
Abstract
Objective
The aim of this population-based validated study was to determine the course of tension-type headache and migraine and to evaluate the predictors of persistence.
Methods
We evaluated the course of headache in a large population from the first assessment in 2008 through a second assessment in 2013. Then we examined the factors associated with persistent migraine and persistent tension-type headache.
Results
Our study in 2013 revealed that only 42.9% of definite migraineurs in 2008 received the same diagnosis again, and of the remaining migraineurs 23.3% were newly diagnosed as definite tension-type headache; 11.6% evolved into probable tension-type headache, 6.4% changed to probable migraine, and 15.8% were headache free. The 17.7% of patients with definite tension-type headache in 2008 were newly diagnosed as having probable tension-type headache, 14.7% as having definite migraine, 6.4% as having probable migraine, and 28.9% as headache free in 2013, and only 32.3% received the definite tension-type headache diagnosis again. Binary logistic regression analysis showed nausea, throbbing and severe headache were the significant parameters for persistent migraine. A multiple regression analysis model with stepwise variable selection revealed that nausea, throbbing and severe headache and osmophobia remained in the final model as predictors of migraine persistence. We found no predictive factor for persistent tension-type headache.
Conclusion
Migraine and tension-type headache did not seem to show a simple bidirectional linear worsening from headache-free state to definite migraine or vice versa, hence the transitions between them are more chaotic, reflecting that there are still unknown modifiers and modulators. Certain headache characteristics of migraine might predict persistent migraine.
Introduction
Primary headache, a global disease, is the most common disorder of the nervous system with migraine and tension-type headache (TTH) being the most frequent types (1,2). Migraine in particular can cause disability for both patients and society because of the high prevalence in the population. Moreover, it is very important for the patient and the physician to understand how the headache types might change over time because of implications for treatment options, such as the use of triptans and new emerging immune therapies in migraine. In respect of understanding this global problem, studies have usually been focused on cross-sectional studies. Little is known about the course of primary headaches over time and associated risk factors for persistent migraine and TTH due to inadequate follow-up studies (3–5). Hospital-based studies may overemphasize the worst scenarios, making the understanding of the natural course of primary headaches more challenging.
For decades, it has been a matter of debate as to whether TTH and migraine are distinct entities or are different clinical ends of the same spectrum (6,7). Migraine and TTHs are distinctly defined and differentiated by the International Classification of Headache Disorders (ICHD) and also some evidence such as response to triptans and familial association of migraine support migraine and TTH being distinct disorders (8). In contrast, some authors hypothesize that migraine and TTH share a common pathophysiology, with TTH being a milder form of migraine (7). The convergence hypothesis suggests that migraine is a physiologic process that evolves over time and headaches resembling TTH are the first manifestation of this process (6). However, there are still unresolved problems associated with the relation of these two entities over time.
This study is based on a 5-year population-based study in Turkey; our aim was to determine the course of TTH and migraine and to evaluate the predictors of persistent migraine and persistent TTH.
Method
In the first step of the study, in 2008 we designed a nationwide, community-based prevalence study in subjects aged 18–65 years in 5323 households. Each household was examined through face-to-face interviews and examinations were performed by 33 trained general physicians. We used a systematic sample selection method and 21 cities showing the characteristics of households selected in seven geographic regions of Turkey. The number of participants was determined based on the ratio of their population to the total population of Turkey. The distribution of urban and rural populations, sex, and groups were all considered in order to minimize selection bias. Only one person was interviewed in each household and the Kish Method was used to select the participant per household to avoid any bias. Details of this initial survey and sampling methodology are described elsewhere (2).
Five years after this study, a second study – a telephone survey – was conducted with the same participants as the first study. A 50-item questionnaire was prepared that included the necessary questions for the diagnosis of migraine and TTH according to ICHD-II, which is fully compatible with ICHD-3 (8,9). ICHD-II criteria did not differ from the recently published ICHD-3 criteria in definite and probable migraine and TTH diagnosis (8,9). For the current study, we did not take chronic migraine as a different group.
The survey was optimized after the first 10 telephone calls. Pre-study and post-study validation studies were performed for the validation of telephone studies, which have been described in detail previously (10). The reliability of headache diagnosis in pre-study and post-study validation revealed that the 50-item questionnaire was strongly reliable. Telephone calls were conducted by trained call center employees. Among the 5323 households, 3001 subjects were eligible, with a 56.4 % responder rate.
We first evaluated the course of headache from the first assessment in 2008 through a second assessment in 2013. Then we examined the factors associated with persistent migraine and persistent TTH. The persistent migraine group included patients with definite or probable migraine at baseline in 2008 with the diagnosis persisting in 2013. The non-persistent migraine group included patients with definite or probable migraine in 2008 but in whom the diagnosis changed to TTH or the patient was headache free in 2013. The persistent TTH group included patients with definite or probable TTH at baseline in 2008 with the diagnosis persisting in 2013. The non-persistent TTH group included patients with definite or probable TTH in 2008 but where the patient was headache free in 2013. The studies were approved by the local Ethics Committee and informed consent was obtained from each participant.
Statistical analyses were performed using the Statistical Package for the Social Sciences (IBM SPSS Statistics, New York, USA) 21.0 software. The Shapiro-Wilk test was used to determine whether the data were normally distributed. p < 0.05 was accepted as the level of significance. Descriptive statistics were applied; the Chi-square test and t-test were used for group comparisons, where appropriate. We used binary logistic regression tests and multiple logistic regression modeling with forward stepwise variable selection to identify the factors associated with persistent migraine.
Results
The main results of these two nation-wide epidemiologic studies (the first being the prevalence study and the second the incidence study) were published previously (2,10) and the current study focuses on the 5-year course of migraine and TTH. The prevalence of headache types was estimated from 5323 participants in 2008 by general physicians, and from 3001 participants through validated telephone surveys in 2013. The overall prevalence of headache was higher in 2013 when compared with the prevalence in 2008 (56.2% in 2013, 44.6% in 2008). The prevalence of definite migraine was 16.7% in 2013, and 16.4% in 2008. The prevalence of definite TTH was higher in 2013 when compared with the prevalence in 2008 (5.1% in 2008, 22.3% in 2013).
Our study in 2013 revealed that only 42.9% of definite migraineurs in 2008 received the same diagnosis again, and of the remaining migraineurs 23.3% were newly diagnosed as definite TTH, 11.6% evolved into probable TTH, 6.4% changed to probable migraine and 15.8% were headache free (Figure 1(a)). Moreover, 17.7% of respondents with definite TTH in 2008 were newly diagnosed as having probable TTH, 14.7% as having definite migraine, 6.4% as having probable migraine and 28.9% as being headache free in 2013; only 32.3% received the definite TTH diagnosis again (Figure 1(c)). The new diagnosis in 2013 of probable migraine, probable TTH, and headache-free participants are also shown in Figure 1.
(a) The new diagnosis of definite migraine, (b) probable migraine, (c) definite TTH, (d) probable TTH, (e) headache-free participants in 2013.
Comparison of demographic characteristics of patients with persistent and non-persistent migraine.
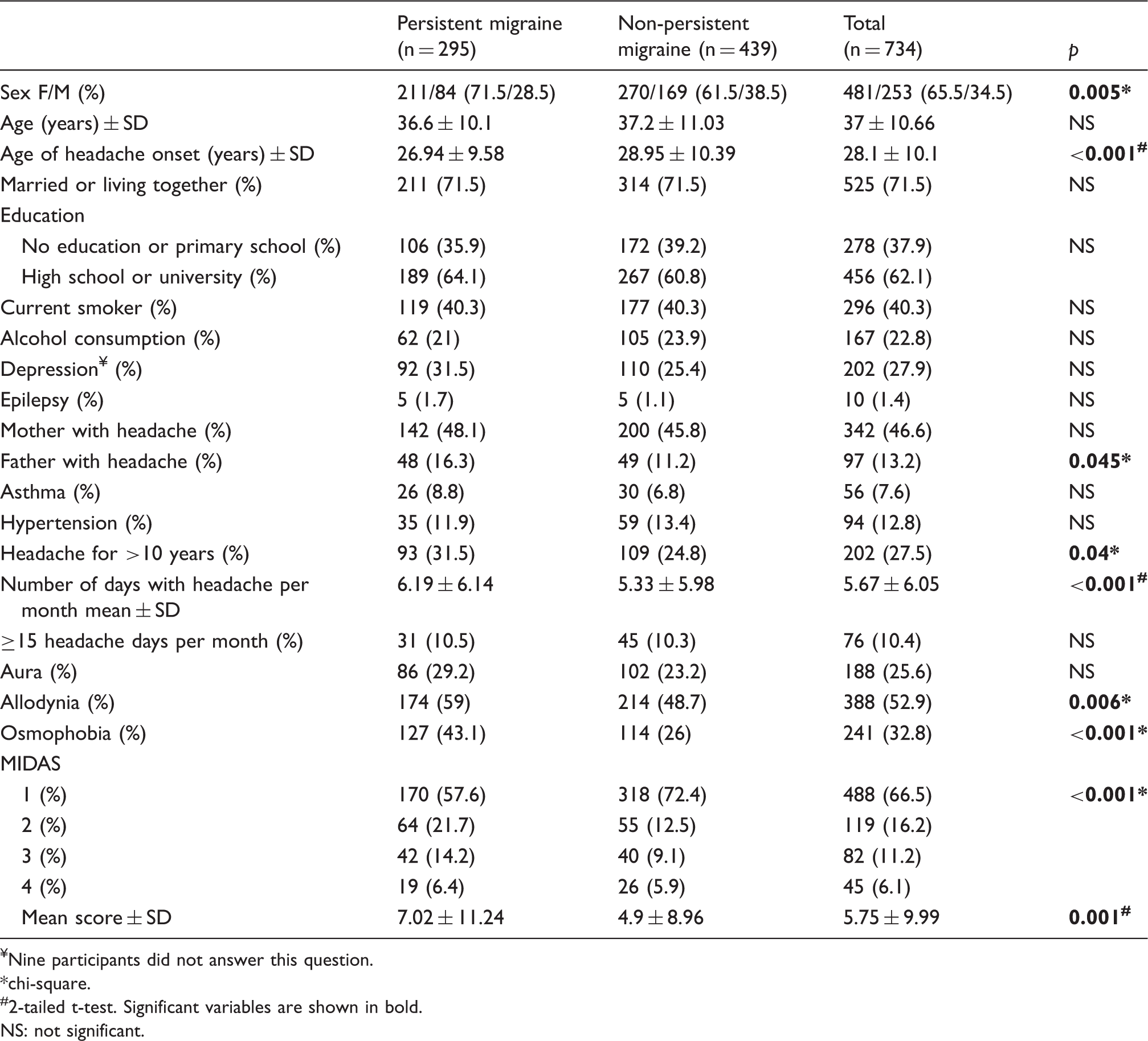
Nine participants did not answer this question.
chi-square.
#2-tailed t-test. Significant variables are shown in bold.
NS: not significant.
Comparison of characteristics of headache in patients with persistent and non-persistent migraine.
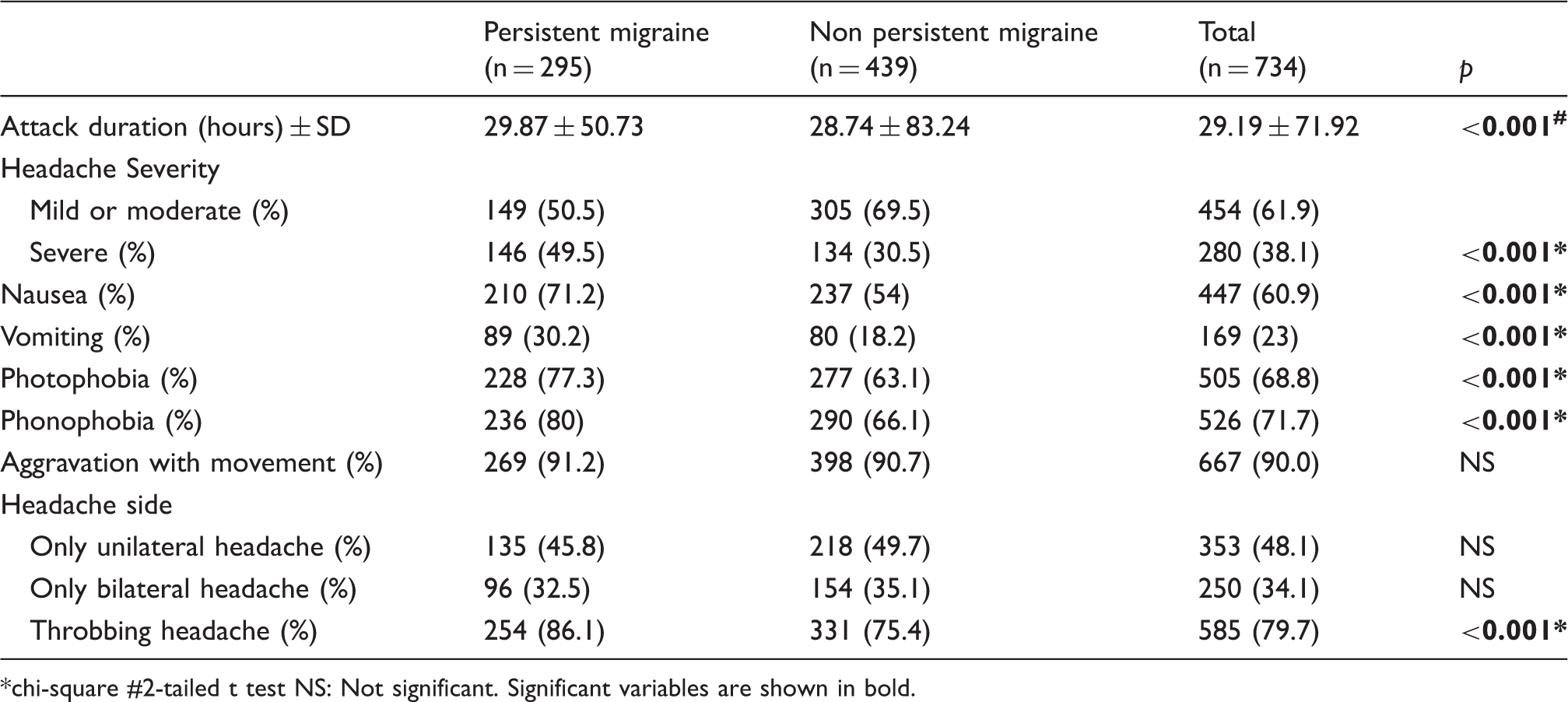
chi-square #2-tailed t test NS: Not significant. Significant variables are shown in bold.
Significant variables of persistent migraine using binary logistic regression analysis.

Ref. cat.: reference category.
Significance of the model: p < 0.001. Significant variables are shown in bold.
Multiple logistic regression – stepwise forward elimination predictors of persistent migraine.

Comparison of characteristics of headache in patients with persistent and non-persistent TTH.

NS: not significant.
Discussion
Our study revealed that only 40.2% of migraineurs continued to have migraine attacks after 5 years, whereas a similar percentage (37.9%) were diagnosed as having TTH; the remaining 21.9 % became headache free after 5 years. On the other hand, 49% of those with TTH continued to have TTH headaches; a remarkable 23.1% of patients with TTH evolved into migraineurs after 5 years and the remaining 27.9% became headache free. These results show that primary headaches did not seem to show bidirectional linear worsening from headache-free state to definite migraine and vice versa, hence the transitions between migraine and TTH are more chaotic, as demonstrated in Figure 2, reflecting that there are still-unknown modifiers and modulators.
Transitions between migraine and TTH.
The so-called “convergence hypothesis” supports that migraine is a physiologic condition that evolves over time, and attacks appearing as TTH might be the initial manifestation of this continuum; migraine and TTH are suggested to be the two ends of the same spectrum with one end being migraine-type headache and the other end being TTH (6,7,11). Although our findings do not solve the debate over whether TTH and migraine are different diseases or parts of the same disorder, the remarkable interchangeability between migraine and TTH in our study supports that these two primary headache types cannot be separated exactly from each other and transition between migraine and TTH is much more complex than predicted.
The transition between migraine and TTH was also mentioned in previous studies and our results are similar to previous literature. Kienbacher et al. showed that of 140 patients initially diagnosed with migraine, 25.7% were diagnosed as headache free, 48.6% still had migraine and 25.7% had TTH after 6.6 ± 1.6 years. Additionally, of the 87 patients with TTH, 37.9% were headache free, 41.4% still had TTH and 20.7% had migraine in the follow-up (12). Their study group was small and included only patients who had been referred to a headache center. In a 30-year prospective Swiss cohort study, 69% of patients with migraine and 58% of participants with TTH revealed the same predominant headache over time and, in accordance with our study, they showed that the stability of primary headache types was quite low (13). In a study by Lyngberg et al. in 2005, of 740 persons (aged 25 to 64 years) examined in a 1989 Danish cross-sectional headache study, 673 were eligible for follow-up in 2001. A total of 549 persons (81.6%) participated in the follow-up study. Of 64 migraineurs at baseline, 42% had experienced remission, 38% had low migraine frequency, and 20% had more than 14 migraine days per year (poor outcome) at follow-up (4). However, the studies’ methods vary in categorization of headache type, responder rate, age group, follow-up duration and, as a result, comparisons between these studies should be done with caution.
It is very important, both from the perspectives of the patient and the physician to understand the prognosis of headache, especially migraine, correctly over time. Some studies have revealed the predictors of remission of migraine, thus elucidating a benign prognostic group, but the predictors of persistence are not well known. To create more homogenous subgroups for future studies exploring the pathogenesis and also the genetics of migraine, insight into the persistent forms is also of crucial importance. Moreover, extrapolating persistent headache types over time would also be very valuable because of the implications for treatment options, such as the use of new emerging immune therapies and other prophylactic options for migraine.
Given that only some patients with migraine or TTH tended to have their headache persist over 5 years, we wanted to extrapolate factors that predicted this persistence in terms of sociodemographic variables and headache characteristics. Intriguingly, we found no predictive factors for persistent TTH, highlighting its non-specific character. However, our results demonstrated predictive factors associated with persistent migraine. According to our results, some well-known associated characteristics of migraine such as nausea/vomiting, throbbing and severe headache in the initial examination were the major predictors of persistent migraine over 5 years. The pathophysiologic mechanisms producing certain headache features of migraine and associated symptoms are complex and not clearly identified. They are presumably related to central sensitization and dysfunction of the locus coeruleus, and its connection with the cerebral cortex and brainstem may induce cortical excitability, and progressive changes in nociceptive thresholds may finally lead migraine to persist (14–16). Severe and throbbing headache is associated with consequential structural and functional changes from trigeminovascular system to dura mater. Nociceptive nerve fibers originating from the trigeminal region innervate the meningeal blood vessels, primarily dural venules, and activation of nociceptive fibers results in sterile neurogenic inflammation; this consequence results in severe and throbbing pain in patients with migraine (17,18). We think that the combination of all these characteristics of migraine is the determining factor of persistence.
Our study showed that osmophobia is another predictive factor for persistent migraine. A total of 43.1% of persistent migraine patients reported osmophobia, which is significantly higher than with non-persistent migraine (26%). Many studies have pointed to osmophobia as a peculiar and highly-specific symptom in migraine (19–21). Although the exact mechanism of osmophobia is unknown, an fMRI study suggested that there is strong relationship between the olfactory system and trigeminal nociceptive pathway in migraine patients. A previous 3-year follow-up study in juvenile patients showed that osmophobia is a predictive factor for evolution of TTH to migraine, supporting the role of osmophobia as an early marker of migraine with a prognostic and diagnostic role in primary headaches (22). Our results corroborated this finding, showing its role in migraine persistence. Although there was a significant difference in photophobia and phonophobia between persistent migraine and non-persistent migraine, they did not predict persistence after regression analysis. Two studies previously showed that osmophobia reflected higher specificity than photophobia and phonophobia in the differential diagnosis between TTH and migraine (23,24). This supports our finding that osmophobia is a specific finding, and can reflect persistence in migraine more than photophobia and phonophobia.
Notably, MIDAS, a self-administered questionnaire that includes questions covering the previous 3-month period, was found to be another important factor, but it did not predict persistence. A higher MIDAS score at baseline was found to be associated with higher rates of persistence in patients with migraine. Accordingly, studies focusing on MIDAS in migraine chronification and transformed migraine showed that higher MIDAS scores in initial examinations were important factors in migraine chronification and also transformed migraine (25,26).
Many studies reported that a familial disposition to migraine was important in the prognosis and persistence of migraine (5,27,28). In a 10-year follow-up study in adolescents, family history was found to be a predictive factor for persistent migraine (5). Although we found a higher prevalence of persistent migraine in patients with a history of headache in the fathers, it was not found to predict the persistence as an independent factor. Moreover, we found no association between persistent migraine and history of headache in the mother, which is more frequently observed. This might be because of the important modifying effects of multiple environmental factors influencing the persistence of migraine headache. Although clinical and environmental factors may potentially contribute to the persistence of migraine, the influence of genetic factors is complex, and we could not examine the genetic role of persistence except through family history. With developing opportunities in migraine genetics, identification of genetic biomarkers for persistent migraine might be a task for researchers of migraine genetics in future studies. Epigenetic studies may enlighten the underlying mechanisms of persistence in migraine.
It is still not known whether the persistence of migraine is associated with comorbid depression. Our results showed that comorbid depression at baseline was not a primary risk factor for persistent migraine or persistent TTH at a 5-year endpoint. Consistent with our study, a previous large epidemiologic study showed no relation between migraine incidence and major depression at baseline (29). On the other hand, some other studies showed increased risk of migraine in patients with major depression (30).
It was intriguing that we found no predictive factors for persistent TTH. This might be because of the very high frequency of patients with infrequent episodic TTH and its non-specific character (31). Recent studies also noted that the accurate diagnosis of TTH has received limited attention and TTH is not well characterized with a definition depending exclusively on symptoms, which can be found in other headache types such as migraine (32).
As a main methodologic strength, our study is based on two nationwide population-based studies including the longitudinal data of a large number of participants. Our findings support and extend the view of chaotic transition between primary headaches, but at the same time show the predictors of persistence of migraine. One of the limitations of this study is that the second evaluation of participants was conducted using a telephone survey and, although validated, it can be biased in several respects. For convenient use of time, questions having less impact on diagnosis were excluded (such as socioeconomic status and lifestyle changes) from the telephone interview; however, all questions necessary for diagnosing primary headaches according to ICHD-II were identical in 2008 and 2013. Moreover, pre- and post-study validation studies were performed for the validation of the telephone survey and these revealed that the 50-item questionnaire was strongly reliable. It has been reported that diagnostic validation of telephone calls has been found to be accurate and reliable, with a very good agreement in previous studies evaluating telephone interviews in comparison with clinical evaluation (33,34). Another potential bias might be the moderate responder rate of 56.4% in the second examination. We also could not ascertain the continuous external social variables such as divorce, change in socioeconomic status, loss of family members and fluctuations in headache characteristics in the 5-year period, which may result in loss of information. Another limitation is that we did not categorize more than one headache subtype in each interview, so we might overestimate the transition between migraine and TTH in patients who met the criteria for both migraine and TTH.
In conclusion, migraine and TTH did not seem to show a simple bidirectional linear worsening from headache-free state to definite migraine or vice versa, hence the transitions between them are more chaotic, reflecting that there are still unknown modifiers and modulators. Certain headache characteristics of migraine might predict persistent migraine, and future studies with follow-up investigations should continue to focus on the associated factors related with persistent migraine.
Clinical implications
The transitions between migraine and tension-type headache are not linear and are much more complex than predicted. Characteristics such as nausea, osmophobia, throbbing and severe headache might predict persistent migraine. No predictive factor was found for persistent tension-type headache.
Footnotes
Acknowledgements
The authors thank the patients for their contribution in the study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by an unrestricted research grant of Ibrahim Ethem Ulagay-Menarini Group, Davutpasa Cad No: 12 Topkapı-Istanbul.