the influence of headaches on daily life. Independent variables were both scales of the ERQ and the outcome was HIT-6. Because of the cross-sectional data set, there might be other variables that account for effects. Therefore, a partial correlation was conducted including the following covariates of Japan and Germany respectively: Age, gender, SHAI, the anxiety and depression scales of the HADS, SSS-8.
Results
Participants
In total, 1131 migraineurs (501 Japanese and 630 German) were recruited (see Table 1). The data for 261 Japanese and 347 German participants were available for final analysis (see Figure 1).
Participant flow of Japanese and German participants. Description of the participants, including both cultural backgrounds.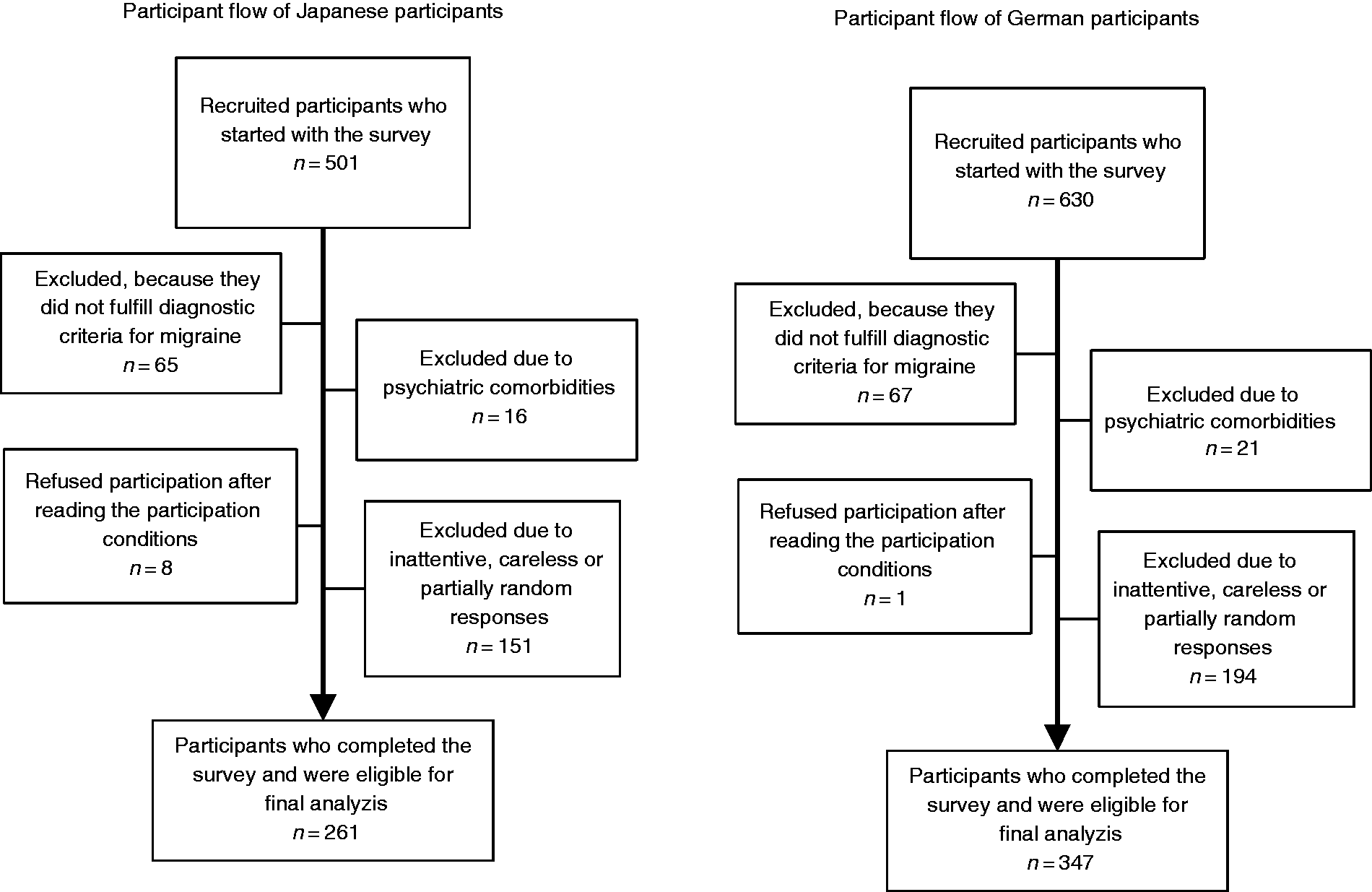

Comparison of Japanese and German participants
There were no group differences found for the SSS-8, HIT-6, SHAI, HADS-D and the frequency and severity of migraine. There was a significant difference in the suppression score of the ERQ in Japan and Germany, with German participants receiving lower scores than Japanese participants. The anxiety scale of the HADS (HADS-A) showed significant differences between Germany and Japan, with German participants receiving higher scores than Japanese participants (see Figure 2 and Table 2). The effect sizes (Cohen’s d) for the HADS-A yielded at d = 0.25 and at d = 0.34 for the suppression scale of the ERQ. This indicates that these effects can be interpreted as small effects.
ERQ Group comparison. Descriptive statistics for the samples of Japan and Germany. t(606) = −4.244, p < .001. t(597) = 3.06, p = .002. ERQ: Emotion Regulation Questionnaire; HADS-A: Hospital Anxiety and Depression Scale, anxiety sub-scale; HADS-D: Hospital Anxiety and Depression Scale, depression sub-scale; HIT-6: Headache Impact Test; SSS-8: Somatic Symptom Scale 8; SHAI: Short Health Anxiety Inventory; NRS: Numeric Rating Scale 0–4.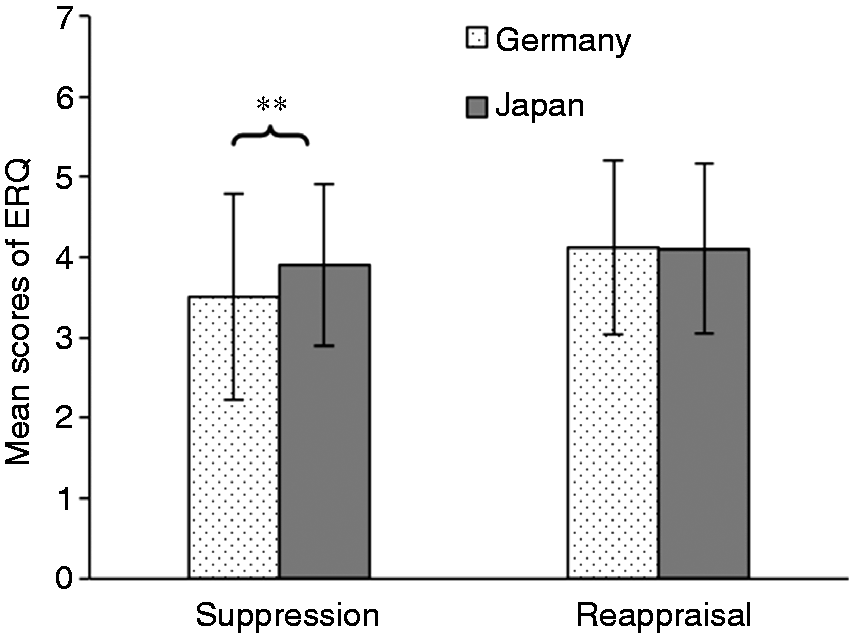

Within-group correlations
Pearson correlation matrix for Japanese (a) and German (b) participants.

Correlation is significant at the 0.05 level (two-tailed).
Correlation is significant at the 0.01 level (two-tailed).
ERQ: Emotion Regulation Questionnaire; HIT-6: Headache Impact Test; SSS-8: Somatic Symptom Scale 8.
Moderator analysis
The regression model showed an R2 score of R2 = .244, F(9) = 20.37, p < .001.
This means that 24.5% of variance of the independent variable can be explained by the moderators and covariates. Under the usage of the covariates SHAI, SSS-8, age, HADS-A, HADS-D and gender, the regression model showed that the affiliation to one cultural group did not moderate the correlation between emotion regulation (ERQ) and impact of the migraine disorder on daily life (HIT-6).
The second regression model showed an R2 score of R2 = .208, F(10) = 14.82, p < .000. This means that 20.8% percent of variance of the independent variables can be explained by the moderators and covariates. Similar to the results in the first model, the affiliation to a cultural group did not moderate the correlation between emotion regulation (ERQ) and the days with migraine per month and pain intensity of migraine headaches. Also, in both models no significant interaction was shown between the suppression scale of ERQ and Group.
Discussion
This is the first study addressing a direct comparison of emotion regulation strategies and migraine complaints in German and Japanese headache patients. Emotion regulation is of major concern in everyday life. Supposedly, it affects the human system and has influence on the human body (4–11). Therefore, we searched for an empirical answer to how strong this impact is, considering a within-group correlation of headache patients. Furthermore, our study scrutinized culture-related differences.
In the cultural group comparison, the study shows minor differences regarding complaints and symptoms between Japanese and German headache patients. Significant differences were observed for the levels of anxiety, whereby German participants showed higher levels of anxiety than Japanese participants. Significant differences were also observed for the suppression scale for the ERQ, with Japanese patients showing more emotion suppression.
Even though the groups differed significantly from each other, the amount of emotion regulation of the within-group correlation did not show any significant influence of emotion regulation on headache complaints either in the Japanese group or in the German group. Nevertheless, there is a weak negative relationship between the suppression scale of ERQ and SSS-8 in Japan, which means that higher levels of suppression are associated with fewer additional somatic symptoms.
That Japanese participants show more emotion suppression is not surprising, because emotion regulation is a big part of Japanese culture (29). Every culture has its own rules regarding both the expression and the control of feelings. The construct of individualism and collectivism can thus explain cultural differences in the way people express their feelings. For instance, individualistic cultures such as that in Germany display on average greater variance in emotional expressions than collectivistic cultures such as that in Japan (30). Studies show that high arousal emotions and the expression of emotions are more valued in Western countries, whereas low arousal emotions and controlling these emotions is considered to be more desirable in Asian civilizations (31). A small but significant difference was observed in the anxiety scale of the HADS, with German participants scoring higher than Japanese participants. Previous studies have shown that anxiety does not have such a big impact on Japanese participants (32).
The scores for the anxiety scale of the HADS lie above average with a score of 7.90 for the German group and 6.97 for the Japanese group.
The recommended cut-off scores for doubtful cases range from 8–10 points (18,33), so both groups of headache patients score at the upper end of normality. This fact is backed up by several other studies that all show how migraine and anxiety correlate (34,35). All other measurements (HADS-D, SHAI, HIT-6 and SSS-8) and frequency and severity of migraine do not differ significantly from each other. Apparently, both German and Japanese groups of headache patients are quite homogenous.
That higher levels of suppression are associated with fewer additional somatic symptoms results in the hypothesis that emotion suppression has fewer physical effects on Japanese participants than on German participants. This would be in agreement with another recent study, which shows that the suppression of emotions leads to a lower physical response and fewer physical symptoms in Asian participants (13). However, it needs to be taken into consideration that only the most common psychosomatic symptoms are asked about in the SSS-8 and, in this regard, other factors are feasible as contributing to this correlation.
Implications for the treatment of migraine
Results of this study suggest that Japanese patients experience migraine complaints to a comparable extent to German patients. Only the differences with respect to emotion regulation techniques and the differentiated emphasis of anxiety have to be kept in mind.
Emotion regulation seems to play a minor role in the development and maintenance of migraine as it is shown that there is no correlation between emotion regulation and headache complaints. Consequently, the focus on individual reaction patterns to stress under consideration of sensory stimulus processing is advisable.
The strengths of the present study are the balanced high number of participants in both countries who were recruited via the same procedure and who were evaluated with the same validated instruments. Baseline characteristics of the two cohorts did not differ significantly in main epidemiological or headache-related items and data were collected using an online survey. This method of data collection guarantees high accuracy and a sensitive selection of participants, because careless responses will automatically be detected. Furthermore, unwanted effects of social desirability can be bypassed.
The present study has some limitations. Firstly, it is difficult to compare Western psychological data surveys with Japanese participants, who might demonstrate a different response behavior. Studies have shown that Japanese participants show a tendency towards more critical self-evaluation than Western participants. Therefore, the comparability to German participants could be restricted (36).
The high rate of excluded participants appeared to be due to strict exclusion criteria. In order to safeguard the quality of the data, the online survey program automatically detected random or inattentive response behavior and excluded the respective participants. Moreover, we excluded participants who did not fulfill the criteria of migraine and who reported acute psychiatric comorbidities. This intention to only include diligent participants also comes with the disadvantage that a high number of participants were rejected and therefore the generalizability is reduced. Also, the self-report of psychiatric disorders bears the risk of a response bias and wrong answers due to the participant’s lack of awareness of a current mental disease.
With respect to data collection and the evaluation of emotion regulation, instead of the generic questionnaire (ERQ) used here, an elaborated test procedure could be used. For example, the response behavior regarding emotion-triggering stimuli could be measured directly. In this way, an enhanced specificity could be achieved. Furthermore, the online survey used self-report measurements for the initial check of migraine disorder and for the questionnaires. In general, self-report measurements bear the risk of a response bias with regard to a liberal or conservative response behavior as well as a different interpretation of the questions, especially with respect to rating scales (37). These questionnaires rely on the introspective ability of the participant and therefore can lack accuracy.
Even though both clinical patients and participants who were not in treatment were included in the survey, the former prevailed in number. As a consequence, mainly participants who showed a higher headache frequency (an average of eight attacks per month) and participants who reported a high burden of their headaches in everyday life were included (HIT-6 score over 60). Also, the prevalence of patients who take preventive drugs is relatively high due to recruitment in a clinical setting and might not be representative of the general German and Asian populations of persons with migraine complaints. Due to the use of preventive drugs, migraine complaints might be not as strong and therefore the effect of emotion regulation might be less visible. So, in order to increase general validity, participants with a lower occurrence of migraine complaints should also be included. Finally, it is to be noted that the German and Japanese participants are only single representatives of Western and Asian participants. A comparison from different Western or Asian countries might result in deviating results.
Because there is no general, validated survey to assess aura status we did not assess the presence of aura within the survey. However, future research should take aura into consideration, because the association between mood disorders and migraine complaints might be increased in migraine patients with aura symptoms (34,38).
Article highlights
The study compares emotion regulation and migraine related complaints in German and Japanese headache patients. Japanese headache patients show a significantly higher amount of emotion suppression and significantly lower levels of anxiety than German migraine patients. The amount of emotion regulation is not associated with headache complaints.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JW received research grants from the German Migraine and Headache Society (DMKG) and the Faculty of Psychology and Neuroscience of Maastricht University, The Netherlands. CG received honoraria for consulting and lectures within the past 3 years from Allergan Pharma, Ratiopharm, Boehringer Ingelheim Pharma, Lilly, Novartis Pharma, Desitin Arzneimittel, Cerbotec, Bayer vital, Hormosan Pharma, electroCore, Grünenthal, Reckitt Benckiser, and TEVA. He does not hold any stocks of pharmaceutical companies or medical device companies. No potential conflict of interest was reported by DD, LV, TT and HY.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a research grant of the German Migraine and Headache Society (DMKG) and by a grant of the Faculty of Psychology and Neuroscience of Maastricht University, the Netherlands.