
Abstract
Objectives
The aim was to evaluate the association of self-perceived levels of attention deficit and hyperactivity symptoms with non-migraine and migraine headaches among university students. We also evaluated their association with migraine aura.
Methods
Study subjects were all participants in the internet-based Students Health Research Enterprise. Scores were built to evaluate global attention and hyperactivity symptom levels, self-perceived attention deficit levels and self-perceived hyperactivity symptom levels based on the Adult Attention Deficit and Hyperactivity Disorder Self-Report Scale (ASRS v1.1.). We used standardised questions to classify headache and group participants into “no headache,” “non-migraine headache,” “migraine without aura” or “migraine with aura”.
Results
A total of 4816 students were included (mean age 20.3 ± 2.8 years; 75.5% women). Compared with participants without headache, we found significant associations between global ADHD scores and migraine. Students in the highest quintile of global ASRS scores had adjusted odds ratio (aOR) of 1.95 (95% CI 1.56–2.45) when compared to the lowest. This association was mainly driven by an association between self-perceived hyperactivity and migraine with aura. The aOR for migraine with aura was 2.83 (95% CI 2.23–3.61) for students in the highest quintile of hyperactivity. No significant association was found for any attention and hyperactivity symptom level measure and non-migraine headache and between self-perceived levels of attention deficit and migraine.
Conclusions
Among students in higher education in France, self-perceived levels of attention deficit and hyperactivity symptoms were selectively associated with migraine. The association was strongest for the hyperactivity domain and migraine with aura.
Introduction
Attention deficit and hyperactivity disorder (ADHD) is a paedopsychiatric disease characterised by inattention, impulsivity and hyperactivity symptoms. There are three subtypes: Predominantly inattentive, predominantly impulsive and hyperactive, or both forms combined. The annual prevalence in children (4–17 years old) is approximately 5% (1). The extent to which ADHD persists in adults is largely unknown, and the clinical importance of these symptoms among adults has only recently been recognised (2). In population-based studies, information on ADHD is often ascertained by auto-evaluations, exploiting only some of the Diagnostic and Statistical Manual of Mental Disorders IV criteria. However, validated questionnaires exist that allow classification of ADHD in population-based settings (3,4).
Migraine and attention deficit and hyperactivity symptoms represent a substantial public health burden, since they involve increases in public spending and substantial individual burden (5,6). While studies have described links between migraine and ADHD in children (7,8), clinical and population-based studies on their association with ADHD symptoms in adulthood are scarce (9). In particular, no data exist among university students, a population in which an association could lead to major consequences for academic performance and general well-being (10–12).
The objective of this study was to evaluate the association of self-perceived levels of attention deficit and hyperactivity symptoms with headache and migraine among university students. While several covariates have been linked with attention deficit and hyperactivity symptoms or migraine, the causal association pattern (i.e. confounding vs. intermediate factors) remains unclear. Thus, we further aimed to evaluate the influence of a priori defined causal association patterns of covariates in several a priori selected modeling approaches to provide insights to potential confounding or effect modification (13).
Methods
Study population
Study subjects were participants in the internet-based Students Health Research Enterprise (i-Share) project, a prospective population-based cohort study of students of French-speaking universities and higher education institutions. The i-Share project was initiated by the Universities of Bordeaux and Versailles Saint-Quentin (France). To be eligible to participate, a student had to be officially registered at a University or higher education institute, be at least 18 years of age, able to read and understand French, and provide informed consent for participation.
Data of this study mainly come from participants at the University of Bordeaux, where active recruitment started in February 2013. Students were informed about the purpose and aims of the study by flyers, information stands at registrations, during lectures, and via social media and newsletters (www.i-Share.fr). Furthermore, a group of trained students informed their peers about the study and collected contact information to initiate the online recruitment process. Enrollment followed a two-step process: First, a formal pre-registration on the i-Share online portal was required. In the second step, the student finalised the registration process and completed self-administered online questionnaires. Only students who filled out the entire baseline questionnaire were eligible for our analyses. The baseline questionnaire asked information on the participant’s health status, personal and family medical histories, socio-demographic characteristics, and lifestyle habits. For this particular study, we used available data as of 16 March 2015 (Figure 1).
Flowchart of the study population.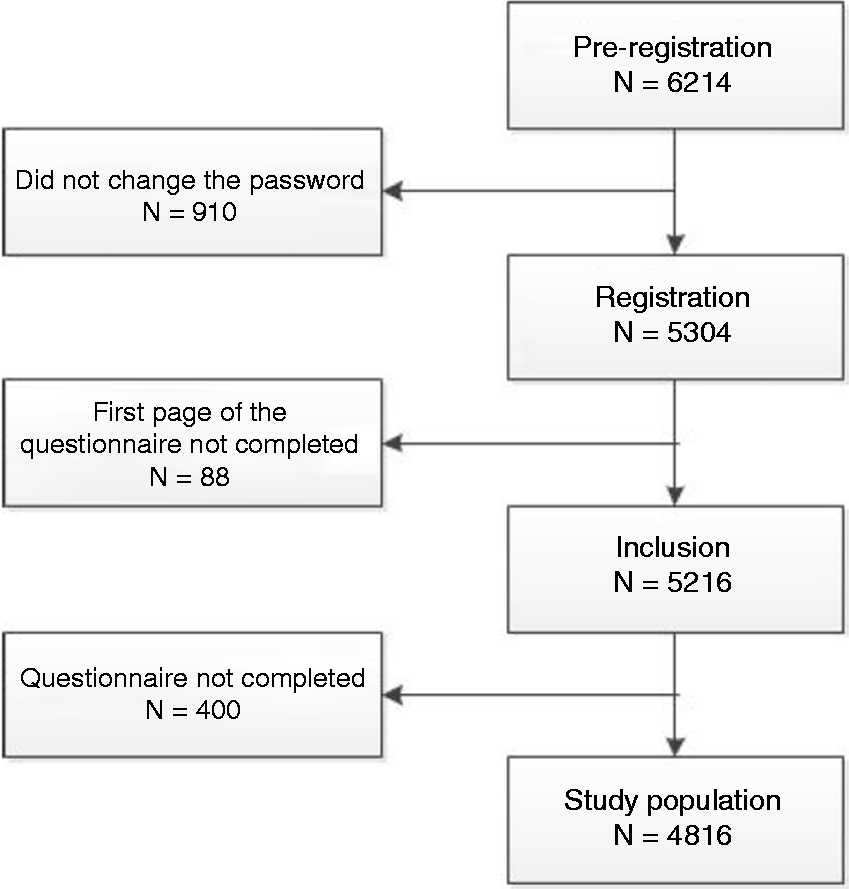
The i-Share project from which this study originated was approved by the Commission Nationale de l’Informatique et des Libertés (CNIL) [DR-2013-019].
Assessment of attention deficit and hyperactivity symptom levels
Students were asked to complete the Adult ADHD Self-Report Scale (ASRS-v1.1) (3,4) concerning their behaviours over the last six months. The scale consisted of six items providing global information on attention and hyperactivity levels. The first four items are related to attention deficit whereas the last two are linked to hyperactivity. Each question had five answer levels, ranging from never to very often. We applied an unweighted scoring for each question and assigned a point value for each response level (never = 0, rarely = 1, sometimes = 2, often = 3, very often = 4) as previously suggested (4,14). The points were then summed up to build a global score (ranging from 0 to 24), a score for the self-perceived attention symptom level (ranging from 0 to 16), and score for the self-perceived hyperactivity symptom levels (ranging from 0 to 8). We categorised the total and attention symptom level scores in quintiles and the hyperactivity level score in quartiles, allowing evaluation of non-linear association patterns. Lastly, we also dichotomised the total score according to the ASRS v1.1 diagnostic criteria for ADHD (4) and classified participants as having ADHD or not.
Assessment of headache and migraine
On the baseline questionnaire, participants were asked: “Have you ever had headache attacks of several hours in the last 12 months?” Participants who did not report headaches during the previous 12 months were included in the “without headache” category. Participants who reported headaches were asked further details about their headache symptoms, including unilateral location, pulsating quality of pain; inhibition of daily activities; aggravation by routine physical activity; nausea or vomiting; and sensitivity to light or sound. Responses were used to classify participants into “non-migraine headache” or “migraine” categories. Participants were further asked whether they had visual, sensory or motor disturbances before the migraine attack. Responses were used to classify those indicating migraine into migraine with aura or migraine without aura.
To establish migraine classification in our study, we used the “probable migraine” category of the International Classification of Headache Disorders 3rd edition (beta version) (15). We distinguished between “no headache,” “non-migraine headache” and “migraine.” In further analyses, we also took migraine aura status into account.
The migraine information in i-Share was validated as previously described (16). In brief, we used the validated French version of the ID migraine™ questionnaire (17,18) to validate migraine self-reports. Compared to the migraine classification of the i-Share questionnaire, only eight of 139 participants in the validation study were not classified as having migraine by the ID migraine™ questionnaire, resulting in a predictive value positive of 90.9% (16).
Statistical analyses
We compared the characteristics of the study population with respect to their attention deficit and hyperactivity symptom level status (very low, low, medium, high and very high) by contrasting means and frequencies.
To evaluate the association between self-perceived levels of attention deficit and hyperactivity symptoms with headache status, we used a multinomial logistic regression model. Multinomial logistic regression is an extension of binary logistic regression, in which the outcome variable is allowed to have more than two categories (in our case the three or four headache status categories). Each calculated odds ratio (OR) is simultaneously compared with two reference categories, one for the exposure (in our case attention deficit and hyperactivity symptom level categories) and one for the outcome. We calculated OR and 95% confidence intervals (95% CI) using participants in the lowest attention deficit hyperactivity score categories and those without headache as the reference group.
We used Directed Acyclic Graphs (DAGs) (19,20) to classify covariates in potential common causes of both our exposure and outcome (i.e. potential variables causing confounding) or potential consequences of our exposure that also relate to our outcome (i.e. potential intermediates). DAGs graphically represent causal effect patterns between covariates that help in the identification of confounding factors that must be controlled for as well as intermediates (Figure 2). They further allow evaluation of whether adjustment for intermediates causes bias (21,22). The resulting hypothesised causal structure allowed for the development of specific multivariable models addressing the different causal association patterns.
Directed acyclic graph.
We considered the following variables as potential covariates in the “confounding” model: Gender (men, women), age (18, 19, 20, 21 years or more), parents’ headache status (yes/no) and family economic condition in childhood (very comfortable, comfortable, correct, hard or very hard). As “intermediate” variables, we considered employment while being a student (yes/no), self-reported physician-diagnosed depression (yes/no), study level (first, second, third, fourth or higher year of post-secondary education), recent change in field of study (yes/no), alcohol consumption (never or once a year, several times a year, once a month, once a week or less, two to three times a week, four to seven times a week), current tobacco consumption (yes/no), cannabis consumption (yes/no) and consumption of other drugs (yes/no). The following variables could not clearly be assigned to either the “confounding” or the “intermediate” variable set and were considered in a separate model (“other”): Current place of living (parent’s residence, university residence, apartment, other), sports practice (yes/no), extracurricular activities (yes/no) and sleep quality (good or pretty good, neither good nor bad, pretty bad or bad).
In addition, we estimated the effect of ADHD on headache status as a binary variable with an inverse-probability-of-treatment weights (IPTW) using a weighted logistic regression model to ensure that control for potential intermediates by using a standard logistic regression model did not introduce bias (21). Bias can be introduced when adjusting for a consequence of the exposure that is also determined by an unmeasured factor, which in addition is also a risk factor for the outcome (21,22).
We performed all analyses in SAS (version 9.3; SAS Institute Inc, Cary, NC) and we considered a two-tailed p-value of less than 0.05 as statistically significant.
Results
Characteristics of the i-Share cohort by self-perceived attention deficit and hyperactivity levels (n = 4816).

The proportion of students with a bad sleep quality was 16.7% higher for students reporting the highest category of self-reported attention problems and hyperactivity compared with students with a low self-perceived attention and hyperactivity symptom level. Students in the highest quintile of attention and hyperactivity symptoms reported depression 12.8% more often than students in the lowest. A family history of headaches was present in 10.3% of students in the highest quintile of level of attention deficit and hyperactivity symptoms compared with students in the lowest. Students with a high level of attention deficit and hyperactivity symptoms reported a worse financial situation during their childhood compared to those with a low level of self-perceived attention deficit and hyperactivity symptoms. Tobacco, cannabis, and other illicit drug consumption were increased with increasing levels of attention deficit and hyperactivity symptoms in our study population.
Multinomial logistic regression of headache and migraine with self-perceived levels of attention and hyperactivity (n = 4816).

CI: confidence interval; Reference: no headache.
Note: Adjusted for: “confounding” gender, age, parents’ headache status, family economic condition in childhood); “intermediates” (self-reported physician-diagnosed depression, paid employment as a student, study level, recent change in field of study, alcohol consumption, current tobacco consumption, cannabis consumption, consumption of other drugs); “others” (current place of living, sports practice, extracurricular activities, sleep quality).
Multinomial logistic regression of headache and migraine with self-perceived levels of attention (n = 4816).

CI: confidence interval; Reference: no headache.
Note: Adjusted for “confounding” variables: gender, age, parents’ headache status, family economic condition in childhood); “intermediates” (self-reported physician-diagnosed depression, paid employment as a student, study level, recent change in field of study, alcohol consumption, current tobacco consumption, cannabis consumption, consumption of other drugs); “others” (current place of living, sports practice, extracurricular activities, sleep quality).
Multinomial logistic regression of headache and migraine with self-perceived levels of hyperactivity (n = 4816).

CI: confidence interval; Reference: no headache.
Note: Adjusted for “confounding” variables: gender, age, parents’ headache status, family economic condition in childhood); “intermediates” (self-reported physician-diagnosed depression, paid employment as a student, study level, recent change in field of study, alcohol consumption, current tobacco consumption, cannabis consumption, consumption of other drugs); “others” (current place of living, sports practice, extracurricular activities, sleep quality).
ADHD and headache status: Comparison of logistic regression and inverse-probability-of-treatment weights analyses (n = 4816).

ADHD: Attention Deficit Hyperactivity Disorder; CI: confidence interval; IPTW: inverse-probability-of-treatment weights; Reference: no headache.
Note: Adjusted for gender, age, parents’ headache status, family economic condition in childhood, weight, self-reported physician-diagnosed depression, paid employment as a student, study level, recent change in field of study, alcohol consumption, current tobacco consumption, cannabis consumption, consumption of other drugs, current place of living, sports practice, extracurricular activities, sleep quality.
Discussion
Results of this large, cross-sectional study among university students show an association of self-perceived attention deficit and hyperactivity symptom levels with migraine. The association increased gradually, suggesting a dose-dependent relationship. We observed the highest adjusted OR for the association between self-perceived hyperactivity level and migraine with aura.
The pattern of association was similar for each modeling setup, suggesting that the variables we considered a priori did not confound the association, nor was the association substantially mediated. However, ORs attenuated when adding either covariates considered “intermediates” or “other,” potentially suggesting an influence of these variables on the association of self-perceived attention deficit and hyperactivity levels on migraine. In addition, the IPTW analysis changed the results of the impact of ADHD on migraine when taking intermediate and potential confounding factors into account, suggesting influence due to potentially inappropriate control for intermediate covariates in this setting (21,22).
Comparisons with previous studies
We are not aware of any other population-based study directly evaluating the association of attention deficits and hyperactivity symptom levels and headache/migraine among young adults. The lack of prior studies may be related to the fact that these symptoms are recognised mainly as a disorder of childhood. Recent evidence, however, suggests that ADHD among adults may not simply be a childhood-onset neurodevelopmental disorder (23). Among children, having both a headache and ADHD are common conditions and links between the two have been described previously (7,8,24). In a population-based study among children between the age of 5–11 years, no association between ADHD and tension-type headache or migraine was found (7) but hyperactivity-impulsivity symptoms could be linked with migraine (relative risk 2.6, 95% CI: 1.6–4.2) (7). This result supports our finding, that mainly the hyperactivity aspect of ADHD is associated with migraine. In a cross-sectional survey of 4921 first-year students at the University of Leuven in Belgium, up to 8.3% had symptoms of ADHD (25). While headache was not evaluated, students with ADHD had a variety of comorbid psychiatric symptoms and poor academic performance.
In our multivariable modeling approach, we evaluated various causal association patterns of covariates. While the association remained overall robust, we found a variation of our effect estimates of up to 22%, indicating the importance of a priori considering the expected links between exposure, outcome, and covariates (19,26). In particular, adjusting for potential consequences of the exposure (in our study self-perceived attention and hyperactivity symptom levels) appears to require a specific modeling approach due to the influence of potential unmeasured covariates or selection bias in this setting.
Our modeling approach considered depression as a consequence of hyperactivity symptoms. Another possibility is to consider depression rather as a comorbidity of migraine. In 2014, in a study of adolescents aged from 12 to 17 years, Blaauw et al. found that migraine was comorbid with depression/anxiety symptoms (risk ratio of 2.1 (95% CI: 1.6–2.6)) (27).
Meaning and implications
As both symptoms of attention deficit and hyperactivity and migraine are frequent and disabling conditions among young adults, potential links may not only result in personal discomfort but also impact academic performance (11,25,28). Thus, students with migraine should be evaluated for symptoms suggestive of ADHD, particularly hyperactivity symptoms. Solutions for students with symptoms of ADHD include self-monitoring (29) and to adapt exam settings for students suffering from these symptoms. Such an intervention is already in place in several universities, where students with a clinical diagnosis of ADHD or impulsivity do their exams in a different room so that they can stand up and move (30,31).
Strengths and limitations
Strengths of our study include the large number of students, the use of standardised assessment tools, available information on a large number of potential confounding and intermediate factors, and the use of modeling approaches that took distinct causal association patterns between exposure, outcome, and covariates into account. Further, a large proportion of the students included in this study were in their first year of post-secondary education, which represents a crucial period for their health and evolution of lifestyles (32).
The following limitations should be considered when interpreting our results. First, our study was cross-sectional, not allowing us to make any inference regarding the timing of the relationship between symptoms of attention deficit and hyperactivity symptoms and migraine as well as interrelationships with covariates. However, we decide a priori on cause and effect patterns that we translated into our modeling approach. Nevertheless, it remains to be determined whether attention deficit and hyperactivity symptoms precede headache and migraine or whether both conditions are the consequence of the same underlying mechanisms. Second, evaluation of migraine and attention deficit and hyperactivity symptoms was conducted with self-administered questionnaires, and misclassification is possible. However, we have no reason to believe that misclassification would be directly related to our research question, which is also supported by increased effect estimates only being observed for students with migraine but not being observable for the non-migraine headache group. Third, in our study, we did not aim to evaluate the influence of a diagnosis of ADHD but, rather, the influence of a self-perceived continuum of attentional problems and hyperactivity symptom levels with headache status. Fourth, the definitive choice for the causal association pattern also does not exclude bias due to misconception or variables not taken into consideration. Lastly, participants in the i-Share cohort come mainly from the University of Bordeaux, and our finding may not apply to other settings. However, we have no reason to believe that our findings are only observable among students enrolled at the University of Bordeaux.
Conclusion
Results from this large cross-sectional study among university students show consistent associations of self-perceived attention deficit and hyperactivity symptom levels with migraine. We found the strongest associations for the hyperactivity domain and individuals with migraine with aura but no associations with non-migraine headache. Future studies are warranted to investigate the mechanisms underlying these associations and to evaluate whether both attention deficit and hyperactivity symptoms and migraine have an impact on academic performance, and how to prevent such impact.
Clinical implications
Patients seen for migraine should be evaluated for symptoms of attention deficit or hyperactivity; in particular, those with migraine with aura. These patients may benefit from a treatment approach that considers both attention deficit/hyperactivity symptoms and migraine.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors have completed the ICMJE uniform disclosure form at ![]() . TK reports having received honoraria from Lilly for methodological advice, from Novartis and Daiichi Sankyo for lectures on epidemiology and research methods, and from the BMJ for editorial services. TK has provided methodological expert advice to CoLucid and Amgen, for which the Charité – Universitätsmedizin Berlin has received unrestricted funds. All other authors report no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
. TK reports having received honoraria from Lilly for methodological advice, from Novartis and Daiichi Sankyo for lectures on epidemiology and research methods, and from the BMJ for editorial services. TK has provided methodological expert advice to CoLucid and Amgen, for which the Charité – Universitätsmedizin Berlin has received unrestricted funds. All other authors report no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The i-Share project is supported by the French National Research Agency (Agence Nationale de la Recherche, ANR), grant number [ANR-10-COHO-05]. This particular study was funded by a grant from the “Future Investments” program in the framework of the IdEx University of Bordeaux program (HEADS program), grant number [ANR-10-IDEX- 03-02].