
Abstract
Objective
Tension-type headache is
*These authors contributed equally to this work.
Methods
Clinical characteristics and demographics were systematically and prospectively collected between March 2014 and December 2015 from 15 participating hospitals in Chongqing, using a semi-structured face-to-face interview. All patients were asked to complete a headache diary for at least 4 weeks.
Results
Out of 1832 patients with headache, 150 patients (97 female/53 male, 44.56 ± 11.9 years old) were diagnosed with tension-type headache based on the standard International Classification of Headache Disorders, 3rd edition beta version, and interestingly, 114 (76%) patients were diagnosed with tension-type headache based on the alternative criteria. One patient was excluded because only two of the four characteristics were fulfilled. Thirty-five (23.3%) patients did not meet the alternative criteria because of associated symptoms, including mild nausea (n = 6), photophobia (n = 1), and phonophobia (n = 28). All patients with TTH had mild or moderate headaches, 98.0% of patients suffered from non-pulsating headaches, 99.3% of patients said their headaches were not aggravated by routine physical activity, and 77.3% of patients had bilateral headache.
Conclusions
Non-pulsating headaches and headaches that are not aggravated by routine physical activity may represent core criteria for screening patients with tension-type headache. Nausea might not be an exclusion feature for diagnosis of TTH, but an important criterion for screening. Further studies are needed.
Introduction
Tension-type headache (TTH) is the most prevalent primary headache disorder, occurring in 20–60% of the general population (1,2). The costs associated with treating TTH are higher than for migraine, because more people suffer from TTH (1). Decreased work efficiency and reduced social activity are reported by up to 60% of TTH patients (3). However, the accurate diagnosis of TTH has received limited attention over the last few decades.
TTH is characterized by nothing more than a pain in the head (4). The definition depends exclusively on clinical symptoms, which can be found in other headache types such as migraine (5,6). In fact, these headaches are often distinguished by difference of clinical features based on the International Classification of Headache Disorders, 3rd edition beta version (ICHD-3 beta) (7).
Further diagnostic criteria for TTH (which we have called alternative criteria) have been proposed to exclude migraine that phenotypically resembles TTH according to ICHD-3 beta criteria. The alternative criteria define a more specific core TTH syndrome, but have not been well tested (8).
We surveyed successive TTH patients attending neurological clinics from 15 hospitals in China to explore the clinical characteristics and diagnosis.
Methods
Patients and clinical setting
This multicenter clinical study was performed at 15 participating hospitals in Chongqing, China. We prospectively enrolled consecutive patients diagnosed with TTH from March 2014 to December 2015 in neurological clinics. The TTH diagnosis was based on the ICHD-3 beta criteria for infrequent episodic tension-type headache (iETTH) and frequent episodic tension-type headache (fETTH) (codes 2.1 and 2.2) and chronic tension-type headache (CTTH) (code 2.3), using a semi-structured face-to-face interview as described previously (9).
Participating neurologists were trained by headache specialist Jiying Zhou in the lead headache clinic. A pioneer trial was conducted in the first month. All enrolled patients were followed up by three neurologists (Xueying Kong, Jinjin Chen, and Huahua Jiang) in the lead headache clinic. Headache characteristics (position, property, duration, intensity, aggravation after physical activity, associated symptoms, etc.) were validated by telephone interview. In addition, medical records were reviewed every week to verify the diagnosis. If the diagnosis was contentious, Jiying Zhou decided the final diagnosis after telephone interview with the patient. Two medium-term meetings were held to conclude the progress of the project and to solve problems that arose in January and August 2015. In the latter part of the study, Xueying Kong and Jinjin Chen from the lead clinic collected and analyzed the data.
Inclusion criteria were for subjects to be between 18–65 years of age, have a TTH diagnosis based on ICHD-3 beta criteria, headache more than 1 year, and the ability to complete a headache diary. Exclusion criteria were an International Headache Society diagnosis of medication-overuse headache (MOH), current or planned pregnancy or breastfeeding, migraine headache for more than 1 day a month, serious somatic or psychiatric illnesses, other pain disorder (e.g. arthritis) requiring analgesic treatment, and failure to complete baseline diary recordings of headache activity and medication use.
Patients presenting at the participating clinics with headache were interviewed. Participating neurologists conducted detailed interviews to determine the demographic and socioeconomic characteristics, headache features, triggers, family history of headache, mood disturbances, Hospital Anxiety and Depression Scale (HADS), and Headache Impact Test (HIT-6). In addition, neurologists performed manual palpation (pressure pain examinations) in each patient in seven locations including frontal muscle, masseter muscle, temporal muscle, alary muscle, sternocleidomastoid muscle, trapezius muscle, and splenius cervicis muscle (10). Symmetrical muscles were palpated simultaneously followed by unilateral palpation to allow for accurate side-to-side comparison.
After their first visit, all enrolled patients received a headache diary and were told to record headache characteristics, including type and amount of medication used for at least 4 weeks (11). Headache frequency, intensity, associated symptoms, and medication consumption at the time of the initial consultation were recorded as baseline values. The headache diary was examined and verified to exclude probable migraine.
The study was approved by the local ethics board and informed consent was obtained from all participants.
Follow-up response
The baseline assessment included 1 month of headache recording. Afterwards, patients were generally treated empirically with amitriptyline (25–50 mg per day), Chinese medicine (Yangxue Qingnao Granule, 12 g per day) (12), or a combination of both based on doctors’ judgements and patients’ preferences. Seven patients received lifestyle adjustments as treatments due to low frequency of headaches. Patients recorded all headaches in a daily headache diary.
Data processing and statistical analysis
Statistical analysis was performed using SPSS software, version 20.0 (Chicago, IL, USA). Patients that fulfilled ICHD-3 standard criteria for ETTH and CTTH were tested for alternative criteria listed in the alternative of ICHD-3 beta (code A2). Continuous variables are presented as means ± SD, and Student’s t-test was used to evaluate differences between the two groups. Categorical variables are presented as frequency distributions (N, %), and Chi-square or Fisher’s exact test was executed where applicable. Significance was set at p ≤ 0.05 for all statistical tests.
Results
A total of 13,537 patients visited the participating neurological clinics and 1832 headache patients were screened during the study period. Of these, 397 patients with tension-type-like headaches were selected for further screening. Twenty-eight patients were excluded based on a diagnosis of secondary headache. The remaining 271 patients were diagnosed with TTH according to ICHD-3 criteria. Among them, 94 (34.7%) patients were excluded after recording migraine or probable migraine (PM) symptoms in their headache diary during screening. An additional 27 (10.0%) patients dropped out. In the end, 150 (55.3%) patients were enrolled in the study (Figure 1).
Flowchart of patients and diagnoses during the run-in period.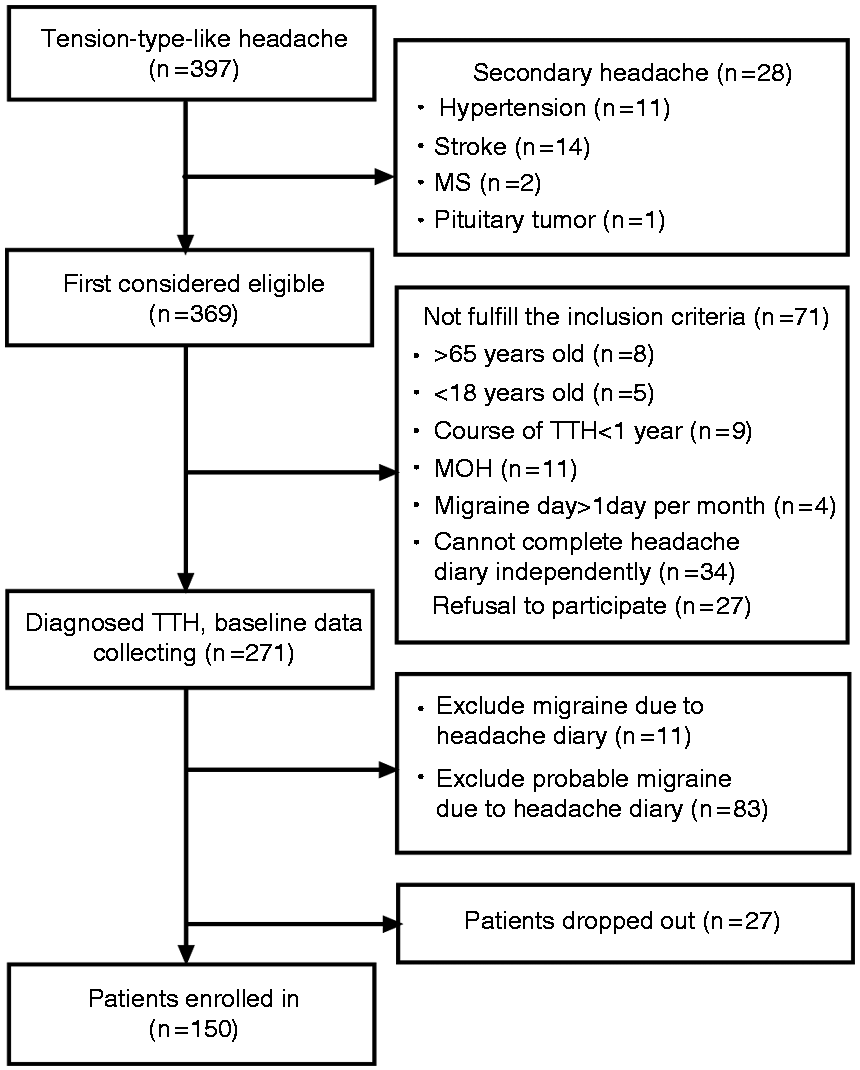
Demographics and clinical characteristics of fETTH and CTTH by ICHD-3β standard criteria
Demographics and clinical features of fETTH and CTTH.
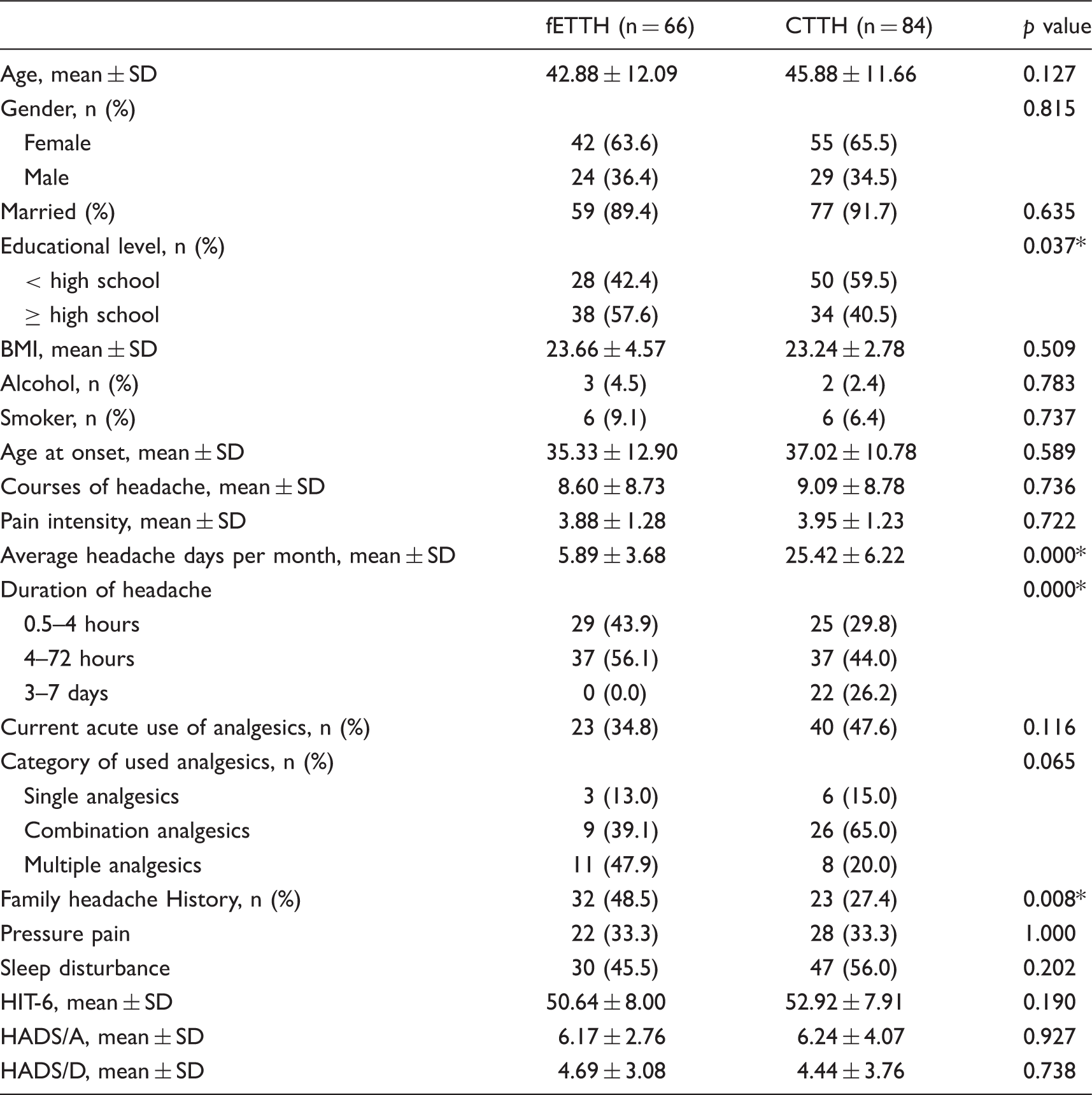
fETTH: frequent episodic tension-type headache; CTTH: chronic tension-type headache; BMI: Body Mass Index; HIT-6: Headache Impact Test; HADS: Hospital Anxiety and Depression Scale. Note: *p ≤ 0.05.
CTTH patients were more likely to be older, female, have a lower educational level, use more analgesics, and suffer from sleep disturbance than fETTH patients (Table 1). The overall mean time of headache duration was significantly longer for CTTH patients than fETTH patients.
Notably, 33% of CTTH patients had muscle pressure pain (Table 1). The same was reported by patients with fETTH. Muscle tenderness had no relationship with headache intensity, course of headache, and headache frequency.
In the 150 TTH patients, the quality of the headache was described as pressing (46%) and dull pain (19%). Tightening pain was reported by 11% of patients, whereas pulsating pain was described by 2% of patients. Stabbing pain appeared in 1% of patients, 18% of patients suffered headache of more than one quality, and 3% of patients accounted to another headache quality that is hard to define.
Testing of the TTH standard and alternative criteria of the ICHD-3 beta
Diagnostic features of TTH according to standard and alternative criteria.

Note: *p ≤ 0.05.
The differences in criteria were the headache characteristics and the associated symptoms. One patient was excluded because only two of the four characteristics were fulfilled. The other 35 patients were excluded because of associated symptoms, including mild nausea (n = 6), photophobia (n = 1), and phonophobia (n = 28).
All patients with TTH had mild or moderate headaches, 98.0% (147of 150) suffered from non-pulsating headaches, 99.3% (149 of 150) said their headaches were not aggravated by routine physical activity, and 77.3% (116 of 150) had bilateral headache, according to standard criteria. There was no difference between patients with fETTH and those with CTTH in terms of headache features.
Socio-demographic characteristics of TTH patients according to standard and alternative criteria
Socio-demographic distribution of patients diagnosed with tension-type headache based on standard and alternative criteria.

Follow-up response
One hundred and forty-three patients received medication. The overall response rate was 71.3% (n = 107, 68 females, 39 males), including telephone and face-to-face interviews. The main reasons for lack of follow-up were patient refusal and changed telephone number. Age, gender, HIT scores, and HADS scores did not differ between participants and non-participants.
The median follow-up time was 5 months (range: 1–12 months). Three patients had a migraine-like combined headache less than 1 day a month. None of the other patients have reported a migraine or other type of headache to date.
Discussion
The validation of diagnostic criteria presented in the ICHD are lacking and highly needed in TTH. We therefore evaluated the standard criteria and alternative criteria of ICHD-3 beta to explore the socio-demographic, clinical characteristics, and follow-up response between the two groups. No significant difference was found except the associated symptoms, such as nausea and phonophobia.
In this multicenter study, we classified all patients with ETTH and CTTH. Indeed, all ETTH patients had at least two headache days per month, another way of saying they were fETTH. On the whole, there were more female TTH patients than males in this study, in agreement with previous studies (13,14). We also observed a strong association between TTH prevalence and education; prevalence increased with education level in fETTH patients, but declined with increasing education level in CTTH patients.
Throbbing/pulsating pain was one of the most prominent migrainous features. The frequency of pulsating pain for TTH in previous studies has varied from 17.5% to 59.9% (5,8,15). Notably, 2% of TTH patients had a pulsating headache in our survey. This wide range of difference was most likely due to various classification criteria of TTH, or inclusion criteria of study groups. Pulsating pain might not be an exclusion feature for diagnosis of TTH, but is an important criterion for screening.
The ICHD-3 diagnostic criteria include shorter duration headaches. There were differences in the duration of headache attacks between fETTH and CTTH patients. CTTH headaches were longer than fETTH headaches. In addition, 74 patients (49.3%) had headaches lasting 4–72 hours, which overlaps with the criteria for migraine. This may make it difficult to distinguish migraine from TTH.
The etiology of TTH is thought to be muscular and pericranial muscle tenderness, which is a unique feature of TTH (16). A previous study in Denmark indicated that 77% of adults with CTTH, and 37% of those with ETTH, had muscle tenderness, investigated on manual palpation only (10). In our study, 33% of patients with CTTH and fETTH had muscle pressure pain. Methodological differences and differences between study populations might explain the discrepancy between these results. Several lines of evidence had revealed that migraine was accompanied by muscle tension or neck pain (17–20). Based on these findings, pericranial muscle tenderness may not be a good criterion for distinguishing between TTH and migraine.
Our study showed a family history of headache in 48.5% of fETTH patients and 27.4% of CTTH patients, in agreement with previous studies (21). This might be attributed to the high prevalence of infrequent and frequent ETTH (22,23). A twin study of ETTH showed that environmental influences were predominantly responsible for ETTH and that genetics had little or no influence (24).
Migraine and TTH were best distinguished by aggravation of pain following routine physical activity. This criterion was more indicative than unilaterality or pulsating quality. Diagnosis of TTH is currently based on the patient’s evaluation of the headache characteristics, because biomarkers or definitive headache features are lacking (25). In our survey, all patients fulfilled three of the four alternative criteria, which are proposed to be more specific than standard criteria. Furthermore, almost all patients reported that their headaches were not aggravated by routine physical activity. In contrast, a Korean study showed that 81.2% of patients fulfill three of the four characteristics (8). The differences might be explained by stricter inclusion criteria and baseline headache recordings, or by different study samples.
Previous studies showed that a minority of patients fulfilled the diagnostic criteria of CM and CTTH (26,27). That was possible when two of the four pain characteristics were present and headaches were associated with mild nausea (28). Therefore, associated symptoms are important for distinguishing between migraine and TTH. For CTTH to be diagnosed, mild nausea, photophobia, or phonophobia may be present. For ETTH diagnosis, photophobia or phonophobia can be present. The majority of TTH patients in this study were diagnosed according to standard criteria, but the missing alternative criteria were due to associated symptoms, such as mild nausea (4.0%), photophobia (0.6%) and phonophobia (18.7%). In conclusion, our findings indicate that three of the four headache characteristics did not reduce the diagnostic sensitivity. However, mild nausea was only present in CTTH (4.0%), and 19.3% of patients had photophobia or phonophobia in our study, therefore further studies are needed to verify the benefits and risks of removing the associated symptoms, and the application the alternative TTH diagnosis criteria.
Distinguishing between migraine/PM and TTH based on ICHD-3 criteria is complicated because each headache type has characteristics of the other. Non-pulsating headaches and headaches that were not aggravated by routine physical activity were present in almost all TTH patients. These may represent useful diagnostic criteria for TTH screening, thereby avoiding over-diagnosis caused by a lack of distinctive TTH features. However, in early reports, pain was shown to be aggravated by physical activity in 21.1–31.8% of TTH suffers (5,15,20). The explanation for the difference in distribution may be the progression of knowledge of TTH.
There are some limitations to be considered. This study was clinic-based and the data cannot estimate the prevalence of TTH in the general population. The findings require further study and cannot be extrapolated to the general population directly. Furthermore, the intermediate headache status was not compared between baseline and follow-up, so the precise course of the headaches was not clarified. Another limitation is that the strict inclusion criteria make it impossible to calculate the sensitivity and specificity of the criteria and might narrow the range of patients included.
In summary, this study provided the clinical features and first testing of TTH in a multi-center study in China. TTH was female predominant, with an onset at middle age. A mild or moderate headache intensity was the core symptom of TTH. Non-pulsating headaches and headaches that are not aggravated by routine physical activity might represent important means of identification for screening patients with headache. Fulfilling three of the four headache characteristics in the alternative criteria did not reduce the diagnostic sensitivity, but further studies are needed to verify the benefits and risks of removing the associated symptoms, and the application the alternative TTH diagnosis criteria.
Clinical implications
This study details the clinical characteristics of TTH. TTH predominantly occurs in middle-aged women. CTTH patients are mainly older, female, have a lower education level, use more analgesics, and suffer more from sleep disturbance compared with fETTH patients. Non-pulsating headaches and headaches that are not aggravated by routine physical activity may represent important means of identification for screening patients with headache.
Footnotes
Acknowledgement
We thank all the physicians. Without their meticulous follow-up, this study could not have been completed. We apologize for not being able to list all the names of physicians who participated in the study owing to limited space. We also thank the chief investigators of each institute.
The authors thank the research support from Tasly Pharm Company.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.