
Abstract
Background
Strength training has shown effects in reducing neck pain. As neck pain is highly prevalent in tension-type headache (TTH), it is relevant to examine the effect of strength training of the shoulder muscles on TTH patients.
Aim
To examine the effect of strength training of the shoulder/neck muscles on TTH frequency and duration.
Methods
Sixty patients with TTH were randomised into strength training or a control group. The strength training group trained ten weeks with elastic resistance bands. The control group performed ergonomic and posture correction. Efficacy was evaluated at follow-up after 19–22 weeks.
Results
Twenty-three patients completed strength training and 21 completed ergonomic and posture correction (per-protocol). No between-group effect was detected, but within groups numerical reductions were noted in both groups from baseline to follow-up. Frequency of TTH in the strength training group decreased by 11% (P = 0.041) and duration decreased by10% (P = 0.036), while the ergonomic and posture correction group showed a significant reduction in frequency of 24% (P = 0.0033) and a decrease in duration of 27% (P = 0.041).
Conclusion
No significant difference between the groups was found and the within-group effects did not reach clinical significance. Combining all the elements into a multifaceted intervention could prove more useful and should be further explored in future studies.
Clinical trials registration number
NCT02984826
Introduction
Globally, tension-type headache (TTH) influences the daily lives and the social and economic situation of a large group of people (1–3). The prevalence of TTH is high. For example, in the adult Danish population, Lyngberg et al. found the prevalence of TTH to be 37.2% and 4.8% for frequent episodic TTH (FETTH) and chronic TTH (CTTH), respectively (2). Muscles are considered to play a major role in TTH (4–6). TTH is characterised by increased tenderness in pericranial myofascial tissues (7,8). As increased tenderness with increasing headache frequency and intensity is not displayed by migraine patients, these can be said to be specific to TTH (6).
A positive association between headache and musculoskeletal symptoms has been described in a cross-sectional analysis in the Norwegian Hunt study, and a high association was found between headache and neck pain (9). Similarly, another study comparing prevalence of neck pain in individuals with and without TTH showed that neck pain was more common among those with TTH than in those without (10).
Trigger points that have been located in shoulder and neck muscles in CTTH patients can potentially influence the muscle function of the neck (11–13). The ability to generate force in the neck muscles can be influenced by muscle pain in the neck region (14). Prolonged dysfunction of particular muscles may therefore have an important influence on both the onset and the chronification of TTH. As a part of this present study, we have reported in a case-control study that the extension/flexion ratio reduces as a result of a reduced extension force in TTH compared with healthy controls (15). Given the strong association between neck pain and TTH, it is therefore plausible that an intervention aimed at reducing neck pain by means of strength training (ST) could also improve the condition of TTH patients.
Unspecific neck pain is often classified as trapezius myalgia (16). In a randomised controlled trial (RCT), a ten-week ST programme targeting muscle pain in trapezius myalgia patients effectively reduced neck pain and increased muscle strength (17,18). Based on these effects of ST that targeted shoulder muscles in trapezius myalgia patients, we hypothesised that there would be a similar beneficial effect for TTH and that ST would result in a greater decrease in frequency and duration of headache than ergonomic and posture correction (EP) (19,20) . EP has been used in previous studies as an element in interventions to reduce TTH (19,20).
The aim of this study was to examine how ten weeks of progressive ST of the upper shoulder muscles would affect headache frequency and duration in adult TTH patients compared with EP.
Materials and methods
Participants
The RCT was performed at the Danish Headache Center, Department of Neurology, Rigshospitalet, Glostrup. The RCT was part of a research project examining muscle force and function of the neck and shoulders. The TTH patients were recruited from tertiary and secondary headache referral centres Danish Headache Center, and the headache clinic, Department of Neurology, Bispebjerg Hospital, Copenhagen. Additionally, TTH patients were taken from among volunteers to a Danish webpage for medical trials (21) and from our database at the Danish Headache Center.
Inclusion criteria were:
All interested patients were asked to fill out a four-week headache diary before their first consultation at the hospital. The baseline diaries were checked by the including physiotherapist (BKM). Only patients who completed the diary and whose diary met the ICHD-II criteria for TTH were included. If the diary was inconclusive as regards days with migraine and TTH, the diary data were supplemented with a consultation with a headache specialist and/or a detailed diagnostic telephone interview with the patient.
Exclusion criteria were:
headache caused by medication overuse (ICHD-II); previous whiplash or head trauma; other major physical or neurological diseases, depression, other mental illness; inability to understand and speak Danish.
The patients were tested for cervicogenic headache according to the procedures described by Jull et al. (23) and were excluded if the test was positive.
The participants received written and verbal information about the study; all participants gave informed written consent. The patients were included within a period of two years from 2010 to 2012 (Figure 1). The patients were included after written and oral information by the physiotherapist (BKM).
Flowchart TTH patients for the intervention study. The dropouts in the ST and the EP occurred during the ten-week intervention.
Allocating groups
The TTH patients were randomised by random sequence generator into two groups and were grouped on the first test day by the physiotherapist (BKM).
For ten weeks, the ST group conducted progressive ST with elastic resistance bands (Thera band) (Figure 2), while the EP control group were instructed in ergonomic and posture correction. For both groups, there was a 12-week follow-up period during which they registered headache frequency, duration and intensity. The RCT was single-blinded; the physiotherapist was blinded to the results of the headache diary until the statistical calculation was made. The participants were informed that they would be randomised and placed in an ST or control group (EP) and that after the intervention and follow-up they could choose the other therapy. Neither of the interventions was presented as being better than the other and both were presented as effective.
Strength training exercises.
Strength training
The specific ST group completed a ten-week training programme and filled out a training diary. In the diary, the dates for training and headache intensity were registered. Further intensity was registered before and after training and specifically 2 h after a session. The training consisted of intense ST three times a week. Patients themselves chose which days to train during the week and they were supervised by a physiotherapist once a week for the first two weeks and thereafter once a fortnight. The ST consisted of four shoulder exercises (Figure 2). During the training, the relative loading was progressively increased from 12 repetitions maximum (RM) (70% of maximal intensity) at the beginning to 8 RM (80% of the maximal intensity).
ST was performed with slow, concentric and eccentric muscle contractions with resistance from the elastic bands. Elastic bands (Theraband) with increasing resistance were selected to meet the requirements of the target force. Over time, the combination of elastic resistance and length was individually adjusted to progressively increase resistance from 12 to 8 RM. During each training session in week 1, patients first performed three of the exercises with two sets per exercise and subsequently three sets per exercise, alternating between the four exercises. Shoulder elevation was, however, performed at every exercise session. The elastic bands were returned after the ten weeks of training.
Ergonomics and posture
The control group (EP) was instructed in ergonomic and posture correction. They were instructed to pay attention to their sitting posture and how they used a computer or other working tools. Further, they were asked to do a posture correction exercise three times a day with ten repetitions. The purpose of the exercise was to increase consciousness of sitting posture. The exercise started with the patient in a posture of a flat lumbar lordosis with protruded shoulders and neck. Thereafter, they over-corrected the lumbar lordosis, shoulder and neck, and after 4 s slowly moved back to the start posture. The EP group were seen twice during the ten-week period and received a phone call every two weeks, during which they were asked if they paid attention to their ergonomics and posture correction, and if they filled in the headache diary. After ten weeks, they were instructed that they should stop the exercise but continue to be conscious of their ergonomics and sitting position.
Headache data collection
A headache diary was used to register the frequency, duration and intensity of headache as well as any medication used (24). The duration of the headache was registered in hours for each day with headache. Frequency was calculated and analysed as days with headache per month. The intensity was registered on a 0–10 numeric rating scale (NRS), where 0 is no pain and 10 is worst possible pain. It was calculated as intensity mean/week and a mean value for four weeks was computed. Further, the additional characteristics of the headache were registered and used to diagnose the headache and differentiate between days with TTH and with migraine. The daily registration of headache was done four weeks prior to the intervention (baseline) and during the ten-week training period and again for the 12-week follow-up. The daily registrations were collated after four weeks as days of headache per month and a mean of headache days was calculated for the group. Use of pain medicine was registered as days of medicine intake throughout the entire period. The headache diary was performed over the total of the 26-week study period. The training diary for the ST group included data on headache before and after training, and specifically 2 h after. The training diary was examined on every visit. The first author (BKM) ensured that the headache diary was completed, but was otherwise blinded to the handling and registration of data.
Statistics
Primary outcomes are frequency and duration of pain at (weeks 19–22); secondary outcomes are intensity and medication intake. The results are presented as mean and confidence intervals at baseline and at follow-up (weeks 19–22) adjusted for baseline difference, with two primary outcome parameters that require a Bonferoni correction, and the significance chosen was P < 0.025.
Stata (Stata Corp LP, USA) was used to calculate the statistics. Regression analysis was used to examine any significant difference between groups. For the within-group results, paired t-test was used to test for significant difference. If normal distribution was not confirmed, data were either tested by Wilcoxson signed rank test or submitted to log transformation followed by a paired t-test and presented as mean and standard deviation (SD). Data are presented as analyses of intention to treat (ITT) and per protocol (PP) differences between ST and EP at weeks 19–22. If participants had completed ten weeks of training according to their diaries, they were considered completers and included in the PP analysis.
In the ITT and PP, mean values of the group were used to substitute missing values at 19–22 weeks. The power calculation did not allow an examination of a different response of the ETTH and CTTH, but for exploratory reasons it is presented as a regression analysis with adjustment for baseline difference in ITT and PP. As to the power calculation, since some pharmacological interventions in chronic pain and chronic headache have noted that a pain reduction of 30% is clinically relevant, it was estimated that a clinically relevant change in headache frequency is δ = 30% and that the SD for the frequency was s = 40%. Accepting a risk of 5% for type 1 error and a risk of 20% for type 2 error (Figure 15.2 in D.G. Altman, Practical Statistics for Medical Research) (25), it was estimated that the necessary number of participants in each group was 25. Allowing for dropout, the study allowed for 30 participants in each patient arm, namely the ST intervention group and EP control group. We aimed, therefore, to include 60 TTH patients. Ethical approval for the study was granted by the regional ethical committee of the capital of Denmark: H-3-2009-080.
Results
The 60 TTH patients included at baseline had a mean headache frequency of 18.6 days/month (SD 7.7), with a mean total duration of 219 h/month (SD 142) and a mean intensity of 4.0 (SD 1.3). Of these, 25 had FETTH and 35 had CTTH.
The ITT analysis
Baseline, age and anthropometric measures of included participants.

Mean and 95% confidence intervals are presented.
BMI: body mass index (weight/height2); EP: ergonomic and posture; ST: strength training.
Results after intervention at 19–22 weeks, adjusted for baseline difference.

Mean and 95% (ci) are presented.
Between-group P value.
NRS: numeric rating scale; ST: strength training; EP: ergonomic and posture.
Subgroup: chronic and episodic TTH; results after intervention at 19–22 weeks, adjusted for baseline difference.
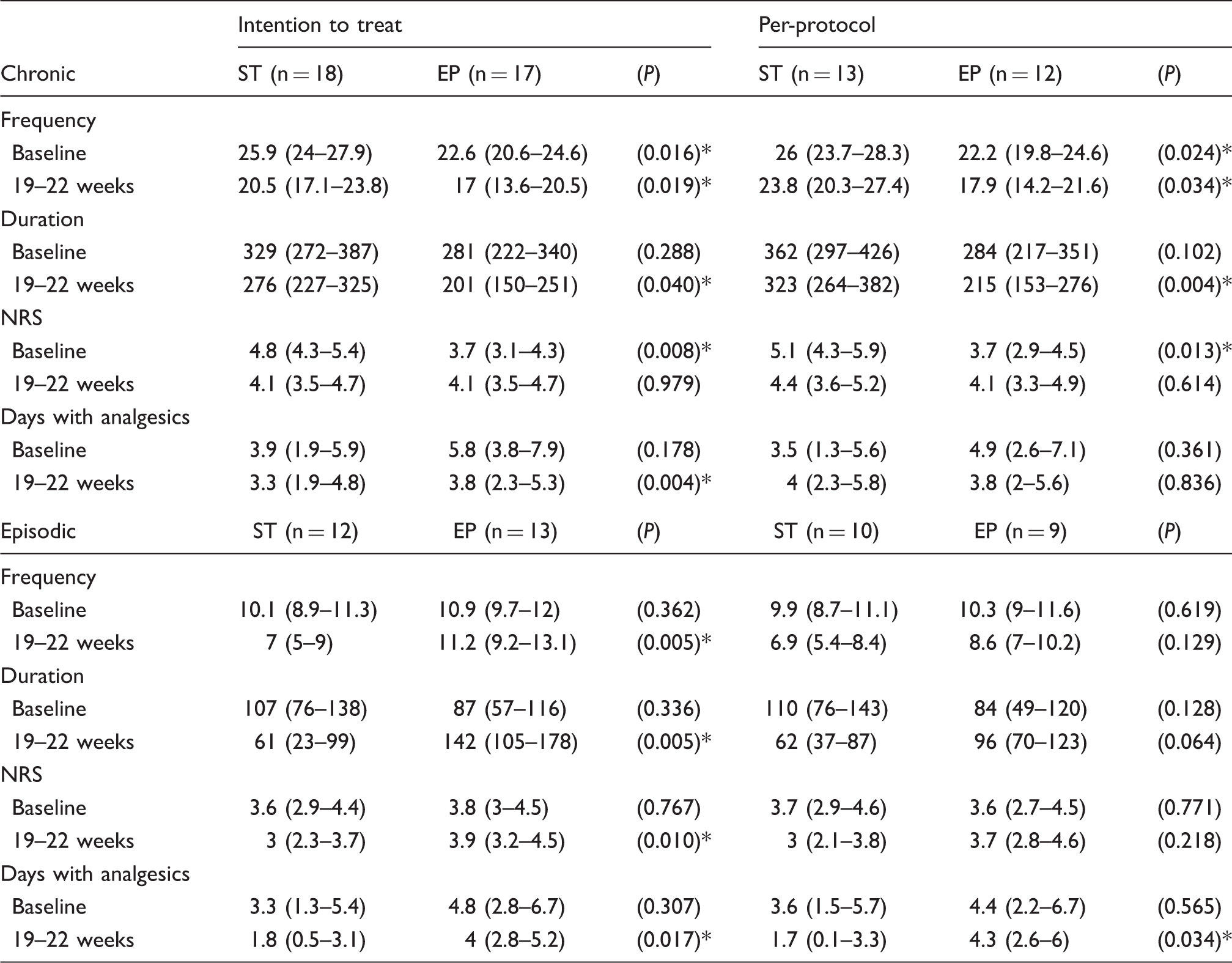
Mean and 95% confidence intervals are presented.
Between-group P value.
NRS: numeric rating scale; ST: strength training; EP: ergonomic and posture.
The per-protocol analysis
Twenty-three patients completed ST and 21 completed EP (Tables 1 and 2). As regards the ST programme, the mean compliance was attendance at 29.8 out of 30 possible sessions.
The 23 ST completers consisted of ten FETTH and 13 CTTH with a mean frequency of 10 day/s month (SD 2) and 26 days/month (SD 3), respectively. The 21 EP completers consisted of nine FETTH and 12 CTTH with a mean frequency of 10 days/month (SD 2) and 22 days/month (SD 5), respectively.
One completer in the ST group and three in the EP group did not complete the 12-week follow-up. Adjusted for baseline difference, no between-group effects were detected at 19–22 weeks between ST and EP, either in primary or secondary outcome (Table 2).
The within-group effect was significant in the EP group frequency but otherwise not significant when adjusted for two primary outcomes. In the ST group at weeks 19–22 follow-up, there was a mean numerical reduction in frequency from 19 days at baseline (SD 9) to 17 days (SD 10) (P = 0.041) as well as a mean reduction in headache duration from 252 h at baseline (SD 153) to 227 h at follow-up (SD 166) (P = 0.036). No significant differences were found in headache intensity (P = 0.231) or use of analgesics (P = 0.158) compared with baseline. In the EP group, there was a mean significant reduction in frequency at 19–22-week follow-up from 17 days at baseline (SD 7) to 13 days (SD 7) (P = 0.003) and a mean numerical reduction in headache duration from 198 h at baseline (SD 138) to 144 h (SD 117) (P = 0.041). No significant difference was found in headache intensity (P = 0.266) or use of analgesics (P = 0.635) at follow-up compared with baseline.
No acute adverse effects of the strength training were recorded for the 23 ST patients. The reported mean pain intensity before the training session was 2.81 (SD 2.32) and at 2.89 (SD 2.26) (P = 0.07) showed no significant change immediately after training or 2 h after training at 2.96 (SD 2.33) (P = 0.16).
Discussion
This study is the first to examine the effect on headache of strength training for the neck/shoulder muscles in carefully diagnosed adult TTH patients.
It was hypothesised that ST of the shoulder muscles would significantly reduce TTH frequency and duration when compared with EP. The hypothesis was not confirmed, as no significant difference was found between groups after 19–22 weeks. When statistically adjusted for two primary outcomes, the only significant difference was the change in frequency within the EP group. At follow-up, numerically, an 11% reduction in frequency and a 10% reduction in duration were found within the ST group, and this was matched by a 24% reduction in frequency and a 27% reduction in duration for the EP group. Unfortunately, the clinically relevant reduction of 30% was not met in any of the groups. Importantly, no adverse effect was recorded in the ST group and there was no aggravation of headache intensity neither immediately after nor 2 h after training.
We hypothesised that a substantially larger effect on the primary outcome could be identified in the ST group, but EP actually produced a numerically larger reduction of headache than ST. Targeting the shoulder muscles through ST was, however, well tolerated.
Posture
In the present RCT study, EP was used as an active control group. Prior to this study, posture correction has been used as part of an intervention that reduced TTH (19). In this RCT study by Van Ettekoven et al. (19), it was used as part of a combined intervention involving physiotherapy and motor control training of the neck, while the control group conducted the same programme but without motor control training.
Fernández-de-las-Peñas et al. reported that CTTH patients had a forward head posture (26). The forward head posture could potentially contribute to a continuous overload of neck muscles and contribute to TTH, and a normalisation of this may reduce the headache. In the present study, EP was chosen as treatment for the active control group. EP does activate and train the neck muscles but with much lower force intensity than the ST. Additionally, EP provides a more functional training specifically targeting the activation of neck muscles in a sitting posture. However, reducing the time with a forward head posture could result in a reduction of muscle load and of muscle tenderness. The reduction in headache was not, however, at a clinically relevant level, and that could suggest that a combined intervention could prove useful.
Strength training
The ST exercises of the neck/shoulder muscles were chosen as an intervention, because previous studies had shown a clinically relevant reduction of neck pain through ST (17). Given the high prevalence of neck pain in TTH patients, we expected a clinically relevant reduction of TTH. The mechanism of exercise training in relieving muscle pain is not yet fully understood. The pain reduction could be related to peripheral factors such as an acceleration of protein synthesis and of degradation or to a general central effect on pain perception, both of which could lead to normalisation of the nociception in the muscle. Further ST could potentially have an effect on trigger points (27,28,29,30). ST could be also expected to increase muscle activation and force generating capacity, thereby lowering the relative workload and reducing TTH. Resistance training has been used to reduce self-diagnosed headache (31,32). With headache as a secondary outcome, Andersen et al. examined the effect of ten weeks of resistance training with either 2 min training per day or 12 min intervention per day (five days per week) or allocation to the control group with weekly health information (31). At baseline, the participants had a mean of 1.3–1.5 headache days per week. After training, their self-diagnosed headache frequency was reduced by 43% and 56%, respectively, in the 2-min and 12-min training groups. This could suggest that even brief daily resistance training can have an influence on low frequency headache. Our exploratory post hoc analysis of FETTH and CTTH also indicates better response of ST for shoulder muscles in FETTH than in CTTH. This could indicate that training of the axio-scapular muscles in the present study is not sufficient to reduce more frequent headaches.
Only a small number of RCT studies have been designed and conducted for TTH patients with low risk of bias and testing non-pharmacological interventions (33).
In a RCT, Castien et al. demonstrated a clinically relevant 50% reduction of frequency in 88% of CTTH patients after eight weeks and in 82% after 26 weeks (20). Their effective intervention consisted of a combination of posture correction, exercises, manual therapy, McKenzie exercises and training of the deep cervical flexor muscles, and the control group received usual treatment through a general practitioner. Castien et al. combined posture correction with the training of neck muscles as part of the intervention (20). Training of the neck muscles could be an important future intervention in both FETTH and CTTH (34). The Bone and Joint Decade Task Force on Neck Pain and its Associated Disorders has evaluated the effectiveness of non-invasive and non-pharmacological interventions for the management of patients with headaches associated with neck pain (TTH, cervicogenic or whiplash-related headaches) through a review of five databases during 1990–2015 (35). From ten studies with a low risk of bias, they concluded that episodic TTH should be managed with low load endurance craniocervical and cervicoscapular exercises. Further CTTH patients could also benefit from low load endurance craniocervical and cervicoscapular exercises, and relaxation training with stress coping strategies or multimodal care with spinal mobilisation, craniocervical exercises and postural correction (35). The results of the present study may indicate that a multi-modal intervention that includes training of the neck muscles could be effective as a TTH intervention with high frequency or chronic TTH.
Strengths and limitations
A strength of this study was the precise diagnosis of the headache and the use of the detailed training diary. Physical training with elastic resistance bands is cheap and easy to use in everyday life, and headaches of the TTH patients did not increase through ST of the shoulder muscles. Likewise, posture training is very easy to apply to everyday life.
A limitation of the present study was the lack of systematic registration of neck pain during the intervention that could have contributed further to the understanding of the correlation between TTH and neck pain. Furthermore, a registration of colour and length of elastic bands throughout the training period could have shown more precisely the progress of resistance in the ST group (36). As part of the trial, neck and shoulder strength were examined, and contrary to expectations, strength was not increased after intervention. The exact effect of ST cannot, therefore, be concluded from the present study. The EP group was asked to do posture correction exercises three times daily, and it is possible that this had an influence on the relative muscle load and TTH. Further, it is possible that consciousness of sitting posture in the EP group after completing the intervention could influence TTH. The effect within both groups could be argued to be the result of a natural development over time. However, considering the long history of high frequency headache in this patient group primarily recruited from a tertiary headache centre, to attribute such an improvement simply to the course of time is rather far-fetched. The effect of placebo could also be considered as a potential influence in both ST and EP, although we tried to avoid attention bias in the present design, giving both groups treatment and attention. It is noteworthy that medication did not increase in any of the groups, indicating that the observed decrease in frequency and duration is not due to change in medication. However, the lack of reduction in acute medication could indicate the limited effect of the exercises.
Conclusion
ST was not significantly better than ergonomic and posture correction in a clinical TTH population. There was a significant reduction of headache frequency in the EP group, and a numerical reduction within both groups from baseline to follow-up, but these did not reach the 30% that was estimated to be clinically relevant. The effect was actually most pronounced in the EP control group. Future RCT studies should evaluate a combined treatment of EP and ST of neck extension and shoulder muscles, as both may potentially be effective as a treatment approach for high frequency or chronic TTH patients.
Article highlights
Strength training was not better at reducing headache than ergonomics and posture correction in a tension-type headache population. Ergonomics and posture correction had a significant 24% reduction in headache frequency, though below 30% clinical relevant reduction. A combined treatment of EP and ST of neck extension and shoulder muscles may be effective in high frequency or chronic TTH patients.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this study was supported by The Tryg Foundation.