
Abstract
Introduction
Although migraine is a common headache complaint in children and adolescents there remains a significant gap in understanding the unique aspects of the disease in these age groups and their evolution with development. The aim of this retrospective cohort study was to identify migraine features that are influenced by age and sex.
Methods
The headache characteristics of 359 paediatric patients with a clinical diagnosis of migraine from a tertiary paediatric headache clinic were assessed. Patients retrospectively reported headache characteristics during a structured intake interview and clinical exam. Headache characteristics, description and associated symptoms were compared between children (age ≤ 12 years) and adolescents (age > 12 years), and between male and female migraineurs.
Results
Several migraine features differed significantly with age and/or sex, including: (i) a marked change from a 1:1 sex ratio in children to a 2:1 predominance of girls in adolescents; (ii) a higher frequency of headache attacks per month in adolescents and female migraineurs; (iii) a higher proportion of adolescents endorsed a ‘throbbing’ pain quality; (iv) a higher proportion of children reporting nausea and vomiting; and (v) a higher proportion of adolescents, particularly female migraineurs, had a diagnosis of a co-morbid anxiety.
Conclusion
The presentation of migraine, both in terms of its headache characteristics and associated symptoms, appear to vary as a function of age and sex. Given that migraine symptoms have a neural basis, it is not surprising that during the key period of neurodevelopment from childhood to adolescence this may impact their presentation.
Introduction
Migraine, along with other primary headache disorders, is one of the most common medical conditions in childhood (1). Despite this high prevalence in the paediatric population there remains some ambiguity as to the unique aspects of migraine in childhood and adolescence (2). It is likely that the differential presentation of migraine in children and adolescents is related, among other factors, to the ongoing development of the nervous system during this critical point in development (3). Thus, while it is proposed that the underlying pathophysiological mechanisms of migraine are the same in both children and adults, their evolution during this developmental period represents a unique opportunity to explore how the central nervous system may mediate the expression of migraine (4).
Several studies have examined age- and sex-related differences in the presentation of migraine and several notable differences have been observed between children and adults or between younger and older children. These include a marked sexual dimorphism in migraine prevalence during adolescence, a shorter duration of headache attacks in younger children, a more frontal location in the spatial distribution of headache in younger children and a higher presentation of nausea and vomiting as associated symptoms in younger migraineurs (5–12).
In this study we examined migraine headache features and associated symptoms in a cohort of paediatric migraine patients (i.e. aged less than 18 years) from a tertiary headache clinic, with the aim of identifying headache features, pain description and associated symptoms that significantly differ in presentation with (i) age, i.e. between children (classified as those aged 12 years and under) and adolescents (classified as those aged older than 12 years) and with (ii) sex, i.e. between males and females.
Patients and methods
A retrospective review was performed for the cohort of paediatric patients (age < 18 years) seen for an initial evaluation at the Multidisciplinary Headache Clinic at Boston Children’s Hospital over a five-year period between January 2011 and 1 May 2016. Approval from the Hospital’s Institutional Review Board was obtained prior to conducting the review.
The cohort sampled consisted of consecutive patients who underwent an evaluation within this time period and received a primary diagnosis of migraine, including migraine with or without aura. Of the 1582 patients seen during this time period, 1223 were excluded based on the following criteria: primary headache diagnosis other than migraine (n = 500); migraine headache with another headache diagnosis (n = 223); significant history of concussion or head trauma (n = 200); incomplete first evaluation (n = 159); diagnosis other than migraine with or without aura (n = 63); patient was unable to provide description of migraine quality (n = 27); other pain disorder (n = 22); evaluation for diagnosis other than headache (n = 11); second initial evaluation (n = 8); not presenting with headaches or headaches resolved (n = 6); and no diagnosis given (n = 4). Therefore, from the total cohort sampled, 359 paediatric migraine patients were included in the analysis.
During the initial evaluation, migraine patients were evaluated by both a staff psychologist and neurologist. Migraine patients were interviewed both with and without the accompaniment of their parent(s)/guardian(s), and parent(s)/guardian(s) were also interviewed separately. Patients were asked to retrospectively recall their migraine history and features during a structured clinical interview conducted and collated by a psychologist. Migraine features measured during this evaluation and assessed in the analysis include:
Basic demographics, including: age, sex and family history of migraine (including first-, second- and third-degree relatives); Headache characteristics, including: aura (with, without and with/without); frequency of headache attacks per month; classification as episodic (<15 headache days per month) or chronic (≥15 headache days per month) migraine; headache duration in hours and headache laterality (either unilateral or bilateral pain); Headache descriptors. Migraine patients were asked to provide a freeform, verbal description of their headache pain. This response was coded into individual sensory and affective descriptors (words); Associated symptoms. Specific accompanying symptoms that are included in the International Classification of Headache Disorders (ICHD-3 beta), i.e. photophobia, phonophobia, nausea and vomiting, were assessed as either present or absent during a migraine attack; Co-morbid internalising disorders (anxiety and depression). Previous diagnoses of any disorders (including those they are currently receiving treatment for) were recorded. The Revised Children’s Manifest Anxiety Scale (RCMAS-2) and the Children’s Depression Inventory (CDI-2) were administered as screening tools and, where appropriate after a clinical interview, a multiaxial diagnosis of a mental disorder may be made based on the Fourth Edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV).
Statistical analysis included all migraine patients, classified according to their age and sex. Patients aged 12 years and younger were classified as children while those aged above 12 years were classified as adolescents. The numbers of patients with missing data on an individual variable are given in Supplementary Table S1 and were otherwise excluded from the analysis. Summary measures for continuous variables are presented as means and standard deviations and for categorical variables are presented as percentages Dependent variables of interest were compared using a univariate general linear model, with age group (child versus adolescent) and sex (male versus female) entered as fixed factors. Both the main effects of age and gender, as well as an interaction term (age group × gender) was modelled. Where appropriate, post hoc comparisons were conducted with Fisher’s least square differences (LSD). All differences were considered to be statistically significant at a 5% probability level and all reported P values are two-sided. Analysis was performed within the SPSS statistical software package (IBM SPSS Statistics v23.0).
Results
Demographic characteristics of the sample of migraine patients, subdivided by age and gender.

n.a.: not applicable.
Among the total sample of migraine patients there was a moderate female predominance in the sex ratio (1.4:1). When children and adolescents were compared there was a significantly higher proportion of female migraineurs in the adolescent group, such that the sex ratio in children was equal, in contrast to a female predominance in adolescents (children: 1:1 versus adolescents: 2:1, P = 0.002).
Among the total sample of migraine patients the vast majority reported a family history of migraine (87.1%). When children and adolescents were compared there was no significant effect of age group (P = 0.606). When boys and girls were compared there was no significant effect of sex (P = 0.770); nor was there a significant interaction effect (P = 0.219).
Headache characteristics
Headache characteristics of the sample of migraine patients, subdivided by age and gender.

Episodic migraine classified as <15 headache days per month.
Among the total sample of migraine patients the mean frequency of headaches was 11.9 ± 10.4 attacks per month. When children and adolescents were compared there was a significant effect of age group (P = 0.007), such that adolescents reported a significantly higher frequency of headaches (children: 9.8 ± 9.2 versus adolescents: 13.8 ± 11.1). Furthermore, when boys and girls were compared there was a significant effect of sex (P < 0.001), such that female migraineurs reported a significantly higher frequency of headaches (boys: 9.0 ± 8.7 versus girls: 14.0 ± 11.0). However no significant interaction effect was observed (P = 0.205).
Among the total sample of migraine patients the majority (65.2%) were classified as episodic (<15 migraine days per month). When children and adolescents were compared there was a significant effect of age group (P = 0.009), such that a higher proportion of adolescents were classified as chronic (children: 26.1% versus adolescents: 43.1%). Furthermore, when boys and girls were compared there was a significant effect of sex (P = 0.001), such that a higher proportion of female migraineurs were classified as chronic (boys: 24.8% versus girls: 43.1%). However no significant interaction effect was observed (P = 0.808).
Among the total sample of migraine patients that reported a discrete headache duration the majority (67.9%) reported a duration of less than 4 h. When children and adolescents were compared there was no significant effect of age group (P = 0.127). When boys and girls were compared, there was no significant effect of sex (P = 0.640); nor was there a significant interaction effect (P = 0.384).
Among the total sample of migraine patients the vast majority of patients reported bilateral headache pain (80.1%). When children and adolescents were compared, there was no significant effect of age group (P = 0.366). When boys and girls were compared, there was no significant effect of sex (P = 0.907); nor was there a significant interaction effect (P = 0.630).
Headache description
For the total sample of migraine patients the ten most commonly given descriptors of their headache pain were throbbing (43.2%), pounding (41.5%), sharp (13.4%), aching (12.3%), pressure (10.3%), uncomfortable (7.8%), stabbing (7.8%), miserable (7.0%), sickening (6.4%) and squeezing (6.4%). The full list of descriptors is given in Supplementary Table S2.
When children and adolescents were compared in their use of these descriptors, throbbing (children: 30.8% versus adolescents: 54.0%; P < 0.001), sharp (children: 7.6% versus adolescents: 18.2%; P = 0.003) and pressure (children: 6.4% versus adolescents: 13.4%; P = 0.028) were more frequently endorsed by adolescent migraineurs, as shown in Figure 1. When boys and girls were compared, there was no significant effect of sex in the use of these descriptors (all P values >0.05); nor was there a significant interaction effect (all P values >0.05).
The five highest endorsed headache descriptors for the patient sample as a whole and subdivided by age (≤12 vs. >12 years). Descriptors that differed significantly (P < 0.05) between the two age groups were ‘throbbing’, ‘sharp’ and ‘pressure’.
Associated symptoms
Associated symptoms as reported by migraine patients, subdivided by age and gender.

Values given for positive reporting of these symptoms.
For the total sample of migraine patients the second highest reported associated symptom was phonophobia (78.3%). When children and adolescents were compared, there was no significant effect of age group (P = 0.179). When boys and girls were compared there was no significant effect of sex (P = 0.101). However, there was a significant interaction effect between age and sex (P = 0.003), such that there was no sex discrepancy in childhood (male children: 82.6% versus female children: 76.7%; P = 0.344) compared with a significant female predominance in reported phonophobia in adolescence (adolescent boys: 63.5% versus adolescent girls: 83.9%; P = 0.002).
Specifically concerning the sensory hypersensitivities (i.e. photophobia and phonophobia), while the majority of patients endorsed multiple hypersensitivities (74.1%), a small proportion endorsed only a single modality (16.2%) or none at all (9.7%). When children and adolescents were compared there was no significant effect of age group (P = 0.814). When boys and girls were compared, there was no significant effect of sex (P = 0.471). However, there was a significant interaction effect between age and sex (P = 0.018), such that there was no sex discrepancy in childhood (male children: 77.9% versus female children: 68.6%; P = 0.351) compared with a significant female predominance in multiple hypersensitivities in adolescence (adolescent boys: 63.5% versus adolescent girls: 80.6%; P = 0.037).
For the total sample of migraine patients the third highest reported associated symptom was nausea (75.5%). When children and adolescents were compared, there was a significant effect of age group (P = 0.023), such that a higher percentage of children reported experiencing nausea (children: 81.4% versus adolescents: 70.1%). When boys and girls were compared, there was no significant effect of sex (P = 0.139); nor was there a significant interaction effect (P = 0.603).
For the total sample of migraine patients the least reported associated symptom was vomiting (41.2%). When children and adolescents were compared there was a significant effect of age group (P < 0.001), such that a higher percentage of children reported experiencing vomiting (children: 51.7% versus adolescents: 31.6%). When boys and girls were compared there was a significant effect of sex (P = 0.002), such that a higher percentage of boys reported vomiting (boys: 52.3% versus girls: 33.3%). There was also a significant interaction effect between age and sex (P = 0.037), such that there was no sex discrepancy in adolescents (adolescent boys: 34.9% versus adolescent girls: 29.8%; P = 0.480) compared with a significant male predominance in vomiting in childhood (male children: 65.1% versus female children: 38.4%; P < 0.001).
Co-morbid mood disorders
Associated symptoms as reported by migraine patients, subdivided by age and gender.

Values given for positive diagnosis.
Among the total sample of migraine patients the proportion with co-morbid depression was 13.2%. When children and adolescents were compared there was a significant effect of age group (P = 0.004), such that a higher percentage of adolescents have co-morbid depression (children: 7.0% versus adolescents: 18.9%). When boys and girls were compared there was no significant effect of sex (P = 0.194); nor was there a significant interaction effect (P = 0.194).
Discussion
The transition from childhood to adolescence is a sensitive and critical period for neurodevelopment, particularly in the context of neurological disorders such as migraine. While the sex difference in the age-related incidence of migraine has been highly noted the influence of age and sex on other aspects of migraine has been less well characterised. In this study we observed multiple migraine and headache aspects that significantly differed with age, sex or their interaction, including: aura; headache frequency; classification as chronic migraine; ‘throbbing’ pain quality; photophobia; phonophobia; nausea; vomiting; and co-morbid anxiety and/or depression. This evolution in certain migraine features during the transitional period of childhood to adolescence suggests that developmental aspects of the nervous system may impact on the presentation of migraine (3).
Headache characteristics in paediatric migraine
The ICHD criteria, since its second inception, has recognised that the distinct features of migraine headaches may differ in children and adolescents in comparison to adults. Features of note include bilateral pain, frontal location and attacks of shorter duration (13). This is in accordance with our current findings of predominantly bilateral pain and headache duration of less than 4 h, regardless of age group and/or sex. However, some caveats in our data concerning headache duration must be acknowledged including the high percentage of migraineurs with this variable missing and the accuracy of retrospective recall. Regardless, from these observations it is not clear at what age the more classical presentation of migraine (i.e. unilateral, headache duration >4 h) may emerge.
Concerning the shorter headache duration in paediatric migraine two opposing factors may contribute: an enhancement of factors which actively terminate versus a reduction of factors that prolong headache (14). Sleep is among the most common active terminators of migraine pain and the less consolidated sleep patterns in early life may make sleep both a preferred and effective terminator in children and adolescents, particularly among younger children (15–17). Conversely, the headache phase of a migraine attack may be prolonged by the initiation and maintenance of central sensitisation, a process that uncouples the activity of central trigeminovascular neurons from incoming peripheral pain signals. The initiation of allodynia may take up to 4 h after headache onset, giving rise to a prolonged headache duration (18). While the area of allodynia in paediatric migraine has not been extensively studied in children some evidence suggests that allodynia may be less common in paediatric migraine (19). However, it is important to note that this same study failed to find a relation between allodynia and headache duration.
The concept of less prevalent sensitisation in paediatric migraine is also of interest in the context of the low percentage reporting ‘throbbing’ pain compared with adult migraineurs (20,21) and the age-related increase in its endorsement. Importantly, no sex differences were observed in the proportion endorsing this pain descriptor. The throbbing pain quality characteristic of migraine is thought to derive from sensitisation of peripheral trigeminal neurons (meningeal nociceptors) and their sensitivity to fluctuations in intracranial pressure (22), although there is opposing evidence to this theory (23). Interestingly, previous work has shown that the endorsement of ‘throbbing’ pain increased between initial and long-term follow-up evaluation in paediatric migraineurs (24). Furthermore, Hershey et al. (8) have previously noted that pain quality forms the least specific feature (compared to location, severity and activity impact) in the diagnosis of paediatric migraine. From the animal literature there is demonstration of an age-dependent resilience to injury-induced sensitisation (25–27), although this has not been modelled in a manner directly relevant to migraine. Although speculative it may be that a developmentally conferred resilience to peripheral and/or central sensitisation underscores some of the key differences in the headache presentation in paediatric migraine (i.e. shorter duration of headache, reduced ‘throbbing’ pain quality).
Associated symptoms in paediatric migraine
While a diverse range of associated symptoms have been reported in migraine the current classification (ICHD-2/3beta) lists only two subsets: nausea and/or vomiting; and photophobia and phonophobia. In this cohort of migraineurs the majority (74%) reported multi-modality sensory hypersensitivity, regardless of age or sex. However, a significant interaction of age and sex was observed such that female adolescents more commonly reported multi-modality sensitivity compared with their male peers, primarily driven by an increase in reported phonophobia. In addition, adolescents overall more commonly reported photophobia, but only by a small percentage (7.8%). ‘Phobia’, characterised as avoidance to external stimuli, is often viewed as one of the hallmarks of migraine and its expression in response to multiple sensory inputs (i.e. both light and sound) is one of the main differentiators between migraine and other primary headache disorders such as tension-type. Other associated symptoms consistent with sensory hypersensitivity, such as osmophobia and cutaneous allodynia, are also commonly reported in migraine. However, they are not currently included in the ICHD criteria. While the exact neurobiological basis underlying this hypersensitivity in migraine remains to be elucidated converging evidence from has implicated several possibly synergistic pathways including cortical hyperexcitability in primary sensory areas and activation of multi-modal sensory neurons in the thalamus (28). Interestingly, cortical hyperexcitability has been demonstrated in both paediatric (29–31) and adult migraineurs (32–35) leading to the proposition that cortical hyperexcitability and its associated symptoms of sensory hypersensitivity may be a primary biological aspect of migraine. However, we did observe an impact of age and sex, although relatively small. Interestingly, both sex and age-related changes in the prevalence of photophobia and phonophobia have also been observed in adult migraineurs and, as yet, the underlying cause is not known (36).
In contrast to the relative stability of sensory hypersensitivities there was a distinct age and sex interaction in the proportion of migraineurs reporting vomiting and nausea driven by younger boys and, to a lesser degree, children overall. While this age- and sex-related difference has been previously reported (8,37) the physiology underlying the propensity of these specific symptoms in younger migraineurs remains unknown. Interestingly, a similar pattern is observed in motion sickness where the highest susceptibility is among children aged less than 12 years (38). The motor act of vomiting includes complex gastrointestinal, respiratory and postural components, which are coordinated by nuclei of the caudal medulla including the nucleus tractus solitarius, the dorsolateral reticular formation and the parabrachial nucleus. While nausea is a sensation that usually proceeds vomiting and is often triggered by the same inputs the two are not necessarily concordant (as exemplified in this study) and the neural pathways that produce nausea and vomiting are at least partially separate. A variety of experimental approaches have indicated that an ascending pathway from the brain stem through the parabrachial nucleus to the hypothalamus, limbic system and other cortical areas is responsible for the perception nausea and its overt symptoms (i.e. cold sweating, pallor, increased heart rate, etc.) (39–41). With respect to migraine-associated nausea and vomiting the prevailing hypothesis is that these symptoms are driven by dopaminergic dysfunction, more specifically, chronic dopaminergic hypofunction leading to dopamine hypersensitivity (42,43). Furthermore, anatomical evidence has suggested that dopaminergic cell groups A11/A13 in the hypothalamus may play a role in both trigeminovascular pain (migraine headache) and the accompanying nausea (44,45). In accordance with this theory dopamine receptor antagonists are the most commonly prescribed treatment for paediatric migraineurs presenting to emergency departments (46). However, as aforementioned, it remains unclear why dopaminergic/hypothalamic symptoms are more prevalent in younger migraineurs, especially in boys, although this may present a valuable therapeutic target in this specific population.
Co-morbid psychiatric disorders in paediatric migraine
Numerous studies of migraine co-morbidity in adults from both clinic-drawn samples and the general population have established an association between migraine and internalising psychiatric disorders (47). In particular, this association appears to be strongest for anxiety and depression (48). It remains unknown if this association is casual or represents a common aetiology (49), with the latter focusing on common aetiopathological pathways related to psychosocial stress, poor lifestyle habits and avoidance behaviours, as well as a common neurobiological basis. Similarly, in children and adolescents migraine and other headache disorders are closely associated with negative psychological symptoms, especially dysfunctional cognitive-emotional traits (50). While the prevalence of anxiety and depression in our study was in line with previous reports (51) this represents only a slightly increased prevalence compared with estimates from the general population (52). More significant was the observed age and sex interaction in the increase of co-morbid anxiety in female adolescents and the overall small increase in depression in adolescents. It cannot be discounted that this potentially reflects an age- and sex-related referral bias, with older paediatric migraineurs with complex headache presentations and significant co-morbidities being more likely to present to a tertiary specialty clinic (53). Previous studies in a similar, clinic-drawn sample of paediatric chronic have also observed increased impairment (including pain severity, depression and anxiety) with increasing age (54). Interestingly, psychiatric co-morbidities in late adolescence have been associated with a worsening or endurance of headache at eight-year follow-up (55) and in girls, but not boys, anxiety/depression was found to be a significant predictor of headaches over four years (56). Under this view it is possible that the association between psychiatric co-morbidities and the burden caused by migraine may perpetuate both conditions over time, particularly for girls (57).
Limitations and future directions
Although this study offers novel findings, several shortcomings are acknowledged. First, the selection bias inherent in conducting a clinical study based on children attending a specialist clinic must be recognised, and the question remains as to whether these findings are generalisable to the general population of paediatric migraineurs. However, recognising age-related patterns in migraine presentation even within this specific population is of importance for studies that draw primarily from tertiary headache clinics for their patient samples (58–60). As with other studies that cover a wide range of age the description of specific headache and migraineus symptoms, particularly the headache-pain descriptors, may be impacted by innate expressivity, previous exposure to the common vocabulary of migraine (i.e. physician use of the word ‘throbbing’) and age-related maturation of language abilities (61). Even so, the structured nature of the clinical evaluation and its conductance by specialist staff gives credence that any observed difference between age groups is due to a true difference and not limitations in reporting. Finally, the limitations inherit to the retrospective design of the study must be acknowledged; that is, headache characteristics are based on self-report and therefore subject to recall bias or distortion (62) rather than objective data obtained prospectively during (or shortly after) a migraine attack (63).
Conclusion
In this retrospective cohort study of paediatric migraine patients the presentation of migraine, both in terms of its headache characteristics and associated symptoms, varies as a function of age and sex. Given that migraine symptoms have a neurologic basis it is not surprising that during the key period of neurodevelopment from childhood to adolescence this may impact their manifestation. As such, these factors may have important implications in terms of understanding basic migraine mechanisms, the difficulty in developing both sensitive and specific diagnostic criteria for this age group and in determining effective treatment options. With respect to the latter, it is becoming apparent that deriving treatment options for paediatric migraine from those effective in adults may be problematic (64) and further work on characterising the clinical presentation and neurobiological basis of migraine across the lifespan is likely necessary to address such issues.
Clinical implications
Prevalence of photophobia, phonophobia, nausea and vomiting for the sample of paediatric migraine patients: (a) overall; (b) divided by age group (C: children, A: adolescents); (c) divided by sex (F: females, M: males); and (d) divided by both age and sex (C-F: children – female, C-M: children – male, A-F: adolescents – female, A-M: adolescents – male). Some features of migraine vary as a function of age and sex. Age- and sex-related differences are evident in migraine frequency, pain description, associated symptoms and psychiatric co-morbidities.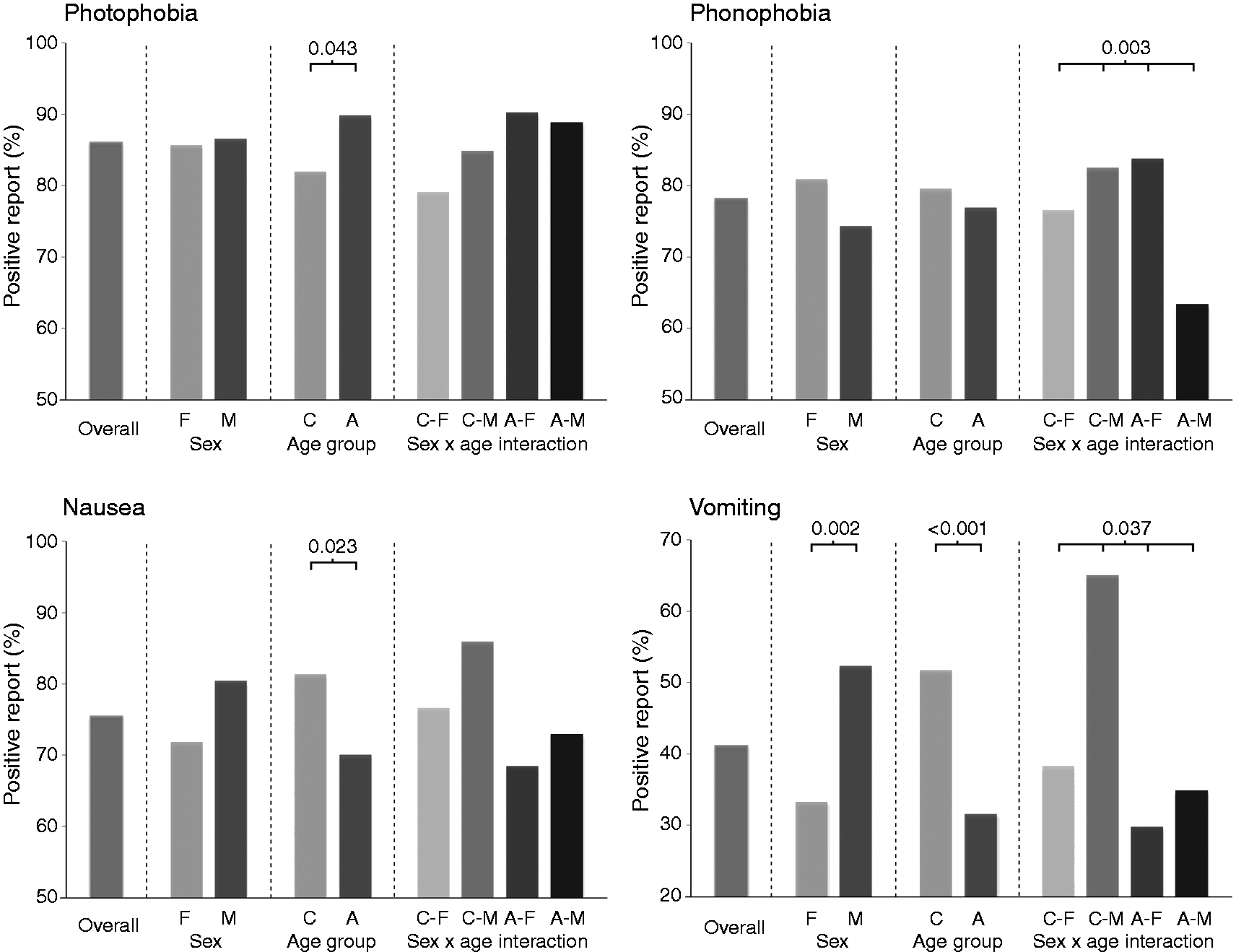
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Neurological Disorders and Stroke at the National Institutes of Health (Grant Numbers: K24NS064050 and R01NS0750182 to DB).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.