
Abstract
Introduction
Migraine and vasovagal syncope are comorbid conditions that may share part of their pathophysiology through autonomic control of the systemic circulation. Nitroglycerin can trigger both syncope and migraine attacks, suggesting enhanced systemic sensitivity in migraine. We aimed to determine the cardiovascular responses to nitroglycerin in migraine.
Methods
In 16 women with migraine without aura and 10 age- and gender-matched controls without headache, intravenous nitroglycerin (0.5 µg·kg−1·min−1) was administered. Finger photoplethysmography continuously assessed cardiovascular parameters (mean arterial pressure, heart rate, cardiac output, stroke volume and total peripheral resistance) before, during and after nitroglycerin infusion.
Results
Nitroglycerin provoked a migraine-like attack in 13/16 (81.2%) migraineurs but not in controls (p = .0001). No syncope was provoked. Migraineurs who later developed a migraine-like attack showed different responses in all parameters vs. controls (all p < .001): The decreases in cardiac output and stroke volume were more rapid and longer lasting, heart rate increased, mean arterial pressure and total peripheral resistance were higher and decreased steeply after an initial increase.
Discussion
Migraineurs who developed a migraine-like attack in response to nitroglycerin showed stronger systemic cardiovascular responses compared to non-headache controls. The stronger systemic cardiovascular responses in migraine suggest increased systemic sensitivity to vasodilators, possibly due to insufficient autonomic compensatory mechanisms.
Keywords
Introduction
Migraine is a common, paroxysmal headache disorder with a complex pathophysiology (1,2). The exact role of the vasculature is a matter of debate (3). Some studies have suggested ictal (4) and interictal (5) functional changes in the systemic circulation in migraine. Interestingly, migraineurs also have an increased rate of vasovagal syncope (VVS) (6,7), which partly explains the white matter abnormalities found in a population-based study (7).
Syncope is transient loss of consciousness due to cerebral hypoperfusion (8,9) and also occurs often in the general population (8,10). In population-based studies, compared to non-migraine controls, more individuals with migraine had ever had syncope (11), frequent syncope (>5 attacks per lifetime) (6) and orthostatic intolerance (6) in between attacks. Syncope can also occur during migraine attacks (12). One third of people with unspecified syncope have migrainous features during episodes of syncope (13). Vasovagal syncope (VVS) is the most likely mechanism for syncope in migraineurs. VVS can be provoked with a tilt table test, which relies on a susceptibility to hypotension in the vertical position (14). Administration of a systemic vasodilator such as nitroglycerin increases the incidence of tilt-induced VVS, likely due to increased venous pooling (14). Nitroglycerin may also provoke migraine attacks, but only in migraineurs (15). Nitroglycerin is de-nitrated to nitric oxide (NO) and vasoactive S-nitrosothiols. Both substances cause vasodilation through activation of cytoplasmic guanylate cyclase, which increases intracellular guanosine-3’,5’-monophosphate (cGMP) and cytosolic calcium (15). NO provokes migraine attacks either directly or indirectly through the NO-activated intracellular cascade (15).
Taken together, the systemic circulation of individuals with migraine seems abnormally susceptible to nitroglycerin. In this study, we assessed whether this response is indeed different in relation to a forthcoming migraine attack.
Methods
Participants
Baseline characteristics of study population.

Note: Baseline characteristics of migraine and non-headache control participants. Continuous variables are depicted as mean ± SD. MO: migraine without aura; n.c: not calculable.
Fisher’s exact probability test.
Study procedure
After screening, eligible individuals were invited to the hospital. After overnight fasting, nitroglycerin was administered. Clinical features and cardiovascular and clinical parameters were monitored continuously immediately before (during 10 min), during (20 min) and immediately after (10 min) nitroglycerin infusion. Headache severity was scored throughout the experiment using a visual rating scale, ranging from ‘0’ (no headache) to ‘10’ (most severe headache). Migraine participants were investigated at least 3 days after a previous migraine attack. All measurements were performed by a single investigator (WPJvO) in a quiet, temperature-controlled room with the participants lying comfortably in the supine position.
Administration of nitroglycerin
Nitroglycerin (0.5 µg·kg-1·min-1 infusion for 20 minutes via cannulation of the antecubital vein in both the control and migraine group) was used to trigger migraine-like attacks in the migraine group (15). This model is widely used and has good reproducibility and reliability (15,19). Infusion of nitroglycerin results in an immediate non-migraine headache in healthy individuals and migraineurs, followed by a migraine-like attack 4–6 hours after infusion in migraine patients but not in controls (19,20).
Photoplethysmography
Continuous finger blood pressure measurements were performed with a Finometer Pro (Finapres Medical Systems BV, Amsterdam, The Netherlands; model 1; 2003.126). This is a reliable non-invasive beat-to-beat blood pressure measurement device using photoplethysmography, enabling analysis of blood pressure (mean arterial blood pressure; mmHg), cardiac output (L·min−1), total peripheral resistance (mmHg·(L·min−1)−1), stroke volume (L), and heart rate (beats·min-1) (21,22). These parameters were obtained using the Beatscope software program (Finapres Medical Systems BV, Amsterdam, The Netherlands). The cuff was placed on the right index finger and the height correction system of the device was active during the whole measurement period, with participants keeping their arms immobilised in a sling with the hand above the heart. The participants were supine and at rest for 5–10 minutes before measurements started. We transformed beat-to-beat photoplethysmography data to averages per minute. The original continuous data were inspected for artefacts (WPJvO; JGvD), for instance due to talking, movements or coughing, in which case the results of that minute were treated as missing values.
Standard protocol approvals, registrations, and patient consents
The study was conducted as part of the Leiden University Medical Center Neuro Analysis Programme (LUMINA) (18). LUMINA and the present study were approved by the local medical ethics committee. All participants provided written informed consent prior to participation. Individual participants can not be recognised based on data published in this manuscript.
Statistics
Student’s t-test was used to compare continuous, normally distributed variables, and Fisher’s exact test for categorical data. Where appropriate, non-parametric tests were applied. Data were analysed in two ways: by ANCOVA (between-group comparison of pre-, during and post-infusion block averages; adjusted for age) and by a generalised estimating equations (GEE) model (between-group comparison of 1-minute averages during the nitroglycerin infusion period; repeated measurements). The primary analysis was the comparison between migraine participants in whom an attack developed after nitroglycerin versus control participants. Group (migraine and control), time (the 1-minute average), and group*time interaction were included in the model. In a further explorative analysis, we assessed whether the cardiovascular response to nitroglycerin depended on the propensity of nitroglycerin to provoke a migraine attack in migraine subgroups. Analyses were performed using SPSS 23.0 (SPSS inc., IBM, USA). The statistical threshold was set to p < .05.
Data availability statement
All data, methods and materials used to conduct this research are mentioned in this article. Research materials related to this paper can be accessed upon request to the authors.
Results
Clinical characteristics
Baseline characteristics of migraine and control participants did not differ (Table 1).
Baseline measurements
Cardiovascular parameters in control participant and in migraineurs (in whom an attack developed), during and after nitroglycerin infusion.

Estimated means ± SE (ANCOVA, adjusted for age) are depicted. M: migraineurs; C: controls; MAP: mean arterial pressure (mmHg); HR: heart rate (beats·min−1); CO: cardiac output (L·min−1); TPR: total peripheral resistance (mmHg·(L·min−1) −1); SV: stroke volume (ml beat−1). Bold indicates p < .05.
Effects of nitroglycerin on migraine attacks and syncope
Both migraine and control participants reported a mild to moderate headache during infusion of nitroglycerin (Figure 1), with a similar peak intensity (2.0 ± 2.5 points vs. 1.4 ± 1.8; p = .10) and no difference in time of onset of headache between groups (group*time interaction: p = .30). Thirteen of the 16 (81.3%) migraineurs developed a migraine attack versus none of the controls (0%; Fisher’s exact test p = .0001), with a mean ± SD of 314 ± 126 minutes (median 270 minutes; range 155–600 minutes) after NTG administration. The six migraineurs in whom a migraine-like attack occurred within 270 minutes after infusion were labelled the ‘early attack’ group. The seven migraineurs who developed a migraine-like attack >270 minutes after infusion were labelled the ‘late attack’ group. No syncope was provoked.
Headache severity in the nitroglycerin provocation experiment. Both the migraine and the control group reported mild-moderate headache during nitroglycerin infusion (time 0–20 min).
Effects of nitroglycerin in migraineurs in whom an attack developed
Analyses of block averages showed that mean heart rate was higher in migraine participants (in whom an attack developed later) during infusion of nitroglycerin as compared to controls (p = .001; Table 2). The time-series analysis, using 1-minute averages, showed that stroke volume, cardiac output and mean arterial pressure decreased during infusion, whereas heart rate and total peripheral resistance increased (all p < .001) in both groups. For all parameters, but especially for total peripheral resistance, stroke volume and heart rate, nitroglycerin-induced changes were more pronounced in migraine participants compared to controls (p < .001 for group*time interaction in the analysis of each of the five outcome parameters). We observed a faster and more prolonged decrease in stroke volume and cardiac output in the group of migraineurs compared to the control group. Total peripheral resistance, after a slight increase, steeply decreased in the migraine group as compared to a small and stable increase in the control group. Mean arterial pressure decreased in both groups, albeit after an initial small increase in the migraine group. Heart rate increased in both groups but more so in the migraine group (Figure 2).
Cardiovascular responses during the course of nitroglycerin infusion in control participants and in migraineurs in whom a migraine attack developed. Time-series analysis showed that the minute-to-minute response to nitroglycerin differed between migraineurs and controls for several cardiovascular parameters. Graphs depict estimated means with 1 standard error as error bar. (a) Total peripheral resistance; (b) Stroke volume; (c) Cardiac output; (d) Mean arterial pressure; (e) Heart rate.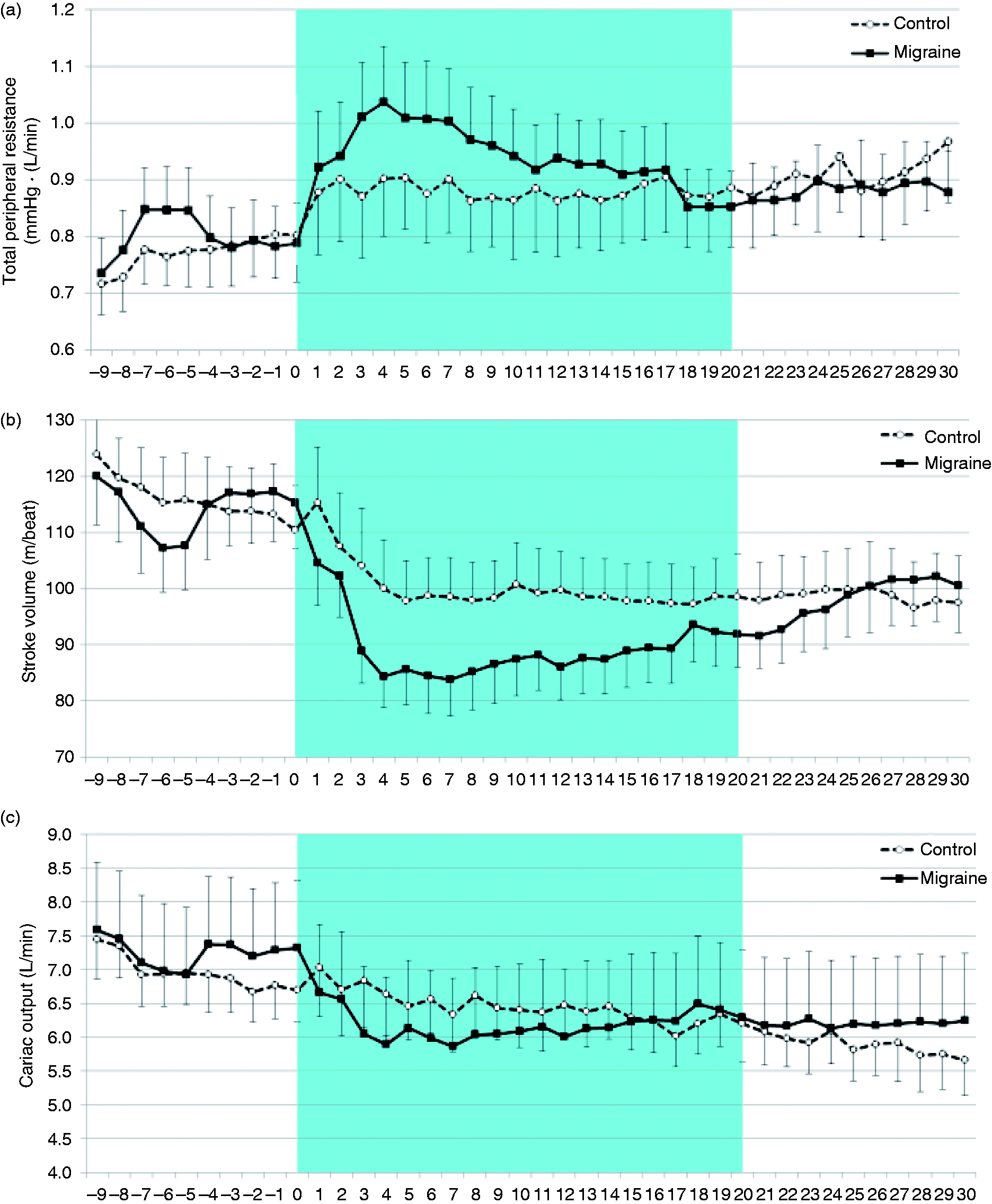
Effects of nitroglycerin in migraine attack onset subgroups
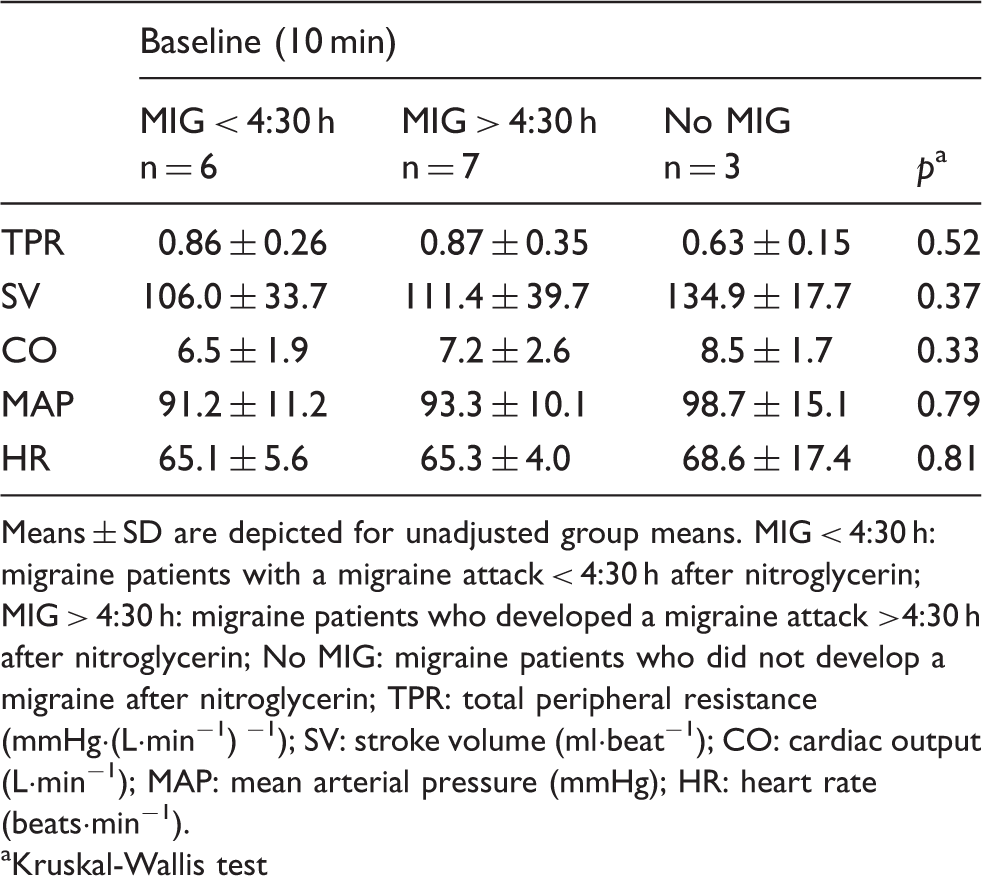
We compared the ‘early attack’ group with the ‘late attack’ and ‘no attack’ groups in an exploratory manner, due to the very small numbers per subgroup. The analyses suggested differences in cardiovascular responses between migraine participants who developed an attack versus those who did not (Table 3; Figure 3). These parameters reacted in the same general pattern during administration of nitroglycerin: those who later had an attack tended to have a lower baseline stroke volume (p = .051) and cardiac output (p = .048). However, our study was not powered to detect any differences. Post-hoc calculation shows that with a sample size of six per group stroke we only had a power of 0.39 to detect a 50% difference in effect size.
Cardiovascular response profiles during nitroglycerin infusion in migraine subgroups based on time-to-onset of the migraine attack. Time-series analysis showed that the minute-to-minute response to nitroglycerin differed between migraineurs, classified in three groups based on time-to-onset of migraine attack. Graphs depict estimated means. Reported p values indicate overall level of significance (ANOVA-based). Superscript letters indicate post-hoc differences (LSD; p < .05) between early attack and no attack groups (a), and between late attack and no attack groups (b). (a) Total peripheral resistance; (b) Stroke volume; (c) Cardiac output (d) Mean arterial pressure; (e) Heart rate. Differences in baseline cardiovascular parameters between different migraine subgroups in relation to time-to-onset of migraine-like attack after NTG administration. Means ± SD are depicted for unadjusted group means. MIG < 4:30 h: migraine patients with a migraine attack < 4:30 h after nitroglycerin; MIG > 4:30 h: migraine patients who developed a migraine attack >4:30 h after nitroglycerin; No MIG: migraine patients who did not develop a migraine after nitroglycerin; TPR: total peripheral resistance (mmHg·(L·min−1) −1); SV: stroke volume (ml·beat−1); CO: cardiac output (L·min−1); MAP: mean arterial pressure (mmHg); HR: heart rate (beats·min−1). Kruskal-Wallis test
Discussion
We tested the hypothesis that the systemic responses to nitroglycerin differ between non-headache controls and migraineurs with a forthcoming attack. Using continuous photoplethysmography, we showed that intravenous nitroglycerin administration induced a faster and more prolonged decrease in stroke volume and cardiac output, a steep decrease in total peripheral resistance after an initial increase, a slightly higher mean arterial pressure, and a sustained increase in heart rate in migraine participants in whom an attack developed later. The most pronounced differences occurred in those migraine patients in whom an early attack developed, whereas the changes were less marked in the three patients in whom no attack developed. The enhanced response of the systemic circulation to nitroglycerin in migraineurs suggest that the systemic vasculature is more susceptible to its (vasodilatory) effects.
Normal circulatory physiology consists of complex feedback mechanisms regulating blood pressure, maintaining adequate tissue perfusion throughout the body (for more details see Figure 4). Some of the differences in cardiovascular responses to nitroglycerin (the overall lower stroke volume, cardiac output, mean arterial pressure and steep decrease in total peripheral resistance after initial increase) that we have reported in this study suggest insufficient compensatory mechanisms to nitroglycerin-induced vasodilation in the migraine group. Interestingly, the mechanism described here in migraineurs is similar to the mechanism described in individuals with VVS who are exposed to nitroglycerin during head-up tilt (23) (Figure 4). Our data suggest that migraineurs have more venous pooling of blood and altered (arteriolar) total peripheral resistance after nitroglycerin in the supine position. Since some of the participants in both groups had had VVS in the past (year), we cannot exclude that the results might in part be due to VVS rather than to migraine itself. Subgroups in this study were too small to run separate analyses and further research is warranted to investigate this.
Normal circulatory physiology and cardiovascular responses to nitroglycerin in individuals with migraine and vasovagal syncope. Blood pressure depends on cardiac output (CO) and on the total peripheral (arteriolar) resistance (TPR): Blood pressure = CO × TPR (neglecting central venous pressure). Mean arterial pressure then is the average blood pressure during one cardiac cycle and is approximated by the sum of 2/3 × diastolic blood pressure and 1/3 of the systolic blood pressure. In turn, cardiac output (CO) is the product of the volume of blood pumped out by the heart per beat (stroke volume; SV) and heart rate (HR): CO = SV × HR. Blood pressure is therefore proportional to heart rate, stroke volume and total peripheral resistance. RA: right atrium; LA: left atrium; RV: right ventricle; LV: left ventricle; CV: circulating volume.
Theoretically, the effects could be due to changes in only one circulatory compartment; for example, the cerebral circulation. However, as cerebral blood flow comprises approximately 15–20% of the cardiac output and is tightly regulated to meet the brain’s metabolic demands (24), our findings suggest involvement of the entire systemic circulation. It is speculative whether the change in systemic circulation might also cause a change in cerebral circulation. Photoplethysmography can unfortunately not distinguish between cerebral and non-cerebral parts of the peripheral vasculature. We can therefore only speculate to what extent our findings reflect changes in the cranial vessels. How much of the total peripheral resistance is based on the cranial vasculature is unknown. It is debated whether or not nitroglycerin may induce transient vasodilatation of extracranial vessels in migraine patients and non-headache individuals (25–27). If so, at least part of the decrease in total peripheral resistance could be due to cranial vasodilatation. Future studies should distinguish between these cerebral and systemic effects to further elucidate the underlying mechanisms.
Nitric oxide donors have a regulatory effect on vascular smooth muscle tone, but we cannot exclude a neuromodulatory effect of nitroglycerin within the central and peripheral nervous system (28). It is therefore likely that its cardiovascular actions are not only confined to direct effects on blood vessels (29,30).
The strengths of our study include the use of the standardised nitroglycerin provocation model (15,19,20), identical study protocols for patients and controls, and a homogenous study group. Furthermore, continuous monitoring of cardiovascular parameters before, during and after NTG infusion has not been reported before, according to our knowledge. Although the inclusion criteria improve group homogeneity and interpretability of results, we are aware that they might limit generalisation of our results to males or migraine with aura patients, as cardiovascular functioning and cardiovascular disease are gender dependent (31).
Only a few studies have investigated cardiovascular parameters in migraine (32–35). Sublingual nitroglycerin induced increases in heart rate but no decreases in total peripheral resistance (35). In a population-based study, higher diastolic and lower systolic blood pressures were found, while mean arterial pressure was normal (32). However, these and other cardiovascular parameters (cardiac output, heart rate, total peripheral resistance) did not differ in case-control studies (5,33,34), in which blood pressure was measured with upper arm cuffs, and only at baseline (no headache) conditions. The findings are nevertheless in agreement with our baseline data. Only one other experimental study reported on the cerebral vascular effects of nitroglycerin infusion in migraine, reporting a higher arterial sensitivity (reflected by higher middle cerebral artery blood flow velocities) to infusion as compared with healthy controls (36).
We can only speculate about underlying mechanisms explaining the differences in the magnitude of the cardiovascular responses to nitroglycerin. Hypothesising on underlying explanations, a stronger response of the systemic or cerebral vasculature might induce a migraine attack, but currently cerebral vasodilation is mostly regarded as an epiphenomenon in migraine (1). Secondly, the systemic effect might occur independent of the migraine-inducing effects, both caused by one underlying mechanism. Sensitivity to nitric oxide (NO) may be enhanced, possibly due to higher perivascular concentrations of NO synthase (37). NO is directly and further downstream implicated in neurogenic (central sensitisation; pain transmission) and vascular (vasodilation) mechanisms (15,37). Since our study was not powered to detect the possible differences between attack-onset subgroups, future studies could be developed to investigate these differences further.
There is a growing interest in the biological functions of the nitrate-nitrite-nitric oxide pathway, and specifically the notion that the nitrate and nitrite anions, previously considered inert, can be recycled in vivo to form nitric oxide. It highlighted the possible therapeutic potential for this pathway, in particular in hypoxic states (38), and has already resulted in the first clinical studies in stroke (39). We could postulate that migraine patients respond better to this effect, as we have shown that they have increased systemic cardiovascular sensitivity to nitric oxide.
Although we showed enhanced systemic cardiovascular responses to nitroglycerin in migraineurs, important remaining questions are whether this stronger response is due to migraine itself or to a concomitant susceptibility to VVS, and what exactly is happening with the cerebral circulation during nitroglycerin triggering.
Clinical implications
Migraine and vasovagal syncope are comorbid conditions that may share part of their pathophysiology through autonomic control of the systemic circulation. We found that intravenous nitroglycerin administration induced stronger systemic cardiovascular responses in migraine patients in comparison to controls. The enhanced response of the systemic circulation to nitroglycerin in migraineurs suggests that the systemic vasculature is more susceptible to its (vasodilatory) effects.
Footnotes
Acknowledgements
The authors would like to thank Cor G.S. Kramer and Robert H.A.M Reintjes, technicians, for their cooperation and aid in pre-processing of the data, and Dr. Erik W. van Zwet, consultant in medical statistics, for his aid in the data analysis.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: WPJvO, GGS, DS, JGvD have nothing to disclose. RDT reports grants from Netherlands Organization for Scientific Research, Medtronic, Dutch Epilepsy Fund, AC Thomson Foundation, Nuts OHRA fund, and speakers fee for UCB Medtronic and GSK during the conduct of the study. MDF reports grants from Netherlands Organization for Scientific Research, grants from European Commission, during the conduct of the study
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Netherlands Organization for Scientific Research (Spinoza 2009 to M.D.F.) and the European Commission (FP7-EUROHEADPAIN - no. 602633 to MDF). They had no role in the design or conduct of the study.
Statistical analysis
The primary author (WPJvO) has conducted the statistical analysis in conjunction with EWvZ, an academic medical statistician.