
Abstract
Objective
To examine treatment utilization patterns and safety of onabotulinumtoxinA for the prophylactic treatment of chronic migraine in routine clinical practice.
Background
Clinical trials support onabotulinumtoxinA for the prophylaxis of headache in patients with chronic migraine, but real-world data are limited.
Design/methods
A prospective, observational, post-authorization study in adult patients with chronic migraine treated with onabotulinumtoxinA. Data were collected at the first study injection and approximately every three months for ≤52 weeks for utilization and ≤64 weeks for safety data, and summarized using descriptive statistics.
Results
Eighty-five physicians (81% neurologists) at 58 practices in the United Kingdom, Germany, Spain, and Sweden participated and recruited 1160 patients (84.2% female, median age 46.6 years). At baseline, 85.8% of patients had physician diagnoses of chronic migraine/transformed migraine and reported an average of 11.3 (SD = 6.9) severe headache days per 28 days; 50.6% had previously used onabotulinumtoxinA for chronic migraine. A total of 4017 study treatments were observed. The median number of injection sites (n = 31) and total dose (155 U) were consistent across all treatment sessions, with a median 13.7 weeks observed between sessions. At least one treatment-related adverse event was reported by 291 patients (25.1%); the most frequently reported treatment-related adverse event was neck pain (4.4%). Most patients (74.4%) were satisfied/extremely satisfied with onabotulinumtoxinA treatment.
Conclusions
Patient demographics/characteristics are consistent with published data on the chronic migraine population. Utilization of onabotulinumtoxinA treatment for chronic migraine appears to be consistent with the Summary of Product Characteristics and published PREEMPT injection paradigm. No new safety signals were identified.
Introduction
The pharmacologic management of chronic migraine, defined as headache occurring on at least 15 days per month for >3 months in which headache with features of migraine occur on ≥8 days per month (1), includes acute treatment of headaches as well as preventive therapies to reduce the frequency of headaches and related migraine disability (2). Chronic migraine has been estimated to affect approximately 1.4% to 2.2% of the population globally (3), with rates of 0.4% to 2.0% reported for German populations depending on how strictly the criteria for chronic migraine were applied (4). As chronic migraine is often associated with substantial disability, functional impairment, and decreased quality of life (5,6), and in many cases may be associated with medication overuse (7), it is important that any treatment is both effective and well tolerated.
The efficacy and safety of onabotulinumtoxinA has been demonstrated in the Phase III Research Evaluating Migraine Prophylaxis Therapy (PREEMPT) trials (8,9). In a pooled analysis of four double-blind placebo-controlled trials, onabotulinumtoxinA was safe and well tolerated, with 3.4% of patients discontinuing treatment with onabotulinumtoxinA due to an adverse event (10). Serious adverse events occurred in 5.4% of patients receiving onabotulinumtoxinA and 3.0% of those receiving placebo. Consistent with the known tolerability profile of onabotulinumtoxinA, the most frequently reported adverse events in the pooled analysis were musculoskeletal in origin and were comparable to the known adverse events associated with onabotulinumtoxinA when used in other indications.
OnabotulinumtoxinA is approved for the prophylaxis of headache in adults with chronic migraine (10,11). There are limited data on the utilization and safety of onabotulinumtoxinA for chronic migraine in a clinical setting. Therefore, the goal of this study was to monitor the utilization practices and describe the safety profile of onabotulinumtoxinA for chronic migraine headache prophylaxis in routine clinical practice settings in Europe as part of post-authorization regulatory commitments.
Methods
Study design/physician recruitment
This was a prospective, observational, multinational European study (NCT01432379). The study protocol was reviewed and approved by the relevant ethics committees in each country. Physicians were recruited for the study in the United Kingdom, Germany, Sweden, and Spain, primarily through attendance at training sessions on the administration of onabotulinumtoxinA for the management of chronic migraine educational meetings.
Patient recruitment was targeted to begin 12 months after regulatory approval in each country, with the first recruitment in the United Kingdom on September 9, 2011. The recruitment period was 27 months in the United Kingdom, 16 months in Germany, and 14 months in Spain and Sweden. Patients were followed up for up to 64 weeks after the baseline treatment, with the last follow-up visit scheduled for approximately 12 weeks after the final study treatment session at 48 to 52 weeks. The total duration of the study from the first patient enrollment through to the final follow-up visit for the last patient was 43 months in the United Kingdom, 31 months in Germany, 27 months in Sweden, and 28 months in Spain. The last patient’s final follow-up visit was conducted in Spain on April 18, 2015.
Study population
The study population consisted of patients receiving onabotulinumtoxinA therapy for chronic migraine, recruited by their participating physicians. Patients were adults aged 18 years and older with a new or established physician diagnosis of chronic migraine. All patients were being treated for chronic migraine headache in routine practice, and could have been new to treatment with onabotulinumtoxinA for chronic migraine (treatment naïve) or could have been previously treated with onabotulinumtoxinA (non-naïve). The decision to initiate or continue treatment was independent of the patients’ enrollment in the study. Written informed consent was provided by all participating patients.
OnabotulinumtoxinA exposure
Patients were administered onabotulinumtoxinA in routine clinical practice for the treatment of chronic migraine. Although participating physicians were provided with the Summary of Product Characteristics, the study protocol did not mandate the treatment paradigm or frequency of administration as outlined in the Summary of Product Characteristics. The intent of the study was to observe treatment utilization and safety in real-world clinical practice with no study intervention.
According to the Summary of Product Characteristics, the recommended dose of onabotulinumtoxinA is 155 U, up to a maximum dose of 195 U, administered intramuscularly using a 30-gauge, 0.5 in needle as 0.1 mL (5 U) injections into 31 to 39 sites, every 12 weeks (12). The injections are recommended to be divided across seven specific head and neck muscle areas (i.e. frontalis, corrugator, procerus, occipitalis, temporalis, trapezius, and cervical paraspinal muscle group) and are recommended to be injected bilaterally with the exception of the procerus, which requires one midline injection. In the case of predominant pain location(s), additional injections can be administered in up to three specific muscle areas (i.e. occipitalis, temporalis, and trapezius) (12).
Data sources and measurement
Practice and physician characteristics were collected at baseline via a questionnaire that captured details including practice type and characteristics, physician experience, and number of patients seen. Patient demographics and clinical characteristics were also collected at baseline. Medical and migraine-related history at baseline was captured from the patient’s medical record. Treatment utilization information was collected at every treatment session for up to 52 weeks and included details on onabotulinumtoxinA dose, number and location of injections, and needle size. Detailed information on any adverse events and specific adverse events of special interest, including worsening of migraine and intractable migraine, reported by patients and occurring during or between treatment sessions, was collected throughout the study period. Information pertaining to dysphagia was also collected. A final follow-up visit was conducted approximately 12 weeks after the final treatment session and collected data on adverse events that occurred after the final treatment session in addition to patient reported overall satisfaction with onabotulinumtoxinA treatment, measured by a single question using a five-point scale from extremely satisfied to extremely dissatisfied.
Study size
This study was not designed for hypothesis testing; therefore, no formal power calculations were performed. The number of patients was chosen based on a practical basis in conjunction with the ability to detect rates of adverse events similar to those in phase 3 trials undertaken previously. With agreement from the Medicines and Health Product regulatory agents in the United Kingdom and the Irish Medicines Board, the final overall study enrollment was targeted at 900 patients, which targeted 320–350 in the United Kingdom, 250–280 in Germany, 200–210 in Sweden, and 70–125 in Spain.
Statistical analysis
Data were summarized using descriptive statistics and stratified by country and prior onabotulinumtoxinA use. As the analysis was descriptive in nature, statistical inference was not performed. Any missing data were excluded from the analysis. Safety data were summarized using terminology from the Medical Dictionary for Regulatory Activities (MedDRA version 17.1). For each system organ class and preferred term, the number and percentage of patients who experienced adverse events were tabulated. Patients experiencing more than one adverse event were counted only once at each MedDRA level. Incidence rates of adverse events were calculated as the number of new events occurring during the study period divided by the person-time at risk and displayed with 95% exact Poisson confidence intervals.
The analysis population for physicians included the principal investigator at each site and any additional physicians/healthcare professionals administering injections to study patients at that site. The analysis population for patients included all patients enrolled in the study who completed at least one onabotulinumtoxinA treatment session.
Results
Practice site and physician characteristics
A total of 97 physicians completed the site feasibility questionnaire and 85 physicians at 58 sites participated in the study (Figure 1). There were 19 physicians from 16 practice sites in the United Kingdom, 39 physicians from 19 sites in Germany, 14 physicians from 12 sites in Sweden, and 13 physicians from 11 sites in Spain. Among participating sites, 71.4% were specialty-based practices (specialty practice, 32.1%; headache specialty, 26.8%; headache/pain clinic, 12.5%), 50.0% were hospital-based practices or based in hospital outpatient clinics, and 21.4% were general practice or ambulatory care practices (Figure 2). Practice characteristics varied across countries, with specialty practice more common in Sweden, and general practice/ambulatory care settings more common in Germany and Spain (Supplementary Figure 1).
Overview of physician recruitment by country. Baseline practice and physician characteristics.

Approximately 75% of the practices saw ≥ 11 patients with chronic migraine in the three months prior to the study. The majority of the participating physicians were identified as neurologists (81.2%; Figure 2); 75 participating physicians (88.2%) had previous experience treating patients with onabotulinumtoxinA for chronic migraine. The average number of years the physicians were licensed was 18.5 (SD, 9.4) years. The majority of physicians (67, 78.8%) had attended onabotulinumtoxinA training for chronic migraine and 75 (88.2%) had previously prescribed onabotulinumtoxinA for chronic migraine. Considerable inter-country variability was observed from a mean (SD) of 21.4 (22.6) patients treated per physician in Germany to 222.7 (299.0) patients treated in Spain
Patient characteristics
A total of 1168 patients enrolled in the study, and 1160 completed at least one treatment session (the analysis patient population). Of these, 783 (67.5%) patients completed the entire 52-week observation period and final interview (Figure 3). A total of 346 (29.8%) patients were treated for less than the maximum 52-week observation period; of these, 34 patients were lost to follow-up. Of the 312 patients who provided a reason for discontinuing treatment, the most common reason was lack of efficacy (n = 164, 14.1% of the analysis population; Table 1).
Patient enrollment and disposition. Reasons for discontinuing OnabotulinumtoxinA treatment prior to completing 52-week observation period. More than one response was allowed; categories are not mutually exclusive; 312 patients provided ≥ 1 reason why treatment was discontinued and 34 patients were lost to follow-up. “Lack of efficacy” and “Treatment successful/migraines subsided” were categories determined from manual review of the Other category free-text responses, provided by 238 patients. UK: Nine patients reported they were getting or seeking treatment on the National Health Service program; four reported they were no longer eligible for treatment based on the NICE guidelines; three reported a pregnancy; two reported adverse effects; two moved away or transferred to another physician; one reported travel distance was too far; one reported treatment was ineffective; one was deceased; two reported other reasons; Germany: Four patients reported travel distance was too far; three reported a pregnancy; two reported adverse effects; one moved away or transferred to another physician; three reported other reasons; Sweden: Two patients moved away or transferred to another physician; one reported adverse effects; one reported a pregnancy; and 11 reported unknown or other reasons; Spain: one patient reported adverse effects; one moved away or transferred to another physician; one was deceased.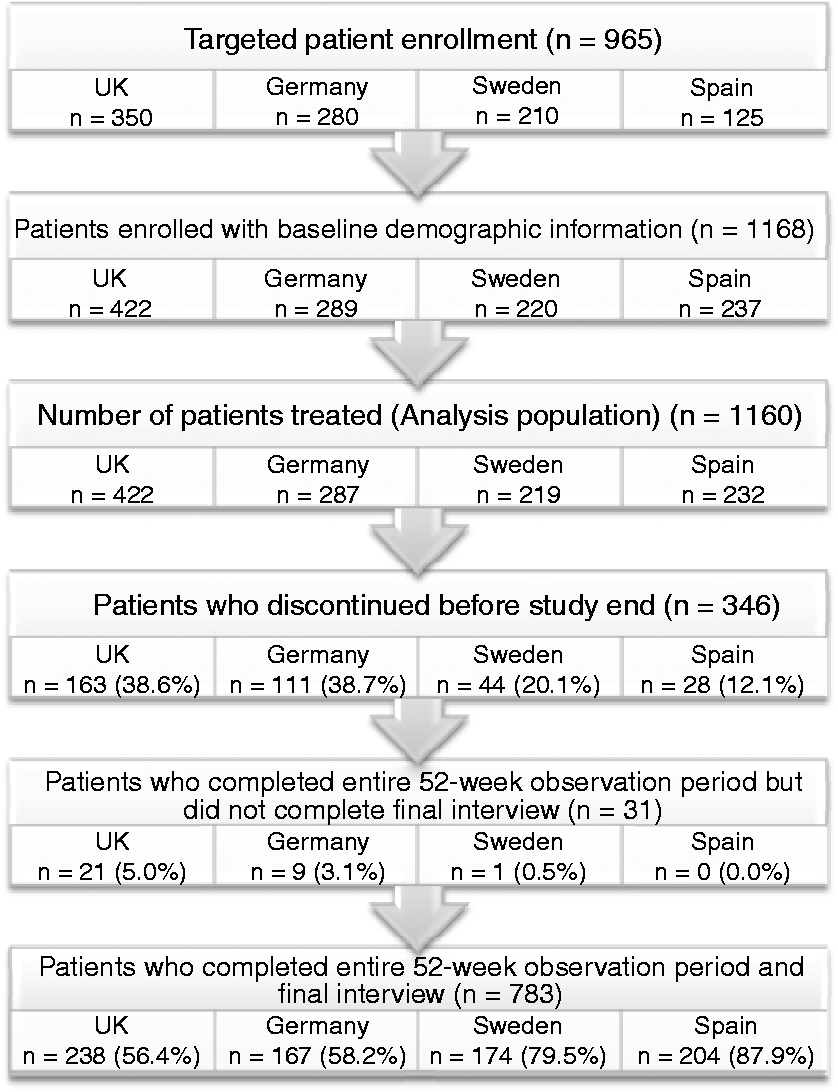

Baseline patient demographics and clinical characteristics of overall analysis population and treatment-naïve patients.

Treatment-naïve patients had not received onabotulinumtoxinA for the treatment of chronic migraine prior to the study.
White is defined differently by country: United Kingdom, white includes English, Welsh, Scottish, Irish, British, Gypsy or Irish Traveler, or any other white background; Germany, white includes white/Caucasian.
Includes all headache diagnoses included in the patient’s medical record; more than one response allowed; categories are not mutually exclusive.
Includes any diagnosis of medication overuse headache, rebound headache, or medication/analgesic overuse.
OnabotulinumtoxinA utilization
OnabotulinumtoxinA treatment utilization characteristics stratified by treatment session.
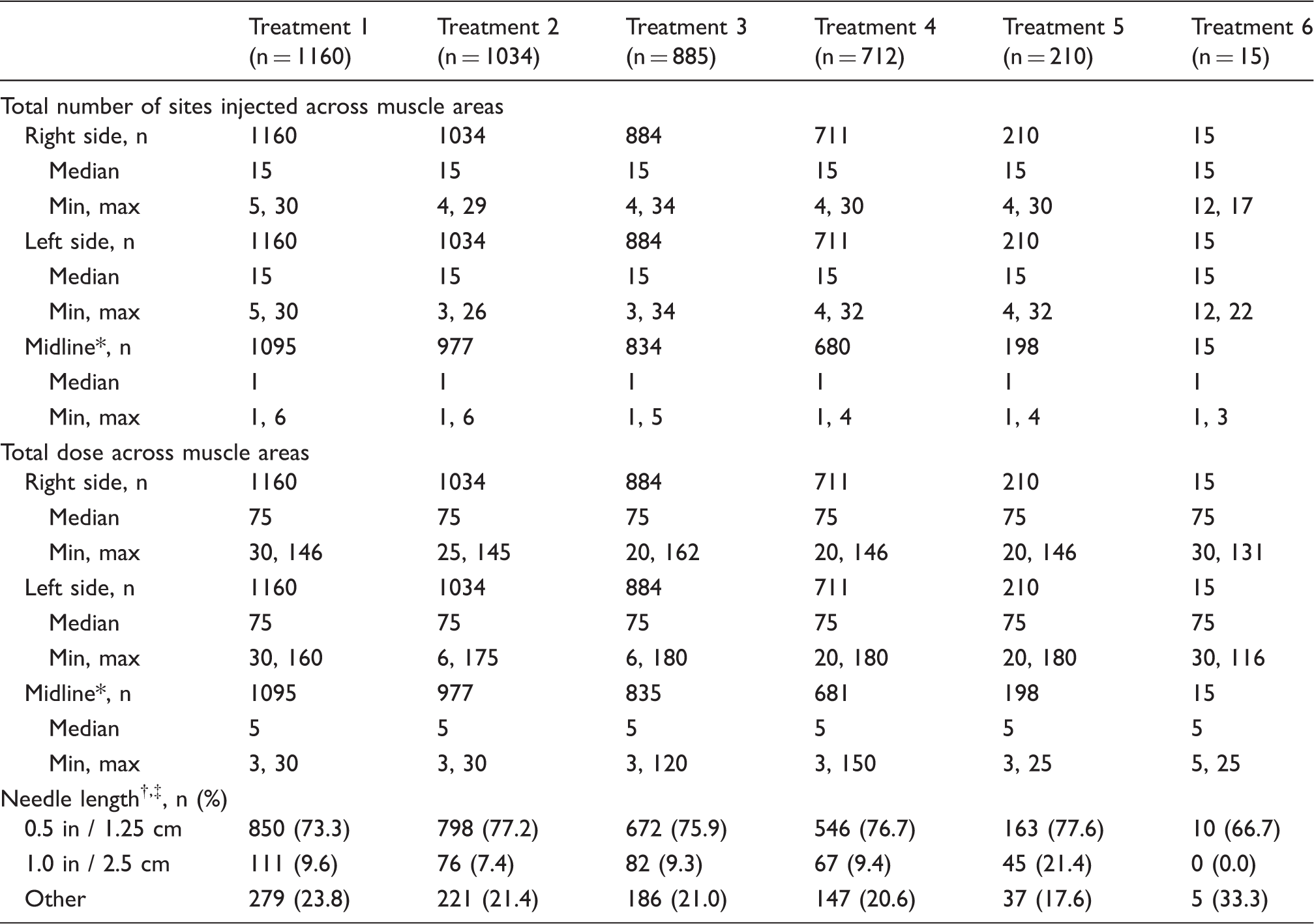
Includes only procerus and “other” midline muscle areas.
More than one response allowed; categories are not mutually exclusive.
Sweden, Germany, and Spain have needles 1.25 cm and 2.5 cm in length; United Kingdom has needle lengths of 0.5 inch and 1 inch.
Muscle areas injected with onabotulinumtoxinA stratified by treatment session.
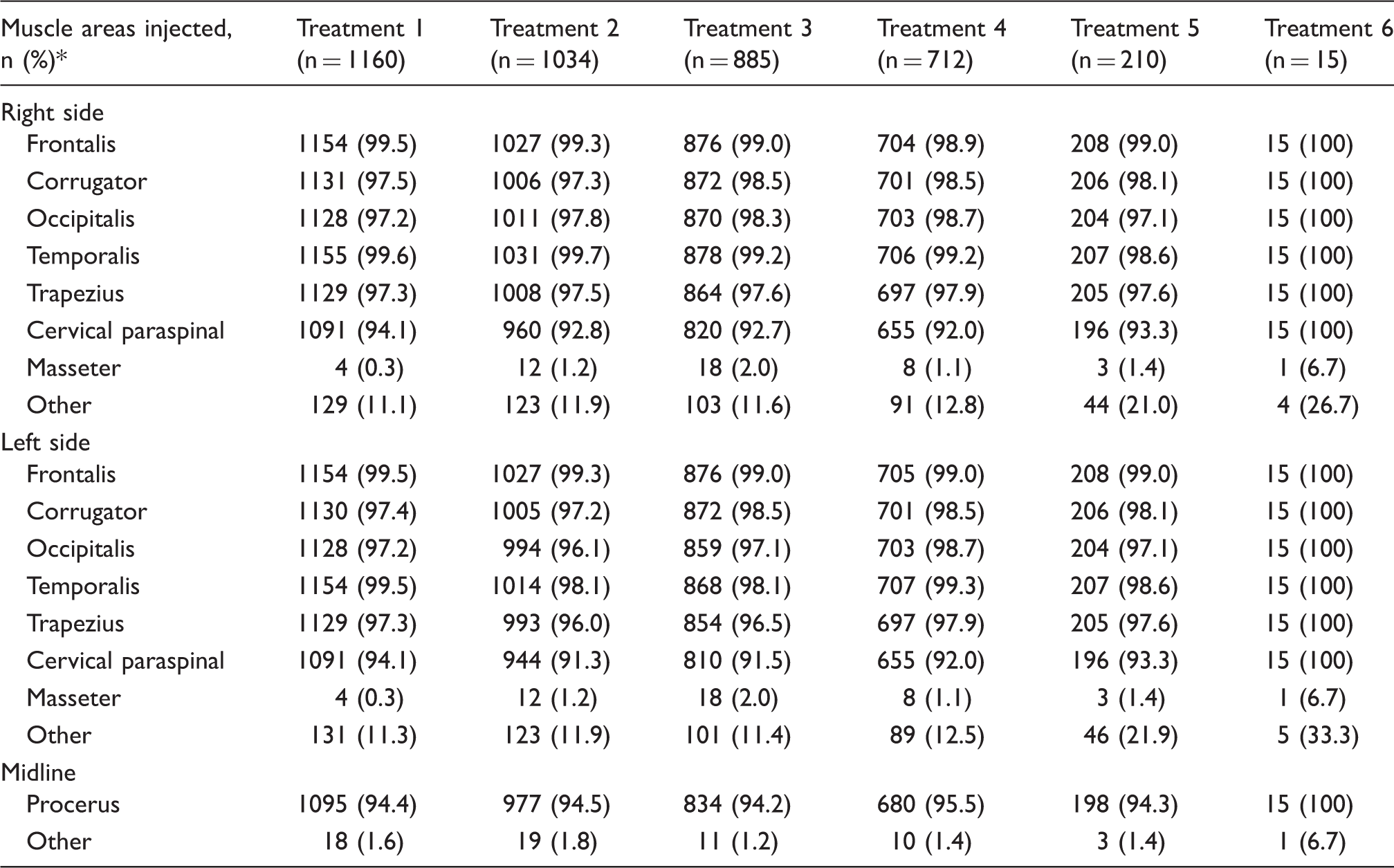
More than one response allowed; categories are not mutually exclusive.

Mean (SD) time between onabotulinumtoxinA treatment sessions. Dotted line indicates recommended treatment interval of 12 weeks between treatment sessions. Descriptive statistics only were undertaken, and there were no intergroup tests of statistical significance performed.
For the purposes of the study, a deviation from the treatment paradigm recommended in the Summary of Product Characteristics was defined as a dose of <155 U or >195 U, injection of <31 or > 39 sites, a dosing interval of <11 or >13 weeks, or use of a needle of length other than 1.25 cm (0.5 in) or 2.5 cm (1 in) for any treatment session; there could be more than one reason for deviation from the recommended label treatment paradigm. If a patient received a treatment with any of these characteristics at any time during the study period, the patient was classified as “deviated” regardless of other treatment sessions.
Overall, 1045 (90.1%) patients in the study were observed to have ≥ 1 treatment deviation. Patients in the United Kingdom were least likely to receive treatment that deviated from the recommended label treatment paradigm (80.1%) and those in Spain were most likely to do so (99.1%; Supplementary Table 3). The majority of the deviations documented were deviations from the recommended dosage schedule, with 844 (72.8%) patients receiving treatment at an interval greater than 13 weeks. In review of treatment deviations during the study, where ≥1 deviation was reported over the course of up to six treatment sessions, nearly half of the patients (n = 480, 41.4%) were administered a dose < 155 U during at least one treatment session. A total of 54 (4.7%) patients received a dose > 195 U during at least one treatment session; however, 626 (54.0%) patients did not have any dose deviations at any treatment session (i.e. received between 155 U and 195 U). A third of the patients (n = 362, 31.2%) received onabotulinumtoxinA into < 31 sites during at least one treatment session, and a quarter (n = 299, 25.8%) were injected with a needle length outside of recommendations.
Adverse events
Summary of adverse events and treatment-related adverse events.

Treatment-naïve patients have not previously received onabotulinumtoxinA for the treatment of chronic migraine.
For the adverse events of special interest, worsening of migraine occurred most frequently (101 of 1160 patients, 8.7%) and was considered serious in six (0.5%) patients. The highest percentage of patients reporting ≥ 1 worsening of migraine event was observed in Spain (12.5%) and the lowest in Sweden (5.5%). Intractable migraine occurred in 20 (1.7%) patients, and was considered serious in three (0.3%) patients. Hypersensitivity reactions, none of which were serious, occurred in 17 (1.5%) patients and dysphagia in five (0.4%). The most commonly reported treatment-related adverse event of special interest was worsening of migraine (n = 46, 4.0%). All other treatment-related adverse events of special interest were reported in < 1% of the study population (Table 5).
Treatment-related adverse events reported by ≥1% of the treatment-naïve or overall analysis population.

Treatment-naïve patients have not previously received onabotulinumtoxinA for the treatment of chronic migraine.
Patient satisfaction with treatment
Overall, 1090 patients responded to the treatment satisfaction question during the final interview (n = 783 for those completing 52 weeks of treatment and n = 307 for those treated for less than 52 weeks). The majority of patients (74.4%) expressed satisfaction (extremely satisfied/satisfied) with onabotulinumtoxinA treatment for chronic migraine (Figure 5a). Patient-reported satisfaction differed by country; the proportion of patients extremely satisfied/satisfied was lowest in Germany (61.3%) and highest in Spain (86.0%). Patient-reported satisfaction differed according to whether patients completed the entire 52-week observation period (90.1% [705/783] extremely satisfied/satisfied) or were treated for less than 52 weeks (34.5% [106/307] extremely satisfied/satisfied) (Figure 5a). Satisfaction among patients who had previously received onabotulinumtoxinA treatment was higher than the satisfaction observed with treatment-naïve patients (Figure 5b). Among those who were treatment-naïve, 338 of 519 (65.1%) were extremely satisfied/satisfied with treatment. The proportion of patients reporting satisfaction with treatment was lower among treatment-naïve patients who were treated for less than the 52-week study period (46/183, 25.1%) than among those who were treated for the full 52 weeks (292/336, 86.9%).
Patient-reported satisfaction with onabotulinumtoxinA treatment for chronic migraine: (a) Overall population stratified by study disposition; (b) stratified by onabotulinumtoxinA treatment history (n = 1070). Data on prior use of onabotulinumtoxinA for chronic migraine were available for 1136 patients out of the 1160 patients in the analysis population.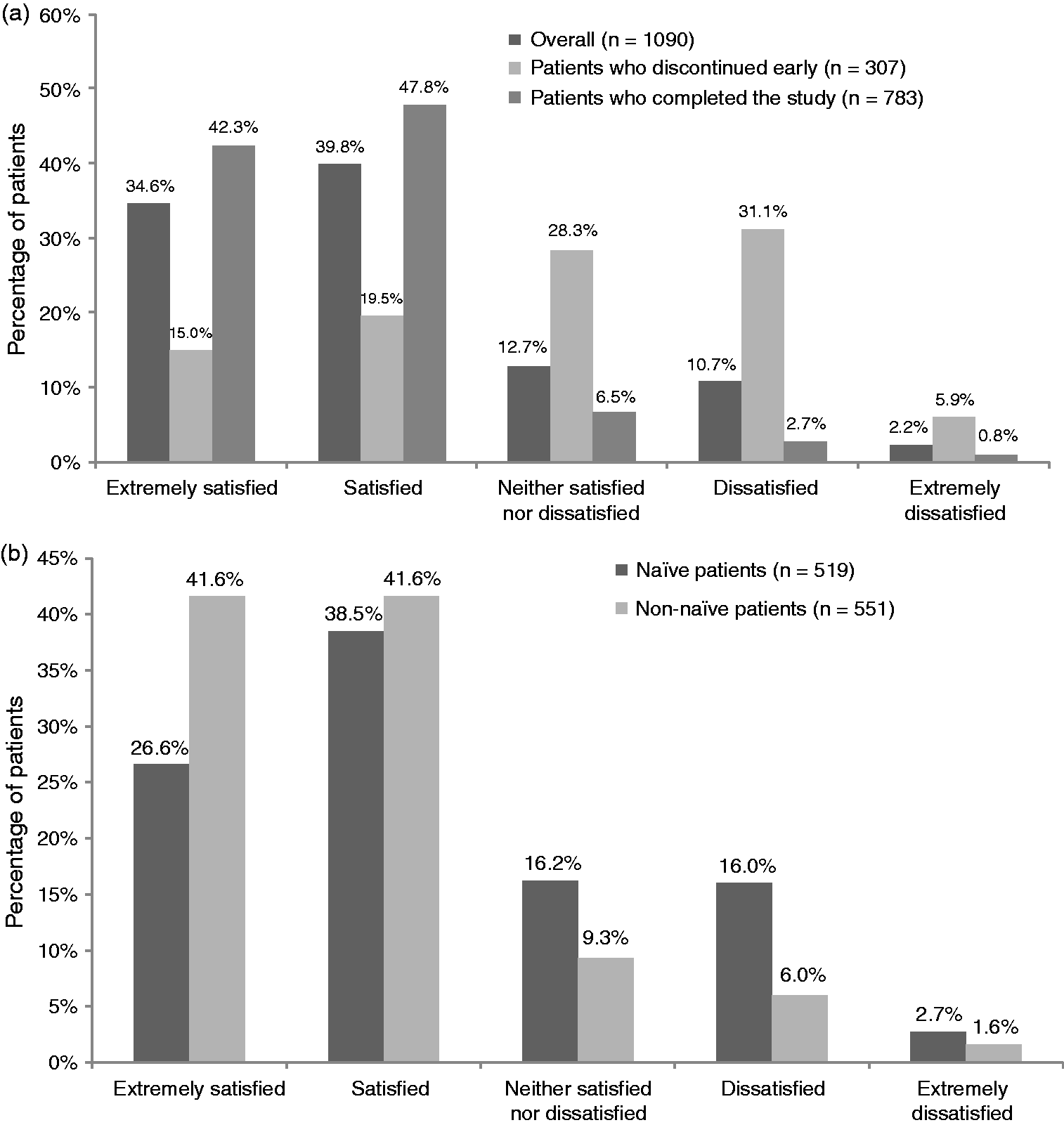
Discussion
The safety and efficacy of onabotulinumtoxinA has been established in controlled trials (8,9); however, real-world data in an actual clinical setting are limited. This study examined the utilization patterns and safety of onabotulinumtoxinA in a routine clinical setting. As such, efficacy and effectiveness were not specifically examined. Consistent with other published studies of chronic migraine, the majority of patients in the study had a diagnosis of chronic migraine at their baseline visit (6,10,13–16). Although other diagnoses were also recorded, it is likely that migraine and chronic migraine diagnoses overlapped, in addition to tension-type headache and medication overuse headache. Overall, patient demographics and clinical characteristics align with typical chronic migraine characteristics; therefore, this study was successful in enrolling and observing chronic migraine patients in a real-world setting.
The doses and muscle areas injected were generally consistent across treatment sessions and with the Summary of Product Characteristics and PREEMPT injection guidelines (12,17). Approximately half of the patients received the recommended 155 U to 195 U dose during all their treatment sessions. Of those treatments that deviated from the recommended paradigm, the majority (72.8%) deviated due to longer treatment intervals (i.e. > 13 weeks between treatments). Although approximately 41% of patients received doses < 155 U, this may be an artifact of packaging restrictions for onabotulinumtoxinA (availability of 50 U, 100 U, or 200 U vials only). Indeed 205 patients (17.7%) received exactly 150 U of onabotulinumtoxinA in ≥1 treatment session. As this was an observational study of routine clinical practice in which the treatment schedule was not specified and instead depended on physicians’ judgment and patient preferences, variability in treatment intervals is to be expected.
Adverse events were consistent with the product label and with the results from the PREEMPT trials (8,9,12,18). The percentage of patients reporting ≥ 1 adverse event was generally lower than that reported from previous pooled registration studies (41.2% vs 72.9%) (10), but the percentage of patients with ≥ 1 serious adverse event was similar (5.3% vs. 5.4%) (10). A reported adverse event rate in a clinical practice setting lower than that reported in a controlled study environment is in line with the expectation that adverse event reporting would be less stringent in an observational study than in a clinical trial. The observed findings also suggest that patients or physicians could have tended to under-report non-serious adverse events.
Although the overall incidence of adverse events was lower in our observational study, the nature of the most frequently reported adverse events was similar to that reported in clinical trials and included neck pain, muscular weakness, headache, facial paresis and musculoskeletal stiffness.
In general, the adverse event incidence rate decreased with each subsequent treatment session, a finding also reported by Diener et al. in a pooled analysis of PREEMPT trials (10). It is likely that the reduction in adverse events reflects the fact that patients experiencing fewer benefits and experiencing adverse events discontinued treatment sooner than those with higher perceived benefit and greater tolerability. The observation that many patients with adverse events continued treatment with onabotulinumtoxinA suggests that these patients experienced a degree of satisfaction/benefit with treatment that outweighed the reported adverse event.
Adverse events associated with potential distant spread of toxin were also assessed, using a conservative approach where all potential cases were counted. No new or unexpected findings were reported from this assessment.
Although the evaluation of efficacy data was not the objective of this observational study, results of the one question on patient-reported satisfaction obtained during the final follow-up interview revealed an overall high level of patient satisfaction by those patients who completed the entire 52-week observational period and attended the final interview. In a post hoc analysis stratified by prior treatment status, the subgroup of patients who had previously received onabotulinumtoxinA for chronic migraine reported higher satisfaction (83.6% of those using onabotulinumtoxinA in the previous six months were extremely satisfied or satisfied) than the treatment-naïve subgroup of patients (65.1% were extremely satisfied or satisfied). It should be noted that patients in these subgroups had a varying number of treatment cycles; typically, at least two to three treatment cycles repeated every 12 weeks are required to determine responsiveness to onabotulinumtoxinA in patients with chronic migraine (19). Because stratification by prior treatment status was a post hoc analysis, these results should be interpreted with caution. Treatment-naïve patients may provide a more accurate “real-world” indication of satisfaction for people new to treatment with onabotulinumtoxinA.
This study is not without its limitations. The design of this study allowed for the observation of onabotulinumtoxinA utilization in actual clinical practice from a diverse sample of physicians and practices, which may increase the generalizability of the data. However, the majority of the physicians were specialists with prior experience with onabotulinumtoxinA for chronic migraine; therefore, the data may more closely reflect results from specialists who have previously treated patients with onabotulinumtoxinA in the countries studied than clinicians new to using the therapy. In addition, the study population included both patients who were treatment-naïve and those who had previously used onabotulinumtoxinA for chronic migraine. These two groups can have a different safety experience. It has been shown that for many therapeutic products, the rate at which adverse events occur varies with time, with increased risk occurring early after the initiation of therapy (20). As the study was initiated so soon after market authorization approval in each of the participating countries, it was unexpected that > 50% of patients would have previously received onabotulinumtoxinA for chronic migraine. As a result of this unexpected finding, we stratified safety results on prior use of onabotulinumtoxinA in a post hoc analysis. Those who had used onabotulinumtoxinA within the six months before the study also had a lower incidence rate per 1000 person-months of discontinuation of treatment due to an adverse event (2.4, 95% CI, 1.3–4.0) than did the treatment-naïve subgroup (5.2, 95% CI, 3.6–7.4). Again, due to the post hoc nature of this analysis, these results must be interpreted with caution.
Those patients who had experienced positive results and tolerable adverse events after prior treatment with onabotulinumtoxinA would be more likely to be treated than patients who either experienced poor clinical outcomes or intolerable adverse events. Patients who were treatment-naïve therefore arguably provide data that may be more generalizable to new users of onabotulinumtoxinA in a real-world clinical setting. However, a real-world setting would likely include a mix of patients (naïve and non-naïve); hence, to observe utilization in a routine clinical practice, we included a mix of patients in our study. Finally, with regards to safety data, the observed adverse events and incidence rate of adverse events were consistent with the Summary of Product Characteristics and previously published results.
Overall, this study captured utilization and safety data from a large population of chronic migraine patients treated primarily in headache or pain specialty clinics or at hospital based practices across four countries in Europe, providing a comprehensive look at real-world practices of onabotulinumtoxinA for the prophylactic treatment of chronic migraine in these practice settings.
To our knowledge, this is the largest observational study to date examining utilization and safety of onabotulinumtoxinA for chronic migraine in actual clinical practice. Results from this study indicate that real-world utilization of onabotulinumtoxinA for chronic migraine appears to be consistent with the recommendations in the Summary of Product Characteristics and the published PREEMPT injection paradigm. No new safety signals were identified in this study, and the data continue to support the favorable safety profile of onabotulinumtoxinA for chronic migraine headache prophylaxis.
Footnotes
Clinical implications
Results from this study indicate that real-world utilization of onabotulinumtoxinA for chronic migraine appears to be consistent with the recommendations in the Summary of Product Characteristics and the published PREEMPT injection paradigm.
No new safety signals were identified in this study, and the data continue to support the favorable safety and tolerability profile of onabotulinumtoxinA for chronic migraine headache prophylaxis.
The majority of patients reported they were satisfied or extremely satisfied with onabotulinumtoxinA treatment for chronic migraine.
This study was able to capture utilization and safety data from a large population of chronic migraine patients across four countries in Europe, providing a comprehensive look at real-world practices of onabotulinumtoxinA for the prophylactic treatment of chronic migraine.
Acknowledgments
Writing and editorial assistance was provided to the authors by Amy Kuang of Allergan plc, and Lee Hohaia and Dana Franznick of Complete Healthcare Communications (West Chester, PA) and funded by Allergan plc. All authors met the ICMJE authorship criteria. Neither honoraria nor payments were made for authorship.
Principal investigators for the study included, from the United Kingdom: Fayyaz Ahmed, Amir Al-Din, Neil Collighan, Paul Davies, Judith Pearson, Giorgio Lambru, Manjit Matharu, Christian Neumann, Susmita Oomman, Arshad Majid, Gerard Saldanha, Nicholas Silver, Thomas Smith, Jitka Vanderpol, Stuart Weatherby, Adam Zemansky; from Germany: Peter Behrens, Andreas Böger, Alexandra Bucheister, Hans-Christoph Diener, Stefan Evers, Katerina Freitag, Charly Gaul, Astrid Gendolla, Wolfgang Jost, Michaela Krause, Torsten Kraya, Borries Kukowski, Klaus Längler, Uwe Reuter, Karl-Otto Sigel, Peter Storch, Andreas Straube, Susanne Urban; from Sweden: Jan Åke Åkesson, Jaan Albo, Sven-Åke Eckernäs, Dimitri Filippov, Rune Johansson, Mats Karlsson, Håkan Löfving, Bahram Nazem, Johan Nyberg, Ingela Remahl, Joakim Tedroff, Dariuz Trojanowski; and from Spain: Samuel Diaz-Insa, Jose Maria Gomez Arguelles, Manuel Gracia Naya, Angel Guerrero, Pablo Irimia, José Miguel Lainez, Annita García, Antonio Martín Araguz, Agustin Oterino, Julio Pascual, Pilar Sanchez Alonso, Margarita Sanchez del Rio, and Sonia Santos. The authors would also like to thank the patients for their participation in the study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.