
Abstract
Introduction
Migraine comorbidity with obesity is not new and studies have focused on how adipose tissue-derived substances such as adipokines might be involved in the migraine pathophysiology. Quantification of the nature and magnitude of the association between each adipokine including leptin, adiponectin and resistin with migraine pathophysiology is the objective of the current study.
Methods
Using systematic reviews and meta-analyses and standardized mean difference as effect size, the levels of three adipokines, leptin, adiponectin and resistin, have been investigated in migraineur subjects in the case-control studies.
Results
Using random-effects models, the final analyses demonstrated the standardized mean differences of leptin, adiponectin and resistin as 0.534 (95% confidence interval, 0.169–0.898), 0.439 (95% confidence interval, 0.132–0.746) and 0.194 (95% confidence interval, −0.158–0.546), respectively. The p-value for test of significance for each pooled standardized mean difference was examined by the z-test and calculated as 0.004, 0.005 and 0.281 for leptin, adiponectin and resistin (clearly considered as statistically significant, significant and non-significant), respectively.
Conclusion
Based on the findings, the blood levels of leptin and adiponectin, but not resistin, of the migraineurs are associated with disease pathogenesis.
Introduction
Migraine is a multifactorial vasculo-neurological condition that manifests as recurrent pain attacks lasting 4–72 hours as headaches (1,2). Interestingly, migraine prevalence is increased in obese individuals compared to normal weight controls and it also increases with overweight status intensity (i.e. from normal weight to overweight to obese) (3–11). Moreover, the association between migraine and obesity may be more evident in women, compared to men, and in those below the age of 50 years in comparison with older individuals (8). These preliminary studies were motivated by focusing on the adipose-derived substances and migraine pathogenesis relationship in more detail. Indeed, migraine comorbidity with obesity is not new and studies have focused on what obesity-related factors might be involved in the migraine pathophysiology. White adipose tissue, either subcutaneous or visceral, is composed of adipocytes, embedded in a meshwork of loose connective tissue containing mature and precursor adipocytes and immune cells, and possesses a substantial nervous and vascular supply as well (12). This tissue is responsible for the secretion of an array of signaling molecules known as adipokines, and a variety of these signaling molecules has been discovered so far including leptin, adiponectin and resistin, and so on (13). In the current study, the circulating levels of leptin, adiponectin, and resistin of the case-control clinical studies have been investigated in migraineurs using systematic reviews and meta-analyses.
Materials and methods
Protocol of the systematic review and meta-analysis
The PRISMA Checklist 2009 was used to conduct this systematic review and meta-analysis (14).
Information sources and search strategies
A systematic literature search was independently carried out by four of the authors (AS-N, SB, MK and SP) using the specialized biomedical Pubmed, Pubmed Central, Medline, Google Scholar, Embase and SCOPUS databases without a start date restriction until January 2018. Publications using the MeSH and non-MeSH terms “migraine”, “headache” in combination with “leptin”, with additional keywords such as “peripheral blood samples”, “circulatory” and “case-control study”, were identified. Moreover, these databases were also searched for MeSH and non-MeSH terms “migraine”, “headache” in combination with “adiponectin”, with additional keywords such as “peripheral blood samples”, “circulatory” and “case-control study”. The third search was accomplished for resistin and the aforementioned databases were searched for MeSH and non-MeSH terms “migraine”, “headache” in combination with “resistin”, with additional keywords such as “peripheral blood samples”, “circulatory” and “case-control study”. The harvested references from studies were also scrutinized to identify any additional relevant studies. Then, the search results were restricted to English language and the review processes were limited to case-control studies by three authors independently, which fulfilled our inclusion and exclusion criteria.
Eligibility criteria
Studies were pre-included if they used standardized methods such as enzyme-linked immunosorbent assay (ELISA) and chemiluminescent methods for detection of resistin, adiponectin and leptin levels. No limitation was applied to the subtypes of migraine, the severity of migraine, pain scale, or race or sex of the study participant subjects. However, studies were excluded if they enrolled populations other than migraineurs, as were reports describing migraine interventional therapies. We only considered resistin, adiponectin and leptin levels for effect size analyses in each study in the case and control groups.
Study selection
Only case-control studies providing enough information about their results to compute an estimate of the effect size (such as means and standard deviations or standardized error of the mean, etc.) for leptin, adiponectin and resistin were included. Due to the different protocol definition used for assessment of adipokine levels, only studies that determined the levels of resistin, adiponectin and leptin in migraineurs in comparison with healthy subjects were considered for inclusion in the current meta-analyses.
Data collection process
The first author of the selected papers, date of publication, the levels of resistin, adiponectin and leptin in migraineurs and healthy controls, evaluated criteria for the migraine, and also the total number of cases and controls and other related information, were extracted from the publications obtained from systematic reviews for meta-analytical processes.
Summary measures and synthesis of results
Stata version 14.0 (Stata Corporation, College Station, TX, USA) was employed for data analyses of the systematic review and meta-analysis. Between-study heterogeneity was assessed using the χ2 based Q-test and also I2. The Q test and I2 statistics were applied to evaluate the inconsistencies and heterogeneities among the studies. A significant Q suggests the existence of heterogeneities, and I2 estimates the magnitude of the inconsistencies among the studies (15). For analysis of an estimated total effect size, the random-effects model and standardized mean difference (SMD) were used. Data were shown as the estimated SMD with 95% confidence interval (CI) for each study. The significance of the total SMD was examined by the z-test, and p < 0.05 was considered as statistically significant.
Risk of bias across studies
For the risk of bias across studies, the papers were scrutinized for method validation and data processing and for pooled effect size estimation from the selected studies; a funnel plot was also developed. For interpretation of any publication bias among studies, visual inspections of the generated funnel plot were employed to evaluate the symmetry. In this plot, the y and x axes represent the standard error and standard difference in means, respectively.
Results
Study selection
The flowcharts of the study selections in the systematic review processes have been presented in Figures 1, 2 and 3. The initial search for leptin identified a total of 6190 potentially eligible studies, and 5918 records were removed as duplicates. Of the remaining 272 records, 260 publications were excluded after reading the titles or abstracts as being obviously irrelevant to the goal of this meta-analysis. Moreover, because of insufficient data presented by the authors of such publications for calculation of the SMD and 95% CI, and because of poor quality, a further three papers were excluded. Finally, nine studies (which are detailed in Table 1 and cited in the References of the current study (5,16–23)) were included in the meta-analytical processes for leptin levels (Figure 1). The initial search for adiponectin blood levels identified a total of 2950 potentially eligible studies and 2784 records were removed as duplicates. Of the remaining 166 records, 157 publications were excluded after reading the titles or abstracts as being obviously irrelevant to the goal of this meta-analysis. Moreover, because of insufficient data presented by the authors of such publications for calculation of the SMD and 95% CI and because of poor quality, two further papers were excluded. Finally, for adiponectin blood levels, seven studies (which are detailed in Table 2 and cited in the References of the current study (5,16–18,20,22,24)) were included in the meta-analytical processes (Figure 2). The initial search for resistin identified a total of 574 potentially eligible studies and 484 records were removed as duplicates. Of the 90 remaining records, 86 publications were excluded after reading the titles or abstracts as being obviously irrelevant to the goal of this meta-analysis. Moreover, because of insufficient data presented by the authors of such publications for calculation of the SMD and 95% CI and because of poor quality, one further paper was excluded. Finally, for resistin blood levels, three studies (which have been detailed in Table 3 and cited in the References of the current study (16,18,22)); were included in the meta-analytical processes (Figure 3).
Systematic review searching strategy for leptin blood levels in migraineurs. Systematic review searching strategy for adiponectin blood levels in migraineurs. Systematic review searching strategy for resistin blood levels in migraineurs. Studies that have been included in this meta-analysis, the demographic data and clinical characteristics extracted from them for leptin blood levels. Note: Data was presented as mean ± standard deviation. Studies that have been included in this meta-analysis and the demographic data and clinical characteristics extracted from them for adiponectin blood levels. Note: Data was presented as mean ± standard deviation. Studies that have been included in this meta-analysis and the demographic data and clinical characteristics extracted from them for resistin blood levels. Note: Data was presented as mean ± standard deviation.



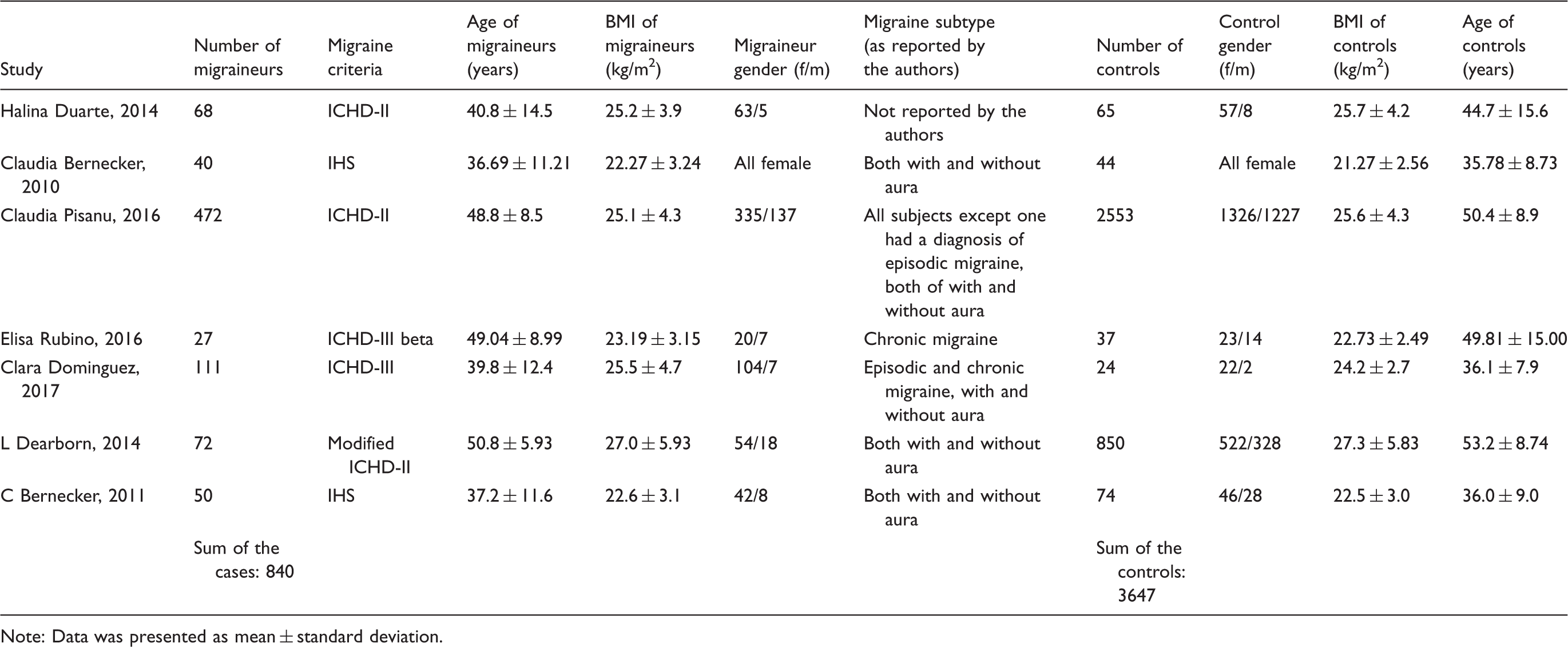

Study characteristics
For each study, the data on epidemiologic and disease characteristics reported by the authors were extracted. The number of migraine cases, migraine subtypes, number of healthy controls, migraine definition criteria, body mass index (BMI), mean age in healthy controls and migraineurs have been presented in Table 1, Table 2 and Table 3 for leptin, adiponectin and resistin, respectively. Actually, this meta-analysis retrieved a total number of 945 cases and 3738 control subjects to January 2018 for blood levels of leptin. For adiponectin blood levels, a total number of 840 cases and 3647 control subjects were retrieved to January 2018 and for resistin blood levels, a total number of 117 migraineurs and 155 controls were retrieved to January 2018.
Risk of bias within studies
The results showed that the selected studies were not homogenous and actually they were inconsistent in some ways. The Q tests were 102.646, 46.102 and 4.078 for leptin, adiponectin and resistin, respectively. The Q statistic test is only applied for testing the existence of heterogeneity among studies but is not suitable for calculation of the extent of heterogeneity. However, a tentative classification of I2 values has been proposed to interpret the magnitude of heterogeneity. Thus, percentages of around 25% (I2 = 25), 50% (I2 = 50), and 75% (I2 = 75) would mean low, medium, and high heterogeneity, respectively (15). Moreover, the I2% tests were 92.206, 86.986 and 50.960 for leptin, adiponectin and resistin, respectively. The I2 index and between-studies variance, τ2, are directly related: The higher the τ2, the higher the I2 index (15). Therefore, the random-effects models of meta-analyses were applied for the presentation of the forest plots of the selected studies in leptin, adiponectin and resistin blood levels in migraineurs.
Synthesis of results
The forest plot showed the mean effect sizes and standard deviations and the SMD with 95 percent CI for each study as well as the overall effect size. The primary analysis for the main hypothesis found that the weighted average effect size for the association between leptin and migraine pathogenesis was as follows: SMD = 0.534 (95% CI, 0.169–0.898) using the random-effects model in the meta-analysis as presented in Figure 4 for the nine included studies. The p-value for the significance of the combined SMD examined by the z-test for leptin was 0.004. The weighted average effect size for the association between adiponectin and migraine pathogenesis was as follows: SMD = 0.439 (95% CI, 0.132–0.746) using the random-effects model in the meta-analysis as presented in Figure 5 for the seven included studies. The p-value for the significance of the combined SMD examined by the z-test for adiponectin was 0.005. The weighted average effect size for the association between resistin and pathogenesis of migraine was as follows: SMD = 0.194 (95% CI, −0.158–0.546) using the random-effects model in the meta-analysis as presented in Figure 6 for the seven included studies. The p-value for the significance of the combined SMD examined by the z-test for resistin was 0.281.
Forest plot of the included studies fulfilled the inclusion/exclusion criteria for blood leptin levels in migraineurs in the case-control studies. Forest plot of the included studies fulfilled the inclusion/exclusion criteria for blood adiponectin levels in case-control studies. Forest plot of the included studies fulfilled the inclusion/exclusion criteria for blood resistin levels.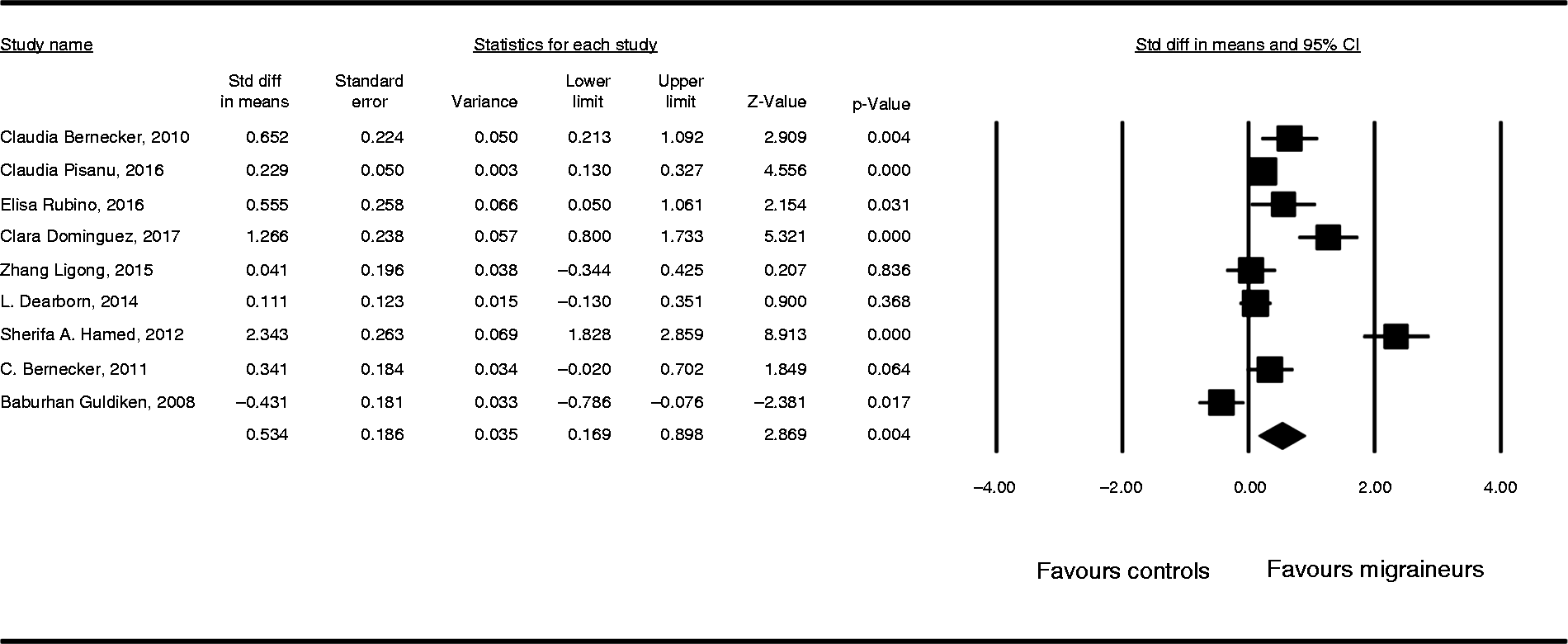


Risk of bias across studies
The shapes of the funnel plots were considered to be moderately asymmetrical, confirming that there was some publication bias in the related accepted papers for leptin, adiponectin and resistin. For leptin blood levels, this bias refers mainly to the right-hand part of the plot, which was mainly occupied by publications demonstrating higher SMD in migraineurs compared with controls (Figure 7). For adiponectin blood levels, the bias refers mainly to the right-hand part of the plot, which was mainly occupied by publications demonstrating higher SMD in migraineurs compared with controls (Figure 8). For resistin blood levels, the asymmetry in the funnel plot was not intense in migraineurs compared with controls (Figure 9).
Funnel plot of the included studies for leptin blood levels. Funnel plot of the included studies for adiponectin blood levels. Funnel plot of the included studies for resistin blood levels.


Discussion
There are multiple areas of overlap between the peripheral and central pathways regulating feeding and pathophysiology of migraine: Inflammatory mediators such as calcitonin gene-related protein (CGRP) and interleukin-6, neurotransmitters such as serotonin, and adipocytokines such as leptin, adiponectin and resistin could explain the common pathogenesis. Even though there are many published papers and systematic reviews that consider adipokines and migraine pathophysiology, to the best of our knowledge a meta-analysis has not been performed in this regard so far. In the current study, among the adipokines, the levels of leptin and adiponectin, but not resistin, in the blood of migraineurs were associated with the disease pathogenesis, as the final analyses demonstrated the combined SMDs for each adipokine, including leptin, adiponectin and resistin, as 0.534 (95% CI, 0.169–0.898), 0.439 (95% CI, 0.132–0.746) and 0.194 (95% CI, −0.158–0.546), using random-effects models, respectively. Thus, leptin and adiponectin circulatory levels are altered in migraineurs. In this study, the number of studies for synthesizing meta-analyses data was sufficient for both leptin and adiponectin. However, in the case of resistin, the number of studies fulfilling the exclusion and exclusion criteria of the current study for blood levels in migraineurs was low, and thus the power of meta-analysis for it was low. Potential confounders may, at least in part, explain the results of the current study for resistin meta-analysis. There were only three studies available describing resistin circulatory levels; however, more studies are needed to draw any conclusions regarding the potential association between resistin blood levels and migraine pathobiology. On the other hand, it is evident that publishing reports that only show significant results disturbs the balance of findings. Thus, there may be potential effects of publication bias on the observed effect sizes of leptin and adiponectin among migraineurs in the current study; however, in these meta-analyses all available published studies in the aforementioned databases were included according to the inclusion and exclusion criteria. One reason why obesity is associated with migraine susceptibility is that obesity is often related to adipose tissue functional activity changes and increased inflammatory response levels. White adipose tissue secretes adipokines that function as circulating hormones to communicate with other organs including the brain and the adipose tissue itself. The dysregulation of adipokine secretion levels has been implicated in a variety of diseases such as Type 2 diabetes, cardiovascular disease, and obesity. The current study only investigated the changes in the blood concentrations of three adipokines, and further studies are needed to elucidate the neurobiological mechanisms underlying their migraine-triggering actions. Interestingly, fasting or skipping meals is considered as a pain-triggering factor for migraineurs, and altered fasting glucose and insulin circulatory levels have been observed in migraine subjects. Therefore, peptides involved in blood glucose and appetite regulation, including pancreatic hormones like insulin and glucagon and adipose tissue-derived hormones such as leptin, could potentially influence the neurobiology of migraine. A potential neurobiological link between migraine pain and impaired metabolic homeostasis of the body may occur through disturbed blood glucose regulation. Surprisingly, a recent study has shown that insulin, glucagon and leptin could alter transmission of trigeminal nerve nociceptive inputs to higher brain levels (25). Therefore, adipokine signaling may modulate specific neural networks relevant to migraine pathophysiology.
Footnotes
Article highlights
Association between blood adipokines and migraine pathogenesis was investigated using meta-analyses (pooled standardized mean difference (SMD) as effect size).
The studies selected from the systematic reviews were heterogeneous and random-effects models.
The pooled SMD for leptin was 0.534 (95% CI, 0.169–0.898). p-value for the z-test was 0.004.
The pooled SMD for adiponectin was 0.439 (95% CI, 0.169–0.898). p-value for the z-test was 0.005.
The pooled SMD for resistin was 0.194 (95% CI, 0.169–0.898). p-value for the z-test was 0.281.
Based on the findings, the blood levels of leptin and adiponectin, but not resistin, of migraineurs are associated with migraine pathogenesis.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics
The present study was approved by the Ethics Committee of Ilam University of Medical Sciences.