
Abstract
Background
Migraine is associated with syncope. We investigated risk factors for syncope and burden of syncope in migraine patients.
Methods
Participants were recruited from a headache clinic. All participants provided information on lifestyle, co-morbidity, syncope, headache and suicide, and completed the MIDAS and HADS questionnaires. Genetic data were available for a subset of participants. Risk of syncope in relation to participant’s characteristics and migraine susceptibility loci, and risks of psychological disorders associated with syncope, were calculated using logistic regression.
Results
Underweight, regular tea intake, diabetes mellitus, and migraine with aura were associated with increased syncope risks, with adjusted ORs of 1.76 (95% CI 1.03–3.03), 1.84 (95% CI 1.22–2.79), 4.70 (95% CI 1.58–13.95), and 1.78 (95% CI 1.03–3.10), respectively. Preliminary results showed that rs11172113 in LRP1 was associated with syncope risks. Comorbid syncope in migraine patients was associated with increased risks of depression (OR 1.95, 95% CI 1.18–3.22) and suicide attempt (OR 2.85, 95% CI 1.48–5.48).
Conclusion
Our study showed the potential roles of vascular risk factors in the association between migraine and syncope. Modifiable risk factors for syncope in patients with migraine include body mass index and tea intake. The debilitating psychological impact of co-morbid syncope in migraine patients warrants clinical attention of treating physicians.
Keywords
Introduction
Syncope has been listed as one of many symptoms commonly found in patients with migraine (1). In a Dutch population-based study, the prevalence of lifetime syncope was higher in migraine patients than healthy adults (46% vs. 31%) (2). When compared with individuals without migraine, studies have shown that patients with migraine have 1.9 to 2.7 times increased risk of syncope (2,3). The high co-occurrence of migraine and syncope suggests that there may be a common disease etiology between them. A meta-analysis of large genetic studies supported vascular etiologies of migraine pathophysiology, while one of our prior studies provided some evidence for endothelial dysfunction in migraine patients with syncope, suggesting that syncope may be associated with vascular dysfunction in migraine (4,5).
Although syncope is a self-limiting condition, it has been shown that it is associated with marked psychosocial and physical impairment (6). Studies have also shown that patients with migraine suffer from substantial disability related to poor physical and psychological health as well as diminished quality of life (7–9). Whether the risks of disability and psychological disorders were magnified in patients with both migraine and syncope remains unclear. In addition, syncope was shown to be associated with a high load of deep white matter lesions, which are predictive of subsequent stroke and dementia, making it important that risk factors for syncope be identified (10,11).
This study aimed to identify risk factors for syncope and to examine psychosocial impairment associated with comorbid syncope in migraine patients. We report an analysis on risk factors for syncope which were associated with vascular dysfunction from three domains: Personal characteristics, basic headache profiles, and genes. We also report the risks of disability, psychological disorders, and suicide associated with comorbid syncope in migraine patients.
Methods
Participants
Between 1 April 2015 and 30 March 2018, patients who consecutively attended the headache clinic in Taipei Veterans General Hospital with newly diagnosed migraine were recruited into this study. All participants completed questionnaires, which asked, among other issues, about basic demographic, lifestyle, comorbid health conditions, suicide, headache profiles, migraine-related disability, and psychological health (see data collection). We excluded participants if they had a reported history of head trauma or epilepsy prior to recruitment into this study, because these participants may report conditions that mimic syncope but are not true syncope.
Diagnosis of migraine and definition of syncope
Diagnosis of migraine and by subtypes (migraine with aura) was made according to the International Classification of Headache Disorders, 3rd edition, beta version (ICHD-3β) criteria (12). Definition of syncope was explained to all participants with the standard statement as “a brief loss of consciousness that may be provoked by prolonged standing in the heat or sight of blood but it usually occurs without a clear provocation, and that it does not include unconsciousness caused by head trauma, stroke, heart attack or epileptic seizure”. Participants were asked to indicate whether they had syncope in the past 12 months.
Data collection
Each participant recruited into the study was given a study questionnaire, the Migraine Disability Assessment (MIDAS) (13), and the Hospital Anxiety and Depression Scale (HADS) questionnaires (14). The study questionnaire collected information on age (continuous), sex (men, women), height (continuous) and weight (continuous) (and derived body mass index [BMI]), dominant hand (right, left), education level (illiterate, elementary school, junior high school, high school or vocational school, undergraduate, post-graduate), marital status (single, married and living with a partner, married and not living with a partner, divorced, widowed), occupation (unemployed, retired, housewives, student, civil workers, military, farmers, industrial workers, office workers, self-employed, others), ancestral home town (open question), lifestyle characteristics such as current smoking (no, yes), current alcohol drinking (no, yes), regular tea and/or coffee intake (no, yes), coke intake or intake of other caffeinated drinks (no, yes), and 14 comorbid health conditions; that is, hypertension (no, yes), thyroid disorders (no, yes), mitral valve prolapse (no, yes), cyclic vomiting disorder (no, yes), epilepsy (no, yes), asthma (no, yes), head trauma (no, yes), diabetes mellitus (no, yes), Raynaud’s disease (no, yes), diarrhea (no, yes), cervical spinal disorders (no, yes), recurrent stomachache/abdominal pain (no, yes), glaucoma (no, yes), and irritable bowel syndrome (no, yes). The study questionnaire has a section for headache, comprising questions, which was designed to collect headache profiles according to the ICHD-3β diagnostic criteria (12), including information on headache frequency (days/month [d/mo]), intensity (Numerical Rating Scale [NRS] 0–10), duration, location, aura symptoms, and other headache characteristics. The study questionnaire also included a section for syncope, which was used to collect information, from those who indicated having syncope, on frequency and triggers of syncope as well as age of onset. All participants also completed the MIDAS (13) and the HADS (14) questionnaires for evaluation of their current level of disability related to migraine and psychological health, respectively. Participants were also asked to indicate whether they ever had suicidal ideation and/or suicide attempt. The information on syncope, disability, psychological health, and suicide was further verified by neurologists seen by the study participants.
Some (but not all) participants of the current study also participated in a case-control genome-wide association (GWA) study for identification of migraine susceptibility genes in Taiwan (15). The GWA study found two novel migraine susceptibility loci (genes), rs655484 (in DLG2) and rs3781545 (in GFRA1), with genome-wide significance in East Asian populations, and successfully replicated findings for two migraine susceptibility loci (genes), rs10166942 (in TRPM8) and rs1172113 (in LRP1), which were reported in GWA studies of European and American populations (5,15). Further details about the study were described elsewhere (15). Data for the four susceptibility loci (genes) for migraine, which was available for a subset of participants in the current study, can be utilized in an exploratory analysis to examine their associations with syncope risks.
Definition of disability and psychological disorders
Disability and psychological disorders in study participants were defined as below: a) Severe disability was defined as having a MIDAS score of 21 and above (13); b) anxiety was defined as having a HADS score for anxiety (HADS-A) score of 11 and above (14); c) depression was defined as having a HADS score for depression (HADS-D) of 11 and above (14).
Standard protocol approvals, registrations, and patient consents
All participants gave written consent to take part in our study, and an ethical approval was obtained from the Institutional Review Board of Taipei Veterans General Hospital. Anonymized information was extracted from the study database for data analysis.
Statistical analysis
Frequency of syncope by characteristics of study participants was presented as number and proportion. For risk factor analysis, we examined the associations between 10 personal characteristics or headache profiles and syncope risks in all study participants using a two-step logistic regression analysis. Initially, risks of syncope (odds ratio [OR] and 95% confidence interval [CI]) in relation to the 10 factors including BMI (underweight: BMI < 18.5; normal: BMI 18.5–24.9; overweight/obese: BMI ≥ 25), alcohol drinking (yes, no), smoking (yes, no), regular coffee intake (yes, no), regular tea intake (yes, no), hypertension (yes, no), diabetes mellitus (yes, no), headache frequency (< 15, ≥ 15 d/mo), headache intensity (NRS < 7, ≥ 7), and migraine with aura (yes, no) were calculated using logistic regression adjusting for age (< 30, 30–39, 40–49, ≥ 50) and sex (men, women). Factors with p < .05 in the age-and-sex-adjusted model were selected for inclusion into a multivariate analysis using logistic regression. The small number of participants with a missing value for each particular variable in the above analyses were assigned a separate category to ensure the same participants were being compared.
For genetic factors, exploratory analyses investigating associations between four migraine susceptibility loci (genes) [rs655484 (in DLG2), rs3781545 (in GFRA1), rs10166942 (in TRPM8), and rs1172113 (in LRP1)](15), and syncope risks were performed in a subset of participants with genetic data. Allele frequency for the four loci between migraine patients with and without syncope were compared, and ORs and 95% CIs for particular risk alleles were calculated. Genotypic associations considering additive (trend), dominant, and recessive models were also examined and ORs and 95% CIs for specific genotypes were calculated using logistic regression.
We also examined psychosocial burdens associated with comorbid syncope in migraine patients. Risk of severe disability (MIDAS ≥ 21), anxiety (HADS-A ≥ 11), depression (HADS-D ≥ 11), suicidal ideation, and suicide attempt in relation to comorbid syncope in migraine patients were calculated using the multivariable logistic regression model.
Statistical significance was defined as a two-sided p of less than .05. All analyses were performed using Stata statistical software version 14.2 (StataCorp, College Station, TX, USA).
Results
Study population and frequency of syncope
Frequency of syncope by characteristic of migraine patients.

Triggers of syncope
Postural change (e.g. getting up from sitting) (43.2%) was the most common trigger of syncope followed by exercise (e.g. running or another sports activity) (19.8%). Other less common triggers of syncope were at the sight of blood (9.9%), getting an injection (5.4%), after a heavy meal (2.7%), and having a shower (1.8%).
Risk factors for syncope
Risk of syncope in relation to demographics, lifestyles, and headache characteristics in migraine patients.
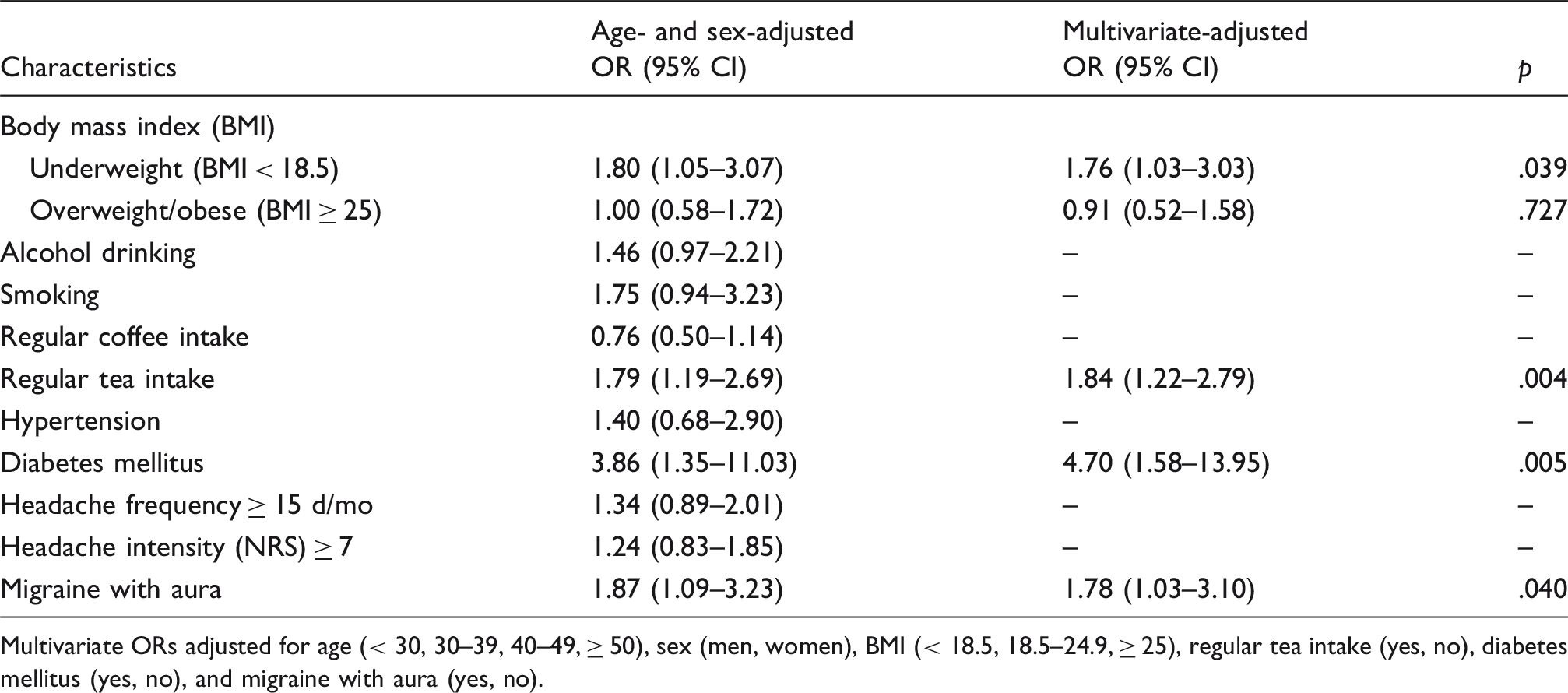
Multivariate ORs adjusted for age (< 30, 30–39, 40–49, ≥ 50), sex (men, women), BMI (< 18.5, 18.5–24.9, ≥ 25), regular tea intake (yes, no), diabetes mellitus (yes, no), and migraine with aura (yes, no).
Risk of syncope in relation to aura, tea intake, underweight, and diabetes in migraine patients.

Multivariate ORs adjusted for age (< 30, 30–39, 40–49, ≥ 50), sex (men, women), and mutually adjusted for BMI (< 18.5, 18.5–24.9, ≥ 25), regular tea intake (yes, no), diabetes mellitus (yes, no), and migraine with aura (yes, no).
There was no participant with diabetes in this category because the number of patients with diabetes was small in our study (n = 23); so participants with any three risk factors were those with aura, regular tea intake, and underweight; synergistic effect of diabetes and other risk factors could not be determined.
Migraine susceptibility loci (genes) and syncope risks
Migraine susceptibility loci (genes) and syncope risks.

Disability and psychological disorders in relation to syncope
In multivariate analysis, comorbid syncope in migraine patients was associated with increased risks of depression (OR 1.95, 95% CI 1.18–3.22), suicidal ideation (OR 1.58, 95% CI 1.04–2.41), and suicide attempt (OR 2.85, 95% CI 1.48–5.48) (Figure 1). The increased risk of suicide attempt (OR 2.64, 95% CI 1.36–5.15) remained significant after adjusting for depression. There were significant trends between an increasing number of comorbid syncope attacks and risks of depression (p = .006), suicidal ideation (p = .017), and suicide attempt (p < .001) (Table 5). Migraine patients with two or more syncope attacks had high risks for depression (OR 2.51, 95% CI 1.17–5.36), suicidal ideation (OR 2.10, 95% CI 1.08–4.07), and very high risk for suicide attempt (OR 5.53, 95% CI 2.36–12.93).
Risk of disability and psychological disorders in relation to syncope in migraine patients. Increasing frequency of syncope attack and risks of depression, suicidal ideation, and suicide attempt in migraine patients. Multivariate ORs adjusted for age (< 30, 30–39, 40–49, ≥ 50), sex (men, women), BMI (< 18.5, 18.5–24.9, ≥ 25), regular tea intake (yes, no), diabetes mellitus (yes, no), and migraine with aura (yes, no).

Discussion
Our study shows that being underweight, having regular tea intake, diabetes mellitus, or migraine with aura are associated with increased risks of syncope in migraine patients. The exploratory genetic analysis shows an association between rs11172113 in LRP1 and syncope risks. Further, we show that comorbid syncope in migraine patients is associated with increased risks of depression, suicidal ideation, and suicide attempt, with a significant trend found between an increasing number of syncope attacks and higher risks. The increased risk of suicide attempt associated with comorbid syncope is independent of depression.
While studies have shown that patients with migraine have an elevated risk of syncope when compared with individuals without migraine (2,3), few have investigated risk factors for syncope in migraine patients. The CAMERA study found that lifetime syncope is more common in female than male migraine patients, and that headache frequency and headache subtypes (with or without aura) are not associated with lifetime syncope risk (2). While the results for sex and headache frequency in our study were similar to the CAMERA study, we found that the risk of syncope in migraine patients with aura is about 1.8 times higher than those without aura. These findings may be explained by endothelial dysfunction associated with migraine with aura. In the US Women’s Health Study, risk of cardiovascular diseases including myocardial infarction and ischemic stroke is increased in migraine patients with aura (non-significant in migraine patients without aura), when compared with women without migraine (16). In one of our prior study, levels of vascular endothelial related-miRNAs such as miR-155 and miR-126 were shown to be associated with frequency of syncope in the past 12 months (4). The mean levels of miRNAs related to angiogenesis and vascular repair were markedly increased in migraine patients with aura compared to those without aura, although they were not statistically significant (4). Migraine patients with aura may be more susceptible to blood pressure drop that manifests as syncope than those without aura as a result of vascular endothelial dysfunction.
Our study also identifies underweight, diabetes, and regular tea intake as independent risk factors for syncope in patients with migraine. While underweight and diabetes were known to be associated with orthostatic intolerance (and also underweight with non-cardiac syncope) (17), the association between regular tea intake and syncope risk is an interesting finding. Although tea contains caffeine, which increases blood pressure transiently in its consumers (18), it also contains some blood-pressure lowering polyphenols (19). Observational studies have shown associations between tea intake and lower systolic and/or diastolic blood pressure (19,20), and between habitual tea intake and decreased risk of hypertension (21). Therefore, tea may predispose migraine patients to syncope when consumed regularly, especially in underweight migraine patients and underweight migraine patients with aura, who were shown to be more susceptible to syncope (Tables 2 and 3). Putting the possible mechanisms for the associations shown here between risk factors and syncope in context, we hypothesize that vascular dysfunction may play a major role in the pathogenesis of syncope in migraine patients. More studies are warranted to examine the association between these factors and syncope risks in migraine patients as well as to investigate the mechanisms behind the observed association.
In an exploratory analysis in this study, we found some evidence for an association between rs11172113 in LRP1 (risk allele C) and increased syncope risks. A meta-analysis of 22 GWA studies including 375,000 study participants showed strong evidence for an association between rs11172113 in LRP1 and risk of migraine (p = 5.6 × 10−49) in European and American populations, and one of our prior study also showed an association between this locus and risk of migraine in a GWA study in Taiwan (permutation p = .029). (5, 15) The findings on rs11172113 in LRP1 and risks of migraine and syncope indicate the presence of a potential common disease etiology between migraine and syncope (5,15). While murine models showed that LRP1 is important for the maintenance of vascular wall integrity, allele C of rs11172113 in LRP1 was shown to be associated with lower gene expression in human vascular tissues such as those of the aorta and tibial artery (22,23). These findings suggest that both syncope and migraine may be diseases of vascular dysfunction, and that migraine patients with syncope are those with more severe manifestation of the disorder, so vascular disease risk assessments may be needed for these patients.
Migraine and syncope are both independently associated with risk of psychological disorders, particularly depression (6,24–27). A meta-analysis showed that migraine is associated with increased risk of depression (summary OR 2.2, 95% CI 2.0–2.3) (24), while in our study comorbid syncope in migraine patients was associated with about two times increased risk of depression. In conjunction, the risk of depression in migraine patients with comorbid syncope could be as high as four times that of healthy individuals. Furthermore, our study shows that comorbid syncope is associated with about three times increased risk of suicide attempt, after adjusting for many factors including aura, which was shown to be associated with suicide risk (28). We also show that the increased risk of suicide attempt associated with comorbid syncope in migraine patients is independent of depression, which is a red flag event that requires clinical attention. Besides, one may wonder whether the increased risks of depression and suicide is associated with potential underlying vascular dysfunction in relation to syncope. We did a post-hoc analysis and found no evidence for an association between rs11172113 in LRP1 and risks of depression, suicidal ideation, or suicide attempt (results not shown).
Strengths of our study include the large sample size of migraine patients and the multi-dimensional approach that we used to assess risk factors for syncope in migraine patients. This allows us to have a greater statistical power than previous studies to detect potential associations between personal or clinical factors of migraine patients and risk of syncope. The main limitation of this study is that all study participants were recruited from a headache clinic in a tertiary hospital originally set up to serve veterans (the proportion of veterans to all patients is about 20% now), and the proportions of female to male participants and those aged < 50 to those aged ≥ 50 are higher than those of general migraine populations, which may reduce the generalizability of the findings from this study. Secondly, the causes of syncope are influenced by the structure of the study populations recruited and may not be representative of those of general migraine populations. Besides, the definition of syncope used in this study is not supported with a valid source like that recently defined by the European Society for Cardiology (29) and syncope was self-reported and was not confirmed by a diagnostic test, so our findings may not entirely be comparable to other studies. Our definition for syncope is, however, similar to that of the CAMERA study, although we recorded a lower proportion of migraine patients with syncope in the past 12 months (7%) than the CAMERA study (12%) (2). This may be due to a more stringent validation of syncope in our study, which required a neurologist’s verification, so our study may underestimate the burden of comorbid syncope. On the other hand, all migraine diagnoses of study participants were made by board-certified neurologists based on the ICHD-3β criteria rather than by self-report. This is especially important for diagnosis of diseases without any objective biomarkers because it reduces misclassification bias, which increases bias toward null for any association understudied. Thirdly, all associations reported here should not be assumed to be causal due to the cross-sectional nature of the current study. Besides, information on the majority of risk factors for syncope examined in this study was collected using questions with binary outcomes (no, yes), resulting in potential loss of information that may be important for the analyses examining associations with syncope risks. In order to generate strong evidence from association analyses, epidemiology research needs to collect comprehensive information on risk factors using a prospective design. Finally, the results for migraine susceptibility loci (gene) and syncope risk are preliminary and were based on a small sample of migraine patients, which warrant further studies for confirmation of these findings. Nonetheless, this is the first study that provides an insight into characteristics and genes of migraine patients that are associated with risk of syncope and highlights the risk of psychological disorders associated with comorbid syncope.
In conclusion, our study showed the potential roles of vascular risk factors in the association between migraine and syncope. Modifiable risk factors for syncope in migraine patients include BMI and tea intake. The debilitating psychological impact of co-morbid syncope in migraine patients warrants clinical attention of treating physicians.
Clinical implications
Vascular disease risk assessments may be needed in patients with migraine and syncope. Avoiding being underweight and/or consuming tea regularly maybe useful in averting syncope in patients with migraine. The debilitating psychological impact and suicide risk of co-morbid syncope in migraine patients warrant clinical attention.
Footnotes
Authors’ contribution
ASK and S-JW conceived the study. All authors contributed to the design of the study. S-PC, Y-FW, J-LF, K-PP and S-JW recruited the study participants. S-PC, Y-FW, J-LF, K-PP, C-YC and S-JW interviewed the study participants. ASK did the literature search, performed the analysis, and drafted the manuscript. All authors read, provided comments, and approved the final manuscript.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: ASK, S-PC, Y-FW, K-PP, J-LF, and C-YC report no disclosures relevant to the manuscript. S-JW has served on the advisory boards of Allergan and Eli Lilly Taiwan; received speaking honoraria from local companies (Taiwan branches) of Pfizer, Eli Lilly, and GSK; and received research grants from the Taiwan Headache Society, all outside the submitted work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by grants from Taipei Veterans General Hospital (V108C-105), Ministry of Science and Technology of Taiwan (MOST 107-2321-B-010-001), Ministry of Health and Welfare, Taiwan, (MOHW 108-TDU-B-211-133001), and Brain Research Center, National Yang-Ming University from The Featured Areas Research Center Program within the framework of the Higher Education Sprout Project by the Ministry of Education (MOE) in Taiwan. The funders of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report.