
Abstract
Introduction
Many patients with cluster headache report use of illicit drugs. We systematically assessed the use of illicit drugs and their effects in a well-defined Dutch cluster headache population.
Methods
In this cross-sectional explorative study, 756 people with cluster headache received a questionnaire on lifetime use and perceived effects of illicit drugs. Results were compared with age and sex-matched official data from the Dutch general population.
Results
Compared to the data from the general population, there were more illicit drug users in the cluster headache group (31.7% vs. 23.8%; p < 0.01). Reduction in attack frequency was reported by 56% (n = 22) of psilocybin mushroom, 60% (n = 3) of lysergic acid diethylamide and 50% (n = 2) of heroin users, and a decreased attack duration was reported by 46% (n = 18) of PSI, 50% (n = 2) of heroin and 36% (n = 8) of amphetamine users.
Conclusion
In the Netherlands, people with cluster headache use illicit drugs more often than the general population. The question remains whether this is due to an actual alleviatory effect, placebo response, conviction, or common pathophysiological background between cluster headache and addictive behaviours such as drug use.
Introduction
Cluster headache is a rare primary headache disorder characterized by severe unilateral headache attacks lasting 15 to 180 minutes accompanied by cranial ipsilateral autonomic symptoms (1). Most people suffer from the episodic form, in which attacks occur in clusters of weeks to months alternating with remissions of several months to years (1). About 14% of people with cluster headache suffer from the chronic form and do not have attack-free episodes longer than a month (1,2). Although most people with cluster headache can be successfully treated with regular medication, in 10–20% this is not effective (3). These people are more likely to experiment with alternative treatments (4), including illicit drugs.
Few epidemiologic studies have investigated the use of illicit drugs in cluster headache (4–7). In two French studies, 26–32% of cluster headache patients used cannabis regularly, which is higher than in the general French population (7%) (6,7). The prevalence of cannabis use was considerably lower (10%) in an American cluster headache cohort (7,8). Illicit drug use in cluster headache has been associated with younger age, male gender, and smoking. Use of alternative treatments in cluster headache has also been associated with lower income and higher annual attack frequency (5,9).
Some patients report an acute effect of cannabis, cocaine, psilocybin mushrooms (PSI) and heroin (4,10,11). In a small open study, 22 of 26 patients reported an acute effect on their cluster headache attacks after psilocybin mushrooms use (11). In Italy, 7–19% of people with cluster headache reported having tried cannabis as an acute treatment, but self-reported effects were inconclusive (4,7). In 25%, it even seemed to trigger attacks (7).
Illicit drugs are not only described as acute treatment, but in several small studies also as alternative prophylactic treatment. Remission-extending qualities have been attributed to PSI, gamma-hydroxybutyrate (GHB) and lysergic acid diethylamide (LSD) (4,11–13). GHB’s sodium salt form (sodium oxybate) reduced attack frequency in five patients with cluster headache (12,13). In a small study, patients reported a perceived prophylactic effect of both LSD and PSI (11).
While these possible alleviatory effects of illicit drugs in cluster headache are intriguing, the studies that have been conducted were all small and uncontrolled. Although restricted use of cannabis is legal in the Netherlands, the use of drugs in cluster headache has not been investigated. Here we systematically assessed (i) the use of illicit drugs in general and (ii) the use of several illicit drugs in a representative Dutch cluster headache population and compared this to the Dutch general population. Additionally, we determined whether illicit drugs influenced cluster headache attack duration and attack frequency in the Dutch cluster headache population.
Material and methods
Study design
This explorative cross-sectional study was conducted as part of the ongoing nationwide Leiden University Cluster Headache neuro-analysis programme (LUCA) and compared to official data of the Dutch general population.
Cluster headache population
The LUCA program is heavily promoted throughout the Netherlands to attract as many potential cluster headache participants of 18 years and older as possible. In addition, participants attending the Leiden University Medical Center and other headache outpatient departments were invited to participate in the LUCA program. All possible participants were invited to fill out a validated, web-based screening questionnaire about cluster headache based on the ICHD-II criteria for cluster headache (14). The screener has been validated and has a diagnostic specificity of 0.89 for cluster headache (15). All people who fulfilled the ICHD-II criteria also fulfilled the latest ICHD-III beta version for cluster headache (16). All people who screened positive received a second, more extensive web-based questionnaire.
For the present study, people who had been screened as positive for cluster headache received an email asking them to fill out a questionnaire concerning illicit drug use. This questionnaire was designed by the authors (IFC and LAW) and included questions about lifetime use of illicit drugs and more specifically the use of cannabis, cocaine, heroin, PSI, 3,4-methylenedioxymethamphetamine (MDMA), LSD, amphetamine and GHB. Also, the questionnaire included two questions about the effect on attack duration and attack frequency of these illicit drugs (there were three answer options: Increased, no effect, decreased). Web-based questionnaires were used, except for people not capable of using the internet, who were allowed to fill out the questionnaires on paper. Those who did not respond to the initial email were reminded twice per email and, when still not responding, they were contacted two more times (once by phone and once by email again). Only people who filled out all items regarding drug use were included.
All LUCA data was securely stored in a web-based database management system of ProMISe (Project Manager Internet Server), which meets ISO 27001 and the requirements for data safety and privacy set by international law.
Dutch general population
Statistics Netherlands (Centraal Bureau voor Statistiek) provided data about the Dutch general population from their annual health survey, which monitors various health and lifestyle aspects including illicit drug use in the Dutch population. Each year, 15,000 randomly selected Dutch citizens of all ages are approached by mail to fill out their online survey. For our study, we only included data from people 18 years old and older. Statistics Netherlands supplies this data as anonymous categorical variables. The information is therefore not traceable to an individual.
For our study, we divided the data into three categories: All, people classified as having headache (migraine or regular severe headache in the previous 12 months), and people classified as having chronic pain (in the previous 12 months).
Ethical approval
The LUCA study was approved by the local medical ethics committee of the Leiden University Medical Center. All participants in the LUCA study provided written informed consent. The survey in the Dutch general population by Statistics Netherlands was exempt from ethical approval according to Dutch laws, therefore no informed consent was needed.
Statistics
Demographics of cluster headache population and the general population.
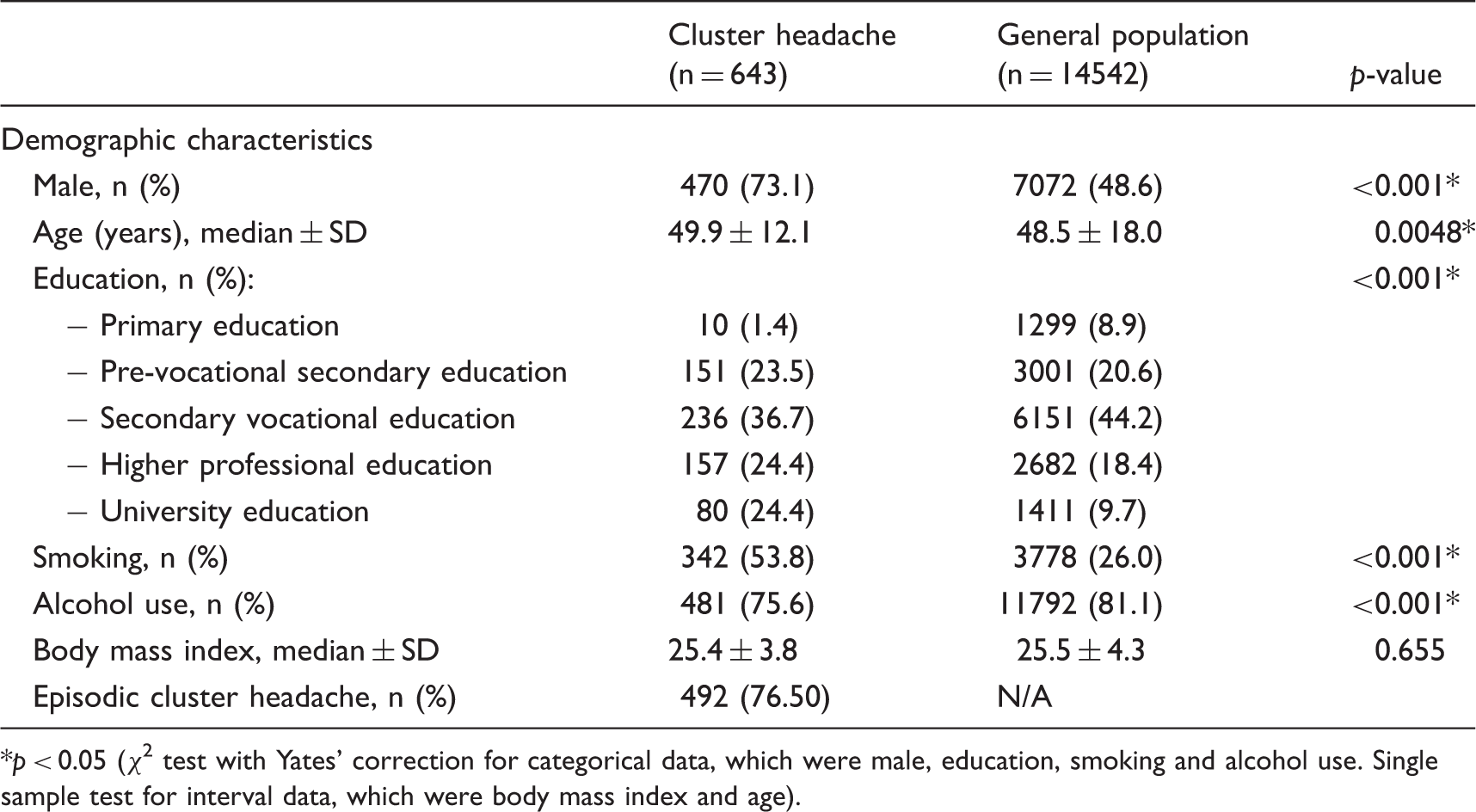
p < 0.05 (χ2 test with Yates’ correction for categorical data, which were male, education, smoking and alcohol use. Single sample test for interval data, which were body mass index and age).
Results
Study population
By August 2014, 756 people with self-reported cluster headache had been invited to this study, of whom 85.1% (643/756) filled out all necessary questionnaires. Of these, 613/643 (95.3%) had received a diagnosis of cluster headache by a physician. A total of 14.542/24.396 (59.6%) of the controls from the general population from the 2014 and 2015 cohorts of the Statistics Netherlands responded to the questionnaire and were included in this study. In the Dutch general population cohort, 3457 (23.8%) people reported having “chronic pain” and 2269 (15.6%) people reported having “headaches”.
People with cluster headache were more often male, higher educated, smokers, and drank alcohol less often compared to the Dutch general population (Table 1).
Cluster headache compared to the general population
Participants with cluster headache more often used illicit drugs (31.7% vs. 23.8%; p < 0.001; Figure 1), cannabis (29.5% vs. 22.7%; p < 0.001), cocaine (8.9% vs. 4.8%; p < 0.001), amphetamine (6.4% vs. 4.2%; p = 0.011), PSI (9.3% vs. 3.9%; p = 0.00) and heroin (1.1% vs. 0.5%; p = 0.037).
Lifetime use of different types of illicit drugs in cluster headache and general population.
Cluster headache compared to people with headache and the chronic pain in the general population
Lifetime use of different types of illicit drugs in the cluster headache, headache and chronic pain subgroup.

Illicit drugs: all drugs; MDMA: 3,4-methylenedioxymethamphetamine; PSI: psilocybin mushroom; LSD: Lysergic acid diethylamide; GHB: gamma-hydroxybutyrate; p-valuea: p-value of comparison cluster headache population to the headache subgroup; p-valueb: p-value of comparison cluster headache population to the chronic pain subgroup.
p < 0.05 (χ2 test with Yates’ correction for categorical data).
Gender differences
Lifetime use of different types of illicit drugs in the cluster headache and general population stratified to gender.

Illicit drugs: all drugs; MDMA: 3,4-methylenedioxymethamphetamine; PSI: psilocybin mushroom; LSD: lysergic acid diethylamide; GHB: gamma-hydroxybutyrate.
p < 0.05 (χ2 test with Yates’ correction for categorical data and Fisher’s Exact test for n < 5).
Males with cluster headache more often used illicit drugs than males from the general population (34.7% vs. 29.2%; p = 0.013), mainly cannabis (33.0% vs. 27.9%; p = 0.019), cocaine (10.4% vs. 6.9%; p = 0.006) and PSI (10.6% vs. 5.5%; p < 0.001; Table 3). There was no difference in illicit drug use between females with and without cluster headache, except for PSI (5.8% vs. 2.3%; p = 0.008).
Age differences
Age distribution of lifetime prevalence of illicit drug use followed the same pattern in people with cluster headache as in the general population and its subgroups (Figure 2). People with cluster headache of all age cohorts, except between 18–24 (55.6% vs. 41.4%; p = 0.502) and 25–30 (58.8 vs. 44.1%; p = 0.127), used more illicit drugs than the general population.
Prevalence of lifetime use of illicit drug stratified to age cohorts.
Episodic versus chronic cluster headache
There were no differences between episodic and chronic cluster headache general illicit drug use (34.4% vs. 30.9%; p = 0.413) or for specific illicit drug use, except for a higher use of MDMA (13.9% vs. 7.5%; p = 0.027) and GHB (4.6% vs. 1.2%; p = 0.015) in chronic cluster headache.
Perceived effects of illicit drug use
Perceived effects of use of different illicit drugs on duration of individual attacks and attack frequency for those who used illicit drugs during a cluster headache episode.

Illicit drugs: all drugs; MDMA: 3,4-methylenedioxymethamphetamine; PSI: psilocybin mushroom; LSD: lysergic acid diethylamide; GHB: gamma-hydroxybutyrate.
Not all patients used the drugs during an attack.
Discussion
In this study, Dutch people with cluster headache more often used illicit drugs during their lifetime than people from the general Dutch population. In particular, cannabis, amphetamine, heroin and cocaine were more used by cluster headache patients. Although it would be thought that this is due to alleviatory effects, most users with cluster headache reported no effect of these illicit drugs on their cluster headache attack frequency or duration when used only during a cluster headache episode. A very limited number reported a positive effect of PSI and heroin on the duration of their individual cluster headache attacks and a positive influence of PSI and LSD on attack frequency. These possible influences of PSI, heroin and LSD should be interpreted with caution, as these drugs were used in only a small fraction of the cluster headache population.
Both in our cluster headache population and in the general Dutch population a higher prevalence of illicit drug use was seen in males, which is in line with earlier studies (5). Males more often exhibit risk-taking behaviour (17). Being a female cluster headache patient has been associated with a decreased response to acute treatment and with more painful nocturnal headache attacks (18). In contrast, it has been suggested that bout frequency and duration are lower in females compared to males (5). These gender differences might influence the use of illicit drugs in women. However, we did not observe an increased prevalence of illicit drug use in female patients.
An increased prevalence of PSI use was found in both females and males with cluster headache. This might be due to the fact that PSI has received Dutch media attention as an alternative cluster headache treatment (19). Its efficacy, however, is limited: In a small retrospective study an acute effect of PSI, and even a termination of a cluster headache period, was only found in half of the few patients studied (11). Further research is therefore needed to shed more light on the acute and prophylactic effects of PSI in cluster headache.
Each cluster headache age cohort in our study used more illicit drugs than their age matched cohort in the Dutch general population, except for the 18–24 and 25–30 age cohorts, which were, however, too small to reach significance. Overall lifetime use of illicit drugs was increased in the younger age groups independent of having cluster headache. This increased prevalence of illicit drug use in younger Dutch generations has been described before and has not been seen in other European countries except for Switzerland (20,21). This seems to confirm the role of cultural differences between countries in drug use.
The increased prevalence of illicit drug use in people with cluster headache compared to people with chronic pain, or further unspecified headache, suggests that increased use is specific for cluster headache and not linked to headache or chronic pain per se. There are several possible explanations for this finding.
First, the question remains whether some illicit drugs actually have alleviatory effects on cluster headache. It is possible that certain illicit drugs may interact with the unknown process that causes cluster headache. Cannabis acts on cannabinoid receptors that are widespread throughout the brain (22). The hypothalamus has cannabinoid receptors and has been implied in the pathophysiology of cluster headache (23,24). In contrast to the sedative qualities of cannabis, cocaine is a strong stimulant, also known for its capacity as a local anaesthetic and vasoconstrictor (25,26). Intranasal cocaine administration is reported to block pain caused by a nitroglycerin-induced cluster headache attack in about 30 minutes (27). However, since the majority of respondents described illicit drugs to have no effect on their cluster headache attacks, it remains questionable whether the possible alleviatory effect of illicit drugs on cluster headache is the actual reason for the increased prevalence of use.
Second, there could be an association between cluster headache and a tendency for addictive behaviour, as suggested before (28,29). This would also be in line with our finding that people with cluster headache are more inclined to smoke.
Third, the reputation of illicit drugs among people with cluster headache combined with the attention that these substances receive on cluster headache blogs, social media, and in some recent publications, may stimulate more patients to try these illicit drugs to treat their cluster headache (30). Last, the placebo effect could have overestimated the effects attributed to the various illicit drugs.
Limitations of this study include the fact that the data analysis needed to be stratified for age groups and gender, because the population data received from the Statistics Netherlands consisted of categorical age data. Age and gender were thus not full co-variates in the analysis and it was not possible to correct for other variables. We therefore tried to give the reader insight into age (Figure 2) and gender distribution (Table 3). Because of the small number of cluster headache patients who used certain drugs, we expect that for those drugs the comparison between females and males could have been underpowered. It is possible that differences were larger than we could demonstrate. The higher education level of cluster headache patients may be a bias of the internet-based recruitment. As higher education is protective towards drug use this might have negatively influenced the results. This could mean that the difference between drug use in the cluster headache versus the general population would be even larger than the difference we found.
The headache subgroup of the general population could have included cluster headache patients. We included data from a representative sample of the Dutch general population (n = 14542), and cluster headache has a known prevalence of 1 in 1000 patients (31). As such, the sample could include 14–15 cluster headache patients. We expect that all these possible cluster headache patients are listed in the headache subgroup, which would amount to 14–15 out of 2268 people. Even if this were so, we expect that this small number of potential cluster headache patients did not influence the outcome of the headache subgroup.
Our questionnaire did not ask about motives for drug use and the time between filling out the questionnaire and drug use itself. Furthermore, it should be noted that our findings on effects of illicit drugs on cluster headache were all self-reported and should thus be met with caution, since the placebo effect could have overestimated the effects.
In conclusion, in the Dutch cluster headache population there is a higher prevalence of illicit drug use compared to the general Dutch population. This might be due to an actual acute or prophylactic effect, but also to a common pathophysiology between cluster headache and sensitivity for drug use. Another explanation could be a false conviction in people desperately seeking relief of their cluster headache and/or to the almost mythological reputation of illicit drugs in the cluster headache community.
Article highlights
People with cluster headache have a higher prevalence of illicit drug use compared to the general Dutch population. Most illicit drug users report no effect of illicit drugs on attack duration and attack frequency. A limited number report a positive effect of PSI and heroin on attack duration. A positive influence on attack frequency is reported for PSI and LSD use. However, these drugs were used in only a small fraction of the cluster headache population studied.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MD Ferrari reports grants and consultancy or industry support from Medtronic, Amgen, Lilly and Electrocore, and independent support from NWO, ZonMW, NIH, European Community, Dutch Heart Foundation, and Fonds Nuts Ohra. This study was supported by grants from the Netherlands Organisation for Scientific Research (NWO) and the European Union's Seventh Framework programme (2007-2013) under grant agreement no. 602633 to MDF. IF de Coo reports support for conference visits from Electrocore. WC Naber, J Haan and R Fronczek report no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.