
Abstract

Headache Pathophysiology - Imaging and Neurophysiology
PO-01-001
Endothelial dysfunction in migraine
Bojana Žvan1, Jan Kobal1, Marjan Zaletel1,* and Denis Perko1
1University Clinical Centre of Ljubljana, Ljubljana, Slovenia
Objectives
We showed different endothelial functions of the anterior and posterior cerebral circulation in healthy subjects, worse vasodilatatory capacity of the posterior cerebral circulation and unimpaired systemic endothelial function in migraine patients without comorbidities. The relationship between cerebral and systemic endothelial function and the anterior and posterior cerebral endothelial function in migraine patients is still not clear.
Methods
We compared cerebral and systemic endothelial function through post-hoc linear regression analysis of cerebrovascular reactivity (CVR) to L-arginine between the middle cerebral artery (MCA) and flow mediated vasodilatation (FMD) of the right brachial artery and posterior cerebral artery (PCA) and FMD in migraine patients without comorbidities and in healthy subjects.
Results
We did not find any significant correlation between CVR to L-arginine in the MCA and FMD and PCA and FMD in migraine patients with aura (p = 0.880 vs. p = 0.682), without aura (p = 0.153 vs. p = 0.179) and healthy subjects (p = 0.869 vs. p = 0.662). On the other hand we found a significant correlation in CVR to L-arginine between the MCA and PCA in migraine patients with aura (p = 0.004), without aura (p = 0.001) and in healthy subjects (p = 0.002).
Conclusion
Our study suggests that the endothelial function of cerebral and systemic circulation might be different in migraine patients without comorbidities, while that of the anterior and posterior cerebral circulation might be coupled with a worse vasodilatatory capacity in the posterior cerebral circulation, which could indicate endothelial dysfunction in this territory.
Disclosure of Interest
None Declared
Headache Pathophysiology - Imaging and Neurophysiology
PO-01-002
Differential sensitivity to blue or red flash light at 5 or 20 Hz in healthy subjects and migraine patients
Simona Liliana Sava1,*, Alain Maertens de Noordhout2 and Jean Schoenen2
1Neurology, Isosl Valdor
2Neurology, CHR Citadelle - CHU, Liège, Belgium
Objectives
Migraine patients are known to be sensitive to light during an attack, but also interictally. We have previously shown that light stimulation decreases trigeminal pain and could thus have therapeutic potentials. Our purpose was to determine whether flash light sensitivity differs between colours and stimulation frequencies in healthy subjects (HS) and episodic migraine patients (EM) during and between attacks.
Methods
We enrolled a total of 36 subjects: 7 HS, 10 interictal EM and 19 ictal EM. Stimulation intensity was increased by steps of 50 Lux, beginning at 50 Lux, each step lasting 5 seconds. We tested in random chronological order 4 dynamic sequences: blue (∼470 nm) at 5 Hz, blue at 20 Hz, red (∼720 nm) at 5 Hz, red at 20 Hz. The subjects were asked to request interruption of the stimulation as soon as they perceived it as uncomfortable.
Results
Compared to HS, interictal EM patients were significantly more light-sensitive to the 5 Hz blue sequence (p = 0.004) while ictal EM patients were more sensitive to the 5 Hz blue stimulation (p = 0.00002), the 20 Hz blue (p = 0.00005), the 5 Hz red (p = 0.0007) and the 20 Hz red (p = 0.00009).
EM patients reported a greater sensitivity during than outside of an attack for the 20 Hz blue sequence (p = 0.002), as well as for the 5 Hz (p = 0.027) and 20 Hz red (p = 0.00019).
Conclusion
Compared to healthy subjects, migraineurs are more sensitive to blue light and low stimulation rates, suggesting that these parameters may not be suitable for therapeutic purposes and that the melanospin ipRGC pathway is chiefly involved. The study also confirms that patients are more sensitive to light during attacks whatever the light parameters are, except for a lower sensitivity to low frequency red.
Disclosure of Interest
None Declared
Headache Pathophysiology - Imaging and Neurophysiology
PO-01-003
Variation of the spontaneous blink rate (SBR) in light and dark: comparison between migraine patients and healthy subjects
Simona Liliana Sava1,*, Alain Maertens de Noordhout2 and Jean Schoenen2
1Neurology, Isosl Valdor
2Neurology, CHR Citadelle - CHU, Liège, Belgium
Objectives
The spontaneous blink rate (SBR) is strongly modulated by dopamine (Karson et al., 1982) and by the occipital cortex (Karson et al., 1996) both of which also play a role in migraine pathophysiology (Charbit et al., 2010). Photophobia is a phenotypic hallmark of migraine both during and between attacks. We searched therefore whether the SBR could be increased in migraineurs because of their sensitivity to light.
Methods
We enrolled a total of 38 subjects: 7 healthy subjects (HS), 19 interictal episodic migraineurs (EM) and 10 ictal EM without prophylactic treatment. The SBR was measured in a lit room at a luminance intensity of 145 Lux or in almost total darkness, 12 Lux, using 2 electrodes placed on the orbicularis muscle of the right eye.
Results
We found no difference between groups during lightened sessions. By contrast, in the dark the SBR was reduced in HS and in ictal EM, but not in interictal EM (p = 0.05). The percentage SBR change between light and dark was −36.71 ± 22% in HS, −18.7 ± 34.74% in ictal EM and 1.9 ± 43.98% [SD] in interictal EM. This change was significant in HS (p = 0.017).
Conclusion
We show that in migraine patients between attacks the SBR is not decreased in the dark like in healthy subjects or migraineurs during an attack. This could be due to an abnormal interictal control by dopamine and/or the occipital cortex that normalizes during the attack.
Disclosure of Interest
None Declared
Headache Pathophysiology - Imaging and Neurophysiology
PO-01-004
Cerebral endothelial dysfunction in migraine: a study on the age-specific risk of stroke in patients with migraine
Mi Ji Lee1,*, Sook-Young Woo2 and Chin-Sang Chung1
1Department of Neurology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
2Biostatistics Team, Samsung Biomedical Research Institute, Seoul, Korea, Republic Of
Objectives
To reveal the mechanisms underlying the age-specific risk for ischemic stroke in migraine patients, we aimed to evaluate cerebral endothelial dysfunction in migraine patients of different age groups.
Methods
We recruited patients with episodic migraine (EM) and normal controls (NC), aged 20–60 years, between October 2015 and August 2016. Cerebral endothelial function was assessed interictally by measuring cerebrovascular reactivity (CVR) using the transcranial Doppler breath-holding test. Breath-holding index of <0.69 was defined as CVR impairment. To compare CVR between EM patients and NCs, both the age- and sex-matched analysis and stratified analysis by age group were performed. A path analysis was used to test the determinants of CVR.
Image:

Results
In total, 145 EM patients and 72 NCs were included this study. The age- and sex-matched analysis showed a decreased CVR in all basal arteries in EM patients. The stratified analysis showed that the CVR impairment was most prevalent in the youngest age group (age 20–29 years) and in the posterior circulation, particularly posterior cerebral arteries. In EM patients, younger age at onset (p = 0.020) and longer disease duration (p = 0.020) had a negative impact on the CVR in the posterior cerebral artery, while the effect of current age on the CVR was only indirect via cerebral blood flow velocity.
Conclusion
Cerebral endothelial function is impaired in young-age migraineurs and in the posterior circulation, similarly to the characteristics of migraine-related stroke. Age at onset and disease duration, not the current age, may be determinants of cerebral endothelial dysfunction.
Disclosure of Interest
None Declared
Headache Pathophysiology - Imaging and Neurophysiology
PO-01-005
Altered structural & functional connectivity of the ventrolateral PAG in chronic migraine related to migraine frequency
Dinant Riks1,*, Andrew Segerdahl1, Zameel Cader1 and Irene Tracey1
1Nuffield Department of Clinical Neurosciences, University of Oxford, Oxford, United Kingdom
Objectives
The neurophysiological mechanisms underlying migraine are not yet well understood. Accumulating evidence supports that numerous factors are involved including changes in brain structure, function and the neuro-vasculature. Most of the migraine studies to date have focused on episodic migraine. Consequently, little is known about what drives chronic migraine, which is defined as more than 15 headache days/month and is linked to significantly increased disability compared to episodic migraineurs.
The periaqueductal gray (PAG) is a brainstem region that plays a key role in the perception of pain and its dysfunction is linked to different chronic pain states. For example, it is implicated in migraine pathophysiology, and resting state functional magnetic resonance imaging (fMRI) studies have shown migraine-related allodynia is associated altered functional connectivity between the PAG and both cortical and subcortical pain regions.
The aim of this study was to investigate if changes in PAG physiology are related to features of chronic migraine. We assessed this using a multi-modal imaging approach that included: measuring PAG glutamate concentrations with magnetic resonance spectroscopy (MRS) and assessing PAG structural and functional connectivity with DTI and BOLD-resting state FMRI, respectively. For each imaging modality, we investigated group differences (CM versus controls) as well as relationships with patient’s migraine frequency (MF).
Methods
FMRI data was acquired interictally from 12 female chronic migraineurs and 12 female healthy controls using a 3 T Siemens Verio and standard fMRI analysis methods. We investigated changes in PAG: i) resting excitability as measured by magnetic resonance spectroscopy (MRS); ii) white-matter tract integrity with DTI/TBSS; and iii) resting-state functional connectivity with the whole brain. For all imaging modalities both simple and multiple regression analyses was performed to investigate group differences and relationships with MF.
Results
i) MRS: We found no group differences between patients and chronic migraineurs in combined Glutamate/Glutamine concentrations (Glx) in the PAG nor a significant correlation between Glx of the PAG and migraine frequency. Ii) DTI: We also did not find significant changes in white matter structure between CM patients and controls. We found a significant negative correlation between migraine frequency and fractional anisotropy, a measure of white matter integrity, in the right saggital stratum and the left anterior corona radiate. These effects were driven by an increase in radial diffusivity. We also found a positive correlation between the concentration of Glx in the PAG and fractional anisotropy in the right anterior corona radiate (t = 3.74, p = 0.048). We also found a significant positive relationship between migraine frequency and functional connectivity between the ventrolateral PAG and bilateral frontal pole, superior and middle frontal gyri.
Conclusion
Our results demonstrate a relationship between migraine frequency and altered structural connectivity in chronic migraine, showing a decrease in white matter structure in frontal cortical regions. Conversely, we found an increased functional connectivity between the vlPAG and multiple frontal and prefrontal regions. These regions have been implicated in higher order affective and cognitive pain processing. These results support the notion that increasing migraine frequency is related to altered connectivity between cortical regions and the vlPAG.
Disclosure of Interest
None Declared
Headache Pathophysiology - Imaging and Neurophysiology
PO-01-006
Comparison of the brain structure and resting-state functional connectivity between female patients with trigeminal autonomic cephalalgias and female migraineurs
Noboru Imai1,*
1Department of Neurology, Japanese Red Cross Shizuoka Hospital, Shizuoka, Japan
Objectives
To investigate differences in the brain structure and resting-state functional connectivity (RSFC) between female patients with trigeminal autonomic cephalalgias (TACs) and female episodic migraineurs.
Methods
Ten female patients with TACs and 10 sex- and age-matched episodic migraineurs were selected for the study. All patients fulfilled the International Headache Society criteria 3 beta for episodic migraine or TACs. High-resolution structural magnetic resonance imaging (MRI) and resting state functional MRI (RS-fMRI) were performed in both groups.
Results
In comparison with episodic migraineurs, patients with TACs showed significant gray matter decrease in the left angular gyrus, right postcentral gyrus, right angular gyrus, right precentral gyrus, and left precuneus using voxel-based morphometry. Next, these lesions with significantly decreased gray matter were defined as sources (seeds) in RS-fMRI. Seed-to-voxel and region of interest (ROI)-to-ROI analyses revealed that only the left angular gyrus showed significant differences in functional connectivity between patients with TACs and migraineurs. In contrast, functional connectivity of the default mode and salience networks showed significant differences between patients with TACs and migraineurs in additional RS-fMRI analysis.
Conclusion
Our study revealed that female patients with TACs and female migraineurs have partly different brain structure and RSFC. Furthermore, structural alteration is not strongly related with RSFC. Alterations in the brain structure and RSFC in TACs and migraine may be caused by different pathophysiological mechanisms.
Disclosure of Interest
None Declared
Headache Pathophysiology - Imaging and Neurophysiology
PO-01-007
Single trial visual evoked potentials in migraine
Marco Lisicki1,*, Kevin D'Ostilio1, Alain Maertens De Noordhout2,3, Jean Schoenen2,3 and Delphine Magis1,3
1Headache Research Unit
2Neurology, Université de Liège
3Neurology, Centre Hospitalier Universitaire, Liège, Belgium
Objectives
A large number of studies have reported abnormalities of averaged transient or steady-state visual evoked potentials (VEP) in migraine patients between attacks, but some results are contradictory (see review by Ambrosini et al. 2011). Single trial analysis of VEP in one study (Gantenbein et al. 2013) showed that increases in VEP amplitudes in migraine could be explained by increases in local amplitude (rather than phase synchronization), which is more energy demanding. It is not known whether this is associated with morphological changes of the visual cortex. The aim of this study was to analyse single trial visual evoked potentials (st-VEP) in migraine patients and healthy controls and their anatomical correlates determined by voxel-based morphometry.
Methods
Twenty healthy volunteers (mean age 34,8 ± 11,3, 15F/5M) and 19 interictal migraine without aura patients (ICHD3beta 1.1) (age: 32,7 ± 12,9, 15F, 4M) participated in the study. For VEP, 600 epochs were uninterruptedly recorded at Oz (Ref Fz) using a pattern reversal stimulus (3.1 Hz, 68°). Artefacted epochs were rejected (<5%). The mean amplitude of st-VEP was extracted for each subject. On a separate day, patients underwent 3T MRI of the brain. Grey matter volume was then correlated with mean st-VEP amplitude, controlling for whole brain size. Statistical analyses and graphs were performed in Prism GraphPad (GraphPad Software). st-VEP and MRIs were processed in EEGLAB and SPM respectively, both running in MATLAB (The MathWorks Inc.).
Results
Mean st-VEP amplitudes were higher in migraine patients (0,7896 µV ± 0,6611) than in healthy controls (0,2523 µV ± 0,6064) (p = 0.012). There was no difference in grey matter volume between the 2 groups of subjects. SPM statistical mapping showed that in migraine patients, but not in healthy controls, mean st-VEP amplitudes were positively correlated with grey matter volume in the primary visual cortex (small volume correction BA 17: 15, −78, 8, pFWE = 0.007, and −14, −78, 9, pFWE = 0.057) and in the right angular gyrus (whole brain analysis: 42, −57, 29 pFWE = 0.007).
Conclusion
This study confirms that migraine patients between attacks have increased amplitudes of mean single trial visual evoked potentials and shows for the first time that this is correlated with grey matter volume in the primary visual cortex.
Acknowledgements: this work was supported by an EU-grant - Euroheadpain n° 602633
Disclosure of Interest
M. Lisicki: None Declared, K. D'Ostilio: None Declared, A. Maertens De Noordhout: None Declared, J. Schoenen Conflict with: Cefaly Technology, D. Magis: None Declared
Headache Pathophysiology - Imaging and Neurophysiology
PO-01-008
Altered brainstem anatomy in migraine
Kasia K. Marciszewski1,*, Noemi Meylakh1, Flavia Di Pietro1, Vaughan G. Macefield2, Paul M. Macey3 and Luke A. Henderson1
1Department of Anatomy and Histology, University of Sydney
2School of Medicine, University of Western Sydney, Sydney, Australia
3UCLA School of Nursing and Brain Research Institute, University of California, Los Angeles, United States
Objectives
Migraine is a common and debilitating neurological disorder characterised by unilateral throbbing, severe headaches, and often accompanied by nausea and photophobia. The exact mechanisms responsible for migraine remain unknown, although it has been proposed that changes in brainstem anatomy and function, even between attacks, may contribute to the initiation and maintenance of headache during migraine attacks. The aim of this investigation is to use brainstem-specific analyses of anatomical and diffusion weighted images to determine if the trigeminal system displays altered structure in individuals with migraine.
Methods
Using a 3 Tesla MRI scanner (Philips) we collected a high resolution T1-weighted anatomical (TR =5.6 sec., TE = 2.5 ms, raw voxel size 0.9×0.9×0.9 mm) and 2 diffusion tensor images (32 directions, b0, b1000, raw voxel size 2×2×2.5 mm) in 24 migraineurs and 57 control subjects. All migraineurs were scanned during their interictal phase, i.e. at least 72 hours after a migraine and not within 24 hours of a migraine attack. All images were processed using Matlab and SPM12 software. In each individual, mean diffusivity maps were created using the DTI image sets. Using the SUIT toolbox, the brainstem region of the T1-weighted anatomical images and the mean diffusivity (MD) images were isolated and normalized to a brainstem specific template in Montreal Neurological Institute space and smoothed using a 3 mm FWHM Gaussian filter. Significant differences in regional brainstem volume and mean diffusivity were then determined using a random effects procedure (p < 0.05, small volume corrected).
Results
We found grey matter volume decreases in migraineurs in the region of the spinal trigeminal nucleus and dorsomedial pons. In addition, reduced grey matter volume and increased free water diffusivity occurred in areas of the descending pain modulatory system, including midbrain periaqueductal gray matter, dorsolateral pons, and medullary raphe. These changes were not correlated to migraine frequency, duration, intensity or time to next migraine.
Conclusion
This data revealed that when compared to controls, interictal migraineurs show decreased grey matter volume within key brainstem areas know to be activated during migraine attacks in addition to areas involved in endogenous pain modulation. Additionally, increased free water diffusivity occurred in areas of the descending pain modulation system. These data suggest that brainstem anatomy changes may underlie changes in activity that result in activation of the ascending trigeminal pathway and the perception of head pain during a migraine attack.
Disclosure of Interest
None Declared
Headache Pathophysiology - Imaging and Neurophysiology
PO-01-009
Nonlinear visual processing is faster in migraine with aura
Matthijs Perenboom1,*, Yuan Yang2, Johannes Carpay1, Frans van der Helm2, Michel Ferrari1, Alfred Schouten2 and Else Tolner1
1Neurology, Leiden University Medical Centre, Leiden
2Biomechanical Engineering, Delft University of Technology, Delft, Netherlands
Objectives
Visual system abnormalities in migraine are linked to symptoms like photophobia and the visual aura. Little is known about the mechanisms contributing to these visual system alterations. Processing of visual input by the brain is a highly nonlinear operation, involving complex interactions among cortical and subcortical neuronal networks. Timing of this process can be estimated by analysing the cortical response to external light input at different frequencies. Using a sum-of-sinusoid light signal, instead of the classic pulse train, as input and novel EEG analyses it is possible to assess the time delay and frequency domain response. Here we investigate nonlinear visual processing in subgroups of migraine patients and headache-free participants.
Methods
Migraine patients with aura, without aura and healthy participants (N = 10/group) were subjected to bi-sinusoidal light stimulation for 320 1 sec-epochs, while scalp EEG was recorded at the occipital, parietal and frontal lobes. Light stimulus frequencies were chosen to guarantee no overlap of their harmonic and intermodulation frequencies for different orders of nonlinearity. Nonlinear interactions and time delay from stimulus to cortical EEG response were analysed in the frequency domain using novel phase clustering measures and amplitude spectral measures.
Results
Higher harmonic and intermodulation interactions were detected between visual input and cortical responses. Amplitude spectrum and phase clustering responses differed per order and group. Migraine patients with aura showed a decreased time delay only at the occipital lobe compared to healthy controls and migraine patients without aura.
Conclusion
Visual processing is altered in migraine patients with aura compared to healthy controls and patients without aura. Furthermore, we demonstrated the potential of quantifying nonlinear interactions and temporal dynamics in the visual system using sum-of-sinusoid light stimulation. We are able to uncover alterations in visual processing in the context of neurological disease.
Disclosure of Interest
None Declared
Headache Pathophysiology - Imaging and Neurophysiology
PO-01-010
TRPA1 channel activation by cinnamaldehyde: Are migraine patients more susceptible than healthy subjects?
Linde Buntinx1,*, Sergio Barroso1, Joyce Vandendriessche1, Bart Govers1, Bart Morlion2 and Jan de Hoon1
1Center for Clinical Pharmacology, Department of Pharmaceutical and Pharmacological Sciences
2Leuven Center for Algology, Department of Cardiovascular Sciences, KU Leuven, Leuven, Belgium
Objectives
Previous studies have shown that some known triggers of migraine activate transient receptor potential (TRP) channels, in particular TRP Ankyrin subtype 1 (TRPA1), which makes this an interesting target for migraine therapy. TRPA1 is a nonselective cation channel functioning as a chemical nociceptor which is activated by cinnamaldehyde (CA). Cinnamaldehyde-induced dermal blood flow (CA-DBF) response has been established as a non-invasive, reproducible in vivo human model for TRPA1 activation in healthy volunteers1. The objective of this study is to determine whether the CA-induced DBF and pain response is different between female migraine patients, with and without aura, and healthy volunteers.
Methods

Results
Topical application of 10% CA evoked an increase in DBF that did not differ between migraine patients (with and without aura) and healthy controls neither when expressed as Area Under the Curve (AUC0–40 min), nor when measuring the pain scores (table 1). The peak mean DBF response was observed 15 minutes post CA application in all groups.
Conclusion
Although preclinical literature suggests that TRPA1 plays an important role in migraine, we did not find a difference in the peripheral DBF response or pain response to CA-induced activation of TRPA1 between migraineurs and healthy subjects.
Disclosure of Interest
None Declared
Headache Pathophysiology - Imaging and Neurophysiology
PO-01-011
Visual evoked potentials in episodic and chronic migraine – a pilot study
Chi-Ieong Lau1,2,*, Tzu-Yu Hsu3,4, Lin-Yuan Tseng3 and Wei-Hung Chen1,5
1Department of Neurology, Shin Kong Wu Ho-Su Memorial Hospital, Taipei City, Taiwan, Republic of China
2Institute of Cognitive Neuroscience, University College London, London, United Kingdom
3Research Center for Brain and Consciousness
4Graduate Institute of Health and Biotechnology Law
5College of Medicine, Taipei Medical University, Taipei City, Taiwan, Republic of China
Objectives
Most studies reported a deficient habituation of visual-evoked potentials (VEPs) interictally in episodic migraine (EM). Chronic migraine (CM), in contrary, exhibits normal habituation, suggesting the presence of persistent ictal-like cortical excitability. Discrepant results, however, exist with regard to VEP amplitudes in migraineurs. In this pilot study, we aimed to confirm these findings by comparing the VEP habituation and amplitudes between EM, CM and healthy controls (HC).
Methods
Pattern-reversal VEPs (6 blocks of 100 sweeps, each for 1 min) were recorded in 10 migraineurs without aura (5 interictal EM and 5 CM with prophylactic treatment) as well as 12 HC. We measured and compared the VEP amplitudes and habituation (slope of the linear regression line of amplitude changes from the 1st to 6th block of 100 sweeps) between the three groups.
Image:

Results
In general, both EM and CM exhibited higher VEP amplitudes than HC. CM showed significantly higher first block VEP amplitudes than EM (p = 0.01). Regarding VEP habituation, controls showed a typical VEP habitation where the amplitudes of VEP decreased as time progressed. Thus, the slope was negative in HC (HC slope: −.52). Yet the VEP slopes in CM and EM were close to zero (CM =−.11, EM = 0.13, figure 1), in which no obvious VEP habituation was found in both groups. In addition, the slope of VEP in HC was significantly lower than that of EM and CM (EM vs. HC, p = .043; CM vs. HC, p = .060).
Conclusion
Our findings confirmed the lack of VEP habituation in EM. In contrast to previous studies, however, CM did not exhibit a normal pattern of habituation, suggesting a possible role of prophylaxis in the modulation of cortical excitability. The increased VEP amplitudes in both EM and CM, as compared to HC, were likely to be related to hyper-responsive visual cortical excitability.
Disclosure of Interest
None Declared
Headache Pathophysiology - Imaging and Neurophysiology
PO-01-012
Time-frequency analysis of visual evoked potentials in migraine: getting a better insight into habituation
Marco Lisicki1,*, Kevin D'Ostilio1, Alain Maertens de Noordhout2,3, Jean Schoenen2,3 and Delphine Magis1,3
1Headache Research Unit
2Neurology, Université de Liège
3Neurology, Centre Hospitalier Universitaire, Liège, Belgium
Objectives
Visual evoked potentials (VEP) are characterized by a lack of habituation during prolonged stimulation in migraine patients between attacks (Schoenen et al). As this abnormality was not found in some studies (Omland et al.), we decided to assess the habituation phenomenon with time-frequency analysis. In detail, the aim of this study was to perform a time-frequency analysis of VEP and their habituation profile, comparing healthy volunteers and interictal migraine patients.
Methods
Twenty-one healthy volunteers (age 35.5 ±11.5, 16F/5M) and 21 interictal migraine without aura patients (ICHD3beta 1.1) (age 34.1 ± 13.9, 16F/5M) participated in the study. For VEP, 600 epochs were uninterruptedly recorded at Oz (Ref Fz) using a pattern reversal stimulus (3.1 Hz, 68°). Artefacted epochs were rejected (<5%). N1-P1 amplitude, event related spectral perturbations (ERSP) and inter-trial coherence (ITC) were calculated in six successive blocks of 95 epochs. For comparison, data from time-frequency analyses were extracted from a 60−120 ms time window (the range where N1 and P1 occur). VEP were processed in EEGLAB running in MATLAB (The MathWorks Inc.). Statistical analyses and graphs were performed in SPSS 20 (IBM Corp.).
Results
Throughout the stimulation, a significant reduction in power, i.e. habituation, was found in healthy volunteers but not in migraine patients. Inter-trial coherence progressively diminished in both groups, but to a greater extent in migraineurs. There was no difference between groups in the time domain. The N1-P1 habituation slope positively correlated with the ITC slope.
Conclusion
Unlike in healthy volunteers, continuous visual stimulation does not induce habituation in migraine patients as evidenced by ERSP analysis. Because of the major role inter-trial coherence plays in classic evoked potential results, peak-to-peak amplitude itself might not accurately reflect neuronal activation. Indeed, significant modifications in brain dynamics can remain undetected when limiting analyses to the time domain.
Acknowledgements: this work was supported by an EU-grant - Euroheadpain n° 602633
Disclosure of Interest
M. Lisicki: None Declared, K. D'Ostilio: None Declared, A. Maertens de Noordhout: None Declared, J. Schoenen Conflict with: Cefaly Technology, D. Magis: None Declared
Headache Pathophysiology - Imaging and Neurophysiology
PO-01-013
Altered brain functional connectome in migraine with and without comorbid restless legs syndrome: A resting-state functional MRI study
Fu-Chi Yang1,*, Kun-Hsien Chou2, Ai-Ling Hsu3, Jong-Ling Fuh4, Jiing-Feng Lirng5, Ching-Po Lin6 and Shuu-Jiun Wang4
1Departments of Neurology, Tri-Service General Hospital, National Defense Medical Center, Taiwan
2Brain Research Center, National Yang-Ming University, Taiwan
3Graduate Institute of Biomedical Electronics and Bioinformatics, National Taiwan University, Taiwan
4Neurological Institute, Taipei Veterans’ General Hospital, Taiwan
5Department of Radiology, Taipei, Veterans’ General Hospital, Taiwan
6Institute of Neuroscience, National Yang-Ming University, Taiwan, Taipei, Taiwan, Republic of China
Objectives
Patients with migraine are frequently comorbid with restless legs syndrome (RLS), although little is known regarding the neurological basis of this association. Both disorders are characterized by distributed functional abnormalities suggesting alterations in the functional connectivity (FC) of multiple brain networks. We investigated functional network changes in migraine patients with and without comorbid RLS to identify common and distinct patterns of functional reorganization associated with these clinically comorbid disorders.
Methods
We used resting-state functional magnetic resonance imaging and network-wise analytical approaches to investigate alterations in functional connectomes in 22 migraine patients with RLS, 22 migraine patients without RLS, and 19 healthy controls. Group comparisons and conjunction analyses were used to identify networks wherein the disorders were associated with common and distinct patterns of functional connectomes changes. Additional regression analysis was used to identify associations between alterations in functional connectomes and clinical profiles.
Image:

Results
Patients with migraine with and those without RLS had lower FC than healthy controls in the dorsal attention, salience, default mode, cingulo-opercular, visual, fronto-parietal, auditory, and sensory/somatomotor networks, which are related to attentional control and sensation. Both migraine groups also shared common patterns of functional connectome changes in sensory/somatomotor, sensory/somatomotor to auditory, and dorsal attention to auditory networks. There was a trend-level significance for functional connectome differences in the salience, default mode to subcortical and fronto-parietal, auditory to salience, and memory retrieval networks between the two migraine groups. Cross-network abnormality in the default mode to subcortical network in particular had a trend-level significance for an association with RLS severity in migraine patients with RLS.
Conclusion
We found disruptions of the brain functional connectome in migraine patients with and without comorbid RLS. This may lead to potential insight into the differential neuropathological mechanisms and the design of potential neuroimaging-driven biomarkers for migraine with and without comorbid RLS.
Disclosure of Interest
None Declared
Headache Pathophysiology - Imaging and Neurophysiology
PO-01-014
Alterations in regional cerebral blood (rCBF) during nitroglycerin (NTG) triggered migraine headache assessed using arterial spin-labelled (ASL) functional magnetic resonance imaging (fMRI)
Nazia Karsan1,2,*, Pyari Bose1,2, Fernando O. Zelaya3 and Peter J. Goadsby1,2
1Headache Group, Department of Basic and Clinical Neuroscience, Institute of Psychiatry, Psychology and Neuroscience, King's College London
2NIHR-Wellcome Trust King's Clinical Research Facility, King's College Hospital
3Centre for Neuroimaging Sciences, Institute of Psychiatry, Psychology and Neuroscience, King's College London, London, United Kingdom
Objectives
Functional imaging in headache research is an increasing area of interest within headache research, because of the insights it can offer in humans into the pathophysiology and neurobiology of the migraine attack. Triggered attacks provide a reproducible and predictable model with which to study migraine.
We aimed to study the phenotype and imaging characteristics of the headache stage of migraine using NTG triggered attacks, which have been shown to effectively headache attacks in a large proportion of migraineurs. The imaging modality we used was pulsed continuous Arterial Spin Labelling (pCASL), performed on a 3T General Electric MR750 MRI scanner.
Methods
Subjects (n = 18) were recruited following screening and informed consent. Each subject was exposed to either a 0.5 mcg/kg/min NTG infusion over 20 minutes or placebo, depending on randomisation. Each subject received both infusions on two different visits and was blinded to which treatment was being administered. Following the infusion, the timeline and phenotype to development of headache symptoms was documented. A standardised physician administered symptom checklist was used for data collection.
Migraine headache was defined as moderate-severe headache which developed after the infusion and was associated with other migraine symptomatology that the subject would usually associate with spontaneous attacks.
Imaging (structural T1, T2 and FLAIR, resting state blood oxygen level dependant imaging (rsBOLD) and two six minute pCASL maps) was conducted over 30–40 minutes at baseline and rsBOLD and pCASL during migraine headache. For the placebo visit the imaging was conducted at the same times following infusion in the absence of symptoms. Following scanning, the migraine headache was treated with either 6 mg subcutaneous Sumatriptan or 1 g intravenous aspirin.
Imaging was analysed using SPM 12 (www.fil.ion.ac.uk/SPM). Voxel based analysis of all subjects’ headache scans compared to baseline was carried out.
Results
With whole brain, voxel-wise analysis, significant increases in rCBF were detected in a large cluster that includes anterior frontal, orbito-frontal and parts of the anterior cingulate cortices (p = 0.004 corrected for multiple comparisons at the cluster level). Using a small volume spherical correction, significant increases were also observed in the posterior cingulate cortex (p = 0.031), in the region of the dorsomedial and centromedian thalamic nuclei and in the rostromedial midbrain (p = 0.05). No significant reductions in rCBF were detected.
Conclusion
The headache stage of NTG-triggered migraine is associated with significant areas of increased rCBF compared to baseline, in frontal cortex, anterior cingulate cortex, thalamus and rostral midbrain. The finding of these areas is consistent with previous work suggesting the vital role of the brainstem and other subcortical areas in migraine, as well as other classical pain matrix areas.
This study demonstrates the usefulness of ASL in a cohort of migraine patients, as a means of interrogating areas of brain activity changing in response to the headache. The results are consistent with previous studies using blood oxygen level dependant (BOLD) and positron emission tomography (PET) imaging. ASL fMRI is promising non-invasive imaging modality, using rCBF as a correlate of neuronal activity, and could be increasingly used in migraine research.
Disclosure of Interest
N. Karsan Conflict with: Dr Karsan is an Association of British Neurologists/Guarantors of Brain Clinical Research Training Fellow, P. Bose: None Declared, F. Zelaya: None Declared, P. Goadsby Conflict with: Dr. Goadsby reports grants and personal fees from Allergan, Amgen, and Eli-Lilly and Company; and personal fees from Akita Biomedical, Alder Biopharmaceuticals, Autonomic Technologies Inc, Avanir Pharma, Cipla Ltd, Colucid Pharmaceuticals, Ltd, Dr Reddy's Laboratories, eNeura, Electrocore LLC, Novartis, Pfizer Inc, Promius Pharma, Quest Diagnostics, Scion, Teva Pharmaceuticals, Trigemina Inc., Scion, Conflict with: personal fees from MedicoLegal work, Journal Watch, Up-to-Date, Oxford University Press; and in addition, Dr. Goadsby has a patent Magnetic stimulation for headache pending assigned to eNeura
Headache Pathophysiology - Imaging and Neurophysiology
PO-01-015
Distinct cerebral metabolic patterns related to trigeminal sensory profiles in migraine patients and healthy volunteers
Kevin D'Ostilio1, Marco Lisicki1,*, Alain Maertens de Noordhout2,3, Jean Schoenen2,3 and Delphine Magis1,3
1HeadRUN
2Neurology, Universitè de Liège
3Neurology, Centre Hospitalier Universitaire, Liège, Belgium
Objectives
Episodic migraine patients are thought to be overall hypersensitive to various stimuli between (Ambrosini 2006) and allodynic during (Burstein et al. 2000) attacks, while chronic migraine patients may be permanently allodynic (Bigal et al. 2008). However, there is great variability within patients groups in all studies. It seems thus of interest to identify subgroups of patients with different pain sensitivities and to investigate whether this reflects in distinct brain activity patterns. We decided to analyse thermal perception and pain thresholds in the 1st division of the trigeminal nerve in large cohorts of healthy volunteers (HV), episodic migraine patients between attacks (EM) and chronic migraine patients (CM), and to search for correlations with brain metabolism assessed with FDG-PET.
Methods
A total of 173 subjects (mean age: 35 ± 14 years) underwent quantitative sensory testing (QST): 54 HV (70% fem); 69 EM patients (83% fem), and 50 CM patients (86% fem). Sensory and pain thresholds to cold and warm stimuli were determined using a 1.5×1.5 cm thermode (Advanced Thermal Stimulator-Medoc.) placed on the right forehead during three consecutive runs. Additionally, fifty-five subjects underwent an 18-FDG-PET scan (Philips Medical Systems): 20 HV, 21 EM without aura and 14 CM.
Results
QST (n = 173).No significant difference was found between subject groups for Cold Sensory Threshold (CST), Heat Sensory Threshold (HST), Cold Pain Threshold (CPT) or Heat Pain Threshold (HPT). A K-means cluster analysis however (Freeman et al. 2014), revealed the existence of 2 distinct sensory profiles within the global population (namely ‘hyper-’ and ‘hyposensitive’), which significantly differed in all QST variables (CST, p < 0.001; HST, p < 0.001; CPT, p < 0.001; HPT, p < 0.001, Fig. 1). Based on k-means cluster pain profiles, both heat and cold pain thresholds were significantly reduced in ‘hypersensitive’ CM compared with ‘hypersensitive’ HV (CPT: p = 0.05; HPT: p = 0.02), indicating that CM patients are hypersensitive to pain.
FDG-PET (n = 55).In EM, compared to HV, FDG uptake was reduced in left visual cortex, left medial frontal gyrus and bilaterally in the insular, somatosensory and motor cortices. CM had also a reduced metabolism in the orbitofrontal (OFC) and rostral anterior cingulate cortices (rACC).
Cerebral metabolism differed between hyper- and hyposensitive individuals with a
distinct pattern in each subgroup (Fig. 2). Compared to hyposensitivity,
hypersensitivity was associated with reduced metabolism in the brainstem in EM, the
thalamus in CM and the somatosensory and anterior cingulate cortices in
HV
Conclusion
Overall, we found no difference in trigeminal perception or pain thresholds for cold or warm stimuli between episodic or chronic migraine patients and healthy subjects. Collectively, cluster analysis of QST results disclosed ‘hypersensitive’ and ‘hyposensitive’ subgroups. When compared to their counterparts, ‘hypersensitive’ subjects had decreased metabolism in key pain processing regions of the CNS, but these regions differed between migraine patients (brainstem, thalamus) and healthy volunteers (somatosensory and cingulate cortices). This suggests that individual pain sensitivity is controlled by cortical pain matrix areas in healthy subjects, but that this control shifts to subcortical structures in episodic and chronic migraine patients. Acknowledgements: This work was supported by the EUROHEADPAIN project, FP7-602633
Disclosure of Interest
K. D'Ostilio: None Declared, M. Lisicki: None Declared, A. Maertens de Noordhout: None Declared, J. Schoenen Conflict with: Cefaly Technology, D. Magis: None Declared
Headache Pathophysiology - Imaging and Neurophysiology
PO-01-016
A conditioning photic stimulation changes the photic driving amplitude in peri-ictal migraineurs
Delphine Magis1,2,*, François Gabrielli3, Marco Lisicki2, Radhouane Dallel3,4, Kevin D'Ostilio2, Jean Schoenen1,5 and Lenaic Monconduit3
1Neurology, Centre Hospitalier Universitaire
2Headache Research Unit, Université de Liège, Liège, Belgium
3Neuro-Dol, Univ. Clermont Auvergne
4Service d'Odontologie, CHU Clermont-Ferrand, Clermont-Ferrand, France
5Neurology, Université de Liège, Liège, Belgium
Objectives
Increased electroencephalographic (EEG) photic driving amplitude (PD) is reported in migraine patients and has been interpreted as a sign of cortical hyperresponsiveness1,2. However PD amplitude may be overestimated2,3 and differs throughout the migraine cycle2. Hence, increased and decreased PD has been reported during peri-ictal and inter-ictal phases, respectively2. The higher discriminating power of PD is usually seen around 20–25 Hz. In this study, we aimed to investigate whether a conditioning photic stimulation influenced the PD power of the following stimuli at different phases of migraine.
Methods
Eighty-one subjects underwent a standard 20-channel EEG (Nicolet, NatusMedical) with intermittent photic stimulation: 26 healthy volunteers (HV, 36.9 ± 14.2 years, 88% F) and 55 episodic migraineurs (EM, 33.6 ± 12.2 years, 83.6% F, 15% with aura). Patients were pseudorandomly assigned to 2 groups: group A (N = 48) was stimulated at 5 Hz, 10 Hz and 20 Hz whereas group B (N = 33) was stimulated at 5 Hz, 20 Hz and 20 Hz frequencies (15s interstimulus and stimulus durations). EM population was divided into inter-ictal (n = 23), peri-ictal (n = 18), and ictal (n = 14) subgroups based on the occurrence of an attack within 72 h preceding/following the recordings.
The EEG data were preprocessed using EEGLAB, an open-source MATLAB toolbox for electrophysiological signal processing and analysis5. After epoch extraction, artifact and eyes contamination rejection, EEG spectral power was computed on each electrode, using Fast Fourier Transform was calculated on de-averaged signals of the parietal, occipital and temporal electrodes. We then compared the maximum of EEG power in the beta-range of the groups A and B EM or HV.
Results
PD to 5 Hz stimuli was similar between HV and all EM subgroups. The conditioning stimulus at 10 or 20 Hz did not change the power of the following PD in HV for the parietal, occipital and temporal electrodes (p = 0.4, p = 0.6, p = 0.9, respectively), nor in EM in ictal or inter-ictal phases. Conversely, in EM peri-ictal phase, PD power significantly decreased after a conditioning stimulus of 10 Hz, but not of 20 Hz. Thus, after the conditioning stimulus at 10 Hz, P3, P4, O1, O2, T5, T6 PD powers were respectively 0.018 ± 0.008, 0.014 ± 0.008, 0.016 ± 0.006, 0.014 ± 0.006, 0.015 ± 0.005, and 0.014 ± 0.005 V2. Hz-1, whereas after the conditioning stimulus at 20 Hz, the values were respectively 0.035 ± 0.012, 0.027 ± 0.016, 0.042 ± 0.010, 0.036 ± 0.015, 0.028 ± 0.013 and 0.027 ±0.007 V2. Hz-1 (p = 0.01, p = 0.03, p = 0.004, p = 0.004, p = 0.03, p = 0.002, respectively).
Conclusion
Photic driving can be modulated by a conditioning photic stimulus in proximity of a migraine attack. This preliminary result suggests that visual cortical processing may be differently influenced by external sensory stimulations during this phase of migraine. More patients are being included to confirm these findings, and especially to compare pre-ictal to post-ictal phases.
References
1 Gantenbein et al, 2014. Cephalalgia 34:554–8
2 Bjork et al, 2010. Cephalalgia 31:444–55
3 Fogang et al, 2015. Acta Neurol Belg 115:39–45
5 Delorme and Makeig, 2004. J Neurosci Methods 134:9–21
Disclosure of Interest
D. Magis: None Declared, F. Gabrielli: None Declared, M. Lisicki: None Declared, R. Dallel: None Declared, K. D'Ostilio: None Declared, J. Schoenen Conflict with: Cefaly Technology, L. Monconduit: None Declared
Headache Pathophysiology - Imaging and Neurophysiology
PO-01-017
Whole-brain resting state default mode network connectivity during spontaneous migraine attacks
Gianluca Coppola1,*, Antonio Di Renzo1, Emanuele Tinelli2, Cherubino Di Lorenzo3, Vincenzo Parisi1 and Francesco Pierelli4,5
1Research Unit of Neurophysiology of Vision and Neurophthalmology, G. B. Bietti Foundation IRCCS
2Department of Neurology and Psychiatry, Sapienza University of Rome, Rome
3Department of Neurology, Don Carlo Gnocchi Onlus Foundation, Milan
4Department of medico-surgical sciences and biotechnologies, Sapienza University of Rome Polo Pontino, Latina
5Headache Clinic, IRCCS-Neuromed, Pozzilli, Italy
Objectives
The default mode network (DMN) is composed by a set of brain regions including medial prefrontal cortex (MPFC), posterior cingulate cortex (PCC), and parietal lobule (PL). Disruption of the integrity of DMN connectivity has been previously observed in migraine between attacks. Here we aimed to investigate whole-brain resting state DMN connectivity during spontaneous untreated migraine attacks.
Methods
Thirteen patients with untreated migraine without aura (MI) underwent 3T MRI scans during the initial 6 hours of a spontaneous migraine attack and were compared to the scans of a group composed of 19 healthy volunteers (HV). Using a seed-based approach, we collected resting state data in the abovementioned regions of the DMN. Thereafter, we collected whole-brain connectivity patterns with the seeds representing DMN (conjunction analysis).
Results
There was greater correlation in MI than in HV between regions associated with DMN, including MPFC, PCC, and PL. The conjunction analysis revealed common activation between i) MPFC and left inferior frontal cortex (pars triangularis), left dorsal posterior cingulate cortex, and left associative visual cortex; ii) right PL and bilateral somatosensory association cortices, and left associative visual cortex.
Conclusion
To summarize, we documented associations between DMN and brain regions involved in multimodal brain processing, including visual, somatosensory, and verbal during spontaneous migraine attacks. Whether present findings are related to the ictal migraineurs abnormal sensory perception, such as photophobia and allodynia, and to the ictal drop in verbal fluency remains to be determined.
Disclosure of Interest
None Declared
Headache Pathophysiology - Imaging and Neurophysiology
PO-01-018
White matter lesions in cronic migraine are not associated with changes in pulsatility index
Davinia Larrosa1, César Ramón Carbajo1, Eva Cernuda Morollón2, Pablo Martínez-Camblor3 and Julio Pascual Gómez4,*
1Neurology, H.U.C.A.
2University of Oviedo, OVIEDO, Spain
3Statistical analysis, Geisel School of Medicine at Darmouth, Hanover, United States
4NEUROLOGY, H.U.M.V., Santander, Spain
Objectives:
White matter lesions (WML) are more prevalent in migraine; it seems that mainly with a high attack frequency. A vascular etiology has been proposed, but their pathogenesis and clinical significance remains unknown. Pulsatility Index (PI) reflects the vascular resistance and an increase of PI is a marker of structural changes of the small vessels due to lipohyalinosis and microatherosclerosis.
White matter lesions (WML) are more prevalent in migraine; it seems that mainly with a high attack frequency. A vascular etiology has been proposed, but their pathogenesis and clinical significance remains unknown. Pulsatility Index (PI) reflects the vascular resistance and an increase of PI is a marker of structural changes of the small vessels due to lipohyalinosis and microatherosclerosis.
The aim of this stydy is to determine whether differences in PI can be used as an indirect marker of an ischemic nature for WML found in cranial MRI studies of chronic migraine (CM) patients.
Methods
This series includes 91 CM women. PI was measured on transcranial Doppler in both middle cerebral arteries (MCA), posterior cerebral arteries (PCA) and in the basilar artery (BA) according to Gosling’s formula. MRIs were acquired on a 1.5T unit following the CAMERA protocol.
Results
A total of 58 CM patients (46.8 ± 10.1 years) had WML, whereas 33 (35,6 ± 12.0 years) did not. Except for age (p < 0.001) the rest of clinical features and comorbidities -including aura, vascular risk factors and acute/preventive treatments- were similar between both groups.
PI was within range in all arteries examined. In patients with WML, mean PI was: MCA 0.888 ± 0.141, PCA 0.886 ± 0.143 and BA 0.852 ± 0.144. In patients without WML, mean PI was: MCA 0.912 ± 0.126, PCA 0.938 ±0.162 and BA 0.876 ± 0.116. There were no differences in mean PI in any of the arteries explored (MCA p = 0.265, PCA p = 0.155, BA p = 0.636) for patients with and without WML.
Conclusion
There were not differences in PI values in the different arteries explored according to the presence or not of WML. These findings argue against an ischemic nature of these lesions in migraine patients.
Disclosure of Interest
D. Larrosa: None Declared, C. Ramón Carbajo: None Declared, E. Cernuda Morollón: None Declared, P. Martínez-Camblor: None Declared, J. Pascual Gómez Conflict with: Supported by the PI14/00020 FISSS grant (Fondos Feder, ISCIII, Ministry of Economy, Spain)
Headache Pathophysiology - Imaging and Neurophysiology
PO-01-019
Cerebral metabolism changes measured with PET-FDG in medication overuse headache before and after withdrawal
Marta Torres-Ferrus1,2,*, Gemma Cuberas3, Manuel Quintana1, Victor J. Gallardo-Lopez1, Carles Lorenzo Busquets3, Jose Alvarez-Sabin2, Joan Castell Conesa3 and Patricia Pozo-Rosich1,2
1Headache and Neurological Pain, Vall d'Hebron Research Institute
2Neurology
3Nuclear Medicine, Vall d'Hebron University Hospital, Barcelona, Spain
Objectives
To evaluate cerebral metabolism in patients with medication overuse headache (MOH) before and after analgesic withdrawal.
Methods
We included adults who fulfilled ICHD-3beta criteria for chronic migraine and MOH who were not taking any migraine preventive treatment or other neurologic/psychiatric medication. We included control subjects without personal or familiar headache history. We collected clinical data and performed a baseline PET-FDG and 6 weeks after analgesic withdrawal. Images were uploaded to a reference atlas to obtain a mean metabolism value for 30 cerebral regions. We performed statistical analysis comparing controls with MOH patients and a paired sample test to compare values before and after withdrawal
Results
We included 11 women; 9 completed the withdrawal protocol. The mean age was 50.8 ± 6.8 (38–62) and the intake of acute medication was 28.2 ± 2.7 (24–30) days/month and 51.4 ± 26.6 (24–90) pills/month. All subjects did a successful withdrawal with a statistical significant change in the number of headache and acute medication intake days and number of pills/month.
Compared to controls, MOH subjects showed an initial global hypometabolism that was more significant in cerebral anterior areas (right/left): precentral gyrus (p =0.002/p = 0.012), olfactory (p = 0.015/p = 0.020), frontal superior (p = 0.020/p = 0.019), rectus gyrus (p = 0.005/p = 0.010) and insula (p = 0.09/p = 0.007). After analgesic withdrawal there was a global trend towards normalization of cerebral metabolism but no individual significant differences were found; the areas that maintain hypometabolism compared to controls were precentral gyrus (p = 0.011/p = 0.047), rectus gyrus (p = 0.009/p = 0.016) and insula (p = 0.021/p = 0.017).
Conclusion
Medication overuse is associated with fronto-temporal cerebral hypometabolism which normalizes after 6 weeks of withdrawal except in the precentral, rectus gyrus and insula areas.
Disclosure of Interest
None Declared
Headache Pathophysiology - Imaging and Neurophysiology
PO-01-020
Nitroglycerin triggering as a human migraine model in clinical research
Nazia Karsan1,2,*, Pyari Bose1,2, Charlotte Thompson1 and Peter J. Goadsby1,2
1Headache Group, Department of Basic and Clinical Neuroscience, Institute of Psychiatry, Psychology and Neuroscience, King's College London
2NIHR-Wellcome Trust King's Clinical Research Facility, King's College Hospital, London, United Kingdom
Objectives
Exogenous triggering with substances such as nitroglycerin (NTG) has been developed to enable migraine attacks to be studied in a predictable and reproducible fashion.
We aimed to study NTG triggering of migraine attacks, with a view to phenotyping these compared to spontaneous attacks and imaging them using functional MRI.
Methods
Potentially eligible subjects were telephone screened, invited to a screening appointment and recruited following informed consent, a detailed migraine history, re-assessment of eligibility, clinical observations, an electrocardiogram, a pregnancy test if applicable and a physical examination. All subjects were aged 18–50 years of age, with a migraine diagnosis and between 0–22 days of headache a month and no contraindications to NTG or any of the study drugs.
Each eligible subject was exposed to a 0.5 mcg/kg/min NTG infusion over 20 minutes. The phenotype and timeline to development of migraine symptomatology following triggering was documented. Migraine headache was defined as moderate-severe headache occurring after the completion of the NTG infusion with associated symptomatology that the subject would usually associate with a migraine. Migraine headache was treated in all subjects with intravenous aspirin 1 g or subcutaneous Sumatriptan 6 mg.
The association between baseline migraine diagnosis (episodic vs. chronic) and effectiveness of NTG triggering migraine headache was analysed using the Chi-squared test. Binary logistic regression was used to analyse the association between headache days and successfulness of triggering. P < 0.05 was considered significant.
Results
Forty-nine (9 males) subjects were recruited. The age range was 18–50 years (mean 36 years). MIDAS scores ranged between 0 and 201 (median = 22). The monthly baseline headache frequency ranged from 0–22 days (median = 8). Subjects with more than 22 headache days per month were excluded from the study, due to the high risk of having a spontaneous headache on study visit days. Of the 49 subjects, 25 had episodic migraine with aura (EMA), 19 had episodic migraine without (EMO) and 5 had chronic migraine (CM).
Migraine headache was successfully triggered in 40 subjects (82%). Aura was triggered in 4 subjects. There was a trend towards a statistically significant association (p = 0.061) between effective triggering and chronic migraine versus episodic. All 9 subjects who did not trigger a headache with NTG had episodic migraine with monthly headache days ranging from 0–10.
Using binary logistic regression, the model correctly calculated which subjects would trigger in 82% of cases (p = 0.039). The relationship between headache days at baseline and the successful triggering of headache using NTG showed a trend (OR = 1.184, 95% CI 0.989–1.147, p = 0.066). Inclusion of age of the subjects did not add to this model.
Conclusion
NTG is an effective migraine trigger. Successful triggering may be related to a threshold effect, associated with baseline headache frequency.
Disclosure of Interest
N. Karsan Conflict with: Dr Karsan is an Association of British Neurologists/Guarantors of Brain Clinical Research Training Fellow, P. Bose: None Declared, C. Thompson: None Declared, P. Goadsby Conflict with: Dr. Goadsby reports grants and personal fees from Allergan, Amgen, and Eli-Lilly and Company; and personal fees from Akita Biomedical, Alder Biopharmaceuticals, Autonomic Technologies Inc, Avanir Pharma, Cipla Ltd, Colucid Pharmaceuticals, Ltd, Dr Reddy's Laboratories, eNeura, Electrocore LLC, Novartis, Pfizer Inc, Promius Pharma, Quest Diagnostics, Scion, Teva Pharmaceuticals, Trigemina Inc., Scion, Conflict with: personal fees from MedicoLegal work, Journal Watch, Up-to-Date, Oxford University Press; and in addition, Dr. Goadsby has a patent Magnetic stimulation for headache pending assigned to eNeura
Headache Pathophysiology - Imaging and Neurophysiology
PO-01-021
Electrophysiological signatures of altered intrinsic connectivity between insula cortex and default mode network in patients with fibromyalgia
Fu-Jung Hsiao1, Wei-Ta Chen2,* and Shuu-Jiun Wang2
1National Yang-Ming Univ.
2Veterans General Hospital, Taipei, Taiwan, Republic of China
Objectives
Fibromyalgia (FM) is a disabling chronic pain syndrome with unknown pathophysiology. Previous functional MRI studies in FM suggested altered brain connectivity between insula and the default mode network (DMN). However, this connectivity change has not been characterized in direct neural signals with spatial and spectrotemporal analyses, especially when neural oscillatory is a hallmark of cortical network function in various brain regions.
Methods
Resting-state magnetoencephalographic (MEG) activities were recorded from 28 patients with FM and 28 age-and sex-matched controls. Source-based functional connectivity between insula cortex and DMN at 1–40 Hz was analyzed using minimum norm estimates (MNE) and imaginary-coherence functional connectivity analysis, and statistically examined with the depression scores, age and sex as covariates. The measurements of connectivity were further correlated with clinical parameters of FM.
Results
Patients with FM reported more tender points and a higher total tenderness scores (TTS) than controls (both p < 0.001). Moreover, the insula-DMN connectivity between was disrupted in FM at theta (4–8 Hz) frequency (vs. controls: left, p = 0.007; right, p = 0.035). Notably, in FM, beta (13–25 Hz) connectivity between right insula and DMN was negatively correlated with the number of tender points and TTS (both p < 0.05); moreover, delta (2–4 Hz) insula-DMN connectivity was negatively correlated with scores of Symptom Severity and the revised fibromyalgia impact questionnaire (all p < 0.05).
Conclusion
FM is a functional brain disorder characterized by a “frequency-specific” connectivity alteration of pain-related cortical regions. Further studies in this network connectivity may help elucidate its potential as a brain signature and causal relationship with FM.
Disclosure of Interest
None Declared
Headache Pathophysiology - Imaging and Neurophysiology
PO-01-022
Brain Functional Connectivity Investigation of Patients with Migraine based on Complex Networks Analysis
Jiajun Yang1,*
1The Sixth People's Hospital Affiliated to Shanghai Jiao Tong University, Shanghai, China
Objectives
Using graph theory to construct the resting-state brain complex networks, the topological structure differences of the functional networks between the migraine patients group (MP) and the normal control group (NC) were investigated in this study.
Methods
We firstly acquired the resting-state functional magnetic resonance imaging dataset from 22 migraine patients and 22 normal subjects, respectively. Then, the functional complex networks of the two contrast groups were constructed, and some essential measures such as the average clustering coefficient, characteristic path length, small worldness, assortativity, and betweenness of these two groups were calculated, respectively. Lastly, two sample T test (P = 0.01) on these measures regarding to the two groups were performed to detect the differences statistically.
Results
Compared with NC, the average clustering coefficient of MP group is larger; the topology measures, i.e., small worldness and assortativity, are also changed; the characteristic path length of the nodes such as the caudate nucleus and putamen areas present abnormity; Betweenness centrality as to part of the regions, i.e., the thalamus, inferior occipital gyrus and occipital gyrus, demonstrates obvious increase.
Conclusion
The abnormal brain regions statistically occurred in MP group, were mainly associated with pain processing, visual processing and sensory information relay, which contribute to better understanding and interpretation of the related clinical condition of migraine.
Disclosure of Interest
None Declared
Headache Pathophysiology - Imaging and Neurophysiology
PO-01-023
High brain serotonin levels in migraine between attacks: A 5-HT4-receptor binding PET study
Marie Deen1,2,*, Hanne D. Hansen2, Anders Hougaard1, Hans Eiberg3, Szabolcs Lehel4, Messoud Ashina1,5 and Gitte M. Knudsen2,5
1Danish Headache Center, Department of Neurology, Rigshospitalet
2Neurobiology Research Unit and Center for Experimental Medicine Neuropharmacology, Department of Neurology, Rigshospitalet
3Department of Cellular and Molecular Medicine, Faculty of Health and Medical Sciences, University of Copenhagen
4PET- and Cyclotron Unit, Rigshospitalet
5Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark
Objectives
To investigate brain 5-HT4-receptor binding with positron emission tomography (PET) as a proxy of serotonin (5-hydroxytryptamine, 5-HT) levels in migraine patients between attacks.
Methods
Brain 5-HT4-receptor binding, assessed with PET imaging of the specific 5-HT4-receptor radioligand, [11C]SB207145, is inversely related to long-term changes in brain 5-HT-levels. Eighteen migraine patients without aura (≥48 hours migraine free) and 16 age- and sex-matched controls underwent PET-scanning after injection of [11C]SB207145. Patients who reported a migraine attack ≤48 hours after the scan were excluded. The mean neocortical [11C]SB207145 binding potential (BPND) was calculated in a blinded manner.
Results
Fifteen patients (age 29.6 ± 10.2 years, 2 men) and 16 controls (28.9 ± 10.2 years, 3 men) completed the study. Migraine patients had significantly lower neocortical 5-HT4-receptor binding than controls (0.62 ± 0.09 vs. 0.68 ± 0.05, p = 0.024). We found no associations between 5-HT4-receptor binding and clinical migraine characteristics.
Conclusion
Migraine patients have lower neocortical 5-HT4-receptor binding than controls, which may reflect a chronic or at least episodically high brain 5-HT-level. Our finding is in apparent contrast with the longstanding hypothesis of migraine being a syndrome of chronic low brain 5-HT-levels. We were unable to demonstrate any associations with attack frequency or years with migraine. This suggests that high brain 5-HT-levels may be a trait of the migraine brain rather than a consequence of migraine attacks.
Disclosure of Interest
M. Deen: None Declared, H. Hansen: None Declared, A. Hougaard: None Declared, H. Eiberg: None Declared, S. Lehel: None Declared, M. Ashina Conflict with: M. Ashina is a consultant or scientific advisor for Allergan, Amgen, Alder, ATI, Eli Lilly, Novartis and Teva, Conflict with: M. Ashina is a primary investigator for Amgen 20120178 (Phase 2), 20120295 (Phase 2), 20130255 (OLE), 20120297 (Phase 3) and GM-11 gamma-Core-R trials., G. Knudsen Conflict with: G. Knudsen has received honoraria as a consultant/speaker for H Lundbeck and Pfizer, and as a board member of Brain Prize and the Elsass Foundation. She is also on the advisory board for the Kristian G Jebsen Foundation.
Headache Pathophysiology - Imaging and Neurophysiology
PO-01-024
Altered thalamic network connectivity during spontaneous attacks of migraine without aura: a resting-state fMRI study
Faisal Mohammmad Amin1,*, Anders Hougaard1, Stefano Magon2, Till Sprenger3, Frauke Wolfram4, Egill Rostrup5 and Messoud Ashina1
1Danish Headache Center, Rigshospitalet Glostrup, Glostrup, Denmark
2Dept. of Neurology, and Medical Image Analysis Center, University Hospital, University of Basel, Basel, Switzerland
3Dept. of Neurology, DKD Helios Klinik Wiesbaden, Wiesbaden, Germany
4Dept. of Radiology
5Functional Imaging Unit, Dept. of Clinical Physiology, Nuclear Medicine and PET, Rigshospitalet, Glostrup, Denmark
Objectives
To investigate brain functional connectivity by the resting-state functional magnetic resonance imaging (rsfMRI) during spontaneous migraine attacks
Methods
Seventeen migraine without aura patients reported at the hospital for a resting-state functional MRI scan during and outside of a spontaneous migraine attack. Primary endpoint was a difference in functional connectivity between the attack and the headache-free days. Functional connectivity was assessed using seed-based analysis in the FMRIB Software Library. The chosen seeds were located in the thalamus (MNI coordinates x,y,z: right, 22,−24,0 and left, −22,−28,6).
Results
We found increased functional connectivity between the right thalamus and several contralateral brain regions (superior parietal lobule, insular cortex, primary motor cortex, supplementary motor area, orbitofrontal cortex and corticospinal tract). There was decreased functional connectivity between the right thalamus and three ipsilateral brain areas (primary somatosensory cortex, corpus collusom and premotor cortex). We found no change in functional connectivity in the pontine or the cerebellar networks.
Conclusion
The study indicates that network connectivity between thalamus and pain modulating as well as pain encoding cortical areas are affected during spontaneous migraine attacks. Thus, the incoming pain signals from the trigeminal afferents during a migraine attack may pass through thalamus without undergoing the normal control mechanisms.
Disclosure of Interest
F. M. Amin: None Declared, A. Hougaard: None Declared, S. Magon: None Declared, T. Sprenger Conflict with: Eli Lilly, Allergan, Actelion, ATI, Novartis, Genzyme, and Teva, F. Wolfram: None Declared, E. Rostrup: None Declared, M. Ashina Conflict with: Allergan, Amgen, Alder, ATI, and Eli Lilly, Conflict with: Amgen 20120178 (Phase 2), 20120295 (Phase 2), 20130255 (OLE), and 20120297 (Phase 3) trials
Headache Pathophysiology - Imaging and Neurophysiology
PO-01-025
Electroencephalogram spectral bicoherence on resting phase: a potential reliable electrophysiological biomarker for migraine
Delphine Magis1,2, François Gabrielli3, James A. Roberts4, Marco Lisicki2, Michael Breakspear4,5, Radhouane Dallel3,6, Kevin D'Ostilio2, Jean Schoenen1,7 and Lénaic Monconduit3,*
1Neurology, Centre Hospitalier Universitaire
2Headache Research Unit, Université de Liège, Liège, Belgium
3Neuro-Dol, Univ. Clermont Auvergne, Clermont-Ferrand, France
4Systems Neuroscience Group, Center for Integrative Brain Function, Herston
5Metro North Mental Health Service, Royal Brisbane and Women's Hospital, Brisbane, Australia
6Service d'Odontologie, CHU Clermont-Ferrand, Clermont-Ferrand, France
7Neurology, Université de Liège, Liège, Belgium
Objectives
Migraine is characterized by abnormal neuronal responsiveness1,2 and there is evidence that the brain could have neuronal networks' properties, hence resilience mechanisms, to avoid attacks3. Electroencephalography (EEG) has been widely used and processed to highlight those mechanisms, one of them being a synchrony between areas of the brain. In migraine, it had been shown previously that photic driving, ie the amplitude of the EEG response of the visual cortex to flicker stimuli above 20 Hz, was overall increased, mainly in preictal period. Whereas synchronization between brain areas has been investigated, phase lock within the same electrode has never been applied to EEG. We hypothesize that higher frequency content (beta) of EEG signal may be less “locked” to lower frequencies (alpha), leading to hyperresponsiveness. This study aims to evaluate the nonlinearities in EEG rhythms4 and the bicoherence of resting phase EEG in healthy volunteers and episodic migraine patients, towards the identification of a novel electrophysiological biomarker of the migrainous brain.
Methods
Twenty-five healthy volunteers (HV, 36.9 ± 14.2 y.o., 88% F) and 41 patients with episodic migraine without aura (ICHD 3 beta 1.1, MO, 33.6 ± 12.2 y.o., 83.6% F) participated to the study. Twenty-three patients were in interictal phase whereas 18 patients were in peri-ictal phase, based on the presence of an attack within 72 hours of the recording. All participants underwent a standard 20 channel EEG (Nicolet, NatusMedical) while resting with eyes closed. EEG data were preprocessed for epoch extraction and artifact rejection. Then bicoherence was calculated on each channel, and its maximum value extracted between 4 Hz and 16 Hz. Ranksum test was used on mean bicoherence over a selection of 5 electrodes between groups and between HV/MO. Classification procedure was based on a polynomial regression (3rd order) on logarithmic transformed bicoherence, trained with 85% of values, and tested with the 15% remaining, with 1000 random selections of training/testing.
Results
Mean bicoherence was significantly lower (p = 0.0035) in migraine patients (0.249 ± 0.093) compared to HV (0.345 ± 0.136) but not significantly different between peri-ictal and interictal subgroups (p = 0.76). Bicoherence values successfully sorted out 71% of individuals in both MO and HV groups. Lower bicoherence in MO patients mirrored a deficit of synchronization between alpha band and its double frequency. This diminution of synchronization was able to successfully sort out patients, and could contribute to the subsequent photic driving observed in the literature.
Conclusion
This study suggests that spectral bicoherence of the electroencephalogram on resting phase is lower in migraineurs, whatever the migraine phase, and may be an additional interesting electrophysiological biomarker for migraine, besides the habituation of evoked potentials. More studies are warranted to confirm and disentangle this finding, and explore its pathophysiological significance.
References
1 Magis et al., 2007. Cephalalgia
2 Magis, et al., 2016. Curr Opinion Neurol
3 Mendon de Souza et al., 2012. Front. Hum. Neurosci
4 Pradhan et al., 2012. Comput. and math. Meth. in med
Disclosure of Interest
D. Magis: None Declared, F. Gabrielli: None Declared, J. Roberts: None Declared, M. Lisicki: None Declared, M. Breakspear: None Declared, R. Dallel: None Declared, K. D'Ostilio: None Declared, J. Schoenen Conflict with: Cefaly Technology, L. Monconduit: None Declared
Headache Pathophysiology - Imaging and Neurophysiology
PO-01-026
Changes of Autoregulation of Cerebral Circulation in Patients with Chronic Tension-Type Headache
Iuliia Iakubenko1,*, Tetyana Litovchenko1, Bogdan Fedak2 and Oleg Chub3
1Department of Neurology and Child Neurology, Kharkiv Medical Academy of Postgraduate Education
2Regional Clinical Hospital - Center of Emergency Medical Care and Disaster Medicine
3Institute for Problems of Cryobiology and Cryomedicine of the National Academy of Sciences of Ukraine, Kharkiv, Ukraine
Objectives
The purpose of our study was to investigate the hemodynamic disturbances and changes of adaptation possibilities of cerebral vessels in patients with chronic tension-type headache.
Methods
We have examined 23 patients with chronic tension-type headache (CTTH). To evaluate the patients’ hemodynamics we took into consideration the indicators of linear velocity of blood flow (LVF) and indicators of reactivity of vessels in the system of the common carotid arteries. We obtained these data by using the method of Doppler ultrasonography with compression tests.
Results
It was detected that in the patients with CTTH all hemodynamic indicators before compression tests did not differ from healthy subjects. However, in the compression of carotid arteries the elevation of LVF to 49.2% was detected in the state of peace (to 38.4% in the control group, respectively). Postcompression evaluation of LVB was in average 28.2% in compression to the primary level of LVF, wich had been measure before compression (47.2% in the control group, respectively). According to the indicators of changes of LVF in common arteries, the CO was 1.15 ± 0.01 (p < 0.01) and FA was 0.68 ± 0.02, respectively (p < 0.01), in the group of patients with chronic headaches of tension. Even with the minimum of compression time was observed paradoxical reaction of cerebral vessels.
Conclusion
In our opinion, these changes are the results of duration of chronic distress and compensatory muscle spasm which determine the type of headaches in combination with a vessels component.
Disclosure of Interest
None Declared
Headache Pathophysiology - Imaging and Neurophysiology
PO-01-027
Cognitive function performance of migraine in auditory evented-related potential and functional magnetic resonance imaging
Shih C. Sen1,*, Liu C. Ju2 and Wu M. Ting3
1Department of Neurology, Kaohsiung Veterans General Hospital
2Science Education & Enviromental Education, National Kaohsiung Normal University
3Department of Radiology, Kaohsiung Veterans General Hospital, Taiwan, Republic of China, Kaohsiung, Taiwan, Republic of China
Objectives
Migraine is a common and painful condition that affects many people, predominantly from young adulthood to middle age; the years of maximum work and family commitments. Although treatment guidelines were proposed for acute and preventive treatment of migraine, the pathogenesis of migraine was still uncertain. Recent studies showed learning disabilities and attention deficit disorder in children and adolescents with migraine were also noted and adult migraine patients often report cognitive complaints, especially regarding attention and memory. Cognitive function change in migraine patients was highly suspected. Because the migraine without aura (MoA) patients are more common, we selected MoA patients as experimental group. We hope to compare the difference of brain physiologic & cognitive function change between MoA patients and normal people by these non-invasive electrophysiologic & neuroimaging techniques [auditory event-related potential (ERP) and functional magnetic resonance imaging (fMRI)] and cognitive assessments [Mini-Mental State Examination (MMSE) and Wechsler Memory Scale-Third Edition (WES-III)]. This study showed some cognitive impairment in cognitive assessments, especial over recall memory and working memory. These cognitive changes could be compatible with some findings in electrophysiologic & neuroimaging techniques.
Methods
Nineteen migraine subjects (M/F = 5/14, age = 42 ± 10 y/o) and thirteen healthy controls (M/F =5/8, age = 32 ± 9 y/o) who had no history of neurological disease participated in this study. All participants received MMSE (Folstein et al., 1975) & WES-III (Larrabee, 1999) mental tests and auditory ERP & fMRI examinations. The auditory ERP and fMRI examination were performed during the ictal phase of the MoA patients. We used an auditory oddball paradigm to analyze target processing using event-related potentials and measured latency and amplitude of P300 target stimulus in P3, Pz and P4 three sites. We also compared the functional connectivity in resting-state fMRI (rsfMRI) between controls and MoA patients and analyzed the data according to Stanford University laboratory. All imaging data were acquired from a 3.0T MR scanner (Skyra, Siemens, Erlangen, Germany).
Results
Our results showed MoA patients have some cognitive impairment in the total score & recall score in MMSE and index scores & percentiles of working memory in WMS-III. More prolonged distal latency and reduced amplitude P300 target stimulus in the MoA patients. There was decreased functional connectivity in rsfMRI in basal ganglion, higher visual and primary visual networks of MoA patients.
Conclusion
These results suggested that patients with migraine might present higher risk of cognitive impairment and the auditory ERP & rsfMRI data provided an evidence of the cognitive dysfunction in these patients.
Disclosure of Interest
None Declared
Headache Pathophysiology - Imaging and Neurophysiology
PO-01-028
The ventilatory threshold is associated with migraine attacks after maximal exercise test in women with episodic migraine
Arão B. Oliveira1,*, Reinaldo T. Ribeiro1, Marco T. Mello2 and Mario F. P. Peres3
1Neurology and Neurosurgery, UNIFESP, São Paulo
2Sports Sciences, UFMG, Belo Horizonte
3Brain Institute, Albert Einstein Israeli Hospital, São Paulo, Brazil
Objectives
To test the association between cardiorespiratory fitness and migraine attacks following a maximal exercise test in women with episodic migraine.
Methods
Patients with episodic migraine (ICHD-III), and no history of exercise-triggered attacks, were recruited from São Paulo Hospital and/or local community. Patients underwent a maximal cardiopulmonary exercise test on treadmill for determination of peak oxygen uptake (VO2peak), a gold-standard measure of cardiorespiratory fitness, and the ventilatory threshold (VO2VT), a cardiometabolic parameter of anaerobic metabolism and early fatigue. Patients’ cardiorespiratory fitness were categorized as “above fair”/”below fair” categories of the sex- and age-predicted classification of the American College of Sports Medicine for VO2peak, or alternatively, “above”/”below” group’s median for VO2VT. Headaches diaries were tracked for the 72 h after the exercise test, and occurrence of attacks were categorized as “<6 h”, “12 h−24 h”, “24 h−48 h”, “48 h−72 h”, and “No attack”, or “Yes/No”, for having attacks within the 72 h-period. Participants whose attacks were attributed to others triggers were excluded from analyses. UNIFESP’s Research Ethic Committee approved the study's protocol, and all participants gave signed informed consent.
Results
Twenty-one patients (mean ± SD age: 35.4 ± 11.6 years, BMI: 26.4 ± 5) were included in the analyses. Sixty-seven percent (14/21) of patients had attacks within the 72 h-period. The majority of patients having attacks within the 72 h-period experienced them <6 h after maximal exercise test (38.1%). Most patients (62%) were within the cardiorespiratory fitness category “below fair” for VO2peak. There were no association between cardiorespiratory fitness for VO2peak and whether patients had or not attacks within the 72 h-period [χ2(2) = 1.875, p = 0.39]. However, there was an association between cardiorespiratory fitness related to the VO2VT and whether patients had or not attacks within the 72 h-period [χ2(2) = 8.472, p = 0.014], indicating that patients with below-medium VO2VT values were more likely to experience a migraine attack after maximal exercise test.
Conclusion
Cardiorespiratory fitness, specifically related to lower ventilatory threshold, is associated with migraine attacks after maximal exercise.
Disclosure of Interest
None Declared
Headache Pathophysiology - Imaging and Neurophysiology
PO-01-029
Peripheral vagal nerve stimulation modulates the nociceptive withdrawal reflex in healthy subjects: a cross-over placebo-controlled study
Roberto De Icco1,*, Daniele Martinelli1, Eric Liebler2, Marta Allena3, Vito Bitetto1, Grazia Sances3, Giorgio Sandrini1, Giuseppe Nappi3 and Cristina Tassorelli1
1Dept. of Brain and Behavioral Sciences, Headache Science Center, C. Mondino National Neurological Institute, Pavia, Italy
2electroCore LLC, Basking Ridge, NJ, United States
3Headache Science Center, C. Mondino National Neurological Institute, Pavia, Italy
Objectives
Peripheral non-invasive vagal nerve stimulation (nVNS) has become a target for the treatment of primary headaches, though its exact mechanisms are unclear. Different studies showed that nVNS modulates both spinal and supra-spinal nociceptive pathways in an inhibitory direction. The nociceptive flexion reflex paradigm is widely used to investigate modulation of nociception and represents a reliable objective measure of the functional activation of the nociceptive network. The aim of our study is to evaluate the effect of nVNS on the nociceptive withdrawal reflex in healthy subjects.
Methods
We enrolled 10 healthy subjects (5 males, age 26.5 ± 2.2 years) in a cross-over placebo-controlled study. Subjects were randomly assigned to: 1) nVNS: one 120-s electrical stimulation on each side of the neck using the gammaCore nVNS device and b) active sham stimulation (SHAM): one 120-s electrical stimulation of the median nerve on each wrist using the same nVNS device. Nociceptive withdrawal reflex was evaluated in the right lower limb according to a standardized paradigm: electrical stimulation delivered at the sural nerve and electromyographic muscular response recorded from the ipsilateral biceps femoris. The reflex threshold following a single stimulus (RT-SS) was the lowest intensity (mA) needed to elicit a stable muscular response. The temporal summation of the nociceptive flexion reflex (RT-TS) was evaluated using a train of 5 stimuli at a frequency of 2 Hz. The other parameters recorded were the area under the curve, the latency of the reflex, and the Visual Analogue Scale (VAS) at RT-SS. Nociceptive withdrawal reflex was investigated at baseline (T0), 5’ minute after stimulation (T5) and 30’ after stimulation (T30).
Results
At T0 the neurophysiological parameters were comparable between groups. In particular RT-SS was 13.86 ± 3.67 and 16.15 ± 3.53 in nVNS and SHAM groups, respectively (p = 0.086), while RT-TS was 11.0 ±2.79 in nVNS group and 12.64 ± 3.67 in SHAM group (p = 0.107).
nVNS caused a significant increase in the RT-SS at T5 (+14.5% ± 4.2, p = 0.023) and T30 (+25.9% ± 6.6, p = 0.011). Also RT-TS increased following nVSN at T5, but statistical significance was only reached at T30 (+21.7 ± 6.7, p = 0.031). SHAM stimulation did not induce any significant modification on the reflex parameters. When comparing groups, we found that the percentage increase of RT-SS at T5 and T30 was significantly higher in nVNS vs. SHAM (p = 0.008 and p = 0.007 respectively). Accordingly the percentage increase of RT-TS at T30 was significantly higher in the nVNS arm vs. SHAM (p = 0.013). We did not observe any significant modification of the other parameters in either group.
Conclusion
Using a consolidated neurophysiological methodology, we have demonstrated that nVNS induces a rapid onset of analgesia in healthy subjects. Because of its neurophysiological signatures, this analgesic activity is likely related to the inhibition of pain facilitation mechanisms occurring at the spinal and/or supra-spinal level. The mechanistic bases of this activity are yet to be elucidated, but the present observation provides additional evidence for the role of nVNS in the acute and prophylactic treatment of primary headaches.
Disclosure of Interest
R. De Icco: None Declared, D. Martinelli: None Declared, E. Liebler Conflict with: electroCore LLC, M. Allena: None Declared, V. Bitetto: None Declared, G. Sances: None Declared, G. Sandrini: None Declared, G. Nappi: None Declared, C. Tassorelli: None Declared
Headache Pathophysiology - Imaging and Neurophysiology
PO-01-030
Processing of mechanical and nociceptive trigeminal input at brainstem-level – an fMRI-study
Maike Moeller1,*, Jan Mehnert1, Jan Hoffmann1 and Arne May1
1Dept. of Systems Neuroscience, University Medical Center Hamburg-Eppendorf (UKE), Hamburg, Germany
Objectives
The trigemino-autonomic reflex is a physiological response to trigeminal nociceptive input leading to parasympathetic outflow. The afferent limb of this reflex arc consists of the trigeminal nerve, and the efferent limb comprises the facial/greater superficial petrosal nerve (parasympathetic) dilator pathway. Autonomic symptoms play an important role in cluster headache (CH) and are a hallmark in trigeminal autonomic cephalalgias (TACs). The brainstem plays a major role in processing and the modulation of trigeminal input during attacks of various primary headaches. The question arises which brain regions are involved in processing different types of trigeminal input, generating cranial autonomic output. Therefore we investigated the neural correlates of processing mechanical input into the trigeminal system, using a new stimulation method combined with a well-established brainstem functional magnetic resonance imaging (fMRI-) protocol.
Methods
Kinetic oscillation stimulation (KOS) of the nasal mucosa generates predominantly ipsilateral autonomic symptoms among which lacrimation is quantitatively measurable. The KOS-paradigm was applied to 31 healthy volunteers (12 f, 19 m). For the stimulation-procedure an inflatable catheter was placed into the left nostril, which oscillated during stimulation (85 Hz/80 mbar). Each of the 21 trials consisted of 30 s of stimulation interleaved with resting periods of 90 s duration (jittered +/−10 s). After each trial pain perception and unpleasantness were assessed by a visual analogue scale (VAS). Altogether 23 participants, perceiving no or only moderate pain during the experiment, were included in the General Linear Model based fMRI-analysis. We controlled for physiological noise including pulse, respiration, movement and flow of cerebrospinal fluid (CSF).
Results
Lacrimation was significantly generated during stimulation. The fMRI-analysis showed stronger activation (p < 0.001 unc; minimum cluster extent of 10 voxel) during stimulation compared to rest within the brainstem, the thalamus and bilateral insular cortices. Left and right amygdala as well as the hippocampus were stronger activated during rest compared to stimulation. Some volunteers reported moderate pain for some trials. For pain-trials we observed increased activations in the brainstem, the thalamus, putamen, bilateral insula and in the frontal operculum compared to non-pain trials.
Conclusion
Various brain regions including the brainstem, insula and the thalamus become activated during processing of a non-painful input into the trigeminal system and the generation of parasympathetic output. Furthermore, we observed that processing at brainstem-level of a mechanical input into the trigeminal system differs from processing of a nociceptive input. These findings contribute to the physiological insights of the trigemino-autonomic reflex arc that plays a crucial role in TACs.
Disclosure of Interest
None Declared
Headache Pathophysiology - Imaging and Neurophysiology
PO-01-031
No association between migraine frequency and brain lesions: a study in a series of chronic migraine women
Angela Meilan1, Davinia Larrosa2, Cesar Ramon2, Antonio Saiz1, Pablo Martínez-Camblor3, Elena Santamarta1 and Julio Pascual4,*
1Radiology
2Neurology, University Hospital Central de Asturias, Oviedo, Spain
3Biomedical Data Science, Geisel School of Medicine, Dartmouth, United States
4Neurology, University Hospital Marqués de Valdecilla, Santander, Spain
Objectives
Several 1.5 T MRI studies suggest that silent infarctions (SI) and hyperintense white matter lesions (WML) are more frequent in migraineurs with a high frequency of attacks. Our aim was to study their prevalence in chronic migraine (CM).
Methods
A total of 96 CM women, and as controls 29 episodic migraine (EM) women, underwent a 1.5 T MRI following the CAMERA protocol. Images were evaluated independently by two expert radiologists who were blind to the diagnosis.
Results
WML were found in 59 (61.5%) of CM and in 17 (58.6%) of EM patients. The majority (63% for CM and 71% for EM) were located in the deep white matter. Exclusive periventricular location was exceptional (2 CM cases and none EM). Regarding deep WML, the average was 7.7 (limits 0–177) in CM and 3.2 (0–27) in EM (p = NS), most of of small size. Of the 739 WML found in CM patients, 734 (99.3%) were hemispheric and among these frontal lesions were the most common (81%). Posterior fossa WML were seen, always in the pons, in 5 (0.7%) CM and in 2 (2.1%) EM women. Age >45 was the only vascular risk factor (VRF) correlating with a higher number of WML. We found 7 SI in 6 CM women (6.3%); 4 in the basilar territory with only one in the cerebellum. At least 2 VRFs were seen in 5 of these 6 CM patients.
Conclusion
This study confirms that the prevalence of WML, in most cases small, deep and in the anterior hemisphere, is increased both in CM and EM (61.5% and 58.6% vs. the 10% expected in the population at this age) and does not support an association of such lesions or SI with a higher frequency of attacks, but with the presence of FVRs and mainly age >45.
(Supported by PI14/00020 FISSS grant)
Disclosure of Interest
None Declared
Headache Pathophysiology - Imaging and Neurophysiology
PO-01-032
Multi-frequency Analysis of Neuromagnetic Activity between Eyes-Open and Eyes-Closed at Resting States in Migraine
Yuying Fan1,2,*, Kun Yang3 and Jing Xiang2
1Department of Pediatrics, Shengjing Hospital of China Medical University, Shenyang, China
2Department of Pediatrics, Cincinnati Children’s Hospital, Cincinnati, United States
3Department of Neurosurgery, Nanjing Brain Hospital, Nanjing, China
Objectives
The objective of the present study was to characterize the differences of neuromagnetic brain activities from low to high frequency ranges between eyes-open and eyes-closed at resting states in migraine.
Methods
We investigated 24 subjects suffering from migraine and 24 age-matched and gender-matched healthy controls using a magnetoencephalography (MEG) system, recording at a sampling rate of 6000 Hz. Subjects were asked to keep eyes-open for 2 minutes and eye-closed for 2 minutes. Source activities were localized with accumulated source imaging method in nine frequency bands, which included delta(1–4 Hz), theta(4–8 Hz), alpha (8–12 Hz), beta (12–30 Hz), low–gamma(30–55 Hz), high–gamma (65–90 Hz), ripple (90–200 Hz), high-frequency oscillations (HFOs, 200–1,000 Hz) and very high-frequency oscillations (VHFOs, 1,000–2,000 Hz). Magnetic source power was quantified for each group.
Results
Compared with eyes-open, eyes-closed was associated with significant increases of alpha (8–12 Hz) and beta (12–30 Hz) activities, and was also associated with significant decreases of delta (1–4 Hz), theta (4–8 Hz), low-gamma (30–55 Hz) and high-gamma (65–90 Hz) in both the migraine and control groups.
Compared with eyes-closed, eyes-open was associated with significant increases of source power in ripples (90–200 Hz), HFOs (200–1,000 Hz) and VHFOs (1,000–2,000 Hz) in the migraine group, but not in the control group.
Conclusion
The results demonstrated that migraine subjects had altered brain activities in multiple frequency bands during eyes-open and eyes-closed states as compared with controls. The significant increases of high frequency brain activities at eyes-open status in migraine might be related to migraine headache attacks, which could explain why some migraine subjects like to stay in a dark place to keep eyes-closed. Though the underlying mechanisms remain unknown, it might be associated with an aberrant visual processing or aberrant resting state activation. The findings may facilitate the development of new therapeutic strategies in migraine treatment in the future.
Disclosure of Interest
None Declared
Headache Pathophysiology - Imaging and Neurophysiology
PO-01-033
Functional MRI of Headache
Shengyuan Yu1,*, Zhiye Chen1, Enchao Qiu1 and Xiaoyan Chen1
1Chinese PLA General Hospital (301 Hospital), Beijing, China
Objectives
Primary headache is a common complaint of general population. Both cluster headache (CH) and migraine are considered as disabling primary neurovascular headache disorders which are severe and moderate to severe in intensity accompanied by autonomic symptoms. The pathogenesis of these disorders is not well understood.
Methods
Functional MRI plays an important role in revealing headache mechanism. In our studies, the resting-state fMRI was used to investigate the altered functional connectivity in patients of disabling primary headache including CH, episodic migraine (EM), chronic migraine (CM), and medication overuse headache (MOH) so that to reveal possible pathogenesis of these disorders.
Results
Our results demonstrate that decreased functional coactivation was detected between bilateral hypothalamus and the salience network (SN) in CH patients of either side headache, altered functional connectivity architecture of marginal division of neostriatum and amygdala in EM, CM and MOH patients.
Conclusion
These results suggest that abnormal hypothalamus–SN coactivation may have a role in CH attacks, and altered functional connectivity of affective emotional processing and cognitive processing network may play an important role in development of migraine chronicization.
Disclosure of Interest
None Declared
Headache Pathophysiology - Imaging and Neurophysiology
PO-01-034
MRI does not identify any abnormality in the local where the myofascial trigger points are palpable
Daniella A. Oliveira1,*, Mariana Luiza D. S. Queiroz2, Paula Rejane B. Diniz2, Debora Wanderley2, Eolo S. de Albuquerque Filho3 and Marcelo M. Valença2
1Physical Therapy
2Neuropsychiatry
3Clinical Hospital, Federal University of Pernambuco, Recife, Brazil
Objectives
To identify the presence of myofascial trigger points in the descending trapezius muscles by MRI.
Methods
A cross-sectional analytic study was conducted among 14 women aged between 18 and 28 years (23 ± 1ys), divided into two groups (8 migranous and 6 control without headache) carried out between December 2013 and November 2014. The study was approved by the Research Ethics Committee of the Health Sciences Center of the Federal University of Pernambuco (CAAE 23792613.0.0000.5208). The patients underwent a neurological examination for diagnosis of migraine according to ICHD III, beta version. The presence of myofascial trigger points was performed using the Simons' criteria and subsequently the areas were marked by linolenic acid capsules. MRI was performed with 1.5 T, T1-weighted sequence and T2 in the axial, sagittal and coronal planes. Gadolinium contrast was used.
Results
The MRI did not show any signal of alterations in the myofascial trigger points area.
Conclusion
The results of previous work show alterations of signals in the areas with trigger points using MRI (Landgraf et al., 2015) as well as in ultrasound imaging (Sikdar et al., 2009). In contrast, in our study MRI did not identify any abnormalities at the sites where the trigger points were palpated.
Disclosure of Interest
None Declared
Migraine Acute Therapy
PO-01-035
A prospective, randomized, single blind, parallel-group, placebo controlled clinical study to evaluate the short-term effectiveness of combined occipital and supraorbital transcutaneous nerve stimulation (OS-TNS) in treating migraine
Rachel Hering-Hanit1,*
1Neurology, Meir General Hospital, Kfar Sava, Israel
Objectives
Combined occipital and supraorbital nerve stimulation (OS-TNS) has previously shown promising results in treating migraine, but this intervention was only available with implanted systems. This study is the first to assess the safety and efficacy of a non-invasive OS-TNS device for acute treatment of migraine.
Methods
We undertook a randomized, single-blind, parallel-group, sham-controlled study at the headache clinic of “Meir” general hospital in Israel. Forty (40) adults suffering from episodic migraine, aged 21–62 years, were enrolled. All individuals met the international criteria for migraine. Subjects were randomly allocated keeping 1:1 ratio to receive active (N = 20) or sham occipital and supraorbital stimulation (N = 20) for 45 minutes. Treatment initiated at no more than 90 minutes after the onset of the migraine episode. Ten (10) subjects were excluded from the trial due to protocol exclusion criteria or inability to coordinate an intervention meeting. The primary endpoint was defined based on relative change (%) in VAS pain score from baseline to end of treatment without using pain medication.
Image:

Results
30 patients treated one acute migraine episode with active OS-TNS device (N = 15) or sham OS-TNS device (N = 15). At the end of treatment there was a significant reduction of the average Pain VAS score in the treatment group vs. an increase in Pain VAS score in the control group (−79.2% vs. +14.9%, respectively; P = 0.0002). Pain-free response rates significantly favored the active OS-TNS device at 2 hours (P = 0.0031) and at 24 hours (P < 0.05) post treatment. Superiority of the OS-TNS device was also shown for functional disability (P = 0.0004) and photophobia (P = 0.002). No device-related serious adverse events were recorded.
Conclusion
The results of this study demonstrate that combined occipital and supraorbital transcutaneous nerve stimulation (OS-TNS) is a safe and highly effective abortive treatment of episodic migraine and may serve as a superior, fast acting, adverse effects free alternative to medications.
Disclosure of Interest
None Declared
Migraine Acute Therapy
PO-01-036
Acute Therapy against Migraine with Kanpo Medicine (Japanese Traditional Medicine, derived from natural hurbs)
Tadashi Matsuda1,*
1Family Medicine, Misato Family Clinic, Misato-shi, Saitama, Japan
Objectives
Goreisan (Poria Powder with Five Herbs; GR) and Goshuyuto (Evodia Decoction; GS) are well-known Kanpo medicine against migraine. Kanpo medicine has been derived from natural herbs, so we can apply to any kinds of patients, such as children, adolescents, pregnant women, breast-feeding mothers, elderly patients, and even dialysis patients as well. On the other hand, it is difficult for general practitioners to decide which Kanpo medicine would be suitable for each migraine, besides effectiveness of single dosage of GR or GS alone has been reported around 50%. We have investigated effectiveness of combination therapy of GR and GS for acute splitting headache.
Methods
Subjects are patients with acute splitting headache who had visited our clinic in 2015. Cases having focal signs, meningeal signs, frequent vomiting, or high fever were excluded, therefore 139 patients were eligible for this study. Subject age; 5 y. o. −75 y. o. (31.8 ± 17.6 y. o. median 33). Female/male = 106/33. All patients were given orally GR and GS simultaneously. Numerical Rating Score (NRS) of each headache had been obtained 10 minutes after intervention.
Results
GR and GS have shown effective in 119 patients (85.6%) within 10 minutes. NRS 0–3/10; 58 cases. NRS 4–5/10; 47 cases. NRS 6–8/10; 14 cases, who had given another GR and GS 15 minutes later after first intervention, subsequently all NRS of this group had dropped below 3/10 after second intervention.
Cases of non-responders (n = 20); Dissection of left vertebral artery found by MRA. Brain tumor found by MRI. 2 cases of Sinusitis found by MRI or CT. Cervical disc herniation found by a plastic surgeon. 6 cases of mental disorders. 7 cases of idiopathic. As to residual 2 cases, one was effective to triptan, the other was effective to second intervention with GR and GS despite of first intervention failure.
Conclusion
Combination therapy of GR and GS is mostly effective against primary headache. This method could triage secondary headache for all generation safely and quickly, suggesting could be very useful for general practitioners but also emergency physicians.
Disclosure of Interest
None Declared
Migraine Acute Therapy
PO-01-037
Emergency care of migraine at a community hospital in Japan
Tatsuya Monzen1,*, Masahiro Ebitani1, Futoshi Saito2 and Fumihiko Sakai3
1Neurology
2Neurosurgery, ota memorial hospital, ota
3Saitama Neuropsychiatric Institute, Saitama, Japan
Objectives
Fifteen years have passed since we became able to use triptan for treating migraine. Subcutaneous injection of sumatriptan is recommended for acute medical treatment of migraine. We give subcutaneous injections of sumatriptan for patients who visit emergency department with severe migraine on holidays or during nighttime. But it is often difficult to make correct diagnosis of migraine at the emergency room by physicians who are not used to diagnosing migraine. In our hospital, emergency medical care of headache patients is conducted by rotating physicians from neurology, neurosurgery and emergency department. In this study, we analyzed patients with migraine who received sumatriptan by subcutaneous injection at our emergency clinic.
Methods
Ota Memorial Hospital is a core hospital accepting emergency patients all day from a medical area with a population of 400,000. In this retrospective study, patients with headache who visited emergency room were extracted from the electronic medical record system during the year of 2016 (January to December). We collected the record of patients with severe migraine who received diagnosis of migraine and received sumatriptan injection. Emergency headache care was performed by mostly by physicians who are not headache specialist. We asked patients if they had visited primary care physicians for their headache before visiting emergency room. We followed the prognosis of patients who were diagnosed as migraine and received injections of sumatriptan for the first time in life at the emergency clinic.
Results
A total of 608 patients visited our emergency room with headache. Subarachnoid hemorrhage (SAH) was 63 (10.4%), migraine 42 (7.0%), meningitis/encephalitis 21 (3.5%), shingles 1, neuralgia 4, headache other than migraine 106 (17.4%) and head injury (head bruise) 372 received emergency medical care at our hospital. Thirty-seven patients with severe migraine, 4 men and 34 women with the mean age of 36.1 years received the diagnosis of migraine by physicians of emergency room. All the patients with severe migraine received subcutaneous injection of sumatriptan. Nineteen patients were diagnosed by neurologist, 11 patients were diagnosed by neurosurgeon, and 7 patients were diagnosed and treated by emergency department physicians. Except for 2 patients, 42 migraine patients had headache improved with sumatriptan subcutaneous injection and returned home. Among patients with migraine, 21 patients visited the emergency room between 5 pm and 0 am. Nine patients visited between 0 am and 9 am. Eight patients visited on Saturdays and holidays. Nine patients came by ambulance. Fifty-nine percent of patients with severe migraine had never visited physician for headache and never diagnosed as migraine before their emergency room visit. Eighty-four percent of patients with severe migraine had no family doctor and had not received medical treatment for headache.
Conclusion
Most of the patients who visited our emergency clinic for severe headache had never consulted primary care physicians for headache before. Diagnosis of such patient was not only SAH (10.4%), but also migraine (as much as 7% of all the headaches at emergency clinic). Making diagnosis of migraine and treating by the injection of sumatriptan were performed properly. We re-realized the importance of headache care at the emergency practice. It is particularly important to educate rotating physicians to the emergency clinic about emergency migraine care.
Our study also emphasized the importance of educating patients to consult primary care physicians for headache. Patient should be able to tell the diagnosis of migraine to the physicians of emergency clinic, which will make the emergency headache care more efficient. Our study promoted our community to establish a patient referral system.
Disclosure of Interest
None Declared
Migraine Acute Therapy
PO-01-038
Opioid Use is Related to Headache Frequency and Severity at Follow-Up in Patients with Intractable Migraine
Brad Torphy1,* and Joseph Babione2
1Diamond Headache Clinic
2Illinois School of Professional Psychology, Chicago, United States
Objectives
Negative consequences of the overuse of opioids in headache can often include dependence, treatment interference, and the development of medication overuse headache. In addition, some evidence has suggested that opioid use may be related to poorer long-term outcomes in headache sufferers. To further explore this, we examined the relationship between opioid use and headache outcomes in patients with intractable migraine.
The aim of this study was to examine the relationship between opioid use and headache frequency and severity over time in patients with intractable migraine.
Methods
The initial sample at baseline assessment included 49 adults presenting to an outpatient specialty headache clinic who reported having experienced headache pain every day within the past month and reported taking opioids on 10 or more days per month for at least three months. At baseline patients were advised to refrain from using opioid medication and adhere to treatment as usual. At three subsequent follow-up points (i.e., 1–3 months; 3–4 months; 6–8 months) current opioid use, headache frequency (i.e., number of headache days within the past month) and severity (i.e., number of headache days with severe pain) were assessed via patient self-report.
Results
At the time of the first follow-up, data was available from 35 patients who had not continued to take opioid medications and 10 patients who had continued to do so. We conducted several independent sample t-tests to examine differences in headache frequency and severity between patients who refrained from opioid use (Opioid−) and those who continued taking opioids (Opioid+) for each follow-up time. Results showed that the Opioid− group reported significantly fewer headache days at all three follow-up visits than the Opioid+ group (i.e., Time 1, p < .01; Time 2, p < .05; Time 3, p < .01). Within the number of total headache days for each group, further analyses showed that the Opioid- group reported significantly fewer headache days that were identified as severe than the Opioid+ group at all three follow-up visits (i.e., Time 1, p < .01; Time 2, p < .01; Time 3, p < .01).
Conclusion
These results provide preliminary support that continued opioid use in patients with intractable migraine may be associated with poorer outcomes (i.e., greater headache frequency and severity) than those who discontinue opioid use and adhere to treatment as usual. Future research in this area will benefit from a larger sample size to corroborate these findings. In addition, extraneous factors related to outcome in headache sufferers should be addressed.
Disclosure of Interest
B. Torphy Conflict with: Avanir Pharmaceuticals, J. Babione: None Declared
Migraine Acute Therapy
PO-01-039
Characterization of several adenosine A2A receptor antagonists using an in vivo pharmacological model of migraine
Alejandro Labastida-Ramírez1,*, Kayi Y. Chan1, Kristian A. Haanes1, Rene de Vries1, Brian Shook2, Paul F. Jackson2, Jimmy Zhang2, Christopher M. Flores2, Carlos M. Villalón3 and Antoinette MaassenVanDenBrink1
1Department of Internal Medicine, Division of Vascular Medicine and Pharmacology, Erasmus University Medical Center, Rotterdam, Netherlands
2Janssen Research & Development, L.L.C., Philadelphia, United States
3Pharmacobiology, Cinvestav-IPN, Unidad Sur, Mexico City, Mexico
Objectives
Migraine pathophysiology is associated with activation of the trigeminovascular system and cranial vasodilatation. Adenosine is a potent cerebral vasodilator (through A2A receptors) that increases in plasma during migraine attacks. Blockade of this receptor could represent a new antimigraine target. The present study investigated the role of five adenosine A2A receptor antagonists in relation to neurogenic sensorial vasodilatation.
Methods
A rat closed cranial window was used to study in vivo vasodilatation of the middle meningeal artery in response to exogenous CGS21680 (A2A agonist) or endogenous CGRP (released by periarterial electrical stimulation), in the absence or presence of one of five A2A receptor antagonists JNJ6008A, JNJ1014A, JNJ3791A, JNJ8446A or JNJ5848A (0.3–10 mg/kg) with varying selectivity over the A1 receptor. Experiments were approved by the Erasmus University Medical Center’s institutional ethics committee, in accordance with National Institute of Health guidelines.
Results
All antagonists tested blocked the in vivo vasodilatation of the middle meningeal artery in response to CGS21680, with the highest potency observed for the antagonists that also display affinity for the A1 receptor. The antagonists did not affect vasodilatation induced by periarterial electrical stimulation.
Conclusion
Whereas the antagonists were effective in blocking A2A and, in certain cases, A1 receptors, as illustrated by the blockade of relaxations to CGS21680, A2A receptors do not appear to be involved in neurogenic sensory CGRP release induced by perivascular electrical stimulation. The therapeutic potential of adenosine receptor antagonists in migraine remains to be determined in clinical trials.
Disclosure of Interest
A. Labastida-Ramírez: None Declared, K. Chan: None Declared, K. Haanes: None Declared, R. de Vries: None Declared, B. Shook Conflict with: Employee Janssen Research & Development, L.L.C, P. Jackson Conflict with: Employee Janssen Research & Development, L.L.C, J. Zhang Conflict with: Employee Janssen Research & Development, L.L.C, C. Flores Conflict with: Employee Janssen Research & Development, L.L.C, C. Villalón: None Declared, A. MaassenVanDenBrink Conflict with: Research support from Janssen
Migraine Acute Therapy
PO-01-040
Comparative study on efficacy of a triptan agent alone and combination with anti-epileptic drugs for migraine seizure
Toshihiko Shimizu1,* and Ichiro Arakawa2
1Neurosurgery, Tokyo Women's Medical University
2Pharmaceutical Science, Teikyo Heisei University, Tokyo, Japan
Objectives
Although the guideline recommends administration of no-steroid inflammatory drugs (NSADAs) with a triptan agent at the same time, it was concerned that initiation of gastric ulcer and bronchitis asthma due to use of NSAIDs.
Many cases of serious non-responders to triptan agents in migraine seizures, which inhibits release of neuro-inflammatory protein from trigeminal nerve existed around cerebrovascular and abnormal extension of cerebrovascular, has potentially existed cephalic hypersensitive condition during migraine seizures. For these cases, regular use of anti-epileptic drug(s) as prophylactic medication with onset use of the triptan agent is common for the migraine seizures.
However, effect of only combination use of both the triptan agent and ant-epileptic drug in ongoing seizures in patients with serious migraine is remarkable in practice. Furthermore, use of anti-epileptic drugs which have long-term half-life period and don’t inhibit GABA at post-synaptic site relives from a seizure experiencing for the following morning.
Methods
Under the circumstance, we conducted a small-group comparative study to evaluate clinical efficacy of combination of anti-epileptic drugs with rizatripan (10 mg per dose) at the same time for approximately thirty patients with serious migraine seizure from several kinds of aspect.
Results
Use of perampanel hydrate with a triptan agent for seizure at an initial day would avoid onset of further seizures at the following days rather than use of sodium valproate despite of no statistical significance between both groups (p = 0.09). Because it was deemed that there is discrepancy on pharmacokinetics between them. Co-administration of tripatn agent and perampanel 2 mg will be recommended in case of severe migraine attacks, and the efficacy of migraine relief continue over 72 hours.
Conclusion
To relief their seizures, our study was definitely demonstrated that combination of perampanel 2 mg with triptan agents would be sufficiently useful in advance.
Disclosure of Interest
None Declared
Migraine Acute Therapy
PO-01-041
Pharmacological analysis of the inhibitory effects produced by moxonidine and agmatine on the sensory vasodepressor cgrpergic outflow in pithed rats
Eloisa Rubio-Beltrán1,2,*, Alejandro Labastida-Ramírez1,2, Oswaldo Hernández-Abreu1, Antoinette MaassenVanDenBrink2 and Carlos M. Villalón1
1Pharmacobiology, Cinvestav-IPN, Unidad Sur, Mexico City, Mexico
2Division of Vascular Medicine and Pharmacology, Department of Internal Medicine, Erasmus University Medical Center, Rotterdam, Netherlands
Objectives
Resistance blood vessels are innervated by perivascular sympathetic and sensory nerves, which modulate vascular tone. Sensory stimulation results in release of the vasodilator calcitonin gene-related peptide (CGRP). CGRP is also present in the trigemino-vascular system and plays a role in migraine pathophysiology. Currently, CGRP receptor antagonists and monoclonal CGRP antibodies are under clinical evaluation for the acute and prophylactic treatment of migraine. An additional antimigraine strategy could be the inhibition of CGRP release. In this respect, our group has shown that spinal (T9T12) electrical stimulation of the rat perivascular sensory CGRPergic outflow results in vasodepressor responses that can be inhibited by activation of prejunctional receptors to several biogenic monoamines.
The aim of this study is to investigate the role of imidazoline I1 and I2 receptors in the inhibition by moxonidine and agmatine of the vasodepressor responses produced by stimulation of the perivascular sensory CGRPergic outflow in pithed rats.
Methods
Male pithed Wistar rats were prepared for electrical spinal (T9-T12; 0.56–5.6 Hz; 50 V, 2 msec) stimulation of the CGRPergic outflow or i.v. bolus injections of α-CGRP (0.1–1 µg/kg) during i.v. continuous infusions of moxonidine (1, 3, 10 or 30 µg/kgċmin) or agmatine (1000 or 3000 µg/kgċmin). Animals were pretreated with the antagonists AGN192403 (I1; 3000 µg/kg), BU224 (I2; 300 µg/kg), rauwolscine (α2; 300 µg/kg) or AGN192403 + rauwolscine. Experiments were approved by our institutional ethics committee, in accord with National Institutes of Health guidelines.
Results
The infusions of moxonidine and agmatine inhibited the vasodepressor responses induced by electrical stimulation, but not by exogenous α-CGRP, implying a prejunctional inhibition. This sensory inhibition was attenuated only by AGN19240, but not by BU224 or rauwolscine.
Conclusion
The inhibition of the CGRPergic outflow by moxonidine and agmatine involves prejunctional activation of imidazoline I1 receptors on perivascular sensory nerves. While our findings should be confirmed in a trigemino-vascular model, our results obtained in a peripheral vascular model suggests the imidazoline I1 receptors as a target for migraine treatment.
Disclosure of Interest
None Declared
Migraine Acute Therapy
PO-01-042
Current status of the primary headache cases in the urban one emergency hospital in Japan
Masaya Kainuma1,*, Hiroyuki Nakaba1 and Tomoyuki Maruo2
1Division of Emergency department, Federation of National Public Service Personnel Mutual Aid Associations, Otemae Hospital
2Division of Neurosurgery, Federation of National Public Service Personnel Mutual Aid Associations, Otemae Hospital, Otemae hospital, Osaka, Japan
Objectives
The international classification of headache disorders second edition published in 2004 has been classified a primary headache in four diseases, and the treatment method to satisfy the patients suffering from chronic headache has been proposed in that guidelines. Now, we are going to report the current status of primary headache cases in our hospital responsible for the urban emergency medical care.
Methods
We targeted this time for 90 cases of patients diagnosed primary headache after visiting our department with symptoms of headache from April 2014 to June 2015.
Results
Their age was 43 ± 18 years, and male was 36 cases, female was 54 cases. Transporting by ambulance was 62 cases (69%), and walk-in was 28 cases (31%). About their consultation day of the week, there are 13 cases in Monday, 17 cases in Tuesday, 17 cases in Wednesday, 14 cases in Thursday, 10 cases in Friday, 12 cases in Saturday, and 7 cases in Sunday. The 13 cases visited our hospital at 0–8 o'clock, 42 cases did at 8–16 o’clock, and 35 cases did at 16–24 o’clock. When they visited, Japan Coma Scale is I-0 in 68 cases, I-1 in 21 cases, I-2 in 1 case and head CT was performed under 69 cases (77%). We diagnosed migraine headache in 36 cases, tension-type headache in 43 cases, cluster and other trigeminal-autonomic headache in 5 cases, and the other primary headache in 6 cases. In 20 cases (22%), we required them hospitalization, and they consisted of migraine 10 cases, tension-type headache 6 cases, 3 cases such as cluster headache, and other in 1 case. Length of hospital stay was 3.8 ± 3.2 days. We performed the treatments by non-steroidal anti-inflammatory drugs in 65 cases, vasoconstrictor in 13 cases (through oral 9 cases, nasal 4 cases, and no subcutaneous injection), an anti-anxiety drugs in 5 cases, Kanpou in 1 case, oxygen in 5 cases, rest only in 19 cases, and other drugs in 7 cases (there were drug combination cases). Their symptoms revealed improvement after visiting our hospital in all cases, and we couldn’t admit death cases. Reconsultation by the same symptoms was seen in 4 cases (4%), and reconsultation cases within 24 hours after visiting hospital were not observed.
Conclusion
We reported 90 patients and current status of the primary headache cases in the urban one emergency hospital in Japan. Primary headache is so a disease that impairs extremely quality of the life of patients, accurate diagnosis and treatment are desirable when the symptoms appear. This time, it was relatively satisfactory results in our case.
Disclosure of Interest
None Declared
Migraine Acute Therapy
PO-01-043
Role of AMPA receptor phosphorylation in nitroglycerin-induced migraine headache
Yuanyuan Tang1, Sufang Liu1, Hui Shu1, Qian Bai1, Qing Lin2 and Feng Tao1,3,*
1Department of Biomedical Sciences, Texas A&M University College of Dentistry, Dallas
2Department of Psychology, University of Texas at Arlington, Arlington
3Center for Craniofacial Research and Diagnosis, Texas A&M University College of Dentistry, Dallas, United States
Objectives
Migraine is the third most common disease worldwide; however, the mechanisms underlying migraine headache are still not fully understood and current therapies for this type of pain are inadequate. AMPA receptor phosphorylation can promote the receptor trafficking and then enhance the switch from Ca2+-impermeable to Ca2+-permeable receptors in the central nervous system, thereby causing activity-dependent changes in synaptic processing of nociceptive information. In the present study, we used an established nitroglycerin (NTG)-induced acute migraine headache mouse model to investigate the effect of blockade of Ca2+-permeable AMPA receptors in spinal trigeminal nucleus caudalis (Sp5C) on the development of migraine headache.
Methods
C57BL/6 male and female mice were used in this study. Intraperitoneal injection of NTG (10 mg/kg, i.p.) was carried out to induce migraine headache. Light-aversive behaviors (immediately following the NTG injection) and mechanical hypersensitivity (120 min after the injection) were measured using a light-dark box and von Frey filements, respectively. 1-naphthyl acetyl spermine (NASPM), a selective Ca2+-permeable AMPA receptor channel blocker, was administrated to examine whether blockade of Ca2+-permeable AMPA receptors affects NTG-induced migraine headache. In addition, Ca2+ imaging was carried out to analyze Ca2+ activities in cultured brainstem neurons following the treatment with NTG and/or NASPM.
Results
Injection of NTG (i.p.) induced photophobia and decreased mechanical withdrawal threshold in both male and female mice. The NTG administration also increased AMPA receptor GluA1 phosphorylation at the Ser831 site in the Sp5C. Intra-Sp5C injection of NASPM (3 mM, 0.9 µl) significantly inhibited NTG-produced mechanical hypersensitivity, but had no effect on NTG-induced photophobia. In cultured brainstem neurons, NTG caused a robust Ca2+ influx, and the incubation of NASPM (5 µM) partially blocked the NTG-enhanced Ca2+ activities.
Conclusion
Our results suggest that AMPA receptor phosphorylation-enhanced switch from Ca2+-impermeable to Ca2+-permeable receptors in the Sp5C contributes to NTG-induced migraine headache.
Disclosure of Interest
Y. Tang: None Declared, S. Liu: None Declared, H. Shu: None Declared, Q. Bai: None Declared, Q. Lin: None Declared, F. Tao Conflict with: Supported by NIH/NIDCR Grants (R01 DE022880 and K02 DE023551).
Migraine Acute Therapy
PO-01-044
Clinical Profile, Management Trends and Functional disability in Patients with Migraine: A Pan-India Cross- Sectional Study
Sumit Singh1,*, Kushal Sarda2 and Rashmi Hegde2
1Artemis Institute of Neurosciences, Gurgoan
2Abbott India Ltd, Mumbai, India
Objectives
Migraine is the third most prevalent and seventh leading cause of disability worldwide. Despite high prevalence, there are no population based studies from India. This observational, cross-sectional pan study was conducted to understand the clinical profile, disease burden, and management trends in patients with migraine in India.
Methods
Patients (≥18 years) diagnosed with migraine based on clinical diagnosis/ICHD criteria were enrolled across 11 centers in India. Details on demographics, history, clinical pattern, comorbidities, treatment for acute attack and prophylaxis, Migraine Specific Quality of Life (MSQ) and Migraine Disability Assessment Score (MIDAS) were recorded.
Results
Of 705 patients enrolled, 81% were females and 19% were males. Mean age of the study population was 35.16 ± 11.09 years. Mean age of onset of migraine was 25.05 ± 8.54 years; mean age of onset was lower in patients in 18–40 years’ group (22.93 ± 6.03 years) compared with patients in 41–60 years (32.70 ± 9.64 years) and >61 years’ group (35.92 ± 14.51 years). Most common trigger for migraine attacks were stress (75%), lack of sleep (67%) and travelling (64%). Nearly half of the patients (54%) had migraine of moderate severity; 38% patients reported severe migraine. Most common drug for acute attacks of migraine was paracetamol (47%) followed by naproxen (13%) and sumatriptan (12%). Propranolol (51%) was the most common medication for prophylaxis of migraine followed by flunarazine (40%). Paracetamol was the most common rescue medication used along with the prophylaxis therapy. Higher proportion of patients had 4 h to 72 h duration of headache attacks (44%), 1 to 10 attacks per month (70%), pulsating type of headache (76%), and sensory symptoms (negative) (45%). Nausea (65%), photophobia (63%), phonophobia (51%) and vomiting (46%) were the most common symptoms reported to be associated with migraine. Majority of the patients had MSQ score of 3 (some of the time) indicating that the patients sometimes felt that migraine was interfering while dealing with family and close friends (32%); sometimes felt that migraine was interfering while doing leisure time activities, such as reading or exercising (33%); had sometimes difficulty in performing daily activities (35%) and had limitations in concentrating on work or daily activities due to migraine (39%). The comorbidities reported were hypertension (7%), diabetes mellitus (3%), anxiety (2%), asthma (2%), and epilepsy and arthritis (1%). Majority of patients (46%) had moderate disability with a total MIDAS score ranging from 11–20; severe disability was reported in 37.3% patients, with a total MIDAS score of 21+. Sleep/rest (64%) and meditation (22%) were the most commonly reported relieving factors from migraine associated headache.
Conclusion
The present study extends the body of literature characterizing treatment patterns, disorder characteristics, and disability profile in migraineurs in India. Consistent with published literature, this study also highlights a higher prevalence of migraine in women. NSAIDs remain the mainstay acute treatment whereas propranolol was the most commonly prescribed prophylactic drug. Moreover, sleep/rest and meditation were the most commonly reported relieving factors from migraine associated headache. Patients demonstrated restriction in their daily activities, reflected by their MSQ score. Moderate to severe disability was reported in majority of the patients, as assessed by their MIDAS score.
Disclosure of Interest
S. Singh Conflict with: The investigator received funding from Abbott India Limited, K. Sarda Conflict with: Is an employee of Abbott, R. Hegde Conflict with: Is an employee of Abbott
Migraine Acute Therapy
PO-01-045
Compared to Oral Sumatriptan, AVP-825 Reduces Disability by Relieving Migraine Severity: An Analysis from the COMPASS Study
James S. McGinley1, R. J. Wirth1, Dawn C. Buse2, Kenneth J. Shulman3 and Richard B. Lipton2,*
1Vector Psychometric Group, LLC, Chapel Hill
2Albert Einstein College of Medicine and Montefiore Headache Center, Bronx
3Avanir Pharmaceuticals, Inc., Aliso Viejo, United States
Objectives
Migraine presents as a symptom complex, where attacks are defined by a series of correlated symptoms. Pain, nausea, photophobia, and phonophobia are symptoms of migraine which are included in the diagnostic criteria. Drug trials for the treatment of acute migraine attacks often use a narrowly defined efficacy outcome measure based only on improvement of pain. But to those with migraine, all of the symptoms experienced during an attack correlate with their disability in some way. Disability can be conceptualized as an indicator of migraine severity or as a consequence of it. Our previous research measured migraine severity as a latent variable comprising pain, nausea, photophobia, phonophobia and disability as individual indicators. In the current study, we evaluated this competing theoretical model that Migraine Severity (a latent variable defined as a composite of all migraine symptoms, including pain, nausea, photophobia and phonophobia) mediates the relation between treatment and disability using structural equation models (SEMs). Specifically, we tested the hypothesis that, compared to 100 mg oral sumatriptan, AVP-825 (a breath powered intranasal delivery system containing 22 mg sumatriptan powder) reduced disability more because it provided better relief of pain and all migraine-associated symptoms, as measured by Migraine Severity.
Methods
The COMPASS Study randomized adults with a diagnosis of migraine to one of two treatment sequences. Participants were instructed to treat up to 5 qualifying migraines within one hour of onset with active study drug (AVP-825 22 mg or oral sumatriptan 100 mg) plus corresponding placebo in each 12-week treatment period. All available data on pain intensity (0 = none to 3 = severe), nausea (0 = no, 1 = yes), photophobia (0 = no, 1 = yes), phonophobia (0 = no, 1 = yes), and associated disability (0 = none to 3 = severe) assessed at pre-dose, 10, 15, 30, 45, 60, 90, and 120 min post-dose were analyzed. SEMs were fitted to test whether the effect of treatment on disability was mediated by the prior Migraine Severity (e.g., Migraine Severity at 10 min predicted disability at 15 min, Migraine Severity at 15 min predicted disability at 30 min, etc.).
Image:

Results
Our analyses included 259 subjects treating an average of 6.8 attacks each. Participants had a mean age of 40 and 84.6% were female. Results showed that the correlational relationship (factor loadings) between each individual migraine symptom and Migraine Severity were statistically significant (pain was most strongly associated with Migraine Severity, then photo/phonophobia, and nausea; data not shown). AVP-825 produced lower levels of Migraine Severity from 10 min through 90 min compared to oral sumatriptan, and increased Migraine Severity predicted increased disability at subsequent time points (p < .01 for all, see Table). Examination of the indirect effect of treatment on disability showed that AVP-825 reduced Migraine Severity from 10 min−90 min which, in turn, led to lower disability from 15 min−120 min relative to oral sumatriptan (p < .01; see Table).
Conclusion
Findings provided empirical support for the theory that Migraine Severity, a composite variable including pain, nausea, photophobia and phonophobia, predicts subsequent disability. AVP-825 offers greater disability improvement because it treats Migraine Severity better than oral sumatriptan. Our study showed that SEMs can rigorously evaluate clinical theory and measure migraine as a symptom complex. Future studies should be designed to explicitly evaluate the various competing migraine theories (e.g., is disability a measure of Migraine Severity or a consequence of it?) to determine which theoretical model best represents real-world experiences.
Disclosure of Interest
J. McGinley Conflict with: Vector Psychometric Group, LLC, R. Wirth Conflict with: Vector Psychometric Group, LLC, D. Buse Conflict with: Allergan, Avanir, and Dr. Reddys, Conflict with: served on scientific advisory board and received compensation from Allergan, Amgen, and Eli Lilly; section editor for Current Pain and Headache Reports, K. Shulman Conflict with: Avanir Pharmaceuticals, Inc., R. Lipton Conflict with: National Institutes of Health, National Headache Foundation, and Migraine Research Fund, Conflict with: serves as consultant, advisory board member, or has received honoraria from Alder, Allergan, American Headache Society, Autonomic Technologies, Boston Scientific, Bristol Myers Squibb, Cognimed, CoLucid, Eli Lilly, eNeura Therapeutics, Merck, Novartis, Pfizer, and Teva, Inc.; receives royalties from Wolff’s Headache, 8th Edition (Oxford University Press, 2009)
Migraine Acute Therapy
PO-01-046
Adverse events of sumatriptan and predicting factors: a clinic-based study
Jong-Ling Fuh1,2,*, Kuan-Po Peng1,2, Shih-Pin Chen1,2, Yen-Feng Wang1,2 and Shuu-Jiun Wang1,2
1Department of Neurology, Taipei Veterans General Hospital
2Faculty of Medicine, National Yang-Ming University School of Medicine, Taipei, Taiwan, Republic of China
Objectives
Triptans are widely used in migraine acute treatment; however, individual responses and adverse events (AE) vary. Sumatriptan remains the most widely used triptan worldwide. We aimed to investigate factors associated with the development of AE.
Methods
We conducted an observational cohort study in a headache clinic in a tertiary medical center. This study is a collaborative study of the original genome-wide association study of migraine. Migraine patients who had been prescribed with sumatriptan were enrolled. Patients were asked of any AE, or triptan sensation after the use of sumatriptan tablet (50mg). Triptan sensation was defined as discomfort, tightness, flushing or paresthesia over the chest, neck, or extending to the face.
Results
A total of 1,270 patients were enrolled, of which 1,008 (79.4%) were women, with a mean age of 38.7 ± 11.3 years. Most patients (91.3%) were diagnosed with migraine without aura; while 32.1% fulfilled the diagnosis of chronic migraine, 20.6% the diagnosis of medication over use headache. Any AE was reported in 321 (25.3%) of 1,270 patients, triptan sensation in 115 (9.1%) patients, and most of these AE lasted for 2–3 hours. Compared to those without AE, patients with any AE were more likely to be women (odds ratio [OR]: 1.82, p < 0.001), younger (OR: 0.984 per year, p = 0.006), had a lower depression score (Hospital Anxiety Depression Score – Depression score, 4.8 ± 3.5 vs. 5.5 ± 4.0, p = 0.013). Certain migrainous features were more prominent among patients who developed AE, including lateralized headache (38.4% vs. 29.8%, p = 0.006), pulsating headache (69.5% vs. 62.7%, p = 0.029), photophobia (64.8% vs. 57.9%, p = 0.033), and phonophobia (85.7% vs. 75.0%, p < 0.001). Of note, mense-related headache worsening was more common among those who developed AE than those without (80.5% vs. 69.1%, p < 0.001). Predictors for triptan sensation were similar to those with any AE.
Conclusion
In this large cohort, one fourth of migraine patients experienced any AE of sumatriptan and 9,1% reported triptan sensation. Women in overall were more likely to experience any AE. A specific link to certain migrainous features suggests central sensitization or trigeminovascular activation might be relevant to the development of AE.
Disclosure of Interest
None Declared
Migraine Acute Therapy
PO-01-047
An innovative treatment of chronic migraine and craniofacial neuralgia
Faro T. Owiesy1,*
1Family Medicine, Corona Doctors Medical Clinics, Inc., Corona, United States
Objectives
A simultaneous treatment of trigeminal and occipital nerves using a combination of dexamethasone, lidocaine, and thiamine never been studied. Migraine headaches or craniofacial neuralgia involving in 90% of cases both trigeminal and greater occipital nerves. Treatment of one nerve without simultaneous treatment of the other did not prove helpful in any of our cases. However, simultaneous treatment of all and both nerves resulted in longest discontinuation of migraine and craniofacial pain. The interaction of genetic signaling with cell surface receptor is a new subject in molecular biochemistry and biology. It is hypothesized that the genetic signals silencing and de -silencing within the autonomic nerve system per se balances the stimulatory effect of the perivascular sympathetic and parasympathetic systems in the peripheral nerves. The objective of this study was the safety and efficacy of simultaneous administration of dexamethasone, lidocaine, and thiamine into the trigeminal nerve branches and the greater and lesser occipital nerve for treatment of chronic migraine, and craniofacial neuralgia.
Methods
The study is a single- center, randomized, patient- centered pilot study of chronic migraine and craniofacial patients in status migrainous with and without aura. Preparation and administration of a combination of sterile dexamethasone phosphate total dose of 20 mg, 4 mg/ml, lidocaine HCL 1% 40 mg, 10 mg/ml, and thiamin(B1), 200 mg/ml in conducted in a single session into the accessible branches of the trigeminal nerve. The index period (June, 1 2007 – September, 2013). Study follow-ups: one week, 4 weeks, 26 weeks, and 52 weeks. Inclusion Criteria:Patient ages ranged from 12 years old (parental consent was obtained) to 87 years old. Forty patients (10 male and 30 female) participated in the study. Patients were randomly selected from those who approached our clinic seeking treatment for acute exacerbation with status migrainous. All patients exhausted their treatment with abortive and prophylactic medications during the previous 12 months. No medical comorbidity discrimination was specified for this study. Exclusion Criteria: Uncontrolled hypertension, including contraceptive induced. History of stroke, transient ischemic attack, or non-migraine-related seizure. History of brain aneurysm, implantation of any type of neuro-stimulator, trigeminal tractotomy, trigeminal or occipital nerve neurectomy, or microvascular decompression. Hypersensitivity or allergy to any components of de novo formula.
Results
We recruited 52 patients who qulified for the de-novo treatment. Of those, 12 patients showed low or no adherence to post-treatment follow ups and were excluded from statistical evaluation, and 40 completed planned follow-ups. All patients received the same clinical evaluation and treatment per protocol. Out of 40 patients, 38(95%) experienced long-term resolution of their migraine or craniofacial neuralgia and 2 (5%) experienced major relief of their complex and chronic migraine with episodic relapse and remisssion. The avergae length of migraine free period was 15.24 months. The single longest migraine free period was 65 months until the end of the trial in 2013. One patient did not demonstrate any respond to treatment. An exploratory revision of rt. Temporo-parietal muscle and fascia revealed presence of a neuroma of zygomatico-facial nerve. A Neuronectomy resulted in complete resolution of migraine and craniofacial neuralgia.
Conclusion
The goal of treatment is to equilibrate and balance autonomous nerve system. Among the multimodal treatment approaches in chronic craniofacial neuralgia and migraines, simultaneous bilateral administration of dexamethasone, lidocaine, and thiamine demonstrated promising results. The de novo treatment is cost effective, safe, and reduces the need for poly-pharmacy.
Disclosure of Interest
F. Owiesy Conflict with: employee research
Migraine Acute Therapy
PO-01-048
Is oral telcagepant a relatively slowly acting drug? a mini-review of 4 rcts
Peer Tfelt-Hansen1,* and Thien P. Do1
1Danish Headache Center, Glostrup Hospital, Glostrup, Denmark
Objectives
Gepants are a new treatment principle, based on CGRP antagonism, in migraine. Patients want a quick effect and to be pain-free. The onset of action is often forgotten when evaluating oral drugs in migraine. The efficacy of drugs is in most cases compared 2 hours after drug administration.
The aim of this mini-review is by correcting by therapeutic gain (active drug minus placebo) (TG) to evaluate the first part of the time-effect curves up to 2 hours for telcagepant, the best documented CGRP-antagonist.
Methods
Calculated therapeutic gains (italics) after oral telcagepant (280 − 300 mg) administered in placebo-controlled RCTs.
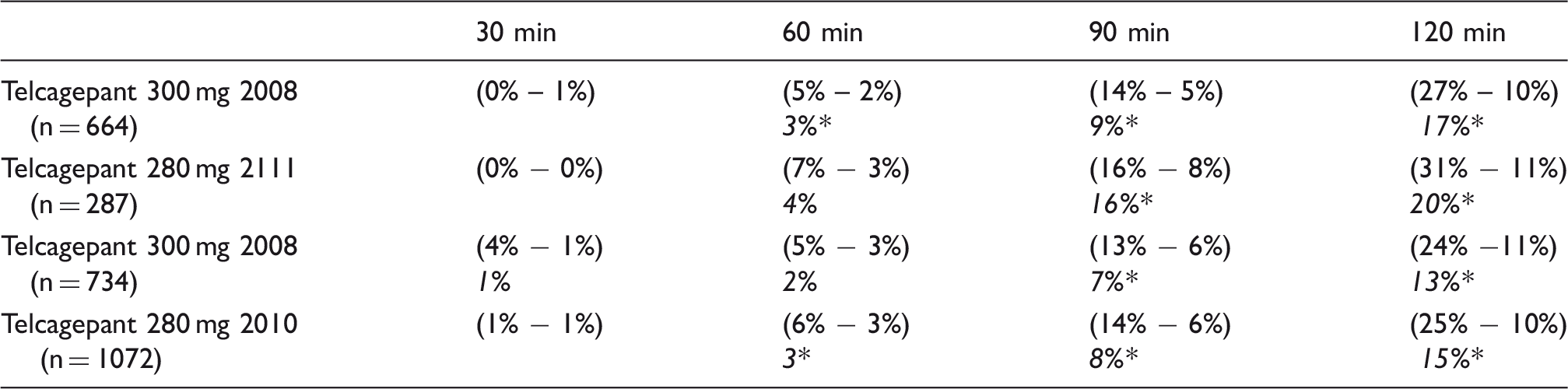
Note: *, P < 0.05, vs. placebo.
Results
In the 4 telcagepant RCTs (280 – 300 mg) the pain-free for the drug at 120 minutes was 26% (369/1377) vs. 10% (143/1394) for placebo. Thus the TG for all studies was 16%. In the large Lancet paper [1] the TG increased 6% (17% to 23%) from 2 to 3 hours; and in a RCTs on combinations of NSAIDs with telcagepant [2] the TG for telcagepant increased 8% (20% to 28%) from 2 to 4 hours.
Conclusion
In 2 placebo-controlled study a statistical significant PF effect vs. placebo after 60 min was demonstrated (Table 1) but the TG was in both studies only 3%. In the other 2 studies (Table 1) telcagepant was first superior to placebo after 90 min. Thus oral telcagepant is relatively slowly acting acute drug in migraine despite the median Tmax of 1.5 hours (min. max.: 1 h to 3 h) in blood (n = 19). This is relatively slow onset of action is supported by the additional increases in TGs in 2 RCTs [1,2] beyond 2 h.
The slow onset of action of the CGRP antagonist telcagepant is difficult to explain to be due mainly to a blocking of the drug effect on tissues without blood-brain barrier, e.g. the meningeal artery and extracranial arteries. Alternative mechanisms for the effect of the gepants should be investigated.
References
1. Ho TW, Ferrari MD, Dodick DW, et al. Efficacy and tolerability of MK-0974 (telcagepant), a new oral calconist of calcitonin gene-related peptide receptor, compared with zolmitriptan for acute migraine: a randomized, placebo-controlled, parallel-treatment trial. Lancet 2008; 372: 2115–23.
2. Hewitt DJ, Martin V, Lipton RB, et al. Randomized controlled study of telcagepant plus iboprufen or acetaminophen in migraine. Headache 2011; 51: 533–543.
Disclosure of Interest
None Declared
Migraine Acute Therapy
PO-01-049
Variation in Prescription Drug Coverage for Triptans: Analysis of Insurance Formularies
Mia T. Minen1,*, Kate Lindberg2, Aisha Langford3 and Elizabeth Loder4
1Neurology, NYU Langone Medical Center
2Barnard College, Columbia University
3NYU Langone Medical Center, New York
4Brigham and Women's/Faulkner Hospital, Boston, United States
Objectives
Triptans are FDA approved migraine abortive medications. Patients frequently state that they have difficulty accessing triptans prescribed to them. We sought to analyze triptan coverage by insurers to examine (1) possible disparities in coverage for different formulations (oral, intranasal, etc.) and (2) quantity limits and stepped care requirements to obtain triptans.
Methods
We searched the 2015 drug formularies of commercial and government health insurers providing coverage in NY State. We created a spreadsheet with all of the commercially available triptans and included information about covered formulations, tier numbers and quantity limits for each drug. We then calculated the number of listed plans that cover or do not cover each triptan or triptan formulation, the total number of medications not covered by an insurance provided across all of its plans, as well as the percentage of plans offered by individual companies and across all companies that covered each drug. We also calculated the number and proportion of plans that imposed quantity limits or step therapy for each drug.
Results
Of the 100 formularies searched, generic sumatriptan (all formulations), naratriptan and zolmitriptan tablets were covered by all plans, and rizatriptan tablets and ODTs were covered by 98% of plans. Brand triptans were less likely to be covered: 4/36 Medicaid plans covered brand triptans. Commercial insurers were more likely to cover brand triptans. All plans imposed quantity limits on 1+ triptan formulations, with >80% imposing quantity limits on 14/19 formulations studied. Almost all plans used tiers for cost allocation for different medications. Generic triptans were almost always in Tier 1. Brand triptans were most commonly in Tier 3. Approximately 40% of brand triptans required step therapy, compared with 11% of generic triptans.
Conclusion
There are substantial variations in coverage and quantity limits and a high degree of complexity in triptan coverage for both government and commercial plans.
Disclosure of Interest
M. Minen: None Declared, K. Lindberg: None Declared, A. Langford: None Declared, E. Loder Conflict with: Editor for the British Medical Journal
Migraine Acute Therapy
PO-01-050
Oral naratritan, sumatriptan and zolmitriptan have, in quipotent doses, similar time-effect curves with maximum effect after 4 hours
Peer Tfelt-Hansen1,*
1Danish Headache Center, Glostrup Hospital, Glostrup, Denmark
Objectives
“Naratriptan 2.5 mg has been shown to be less effective and has a slower onset of action, but is better tolerated than sumatriptan 100 mg. It is one of the two slower-acting triptans” [1].
The affinities of naratriptan to the human 5-HT1B and 5-HT1D receptors are similar to those of sumatriptan, and zolmitriptan; in in vitro and in vivo models naratriptan has a pharmacological profile similar to sumatriptan. The oral bioavailability of naratriptan is 74 % (Tmax = 2 h) vs. sumatriptan 14% (Tmax = 1½ h). Subcutaneous naratriptan, 10 mg pain free (PF) at 2 h = 88%, is superior to subc. sumatriptan 6 mg (PF at 2 h = 55%) (P < 0.05).
One can thus wonder why naratriptan is “a less effective triptan”, see vignette. This question will be explored in the following.
Methods
Effect of naratriptan, sumatriptan and placebo on headache relief in 2 RCTs in migraine.

Results
Therapeutic gain (TG), active drug minus placebo.
The combined headache relief for naratriptan 2.5 mg was 46% at 2 h (TG = 19%), and it was 66% at 4 h (TG = 33%).
The combined headache relief for zolmitriptan 2.5 mg was 64% at 2 h (TG = 29%), and it was 73% at 4 h (TG = 39%).
In addition, in one RCT headache relief for frovatriptan 2.5 mg was 46% at 2 h (TG = 19%), and it was 65% at 4 h (TG = 27%), but the instructions to patients about escape medication was unclear.
Conclusion
1. The time-curves for triptans can depend on the dose of drugs, confer the results with naratriptan. 2. Tmax in plasma for triptans is 1½ − 2 h. The antimigraine effect of triptans has an increase up to 4 h, and this discrepancy remains unexplained and should be investigated further.
Reference
1. Johnston MM, Rapoport AM. Triptans for the management of migraine. Drugs. 2010; 70:1505–1518.
Disclosure of Interest
None Declared
Migraine Acute Therapy
PO-01-051
Remission of Migraine Headache Frequency During Pregnancy
Devi A. Sudibyo1,*, Isti Suharjanti1 and Nurlisa N. Aulia1
1Neurology, Airlangga University, Surabaya, Indonesia
Objectives
Migraine is one of primary headache which affects about 12% population. It is most common between the ages 20 and 45, with women predominantly. Hormonal changes, especially during pregnancies is one of the trigger factors. We report a case with migraine attack that dramatically reduce during pregnancy.
Methods
Women 43 - years old, with recurrent pulsating headache on the left side. It lasted for almost 24 hours without any medication and relieved with either medication or cessation. The headache occurred approximately 15 times a month and worsen with activities, photophobia, and phonophobia. Patients had been experienced nausea and vomiting. Visual loss nor flashing lights phenomenon were not found, neither numbness nor tingling, no weakness of the body neither language disturbance prior to headache. The physical and neurologic examination were normal. Numeric Rating Scale (NRS) was 8 during acute headache attack. MRI and MRA with contrast were perform to exclude intracranial lesion. Patient had been taken paracetamol, diazepam, amitriptyline.
Results
The migraine attack’s frequencies dramatically reduce 3–4 times a month during pregnancy because the estrogen hormone increased. Estrogen can modulate neurotransmitter system involving serotonin, noradrenaline, γ aminobutyric acid (GABA). Increasing serotonin concentration is able to increase the activation of 5HT receptor that can block the neuropeptide vasoactive at trigeminal nucleus of brain stem.
Conclusion
Increasing estrogen level during pregnancy can reduce the migraine attack frequency.
Disclosure of Interest
None Declared
Migraine Acute Therapy
PO-01-052
Study of genes involved in Migraine
Nitin Kumar1,* and R Khanna1
1Department of Basic and Applied Biology, VIVEKANANDA GLOBAL UNIVERSITY, Jaipur, India
Objectives
Migraine is a common brain disorder although the molecular mechanisms involved are poorly understood. Genetic factors essentially contribute to migraine. However approaches to identify genes for common forms of migraine have been of limited success. Genome-wide association (GWA) studies are an important approach used to uncover the genetic susceptibility components of complex diseases such as migraine.
Methods
We selected 11 genes from previously published candidate gene association studies and nine additional genes from other studies in migraine.
Results
Side-locked unilateral headache and facial pain include a large number of primary and secondary headaches and cranial neuropathies. The SNPs situated within and near the selected identified genes, including those SNPs that were previously thought to be associated with migraine could not confirm with the Bonferroni-corrected significance threshold.
Conclusion
The selected genes could not provide any clear evidence for their involvement as a promising candidate genes involved in migraine.
Disclosure of Interest
None Declared
Migraine Preventive Therapy
PO-01-053
Preventive treatment with lomerizine hydrochloride increases cerebral blood flow during the interictal phase in migraineurs
Ken Ikeda1,*, Joe Aoyagi1, Masahiro Sawada1, Masaru Yanagihasi1, Yuichi Ishikawa1, Ken Miura1, Takehisa Hirayama1, Takanori Takazawa1, Osamu Kano1 and Yasuo Iwasaki1
1Neurology, Toho University Omori Medical Center, Tokyo, Japan
Objectives
Migraine is a common, primary, chronic-intermittent neurovascular headache disorder. Previous studies of brain single photon emission tomography (SPECT) showed changes of regional cerebral blood flow (rCBF) in migraineurs during a prodrome, an aura or a headache attack. Sumatriptan (6 mg, sc) did not alter rCBF significantly at a migraine attack (Ferrari et al. Arch Neurol 1995). However, little is known how preventive medication of migraine can influence rCBF. Lomerizine hydrochloride (LH), a calcium channel blocker, has been used widely as a migraine prophylactic drug in Japan. We aimed to analyze brain SPECT findings before and after LH treatment.
Methods
Migraine was diagnosed according to the criteria of the International Classification of Headache Disorders, 3rd Edition beta. Migraine was classified into migraine with aura (MA) and migraine without aura (MO). LH (10 mg/day, po) was administered for 3 months. Headache Impact Test-6 (HIT-6) compared before and after LH treatment. Brain SPECT using 99mTc-ethyl cysteinate dimer was performed at the headache-free interictal period. Brain SPECT data were analyzed according to revised version of 3-dimensional stereotaxic region of interest (ROI) template (Takeuchi et al. Eur J Nucl Med 2002). A total of 636 ROIs were set in bilateral cerebral cortexes and cerebellar hemispheres. Global CBF was calculated from all data of 636 ROIs in whole brain, including both cerebral hemispheres and cerebellum. SPECT images were divided as regional CBF into 24 symmetrical (right and left) regions per patient: the callosomarginal, the precentral, the central, the parietal, the angular, the temporal, the posterior, the pericallosal, the lenticular nucleus, the thalamus, the hippocampus and the cerebellar hemisphere. Data of global and regional CBFs were shown in mL/100 g/min. rCBF was compared before and after LH treatment. All data of HIT-6 score and rCBF were analyzed by Wilcoxon singed rank test.
Results
A total of 10 migraineurs (4 men and 6 women) were participated in the present study. Mean age (SD) of migraineurs was 55.5 (15.8) years. Mean duration (SD) of migraine was 15.3 (7.7) years. Migraine subtype showed 4 patients with MA and 6 patients with MO. Mean score (SD) of HIT-6 was 66.3 (11.7) points. LH treatment decreased HIT-6 scores significantly (P < 0.01). Compared to rCBF at baseline before LH treatment, LH treatment increased rCBF significantly at 10–20% in the frontal, the parietal and the occipital regions (P < 0.05). These changes of brain SPECT findings and HIT-6 score did not differ between MA sufferers and MO sufferers.
Conclusion
Previous experimental studies suggested that LH inhibited cerebral hypoperfusion and expression of c-Fos-like immunoreactivity induced by cortical spreading depression via the blockade of Ca2+ influx into brain cells in anaesthetized rats. (Shimazawa et al. British J Pharmacol 1995). LH had greater effects on CBF than on blood pressure and heart rate in anaesthetized rats and beagle dogs. (Hara et al. Exp Pharmacol Physiol 1999). LH blocked 5-hydroxytryptamine (5-HT)2A receptors, and reduced 5-HT-triggered contraction in rat basilar artery (Ishii et al. J Pharmacol Sci 2009). Our study limitation included the small number of patients, rCBF analysis only at interictal phase, and costs and radiation exposure of brain SPECT. Finally, brain SPECT disclosed significant increase of rCBF in the anterior and posterior circulation areas after migraineurs received LH medication for 3 months. The present study indicated that alternation of cerebral circulation during the interictal period could contribute to preventive effects of LH in migraineurs with and without aura.
Disclosure of Interest
None Declared
Migraine Preventive Therapy
PO-01-054
What happens when chronic migraine patıents quit onabotulinumtoxina?
Pinar Yalinay Dikmen1,*, Seda Kosak1, Elif Ilgaz Aydınlar1 and Ayse Sagduyu Kocaman1
1Neurology department, acibadem university school of medicine, istanbul, turkey
Objectives
The present study was designed to evaluate the efficacy and rates of quitting OnabotulinumtoxinA (OnabotA) and the reasons for doing so among CM patients treated with at least one OnabotA. Our aim was to analyze our 4.5 years’ real-life experience of OnabotA treatment of CM, paying special attention to what happens after 4.5 years. The second objective of this study was to evaluate the latest migraine-related disability and current medication use of CM patients.
Methods
203 patients with CM (40.6 ± 10.1; 177 females, 25 males) were injected with OnabotA as per PREEMPT Protocol between February 2012 and December 2016. The results of a Migraine Disability Assessment Test (MIDAS), duration of migraine and concomitant medication overuse headache were recorded at the first OnabotA treatment. Data were collected by telephone using a standardized interview. The patients were asked about their current MIDAS and the number of analgesic usages and past OnabotA experience.
Results
The duration of migraine in CM patients was 10.5 ± 9.1. In total, 513 treatment cycles (n = 1–13) were administered. The mean OnabotA cycles of the patients were 2.5 ± 2.0. At the first injection, the MIDAS scores of the patients were 52.7 ± 25.5 and the mean analgesic usage per month was 26.6 ± 22.7. The subsequent MIDAS scores were significantly lower than the first one; respectively, (17.4 ± 18.6; n = 97); (15.1 ± 15; n = 60);(10 ± 11.1; n = 32);(10.5 ± 10.5; n = 21);(10 ± 8.3; n = 12);(11.4 ± 11.8; n = 12);(17.7 ± 20.2; n = 7);(6.0 ±8.7;n = 5).
Sixty-six percent of the patients (n = 134) answered questions about the benefit of the treatment, their reasons for quitting OnabotA treatment, and their current headache features. Fifty-five patients could not be reached and fourteen patients refused to take part in the study. Seventy-six percent of the patients (n = 102) thought they had benefited from OnabotA; however, 24 percent of the CM patients (n = 32) did not respond to OnabotA. 134 patients gave a number (from 0 to 10) to represent the efficacy of their treatment; 83 percent of the patients (n = 111) gave a score of 5 or above 5 for its usefulness (6.8 ± 2.8).
The reasons for quitting OnabotA among CM patients (n = 107) were as follows: no benefit (n = 31; 29 %); no need any more/significant improvement of headache (n = 30; 28 %); expensiveness/economic reasons (n = 27; 25 %); distance to hospital/location (n = 5; 5 %); painful needles (n = 4; 4%); side effects/cosmetic reasons (n = 4; 4 %); busy schedule (n = 6; 5 %). Six of the 134 patients continued to receive OnabotA treatment at different center now.
The current MIDAS scores of the patients were 16.6 ± 16.5 and the mean number of analgesics per month was 9.0 ± 14.6. Comparing the current and the first MIDAS scores (p < 0.001) and the number of analgesic usages (p < 0.001) now and at first showed a statistically significant decline in both.
Conclusion
The most important reasons of the quitters were no benefit from OnabotA, significant improvement of headache and economic difficulty. Our results confirm the usefulness of OnabotA treatment in 76 % of patients. Moreover, the migraine-related disabilities of the patients were greatly reduced after only one OnabotA injection and remained the same for several years. Real-life experience with OnabotA showed that the CM patients, even though they had not completed four cycles of the treatment, had extremely diminished migraine-related disability and medication overuse, even after 4.5 years, compared with their condition at first.
Disclosure of Interest
None Declared
Migraine Preventive Therapy
PO-01-055
Chiropractic spinal manipulative therapy for migraine. A three-armed, single-blinded, placebo, randomized controlled trial
Aleksander Chaibi1,2,*, Jurate Š. Benth1,3, Peter Tuchin4 and Michael B. Russell1,2
1Institute of Clinical Medicine, Akershus University Hospital, University of Oslo
2Head and Neck Research Group
3HØKH, Research Centre, Akershus University Hospital, Oslo, Norway
4Department of Chiropractic, Macquarie University, NSW, Sydney, Australia
Objectives
To investigate the efficacy of chiropractic spinal manipulative therapy (CSMT) for migraineurs.
Methods
Prospective three-armed, single-blinded, placebo, randomized controlled trial (RCT) of 17 months duration including 104 migraineurs with at least one migraine attack per month. The RCT was conducted at Akershus University Hospital Oslo, Norway. Active treatment consisted of CSMT, while placebo was a sham push manoeuvre of the lateral edge of the scapula and/or the gluteal region. The control group continued their usual pharmacological management. The RCT consisted of one month run-in, three months intervention and outcome measures at the end of the intervention and at three, six and 12 months follow-up. Primary end-point was number of migraine days per month, while secondary end-points were migraine duration, migraine intensity and headache index (HI) and medicine consumption.
Results
Migraine days were significantly reduced within all three groups from baseline to post-treatment (p < 0.001). The effect continued in the CSMT and placebo group at all follow-up time points, while the control group returned to baseline. The reduction in migraine days was not significantly different between the groups (p > 0.025 for interaction). Migraine duration and headache index were significantly more reduced in the CSMT than the control group towards the end of follow-up (p = 0.02 and p = 0.04 for interaction, respectively). Adverse events were few, mild and transient. Blinding was concealed throughout the RCT.
Conclusion
It is possible to conduct a manual-therapy RCT with concealed placebo. The effect of CSMT observed in our study is likely due to a placebo response.
Disclosure of Interest
None Declared
Migraine Preventive Therapy
PO-01-056
Adverse events in a chiropractic spinal manipulative therapy single-blinded, placebo, randomized controlled trial for migraineurs
Aleksander Chaibi1,2,*, Jurate Š. Benth1,3, Peter Tuchin4 and Michael B. Russell1,2
1Institute of Clinical Medicine, Akershus University Hospital, University of Oslo
2Head and Neck Research Group
3HØKH, Research Centre, Akershus University Hospital, Oslo, Norway
4Department of Chiropractic, Macquarie University, NSW, Sydney, Australia
Objectives
Unlike pharmacological randomized controlled trials (RCTs), manual-therapy RCTs do not always report adverse events (AEs). The few manual-therapy RCTs that provide information on AEs are frequently without details, such as the type and-, severity of the AE and reason for withdrawal. Thus, we prospectively reported all AEs in a chiropractic spinal manipulative therapy (CSMT) RCT in a prospective 3-armed, single-blinded, placebo, RCT.
Methods
Seventy migraineurs were randomized to the CSMT or a placebo, with 12 intervention sessions over three months. The recommendations by CONSORT and the International Headache Society's Task Force on AEs in migraine RCTs were followed. A standardized reporting scheme designed for pharmacological RCTs was used, and the AEs were described as frequencies and percentages within each group. The 95% confidence intervals (CIs) for the percentages (absolute risk) of AEs in each group were calculated when possible. Attributable risk (%) and relative risk were calculated with the corresponding 95% CIs.
Results
AEs were assessed in 703 sessions, with 355 in the CSMT group and 348 in the placebo group. Local tenderness was the most common AE, reported by 11.3% and 6.9% of the CSMT group and the placebo group, respectively, and tiredness on the intervention day was reported by 8.5% and 1.4% of CSMT group and the placebo group, respectively. The highest attributable risk was for tiredness on the treatment day, 7.0% (CI 3.9–10.2%) which presented a relative risk of 5.9 (CI 2.3–15.0).
Conclusion
AEs were few, mild and transient, and severe or serious AEs were not observed.
Disclosure of Interest
None Declared
Migraine Preventive Therapy
PO-01-057
Sustained Reduction in Chronic Migraine following Occipital Nerve Decompression Surgery: Further Implications for Extracranial Origin of Headache
Pamela Blake1,*, Carlton Perry2 and Rami Burstein3
1Memorial Hermann Medical Group
2River Oaks Plastic Surgery Center, Houston
3Neuroscience, Harvard Medical School, Boston, United States
Objectives
We aimed to determine if Nerve Decompresion Surgery (NDS) of the bilateral lesser and greater occipital nerves (bLON/GON) would reduce the burden of chronic migraine (CM). CM afflicts nearly 5% of the 36 million Americans with migraine. A subset of individuals with CM experience chronic occipital headache with chronic tenderness of suboccipital neck muscles and soft tissue. Recently a subset of these patients who underwent NDS for alleviation of their daily headaches also underwent biopsy of the occipital periosteum, and these biopsies were characterized by upregulation of proinflammatory genes. As animal studies have demonstrated that compression of peripheral nerves can cause local inflammatory changes, we hypothesized that compression of bLON/GON and may be the cause of the observed inflammtion, and that NDS may reduce inflammation and associated CM.
Methods
Eightees patients with CM and predominantly occipital pain underwent NDS of the bLON/GON. Twenty-three patients identified in a similar time frame with similar headaches who were referred for NDS but unable to undergo the procedure served as a control group. Log recordings of headache frequency and intensity were obtained for three months prior to surgery and for six months post-operatively. NDS included removal of compressive portions of trapezius and semispinalis capitis muscles and their fascial attachments, as well as perineural inflammatory tissue.
Results
No adverse events were associated with the outpatient surgical procedure. At study entry, the number of predominantly occipital CM days per month was 30 for subjects assigned to the control group, and 29.17 for subjects in the surgical group. In follow-up at mean of 46 months following study entry, the number of occipital CM days per month was 30 for the control group and 7.28 for the surgical group. Statistical analysis of the date was performed using a non-paramtric, two tailed Wilcoxon signed-rank test. The change in the number of headache days per month before and after surgery in the sugical group was statistially significant (p < 0.001), and the difference between the control group and the surgical group at follow-up was also statistically significant (p < 0.0001). More than 50% of surgical subjects experienced a >50% reduction in headache days.
Conclusion
Decompression of bLON/GON reduces headache burden in some patients with CM, most likely through a mechanism of reducing inflammation in the molecular environment surrounding periosteal pain fibers. This study provides further benefit for localized extracranial pathophysiology in CM, and also reports an effective treatment option for some patients with predominantly occipital CM.
Disclosure of Interest
P. Blake: None Declared, C. Perry: None Declared, R. Burstein Conflict with: Trigemina, Allergan, Teva, DepoMed, Dr, Reddy, SST, Conflict with: ATI
Migraine Preventive Therapy
PO-01-058
Cognitive Tolerability with Once-Daily Trokendi XR® (extended-release topiramate) vs. Immediate-Release Topiramate
Welton O'Neal1,*, Elizabeth E. Hur1, Tesfaye Liranso1, Peri Barr2, Haechung Chung3, Tao Gu3, Ozgur Tunceli3 and Ralph M. Turner3
1Supernus Pharmaceuticals, Inc., Rockville, MD
2iTTM Indegene, Kennesaw, GA
3Healthcore, Inc., Wilmington, DE, United States
Objectives
In studies of immediate-release topiramate (TPM-IR) dosed BID, migraineurs demonstrated greater susceptibility to TPM-related adverse events (AEs), particularly cognitive dysfunction, vs. patients with epilepsy. Trokendi XR® (extended-release topiramate, Supernus Pharmaceuticals, Inc.) is a novel, extended-release formulation producing more constant steady-state TPM plasma concentration-time profiles with QD dosing than TPM-IR BID. We report a series of studies suggesting the potential for better cognitive outcomes with Trokendi XR vs. TPM-IR.
Conclusion
Multiple datasets comparing Trokendi XR and TPM-IR suggest the potential for improved cognitive tolerability of Trokendi XR vs. TPM-IR, which may positively impact persistence. Additional prospective studies and analyses of additional datasets are needed to confirm these observations. Studies funded by Supernus Pharmaceuticals, Inc.
Disclosure of Interest
W. O'Neal Conflict with: Supernus Pharmaceuticals, Inc., E. Hur Conflict with: Supernus Pharmaceuticals, Inc., T. Liranso Conflict with: Supernus Pharmaceuticals, Inc., P. Barr Conflict with: Supernus Pharmaceuticals, Inc, H. Chung Conflict with: Supernus Pharmaceuticals, Inc, T. Gu Conflict with: Supernus Pharmaceuticals, Inc, O. Tunceli Conflict with: Supernus Pharmaceuticals, Inc, R. Turner Conflict with: Supernus Pharmaceuticals, Inc
Migraine Preventive Therapy
PO-01-059
Retrospective Claims-Based Comparative Health Outcomes Study: Trokendi XR® (extended-release topiramate) vs. Immediate-Release Topiramate as Migraine Preventives
Welton O'Neal1,*, Elizabeth E. Hur1, Tesfaye Liranso1, Haechung Chung2, Tao Gu2, Ozgur Tunceli2 and Ralph M. Turner2
1Supernus Pharmaceuticals, Inc., Rockville, MD
2Healthcore, Inc., Wilmington, DE, United States
Objectives
Effective preventives such as topiramate (TPM) can significantly reduce migraine disability, although clinical usefulness is often limited by issues of patient acceptance/adherence and tolerability. Trokendi XR® (extended-release topiramate, Supernus Pharmaceuticals, Inc.) is a novel, extended-release formulation producing more constant steady-state TPM plasma concentration-time profiles with QD dosing than immediate-release (IR) TPM dosed BID. Studies in healthy volunteers and migraineurs signaled potential for improved cognitive tolerability with Trokendi XR, which could enhance adherence/persistence with TPM therapy. A retrospective study using a large national claims database compared outcomes with Trokendi XR and TPM-IR.
Methods
This retrospective study used medical and pharmacy administrative claims data from the HealthCore Integrated Research Database. Inclusion criteria encompassed patients that were entered into the database between August 1, 2013 to October 31, 2014 (i.e. intake period = treatment initiation/first [index] pharmacy claim for Trokendi XR or Topamax® or generic TPM-IR). Other inclusion criteria: ≥6 yrs of age at index prescription; ≥12 months of continuous pre-index health plan enrollment; ≥6 months continuous health plan post-index enrollment; ICD-9 code for migraine (346.xx). Continuous TPM therapy was defined as <45 day gap in medication possession. Post-index claims for complications potentially related to TPM treatment were proxies for treatment-related adverse events (TEAEs) resulting in medical care.
Results
Total migraine patients meeting eligibility criteria: N = 9,219 (TPM-IR, 8596; Trokendi XR, 468). Chronic migraine patients comprised a substantially larger proportion of Trokendi XR cohort (35%) vs. TPM-IR (10%). Mean (SE) estimated time to discontinuation for patients on Trokendi XR was 7.7 (0.36) months compared to TPM-IR, 6.4 (0.08) months (p < 0.001). Difference between Trokendi XR and TPM-IR emerged within the first 2 months and persisted throughout the observation period. Medication possession ratio (MPR) and adherence (≥80% MPR) were significantly (p < 0.001) higher in the Trokendi XR cohort. In patients treated continuously for ≥6 months (TPM-IR, n = 3118; Trokendi XR, n = 217), the mean change in average monthly migraine events per patient significantly favored Trokendi XR over TPM-IR (p = 0.01 with pre-index count as covariate), as did healthcare utilization measured as outpatient visits (p < 0.001) and prescription drug use (p < 0.001). Occurrence rates for cognitive effects and paresthesia resulting in medical care were lower in the Trokendi XR cohort.
Conclusion
In this claims-based study, Trokendi XR was associated with significantly better outcomes vs. TPM- IR, manifested as significantly higher persistence – a composite measure of effectiveness, tolerability, and adherence. A key advantage of Trokendi XR may be in the early phase of treatment – as TPM therapy is initiated – producing a more favorable trajectory for persistence with TPM therapy. Analyses of larger datasets are needed to confirm these findings. Study funded by Supernus Pharmaceuticals, Inc.
Disclosure of Interest
W. O'Neal Conflict with: Supernus Pharmaceuticals, Inc., E. Hur Conflict with: Supernus Pharmaceuticals, Inc., T. Liranso Conflict with: Supernus Pharmaceuticals, Inc., H. Chung Conflict with: Supernus Pharmaceuticals, Inc, T. Gu Conflict with: Supernus Pharmaceuticals, Inc, O. Tunceli Conflict with: Supernus Pharmaceuticals, Inc, R. Turner Conflict with: Supernus Pharmaceuticals, Inc
Migraine Preventive Therapy
PO-01-060
GAS (Group A Streptococcus) induces migraine
Tadashi Matsuda1,*
1Misato Family Clinic, Misato-shi, Saitama, Japan
Objectives
GAS infection sometimes induces severe splitting headache. Especially in adults, strong headache would be more recognized than sore throat or any other symptoms.
Goreisan (GR) and Goshuyuto (GS) are famous Kanpo medicine (Japanese traditional medicine derived from natural herbs) against migraine, then we have reported combination therapy with GS and GS are mostly effective to primary headache within 10 minutes.
Methods
We have already noticed this intervention could be effective to headache accompanied by GAS infection, but not effective to headache accompanied by influenza at all. We have speculated different mechanisms which trigger headache between GAS infection and influenza. Characteristics of headache induced by GAS infection resemble migraine well.
On the other hand, first attack of migraine would be occurred around 5 years old. GAS infection would also be firstly encountered at the same age. Susceptible age for both migraine and GAS infection is similar, besides interestingly, as to migraine patients less than 10 years old, boys are slightly predominant over girls, which is also the same gender difference of GAS infection.
Results
We would present two typical cases below.
Case 1. 4 year - 10 month - male
Past History; infantile colic, had been treated with Kanpo medicine (Kanbakutaisoutou)
Family History; mother, two elder brothers and one elder sister have had migraine.
Present illness;
4 years 1 month; First GAS infection
4 years 3 months; First attack of splitting headache treated with Kanpo medeicine. Since then headache attack with nausea occurred several times, which had been diagnosed migraine.
4 years 10 months; He had high fever (39.1°C), abdominal pain, nausea and migraine attack. Since his Strep test was positive, he was given antibiotics and Kanpo medicine simultaneously. His headache successfully disappeared within 10 minutes after intervention.
Case 2. 41-year-old female
At age of 12, she had been diagnosed migraine with aura.
Up to 24 years old, she had suffered from migraine attack frequently. Especially taking red wine and cheese had triggered migraine attack within a few minutes.
Since age of 30 she had never taken wine or cheese, as a result she has been free from migraine attack.
At age of 41, she had visited our clinic with strong splitting headache, sore throat and slight fever (37.5°C). Her Strep test was positive. GR and GS had been given to her, 10 minutes later her headache had been completely disappeared. She has recognized her headache was migraine later, because she had not experienced migraine attack for more than 10 years.
Conclusion
GAS infection induces migraine. If we could get vaccine against GAS infection, it could reduce morbidity of migraine.
Disclosure of Interest
None Declared
Migraine Preventive Therapy
PO-01-061
Clinical characteristics of the patients with migraine in whom Goshuyutou is effective
Yasushi Shibata1,*
1Neurosurgery, University of Tsukuba, Mito, Japan
Objectives
Goshuyutou is a traditional Chinese medicine that is effective for the management of chronic headache. However, no large clinical scientific study of goshuyutou has yet been reported. We use Western medicines as the first choice for treating migraine at present, however, for many patients, their headache is uncontrollable with typical Western medicines. We prescribed goshuyutou for such patients with chronic migraine. The purpose of this study is to investigate the clinical characteristics of the migraine patients in whom goshuyutou is effective.
Methods
We examined 20 patients (5 men and 15 women) who were diagnosed with migraine and prescribed goshuyutou at our headache clinic. The patient age ranged from 14 to 63 years old. The migraine diagnosis was based on the International Classification of Headache Disorders 3β and was made by a single physician (author) on the Board of the Japanese Headache Society and certified as a headache master by the International Headache Society. Secondary headache was missed in most patients, even with appropriate examinations, including computed tomography (CT) or magnetic resonance imaging (MRI). Several patients had accompanying disease, but the cause of headache was diagnosed as migraine.
We prescribed triptan for all patients. In Japan, five brands of triptan are available, so if one triptan was not effective, another brand was prescribed. For patients with frequent migraine attack (more than four times per month), preventive medication was also prescribed. Our first choice of preventive medication is 10 mg of lomerizine hydrochloride (Migsis®), because no major side effects have been observed. If this prescription was not effective, we increased the dose of lomerizine hydrochloride or added 5–10 mg of amitriptyline (Tryptanol®). The clinical effects of these preventive medications were evaluated for several months. For patients with intractable migraine attack, we added 5–7.5 g of goshuyutou. Western medications were basically continued at the same doses. At one month after the start of goshuyutou, the clinical effects of goshuyutou were evaluated by the patients themselves. We interviewed the patients who did not visit our clinic by telephone. The clinical effects were classified as very effective (headache disappeared), effective (frequency or intensity of headache decreased) and no effect (no change).
Results
The headache did not disappear after one month of goshuyutou medication in any patients. However, the intensity or frequency of the headache improved in 13 patients. No effect was observed in 4 patients. Three patients did not visit the clinic after the medication or could not be contacted by phone. Therefore, the final effective rate was 76%. All patients continued to take preventive drugs and triptan.
There were no marked differences in the age or sex between the effective and ineffective groups. Neck pain, shoulder stiffness, nausea, photo sensitivity, phono sensitivity, family history of migraine, medication overuse headache and coldness of extremities were observed in both groups.
The effective group tended to have low migraine frequency and a long migraine history; however, because of the small number of patients, Mann Whitney test demonstrated no significant differences (p < 0.05). Five patients in the effective group had aura; however, no patients in the ineffective group had aura. Menses-related migraine was observed in 1 of 3 female patients in the ineffective group and 6 of 10 female patients in the effective group.
Conclusion
Goshuyutou was effective for the patients with aura and menses-related migraine.
Disclosure of Interest
None Declared
Migraine Preventive Therapy
PO-01-062
Onabotulinumtoxin A for Chronic Migraine with Medication Overuse: clinical results of a long-term treatment
Licia Grazzi1,*, Frank Andrasik2, Domenico D'Amico1, Matilde Leonardi1, Alberto Raggi1 and Emanuela Sansone1
1Neurological Institute C. Besta IRCCS, Milano, Italy
2University of Memphis, Memphis, United States
Objectives
The use of OnaBotulinumtoxin A (BonTA) as treatment of different neurological conditions is always more common in the last decades; its application has been consolidated on the basis of the significant results according to the results of the PREEMPT studies. The possibility for patients to be treated with a second cycle of therapy after the first year of treatment is under discussion, in particular for patients who obtained significant clinical benefit from the first period of treatment. In this report a group of patients, treated with BonTA for one year according to the PREEMPT, has been retreated for one more year in order to confirm the clinical benefit obtained after the first year of treatment.
Methods
A first group of 50 patients, 8 male; 42 females, mean age 51.2 ± 9.0; onset of
migraine18.2 ± 8.3, suffering from Chronic Migraine with Medication Overuse (CM)
according to HIS criteria
Results
16 patients, 15 females,1 male, (mean age 52.5 ±9.9; onset of migraine 15.4 ± 3.9) were submitted to a second period of treatment for one more year, are encouraging: they evidenced a significant decrease of days of headache per month at one year and the results were confirmed after 2 years of treatment: (25.3 ± 6.1 baseline vs 15.1 ± 7.8 at one year vs 15.5 ± 8.7 at 2 years) and also a significant decrease of medication intake per month (23.8 ± 6.8 baseline vs 13.8 ± 7.68 at one year vs 15.8 ±8.48 at 2 years). Patients did not report any side effect and they considered the treatment safe and well tolerated, although we did not record these indexes specifically.
Conclusion
In preceding studies it has been demonstrated the efficacy and safety of BonTA in CM over a period of 24 months and also at different dosages, higher than 155 U well tolerated. In terms of mean reduction of days of migraine and medication consumption, our clinical experience, show significant results even if the dosage was limited to 155 over a period of 24 months. The treatment was safe and well tolerated. Patients adherence to treatment was high, no missed appointments and side effects (usually reported from oral prophylaxis as weight gain, somnolence, fatigue, hypotension) were not recorded during the course of treatment. All patients were able to manage the medication intake, without relapses of medication overuse in absence of other prophylaxis for their migraine. BonTA seems to be effective for patients with CM, in particular the long duration of action and favourable adverse events make it a suitable therapeutic alternative for those patients not compliant with oral preventive medications. The application of BonTA is indicated also in the early stage of the disease and this may result in better treatment outcome. Although our results are preliminary, as the limited group of patients retreated, they led to intense efforts to evaluate analgesic properties of BonTA and to assess its clinical applicability for period longer than one year.
Disclosure of Interest
None Declared
Migraine Preventive Therapy
PO-01-063
Effects of high-intensity interval training versus moderate continuous aerobic exercise training on attack frequency and microcirculation in episodic migraine: A randomized controlled trial (RCT)
Alice Minghetti1,*, Lars Donath1, Till Sprenger2, Stefano Magon3, Athina Papadopoulou3, Henner Hanssen1, Oliver Faude1 and Lukas Zahner1
1Department of Sport, Exercise and Health, University of Basel, Basel, Switzerland
2Department of Neurology, Wiesbaden, Germany
3Department of Neurology, University Hospital Basel, Basel, Switzerland
Objectives
Migraine is a highly prevalent and disabling neurological disease. The objective of this study was to elucidate whether different aerobic exercise programs at high vs. moderate exercise intensities distinctly affect migraine frequency and retinal vessel parameters using a three-armed RCT. Effects of different exercise modalities on migraine and retinal vessel diameters have not been systematically studied.
Methods
24 migraineurs were enrolled in the present RCT (20 female, 4 male, age: 36.4 (11.0), BMI: 22.9 (4.0), migraine days: 4.6 (2.6)). Participants were randomly assigned to either high intensity interval training (HIT), moderate continuous training (MCT) or the control group (CON). Both intervention groups trained twice a week during a 12 week intervention period. HIT followed a 4×4 interval program alternating between 4 minutes at 90% followed by 3 minutes at 70% HRmax while MCT ran at 70% HRmax for 45 minutes. Both training regimen were equicalorically adjusted. In total, 24 training sessions were conducted. CON received no exercise intervention. The primary outcome was the number of migraine days recorded during the last 4 weeks of the training intervention compared to the 4-week run in period.

Results
Large effects of both interventions on migraine days with more pronounced effects in favor of HIT compared to MCT were observed (see Table). Retinal AVR improved with a large time × group interaction (ηp2, = 0.14) in favor of HIT vs. MCT (HIT: pre: 0.89 (0.06), post: 0.92 (0.07), SMD = 0.46); MCT: pre: 0.85 (0.07), post: 0.86 (0.07), SMD = 0.25), whereby the increase of AVR in HIT is attributed to a pronounced increase in arteriolar diameters (CRAE pre: 188.0 (17.2), post: 192.8 (20.0), SMD = −0.26) while MCT revealed a constriction of venules (CRVE pre: 234.7 (8.5), post: 230.0 (9.6), SMD = 0.52).
Conclusion
Both exercise intensity modalities resulted in significant reductions of migraine days and headache days in migraineurs. HIT is a safe training modality for migraineurs showing more pronounced effects on migraine attack reduction, cerebrovascular health indices and maximal oxygen uptake compared to MCT. Thus, supervised aerobic exercise should be considered a complementary preventive and treatment strategy for migraineurs.
Disclosure of Interest
None Declared
Migraine Preventive Therapy
PO-01-064
Improved efficiency of a nurse–led Migraine Botox service by implementation of a ‘lean’ management approach
Siobhan Jones1,*, Adam Zermansky1, Jared Szpakowski1, Paul Button2 and Julie Button2
1Greater Manchester Neuroscience Centre, Salford Royal NHS Foundation Trust, Salford
2ProcEx Solutions Ltd, Wales, United Kingdom
Objectives
Demand for Botox treatment for chronic migraine is increasing, resulting in pressure on the service. In 2015 we had an increasing waiting list of 35 patients with a wait time of approximately 4–6 months. Botox was administered by several consultants and a clinical nurse specialist, often in ad-hoc clinics. Appointment time-slots were 30 minutes per patient. The challenge faced in 2016 was to substantially increase the number of patients receiving Botox without additional resources. The main objective was to develop a standardised approach for Botox clinics enabling the highest level of efficiency resulting in an increased number of patients treated without increasing clinical staff, shifting the patient load from consultants to specialist nurse led service.
Methods
A 4-day assessment by a management-efficiency company [ProcEx Solutions Ltd] scrutinised every part of the patient pathway and consultation, and identified many opportunities for improvement. A few months later we participated in a 4-day kaizen (rapid improvement) event where we implemented the recommendations identified in the assessment. We were able to standardise the configuration of our clinic set up utilising lean techniques. We categorised patients as ‘runners’ (uncomplicated), ‘repeaters’ (more time-consuming, complex) and ‘strangers’ (new patients), which enabled implementation of a standardised patient pathway with fixed appointment times. The time allocated depended on the type of patient and whether the patient could be treated in a 15 minute or a 30 minute time slot. The table below illustrates the patient categorisation.

Results
There was an actual increase from 55 treatments per month in the first half of 2015 to 91 treatments per month in the second half of 2016. In 2015 we were able to treat a total of 28 new patients and this increased to a total of 63 new patients in 2016.
Conclusion
Implementation of these standardised practices has improved clinic efficiency, treating significantly more patients in the unit with the same number of staff. Furthermore, it facilitated a shift from consultant to nurse-led treatment, making it more cost effective. As a result of this, the waiting list has been eliminated and the wait time for treatment reduced from 4 months to 6 weeks. We continue to see an upward trend in treatment numbers.
Disclosure of Interest
S. Jones Conflict with: Allergan, A. Zermansky Conflict with: Allergan, J. Szpakowski: None Declared, P. Button Conflict with: ProcEx Solutions Ltd, Conflict with: Allergan, J. Button Conflict with: ProcEx Solutions Ltd, Conflict with: ProcEx Solutions Ltd, Conflict with: Allergan
Migraine Preventive Therapy
PO-01-065
Long-Term Safety and Tolerability of OnabotulinumtoxinA Treatment in Chronic Migraine Patients: COMPEL Analysis by Treatment Cycle
Paul K. Winner1, Andrew M. Blumenfeld2, Eric J. Eross3, Amelia Orejudos4, Aubrey Manack Adams4,* and Mitchell F. Brin4
1Palm Beach Headache Center Premiere Research Institute @Palm Beach Neurology, West Palm Beach
2Headache Center of Southern California, The Neurology Center, Carslbad
3The CORE Institute, Scottsdale
4Allergan plc, Irvine, United States
Objectives
The COMPEL study was a 108-week multicenter, open-label study designed to evaluate the efficacy and safety of onabotulinumtoxinA in adults with chronic migraine (CM). This analysis of the COMPEL data examines the safety and tolerability of onabotulinumtoxinA after each treatment cycle over a total of 9 cycles (108 weeks).
Methods
The COMPEL Study enrolled adults with CM. OnabotulinumtoxinA 155 U was administered every 12 weeks as 31 fixed site, fixed dose injections. The primary outcome was the reduction in headache day frequency per 28-day period at week 108 (after 9 cycles) compared to baseline. Safety and tolerability, overall and by treatment cycle, were assessed through the collection of data on the incidence and nature of adverse events (AEs), including serious AEs and those that occurred in patients who withdrew. AEs were based on patient reports at each follow-up visit, and physical examination, including vital signs, at screening, week 48 and 108. Patients were withdrawn from the study if suicidal ideation was identified or if pregnancy occurred. Any AE with a start day or an increase in severity in the period between successive treatments was attributed to the preceding treatment. The safety population consisted of all patients who received ≥1 dose of onabotulinumtoxinA.
Results
Of 716 patients enrolled in the study, the majority were Caucasian (81%), women (84.8%), and had a mean (SD) age of 43 (11.3) years. Patients typically had a family history of migraine (62.7%) and a mean (SD) time since onset of 10.6 (11.0) years. 373 patients (52.1%) completed the study and 343 (47.9%) withdrew. The primary reasons for discontinuation were withdrawal of consent (n = 92, 12.8%), loss to follow-up (n = 82, 11.5%) and protocol violation (n = 60, 8.4%). Overall, 481 patients (67.2%) received 60 weeks of treatment; 402 (56.1%) received 108 weeks. OnabotulinumtoxinA met the primary endpoint of significantly reducing headache day frequency (n = 715) by 10.7 (6.4) days, P < 0.0001 at week 108 from a baseline mean (SD) of 22 (4.8) days. AEs were reported by 436 patients (60.9%), most of which were mild to moderate in severity. 32 patients (4.5%) discontinued the study after experiencing AEs. 6 women became pregnant and discontinued from the study. The incidence of AEs tended to decrease with repeated onabotulinumtoxinA treatment; 24.2% after the first cycle, 18.4% after the fourth and 12.2% after the ninth (last). Neck pain (2.7%), eyelid ptosis (1.8%), musculoskeletal stiffness (1.4%), injection-site pain (1.3%), and headache (1.3%) were the most common AEs after the first cycle. The incidence of these AEs tended to decrease with each subsequent onabotulinumtoxinA treatment cycle. Neck pain reduced from 2.7% to 0.2% after the last cycle; eyelid ptosis: 1.8% to 0.0%; musculoskeletal stiffness: 1.4% to 0.2%; injection site pain: 1.3% to 0.0%; and headache: 1.3% to 0.5%. 75 (10.5%) patients reported serious AEs. Treatment-related AEs were reported by 131 patients (18.3%), 1 of which was considered serious; 13(1.8%) withdrew.
Conclusion
The COMPEL study results demonstrated that when administered using a fixed dose, fixed-site paradigm over 108 weeks, onabotulinumtoxinA was well tolerated and no new safety signals were identified. The incidence of overall AEs and the most common individual AEs decreased with repeated administration of onabotulinumtoxinA.
Disclosure of Interest
P. Winner Conflict with: Allergan, Amgen, NuPathe, AstraZeneca, Avanir, Eli Lilly, Novartis, Conflict with: Allergan, Amgen, Supernus, Conflict with: Allergan, Avanir, Supernus, A. Blumenfeld Conflict with: Allergan, Pernix, Teva, Avanir, Depomed, Supernus, Conflict with: Allergan, E. Eross Conflict with: Allergan, Conflict with: Allergan, Avanir, Depomed and Pernix, Conflict with: Owner and President, Glia Sciences, Inc., A. Orejudos Conflict with: Allergan, A. Manack Adams Conflict with: Allergan, Conflict with: Allergan, M. Brin Conflict with: Allergan, Conflict with: Allergan
Migraine Preventive Therapy
PO-01-066
Real-Life Use of OnabotulinumtoxinA for the Symptomatic Treatment of Chronic Migraine: The Repose Study
Fayyaz Ahmed1,*, Charly Gaul2, Paolo Martelletti3, Juan Carlos Garcia-Monco4 and Aubrey Manack Adams5
1Spire Hesslewood Clinic and Hull York Medical School, Brough, United Kingdom
2Migraine and Headache Clinic, Koenigstein, Germany
3Sapienza University, Regional Referral Headache Centre, Rome, Italy
4Hospital de Galdakao, Vizcaya, Spain
5Allergan plc, Irvine, United States
Objectives
The REPOSE Study is a multi-center, prospective, non-interventional, observational, open-label study which aims to investigate the long-term real-life use of onabotulinumtoxinA for the treatment of symptoms of chronic migraine (CM) in adult patients in Europe. The effectiveness of onabotulinumtoxinA in a clinical setting was assessed, as were onabotulinumtoxinA treatment patterns and safety over the 2-year period.
Methods
Adult patients were enrolled into the study if they were prescribed onabotulinumtoxinA for CM and if they had not received any botulinum toxin for the 26 weeks before enrollment. Patients received onabotulinumtoxinA injections approximately every 12 weeks according to their physician’s usual practice, guided by the treatment recommendations outlined in the Summary of Product Characteristics. OnabotulinumtoxinA injection practices, Migraine Specific Quality of Life Questionnaire (MSQ), and headache-day frequency data were collected at baseline and at follow-up visits. Safety and tolerability of onabotulinumtoxinA was also assessed.
Results
Among 644 patients enrolled in the REPOSE Study, 633 patients from 78 centers across 7 European countries received at least one onabotulinumtoxinA dose. Patients had a mean (SD) age of 45.4 (12) years and were typically women (85.3%). Among the 633 patients, 3499 onabotulinumtoxinA treatments were administered. The mean dose of onabotulinumtoxinA per session (baseline up to treatment session 8) ranged from 152.6 U to 156.0 U (median, 155 U) across all treatment sessions. The mean number of injection sites per session (baseline up to treatment session 8) ranged from 31.2 to 31.5 (median, 31) sites across all treatment sessions. The mean number of headache days at baseline was 20.6. At each follow-up session (through follow-up session 8), patient-reported estimates of the number of days per month with headache (≥4 hours) were significantly reduced from baseline (P < 0.001 at each follow-up session). On the MSQ Role-Restrictive domain, the mean score at baseline was 29.3, and significant reductions from baseline were observed at each follow-up session (P < 0.001 at each follow-up session). Similar significant findings were observed at each follow-up session through week 8 for the MSQ Role-Preventive domain and the MSQ Role-Emotional domain. Among the 18.3% (116/633) of patients who reported an adverse drug reaction, most were of mild to moderate severity. The most frequently reported adverse drug reactions (>2%) were eyelid ptosis (n = 34/116, 5.4%), neck pain (n = 19/116, 3.0%), and musculoskeletal stiffness (n = 17/116, 2.7%). OnabotulinumtoxinA was well tolerated with no new safety signals identified.
Conclusion
Results from the REPOSE Study, which was conducted among 7 European countries, demonstrates that preventive treatment of CM with onabotulinumtoxinA in a longer-term (24-month) real-world setting sustains a reduction in the frequency of headache days and significantly improves quality of life relative to baseline. No new safety concerns were identified.
Disclosure of Interest
F. Ahmed Conflict with: Received honorarium for consultancy and lecturing from Allergan, Eneura, Electrocore and Novartis, which is paid to the British Association for the Study of Headache and the Migraine Trust, Conflict with: Allergan, C. Gaul Conflict with: Allergan Pharma, Ratiopharm, Boehringer Ingelheim Pharma, Lilly, Novartis Pharma, Desitin Arzneimittel, Cerbotec, Bayer vital, Hormosan Pharma, electroCore und Grünenthal, Reckitt Benckiser, Ratiopharm, TEVA. Employee: Migraine and Headache Clinic Königstein, Germany, P. Martelletti Conflict with: Allergan, Teva, Bayer, Conflict with: Allergan, Teva, Bayer, J. C. Garcia-Monco Conflict with: Allergan, A. Manack Adams Conflict with: Allergan, Conflict with: Allergan
Migraine Preventive Therapy
PO-01-067
Burden of illness among treated migraine patients with ≥4 headache days in the past month
Lulu Lee1, Jvawnna Bell2,*, Timothy Fitzgerald2 and Joshua M. Cohen3
1Kantar Health, LA
2Teva Pharmaceuticals, Malvern
3Teva Pharmaceuticals, Malvern, United States
Objectives
To determine the burden of illness among patients treated for migraine with ≥4 headache days in the past month.
Methods
The data source was the 2016 US National Health and Wellness Survey (NHWS; N = 97,503), a self-administered, nationally representative sample of adults (≥18 years). Respondents were included in this analysis if they self-reported a diagnosis of migraine, experienced ≥4 headache days in the past 30 days, and were currently using a prescription treatment for migraine. Using propensity score matching to reduce bias, respondents meeting the above criteria were matched with people without migraine on age, gender, comorbidities (Charlson Comorbidity Index), annual household income, education, insurance status, body mass index (BMI), and smoking status. Outcomes included mental health comorbidities, work productivity and activity impairment as measured by the Work Productivity and Activity Impairment Questionnaire (WPAI), health utilization in the past 6 months (i.e., healthcare provider (HCP) visits, emergency room visits, and hospitalizations), and estimated annual indirect and direct costs. Post-match, groups were compared using One-Way ANOVAs and chi-square tests on outcomes.
Results
There were 197 respondents in each cohort. A statistically significantly greater proportion of treated migraine patients reported being diagnosed with depression than non-migraine controls (58.4% vs. 27.9%, p < 0.001). A greater portion of treated patients also reported being on long-term disability compared to non-migraine controls (13.7% vs. 5.6%,p < 0.003). Treated migraine patients reported greater losses in work productivity and increases in activity impairment. Compared to non-migraine controls, treated patients experienced greater absenteeism (11.8% vs. 6.3%, p = 0.03), presenteeism (36.0% vs. 17.5%, p < 0.001), overall work impairment (40.9% vs. 20.9%, p < 0.001), and activity impairment (45.4% vs. 25.4%, p < 0.001). These patients also reported more HCP visits (7.55 vs. 4.43, p < 0.001) and ER visits (0.48 vs. 0.25, p = 0.030) compared to non-migraine controls in the previous 6 months. Greater work productivity loss among treated migraine patients resulted in higher estimated annual indirect costs ($14,770.57 vs. $5,764.93, p < 0.001) compared to non-migraine patient controls. Treated migraine patients utilized more healthcare services than non-migraine patients ($24,499.90 vs. $15,318.91, p = 0.013).
Conclusion
The overall burden associated with migraine is substantial despite the availability of treatment options. Migraine patients in this survey reported a higher percentage of depression, long-term disability, work productivity loss, absenteeism, presenteeism, activity impairment, and use more health care services compared to people without migraine. As a result, patients treated for migraine incurred substantially greater direct and indirect costs compared to non-migraine controls.
Disclosure of Interest
L. Lee Conflict with: Kantar Health, J. Bell Conflict with: Teva Pharmaceuticals, T. Fitzgerald Conflict with: Teva Pharmaceuticals, J. Cohen Conflict with: Teva Pharmaceuticals
Migraine Preventive Therapy
PO-01-068
The impact of headache free days on quality of life and costs among people with migraine with ≥4 headache days in the past month
Lulu Lee1, Jvawnna Bell2,*, Timothy Fitzgerald2 and Joshua M. Cohen2
1Kantar Health, LA
2Teva Pharmaceuticals, Malvern, United States
Objectives
To determine the relationship between quality of life measures and headache free days (HFDs) among patients with ≥4 headache days in the past month. This patient population is at risk of progressing to chronic migraine, which is defined as ≥15 headache days per month. Increasing the number of HFDs may substantially improve a patient’s quality of life
Methods
The data were drawn from the 2016 US National Health and Wellness Survey (NHWS; N =97,503), a self-administered, nationally representative sample of adults (≥18 years). Patients who indicated they were diagnosed with migraine and reported experiencing ≥4 headache days a month were considered at risk for progressing to chronic migraine. Multivariable analyses were conducted in this subgroup of patients. The primary independent variable was the number of HFDs as both a continuous (30 minus number of HFDs in the past 30 days) and categorical (0–10, 11–20, and 21–26 HFDs) measure. Each measure was used as a predictor in separate generalized linear models (GLMs).
Outcomes included patient reported number of days absent from work and days of household activities missed due to migraine, estimated annual indirect costs due to work productivity loss (assessed via Work Productivity and Activity Impairment Questionnaire [WPAI]) and estimated annual direct costs from healthcare resource use (healthcare provider visits, emergency room visits, and hospitalizations). The Headache Impact Test (HIT-6), a measure of the effect of headaches on daily life, was also assessed.
Results
Using HFDs as a continuous variable in the multivariable regression, each HFD was found to be associated with a 0.15 (regression coefficient) point reduction in HIT-6 scores. As a categorical variable, each 10 day increase in HFDs was associated with significantly lower HIT-6 total scores (adjusted means = 66.59 [0–10 HFDs], 65.66 [11–20], 63.91 [21–30], all p < 0.02).
Each HFD was associated with 0.95 (Rate Ratio [RR]) times days of work missed due to migraines and 0.95 (RR) times days of household activities missed due to migraines. In other words, each HFD reduces both number of work days missed and number of days of household activities missed by 5%.
Increasing the number of HFDs from 0–10 to 21–26 (adjusted means = 4.44 vs. 1.46, p = 0.002) and from 11–20 to 21–26 (3.36 vs 1.46, p = 0.009) categories was associated with significantly fewer work days missed due to migraine. Similarly, increasing the number of HFDs from 0–10 to 11–20 (adjusted means = 22.99 vs. 9.72, p < 0.001) and from 0–10 to 21–26 (22.99 vs. 7.34, p = 0.001) categories was associated with significantly fewer days of household activity missed due to migraine.
In terms of costs, increasing HFDs did not significantly reduce direct costs (means for 0–10 HFDs = $20,171; 11–20 HFDs = $20,954; 21–26 HFDs = $23,268). However, increasing the number of HFDs from 0–10 to 21–26 per month was associated with significantly lower indirect costs (adjusted means = $16,975 vs. $6,919, p = 0.025).
Conclusion
Increasing the number of HFDs is associated with an increase in quality of life among
patients suffering from migraine and at risk for developing chronic
migraine
Disclosure of Interest
L. Lee Conflict with: Kantar Health, J. Bell Conflict with: Teva Pharmaceuticals, T. Fitzgerald Conflict with: Teva Pharmaceuticals, J. Cohen Conflict with: Teva Pharmaceuticals
Migraine Preventive Therapy
PO-01-069
Preliminary Data on Exogenous Ketone Bodies in Migraine Prevention
Elena C. Gross1,*, Peter Sandor2 and Dirk Fischer3
1Neurology, University Children's Hospital Basel, Basel
2RehaClinic Kantonsspital Baden, Baden
3Neuropediatrics, University Children's Hospital Basel, Basel, Switzerland
Objectives
Currently available prophylactic migraine treatment options are limited and are associated with many – often intolerable - side-effects. Various lines of research suggest that abnormalities in energy metabolism are likely to be part of migraine pathophysiology. Previously, fasting or a ketogenic diet (KD) have been reported to lead to a drastic reduction in migraine frequency. An alternative method to a strict KD is inducing a mild nutritional ketosis (0.4–1 mmol/l) with exogenous ketogenic substances. The aim of this open label pilot study was to 1) assess the pharmacokinetics of a one-time dose of 10 g beta-hydroxybutyrate (βHB) – one of the three physiological ketone bodies - in mineral salt form and 2) the effect of a one month supplementation with daily 20 g βHB on migraine days compared to a one month baseline period.
Methods
Five treatment refractory patients (age range: 25–61 years, 1 male, attack frequency range: 6–24 migraine days/months) received 20 g/day of sodium and calcium βHB (n = 5) in two oral doses for the duration of 4 weeks. Blood βHB and glucose concentrations were assessed using an Abbot Freestyle Neo blood ketone and glucose meter once a week in a fasted state at 3 different time points: before βHB (baseline) and 30 mins and 60 mins after ingestion.
Results
10 g βHB (n = 5) lead to a quick elevation in blood βHB levels (peak 0.62 mmol/l after 1 hour, SEM = 0.08). No serious side-effects were reported. Adverse events observed included diarrhoea, nausea or gastrointestinal upset. These led to one drop-out. During the one month of intervention with 20 g of βHB per day, an average reduction of 51% in migraine days compared to baseline could be observed (mean baseline = 16.25 days, SEM = 3.71; mean after βHB = 8 days, SEM = 2.92). This perceived benefit from βHB seemed to coincide with a drop in average peak βHB blood levels from 0.62 mmol/l to 0.3 mmol/l after 1–2 weeks of ingestion.
Conclusion
The drop in average peak βHB blood levels after 1–2 weeks of ingestion is likely to be a consequence of adaptation, enabling a quicker uptake and usage of βHB. While it is too early to draw any conclusions from this case series, these preliminary results might warrant the conduction of a randomised, placebo-controlled, double-blind efficacy and safety trial to assess the potential of exogenous ketogenic substances in migraine prevention.
Disclosure of Interest
None Declared
Migraine Preventive Therapy
PO-01-070
A randomized controlled clinical trial on the efficacy of acupuncture for migraine prophylaxis: the ACUMIGRAN study
Sabina Cevoli1,*, Giulia Giannini2, Valentina Favoni2, Annunzio Matrà3, Carlo M. Giovanardi3, Giulia Pierangeli2 and Pietro Cortelli2
1IRCCS Istituto delle Scienze Neurologiche, Bologna, Italy
2Department of Biomedical and NeuroMotor Sciences (DiBiNeM), Alma Mater Studiorum – University of Bologna Italy, IRCCS Istituto delle Scienze Neurologiche
3Associazione Medici Agopuntori Bolognesi (AMAB) study group, Scuola Italo-Cinese di Agopuntura Italy, Bologna, Italy
Objectives
The efficacy of acupuncture for migraine prophylaxis still remains controversy [1–3]. The aim of our study was to evaluate the non-inferiority of acupuncture compared to that of pharmacological treatment as prophylaxis for migraine with and without aura.
Methods
This is a randomized controlled clinical study. Patient suffering from migraine without preventive treatment in the past three months were recruited. After the run-in period episodic migraineurs were assigned randomly to two groups: the acupuncture group (A) was treated with 12 sessions of acupuncture and the pharmacological group (B) was treated with the most appropriate medication for each patient. Headache frequency was compared at baseline and at the end of treatment.
Results
A total of 105 patients (19 males and 86 females) were enrolled in this study. Out of these, 52 were randomized at A and 53 at B. At baseline no significantly differences were found between the two groups. Of the overall sample 74 patients completed the protocol. After 4 months, the migraine frequency decreased from 9.19 ± 2.99 to 4.36 ± 2.66 in A and from 8.25 ± 2.53 to 4.44 ± 2.37 in B. Headache frequency decreased significantly after treatment without differences between the two groups (time-effect: p < 0.001; group effect: p =0.332; interaction time-group effects: p = 0.556). Responders (migraineurs with a reduction of headache days by at least 50%) were 35.71% in A and 31.25% in B (p = 0.687).
Conclusion
Our preliminary data suggest that acupuncture was as effective as pharmacological treatment in decreasing migraine frequency.
This study was funded by II Programma sperimentale regionale per l’integrazione delle MNC nel servizio sanitario dell’Emilia-Romagna.
References
1- Linde K, Allais G, Brinkhaus B, et al.
2- Chen J, Zhao L, Zheng H, et al.
Disclosure of Interest
None Declared
Migraine Preventive Therapy
PO-01-071
Magnesium in migraine prophylaxis – is there an evidence-based rationale? A systematic review
Alexander Von Luckner1 and Franz Riederer2,*
1Neurology, University Hospital Zurich, Zurich, Switzerland
2Neurology, Neurological Center Rosenhuegel, Karl Landsteiner Institute for Clinical Epilepsy Research and Cognitive Neurology, Vienna, Austria
Objectives
Magnesium plays a decisive role in intracellular energy production and neuronal excitability, which are critical factors in the pathophysiology of migraine. Experimental studies indicate reduced intracellular levels of magnesium in migraineurs. We performed a systematic review of randomized controlled trials investigating magnesium for migraine prevention.
Methods
Clinical trials published from 1990–2016 were sorted and analyzed in a structured selection procedure with regard to evidence and under consideration of the guidelines for controlled trials for drugs in migraine by the International Headache Society. The number of migraine days and number of migraine attacks were chosen as efficacy parameters.
Results
Out of 205 search results, 5 clinical trials fulfilling the selection procedure were found. One out of two Class I evidence trials showed a significant reduction of the number of migraine attacks compared to placebo, while two out of three Class III trials evinced a statistically significant reduction of the primary efficacy parameters compared to placebo.
Conclusion
This systematic review provides Grade C evidence for treatment of migraine with magnesium. Prophylactic treatment of migraine by means of high levels of magnesium dicitrate (600 mg) seems to be a safe and cost efficient strategy in clinical use.
Disclosure of Interest
None Declared
Migraine Preventive Therapy
PO-01-072
Sustained Reduction in Days Using Acute Medications with Fremanezumab (TEV-48125)
Rashmi Halker1,*, Ernesto Aycardi2, Marcelo Bigal2, Pippa Loupe3 and David Dodick1
1Neurology, Mayo Clinic, Scottsdale
2Teva Pharmaceuticals, Frazer
3Teva Pharmaceuticals, Overland Park, United States
Objectives
Fremanezumab, (formerly known as TEV-48125), a fully humanized monoclonal antibody that selectively binds to both isoforms of the CGRP ligand and prevents CGRP from binding to the CGRP receptor, has been shown to be effective for high-frequency episodic migraine (HFEM) and chronic migraine (CM) prevention. The sustained effect on acute medication use, which is a marker of migraine-related disability and a risk factor for migraine chronification, has not been previously reported.
Methods
Fremanezumab was evaluated in randomized, double-blinded, placebo-controlled 12-week phase 2 studies in patients with HFEM and CM. Participants allocated to fremanezumab received one of two dosing strategies: HFEM participants were randomized to receive monthly injections of 225 mg or 675 mg for 3 months; CM participants were randomized to receive either monthly injections of 900 mg, or an initial loading dose of 675 mg and subsequent injections of 225 mg for 3 months. An electronic headache diary captured headache-related data. Using post-hoc analyses, we determined the percentage of patients with at least a 50% and 75% reduction in the number of days requiring acute medication use at month 1 that continued to sustain this 50% or 75% reduction over 3 months.
Image:

Results
Figure 1 illustrates sustained 3-month response results in HFEM patients. Figure 2 illustrates sustained 3-month response results in CM patients.
Figure 1. HFEM: Sustained 3-month reduction in days using acute medications.
Figure 2. CM: Sustained 3-month reduction in days using acute medications.
Conclusion
As these findings are from post-hoc analyses, they must be interpreted with caution; nonetheless, significant percentages of patients on fremanezumab were able to demonstrate a sustained 3-month 50% and 75% reduction respectively in the use of abortive migraine medications. Given the importance of acute medication usage on disability and the risk of future progression, future trials should prospectively collect and report the percentage of study participants who are able to sustain a reduction in acute medication use over a meaningful period of time.
Disclosure of Interest
R. Halker: None Declared, E. Aycardi Conflict with: Dr. Aycardi is employed by Teva, M. Bigal Conflict with: Employed by Teva, P. Loupe Conflict with: Dr. Loupe is employed by Teva, D. Dodick: None Declared
Migraine Preventive Therapy
PO-01-073
The validity of wireless sensors for measurement of surface electromyography and skin temperature: Basis for a novel preventive headache treatment
Anker Stubberud1,*, Petter M. Omland1, Erling Tronvik1,2, Alexander Olsen3,4, Trond Sand1,2 and Mattias Linde1,2
1Department of Neuromedicine and Movement Science, NTNU Norwegian University of Science and Technology
2National Advisory Unit on Headaches, St. Olavs Hospital
3Department of Psychology
4Department of Physical Medicine and Rehabilitation, NTNU Norwegian University of Science and Technology, Trondheim, Norway
Objectives
Delivery of preventive biofeedback treatment to young migraineurs is a tedious and time-consuming undertaking, and it is unavailable to the majority of those in need, despite its effectiveness [1]. The aim of the present study was to assess the validity of Bluetooth compatible sensors for measurement of surface electromyography (SEMG) and peripheral skin temperature, in combination with a mobile phone application (app), as a basis for a novel, innovative mHealth delivery of biofeedback self-treatment for young persons with primary headache. This abstract presents data from the ongoing study.
Methods
Sensors fulfilling the three criteria (1) wireless setup, (2) small size and (3) low cost were identified. An iOS compatible application was programmed to communicate with the biosensors. Twenty healthy volunteers were recruited to use the biosensors through the app with simultaneous control measurements made with stationary neurophysiological equipment. SEMG sensors were attached to the right trapezius muscle and temperature sensors were attached to the right distal index finger. Investigations were made to assess agreement in change values for SEMG and temperature. Agreement between wireless and stationary SEMG sensors was assessed through the following activities: maximal voluntary contraction (MVC) of the trapezius muscle followed by submaximal voluntary contractions at 50% (VC50%) and 25% (VC25%) force. Similarly, agreement between wireless and stationary temperature sensors was investigated for the difference between room temperature and finger temperature.
Image:

Results
The app was programmed as a minimal viable product (MVP) to receive data from the wireless biosensors, to process this data and feed it back to the user through a simple interface. The app also allowed for viewing previous recorded sessions and extraction of data for analysis. Results from twelve participants (age 18–29 years) showed convincing visual agreement of muscle activation patterns. Root mean square (RMS) values were calculated for contraction periods. Table 1 shows ratio of RMS values between VC50% and VC25% for the stationary and wireless setup, indicating good consistency of agreement between stationary and wireless equipment. Table 1 also shows difference from room temperature to finger temperature in degrees Celsius for both temperature sensors.
Conclusion
Results indicate that wireless sensors may be suited to use as an integrated part of an app to monitor physiological parameters with the intention of biofeedback-treatment. The results also emphasize the general concept of using wireless sensors and apps to measure physiological parameters as useful and feasible.
Disclosure of Interest
None Declared
Migraine Preventive Therapy
PO-01-074
Effects of OnabotulinumtoxinA Treatment on Disability and Quality of Life in Patients with Chronic Migraine with Baseline Headache Every Day: A COMPEL Subanalysis
Jorge Ivan Lopez1,*, Andrew M. Blumenfeld2, William B. Young3, Aubrey Manack Adams4 and John F. Rothrock5
1University of Nevada, Reno School of Medicine, Reno
2Headache Center of Southern California, The Neurology Center, Carlsbad
3Jefferson Hospital for Neuroscience, Philadelphia
4Allergan plc, Irvine
5George Washington School of Medicine, Washington DC, United States
Objectives
Chronic migraine (CM) is a disease with varied attack frequency and pain symptoms. The objective of this subanalysis of the 108-week, multicenter, open-label COMPEL study addresses the efficacy and safety of onabotulinumtoxinA in CM patients with baseline compared with no baseline headache every day (HED).
Methods
Patients received onabotulinumtoxinA 155 U with/without concomitant prophylaxis. A subpopulation with baseline HED was assessed, which was defined as a diary entry of HED with an entry during the 28-day screening period. The primary outcome was the reduction in headache frequency per 28-day period at 108 weeks (9 treatments). Exploratory outcomes included, but were not limited to, scores for the Migraine Disability Questionnaire (MIDAS), with higher scores indicating greater disability; Migraine-Specific Quality of Life (MSQ), consisting of 3 subscales, Role Function Preventive, Role Function Restrictive, and Emotional Function, with higher scores indicating greater quality of life; and Patient Global Assessment of Treatment (PGAT), which assesses patient satisfaction with their treatment. Adverse events and their relatedness were recorded.
Results
In patients with baseline HED (N = 153) and without baseline HED (N = 562), onabotulinumtoxinA reduced 28-day headache frequency relative to baseline (week 60: HED, −7.9 ± 8.6; no HED, −10.7 ± 6.5; week 108: HED, −10.5 ± 9.4; no HED, −12.0 ± 6.8; between-group comparison for both timepoints P < 0.001). MIDAS scores were significantly decreased (improved) at week 60 (HED, −36.3 ± 69.4; no HED, −44.8 ± 51.4) and week 108 (HED, −44.8 ± 73.7; no HED, −44.0 ± 46.3; between-group comparison for both timepoints P < 0.001). Similarly, MSQ subscale scores improved from baseline at weeks 48, 96, and 108 (Role Function Preventive subscale scores: week 48, HED = 16.9 ± 23.1, no HED = 19.0 ± 20.1; week 96, HED = 16.3 ± 25.2, no HED = 19.7 ± 21.8; and week 108, HED = 15.0 ± 27.0, no HED = 19.2 ± 19.7, P < 0.001; Role Function Restrictive subscale scores: week 48, HED = 21.1 ± 25.6, no HED = 24.4 ± 21.4, P < 0.05; week 96, HED =24.2 ± 25.7, no HED = 27.0 ± 23.8; and week 108, HED = 25.5 ± 25.3, no HED = 26.3 ± 22.4; and Emotional Function subscale scores: week 48, HED = 22.1 ± 27.3, no HED = 24.9 ± 25.5; week 96, HED = 25.7 ± 29.6, no HED = 26.8 ± 26.0; and week 108, HED = 27.2 ± 28.2, no HED = 25.7 ± 25.8). Similarly in both groups, the proportions of patients who were extremely satisfied/satisfied (by PGAT) typically increased, and the proportions dissatisfied decreased. 3.3% HED and 1.4% non-HED patients who discontinued reported a treatment-related adverse event.
Conclusion
These results support the efficacy of onabotulinumtoxinA for reducing headache days and disability and improving quality of life for up to 108 weeks in CM patients with or without HED. Both groups had similar beneficial treatment effects, with a slightly greater benefit observed in patients without HED. No new concerns regarding safety were identified.
Disclosure of Interest
J. I. Lopez Conflict with: Dr. Lopez and his parent institution, Renown Health, have received clinical research funding from Allergan plc, Conflict with: Has served on the advisory boards for Alder, Allergan, Cipla, Lilly, and Supernus, A. Blumenfeld Conflict with: Allergan, Pernix, Teva, Avanir, Depomed, and Supernus, Conflict with: Received funding for travel, speaking, and/or royalty payments from Allergan, W. Young Conflict with: AGA, Alder, Allergan, Amgen, Autonomic Technology, Cumberland, Dr. Reddy Laboratories, Eli Lilly, Eneura Inc, Merz, and St. Jude Medical Consultant: Allergan and Supernus, A. Manack Adams Conflict with: Allergan, Conflict with: Allergan, J. Rothrock Conflict with: His parent institution has received funding from Allergan plc for clinical research he has conducted, Conflict with: has received honoraria from Allergan plc for participating as a speaker and preceptor at Allergan-sponsored educational programs
Migraine Preventive Therapy
PO-01-075
Effects of OnabotulinumtoxinA Treatment on Disability and Quality of Life in Patients with Chronic Migraine with Baseline Allodynia: A COMPEL Subanalysis
William B. Young1,*, J. Ivan Lopez2, John F. Rothrock3, Aubrey Manack Adams4 and Andrew M. Blumenfeld5
1Jefferson Hospital for Neuroscience, Philadelphia
2University of Nevada, Reno School of Medicine, Reno
3George Washington School of Medicine, Washington DC
4Allergan plc, Irvine
5Headache Center of Southern California, The Neurology Center, Carlsbad, United States
Objectives
Allodynia is common in the chronic migraine (CM) population. The presence of allodynia has been reported to reduce the likelihood of a positive response to migraine therapies. The objective of this subanalysis of the 108-week, multicenter, open-label COMPEL study is to evaluate the efficacy and safety of onabotulinumtoxinA in CM patients with baseline compared with no baseline allodynia.
Methods
Patients received onabotulinumtoxinA 155 U with/without concomitant prophylaxis. Based on the Allodynia Screening Questionnaire, a subpopulation with baseline allodynia was identified during the 28-day screening period. The primary outcome was the reduction in headache frequency per 28-day period at 108 weeks (9 treatments). Exploratory outcomes included but were not limited to scores for the Migraine Disability Questionnaire (MIDAS), with higher scores indicating greater disability; Migraine-Specific Quality of Life (MSQ), consisting of 3 subscales, Role Function Preventive, Role Function Restrictive, and Emotional Function, with higher scores indicating greater quality of life; and Patient Global Assessment of Treatment (PGAT), which assesses patient satisfaction with their treatment. Adverse events and their relatedness were recorded.
Results
In patients with baseline allodynia (N = 289) and without baseline allodynia (N = 426), onabotulinumtoxinA reduced 28-day headache frequency relative to baseline (week 60: allodynia, −9.9 ± 6.7; no allodynia, −10.3 ±7.3; week 108: allodynia, −10.8 ± 7.1; no allodynia, −12.5 ±7.4). MIDAS scores were significantly decreased (improved) at week 60 (allodynia, −48.6 ± 60.3; no allodynia, −38.9 ± 51.5; P < 0.05 between-group comparison) and week 108 (allodynia, −53.0 ± 50.3; no allodynia, −37.7 ± 53.0). Similarly, MSQ subscale scores improved from baseline at weeks 48, 96, and 108 (Role Function Preventive subscale scores: week 48, allodynia =19.8 ± 20.9, no allodynia = 17.6 ± 20.6; week 96, allodynia = 20.8 ± 23.1, no allodynia = 17.8 ± 22.0; and week 108, allodynia = 20.6 ± 21.9, no allodynia =16.9 ± 20.7; Role Function Restrictive subscale scores: week 48, allodynia = 26.5 ± 22.3, no allodynia =21.6 ± 22.1; week 96, allodynia = 28.9 ± 25.0, no allodynia = 24.6 ± 23.4; and week 108, allodynia =28.0 ± 23.3, no allodynia = 24.7 ± 22.7; and Emotional Function subscale scores: week 48, allodynia = 26.7 ± 26.4, no allodynia = 22.5 ± 25.3; week 96, allodynia =28.3 ± 27.0, no allodynia = 25.3 ± 26.5; and week 108, allodynia = 27.6 ± 26.5, no allodynia = 24.9 ± 26.1). Similarly in both groups, the proportions of patients who were extremely satisfied/satisfied (by PGAT) typically increased, and the proportions dissatisfied decreased. 2.1% allodynic and 1.6% non-allodynic patients who discontinued reported a treatment-related adverse event.
Conclusion
These results support the efficacy of onabotulinumtoxinA for reducing headache days and disability and improving quality of life for up to 108 weeks in CM patients with or without allodynia. Both groups had similar beneficial treatment effects, with a slightly greater benefit commonly observed in patients with allodynia despite its reported treatment-resistant phenotype. No new concerns regarding safety were identified.
Disclosure of Interest
W. Young Conflict with: AGA, Alder, Allergan, Amgen, Autonomic Technology, Cumberland, Dr. Reddy Laboratories, Eli Lilly, Eneura Inc, Merz, and St. Jude Medical Consultant: Allergan and Supernus, Conflict with: Has served on the advisory boards for Alder, Allergan, Cipla, Lilly, and Supernus, J. I. Lopez Conflict with: Dr. Lopez and his parent institution, Renown Health, have received clinical research funding from Allergan plc, J. Rothrock Conflict with: His parent institution has received funding from Allergan plc for clinical research he has conducted, Conflict with: has received honoraria from Allergan plc for participating as a speaker and preceptor at Allergan-sponsored educational programs, A. Manack Adams Conflict with: Allergan, Conflict with: Allergan, A. Blumenfeld Conflict with: Allergan, Pernix, Teva, Avanir, Depomed, and Supernus, Conflict with: Received funding for travel, speaking, and/or royalty payments from Allergan
Migraine Preventive Therapy
PO-01-076
Evaluation of the Effects of an Organic Light Emitting Diode Lighting Environment for Patients with Migraine
Muneto Tatsumoto1,*, Makoto Akashi2, Hiroshi Ohata3, Saiko Takaku3 and Koichi Hirata1
1Neurology, Dokkyo Medical University, Tochigi
2Research Institute for Time Studies, Yamaguchi University, Yamaguchi
3OLED Group, Research Division, Chemical Materials Evaluation and Research Base (CEREBA), Ibaraki, Japan
Objectives
This study aims to reduce migraine attacks for migraine patients caused by the uniform emitting surface of Organic Light Emitting Diode (OLED) lighting in their lives. We also sampled hair at the time of OLED lighting, identified the expression rhythm of the human clock gene (Per3), and investigated the correlation between headaches and the number of days’ drug is taken.
Methods
Subjects of the study were seven migraine patients residing in a room installed with OLED (3000K) and Light Emitting Diode (LED) (3000K) lighting. Ages were 20 to 22 years old. The study was first performed for a period of four weeks with LED lighting followed by another four weeks with OLED lighting. The method used was to investigate were headache conditions of the subjects (headaches, number of days taking drug), Beck Depression Inventory (BDI), Profile of Mood States (POMS), and Pittsburgh Sleep Quality Index (PSQI). The Unified Glare Rating (UGR) was calculated using a Luminance & Color Environment Photometric Tool (L-CEPT). The human clock gene (Per3) was measured by sampling hair four times a day every six hours, purifying the RNA from the attached hair follicle cells, and analyzing it with the real-time PCR method.
Results
The average number of days with a headache throughout the four weeks’ period with LED for the seven migraine patients was eight days, which was reduced to 6.9 days with OLED. The average number of days’drug was taken throughout the four week periods was 2.1 days with LED and 2 days with LED, showing no variation. The BDI average showed improvement for depression, from 3 with LED to 1.1 with OLED. The average Total Mood Disturbance score for POMS also showed improvement for mood, from 18.2 with LED to 16.4 with LED. The average of the total score for the PSQI showed an improvement for sleeping condition, from 3.6 with LED to 2.7 with OLED. The average sleep efficiency also rose from 91.9% with LED to 97.9% with OLED. Results of measuring with the L-CEPT showed that the UGR was higher with LED at 32.3 (begin to feel uncomfortable) when compared to OLED at 18.3 (begin to feel concerned). In addition, while both OLED (average 14 cd/m2) and LED (average 12.5 cd/m2) were mostly the same, the standard deviation (OLED 100.9 cd/m2, LED 427.1 cd/m2) and coefficient of variation (OLED 7.2 cd/m2, LED 34.2 cd/m2) displayed significant difference. In other words, OLED had a high spatial uniformity when compared to LED. The expression rhythm of the human clock gene (Per3) of hair follicle cells (performed on six subjects) was a correlated phase for three subjects, somewhat nocturnal for two subjects, and somewhat toward the morning for one subject. There was no relation between the Per3 gene expression rhythm, headaches, and the number of days medicine was taken.
Conclusion
As a result of setting the same lighting conditions (3000K) for both OLED and LED and examining whether there is an effect on migraine attacks, a change from LED to OLED reduced the number of days with a headache for migraine patients and improved depression, mood, and sleeping condition. The high spatial uniformity of OLED lighting was likely the cause for OLED lighting having improved migraine attacks. Results suggested that improving the lighting environment can possibly reduce migraine attacks.
Disclosure of Interest
None Declared
Migraine Preventive Therapy
PO-01-077
A comparison of approaches to model migraine day frequency in migraine
Richard B. Lipton1, Joshua K. Porter2, Neel Shah3,*, Sandhya Sapra3, Pooja Desai3, Guillermo Villa2, Alan Brennan4, Stephen Palmer5 and Jeroen Jansen6
1Albert Einstein College of Medicine, Bronx, NY, United States
2Amgen (Europe) GmbH, Zug, Switzerland
3Amgen Inc, Thousand Oaks, United States
4University of Sheffield, Sheffield
5University of York, York, United Kingdom
6Precision Health Economics, San Francisco, United States
Objectives
Efficacy of migraine prophylaxis is typically measured by its ability to reduce the frequency of migraine days (MD) per 28 days. A previous economic model of migraine prophylaxis stratified migraine patients into health states based on their headache day frequency per 28 days (0–3, 4–9, 10–14, 15–19, 20–23, 24–28). The aim of this analysis is to explore the performance of parametric distributions to model MD frequency continuously, in contrast to the traditional health state approach, based on the headache day definitions used previously.
Methods
Patient level data from a phase 2 study (NCT01952574) of erenumab 70 mg as prophylaxis in episodic migraine (EM) were used to compare the distribution of patients by MD frequency at each time point during the study double-blind phase and open-label extension up to 52 weeks, using three approaches: 1) the distribution of individual patients as observed in the study, 2) the split of patients across the six health states defined above, and 3) a beta-binomial distribution fit to the study observations.
The observed and beta-binomial distributions were used to generate a weighted average MD frequency for patients within each health state. The health state approach assumed that patients were uniformly distributed, and that the mean MD frequency in each health state was the midpoint of the defining range. Bootstrapped confidence intervals were generated to identify any significant differences between approaches.
The three approaches were used to estimate the mean MD frequency per 28 days for each health state and the overall mean frequency across 1 year of study follow-up.
Results
Data from 103 EM patients treated with 70 mg erenumab were available for at least one study visit, with 73 patients followed up to 52 weeks. A total of 83.4 patient-years of treatment were included in the analysis. Over 1 year, the mean frequency of MD observed was 56.6 (Bootstrapped 95% CIs: 54.1–59.3). The health state and beta-binomial approaches estimated 61.7 (59.1–64.3) and 56.7 (54.1–59.5) MD, respectively.
Observed mean MD frequencies for patients in the “0–3”, “4–9” and “10–14” MD health states were numerically lower than the health state midpoints; 1.4 (0.9–2.0), 5.9 (5.3–6.5) and 11.3 (10.0–12.4), respectively. Reliable estimates for the heath states with 15 + MD could not be generated, as these were not well represented in the EM study population.
Conclusion
The results of this analysis suggest that the use of a parametric distribution is able to provide accurate approximations of the MD frequency observed in the EM study dataset analyzed.
Modeling MD frequency as a continuous outcome, rather than as a series of categories, retains all of the observed information on the distribution of patients by MD frequency, and does not require arbitrary health states to be defined. Furthermore, it is possible to use the parametric distribution to populate health states, but the reverse is not true.
The continuous distribution approach may also offer additional advantages for economic evaluation. Firstly, it more readily allows for indirect comparisons based on study primary endpoints (e.g. change in MD frequency per 28 days). Secondly, the number of MDs and associated events (e.g. emergency room visits) can be directly quantified. Based on the numerical error observed in this analysis, it does not appear that this estimation is possible to do accurately using the health state approach.
Disclosure of Interest
R. Lipton Conflict with: eNeura Therapeutics, Conflict with: NIH, Migraine Research Foundation, National Headache Foundation, Conflict with: American Academy of Neurology, Alder, Allergan, American Headache Society, Amgen, Autonomic Technologies, Avanir, Biohaven, Biovision, Boston Scientific, Colucid, Dr. Reddy’s, Electrocore, Eli Lilly, eNeura Therapeutics, GlaxoSmithKlein, Merck, Pernix, Pfizer, Supernus, Teva, Trigemina, Vector, Vedanta, Conflict with: Oxford Press University, Wiley, Informa, J. Porter Conflict with: Amgen Inc, N. Shah Conflict with: Amgen Inc, Conflict with: Amgen Inc, S. Sapra Conflict with: Amgen Inc, Conflict with: Amgen Inc, P. Desai Conflict with: Amgen Inc, Conflict with: Amgen Inc, G. Villa Conflict with: Amgen Inc, Conflict with: Amgen Inc, A. Brennan Conflict with: NIHR, PHE, NIH (US), DH, Conflict with: Amgen, GSK, RTI, TeamDRG, S. Palmer Conflict with: Amgen Inc., J. Jansen Conflict with: Precision Health Economics
Migraine Preventive Therapy
PO-01-078
Botulinum toxin A and acute detoxification in chronic migraine and medication overuse: a randomised, double-blind, placebo-controlled trial
Judith A. Pijpers1,*, Dennis A. Kies2, Mark A. Louter1,3, Erik W. van Zwet4, Michel D. Ferrari1 and Gisela M. Terwindt1
1Neurology
2Radiology
3Psychiatry
4Medical Statistics, LUMC (Leiden University Medical Centre), Leiden, Netherlands
Objectives
Results from two randomised controlled studies suggest efficacy of botulinum toxin A in chronic migraine. However, many of the patients in these studies also had medication overuse. In such patients, acute detoxification alone might also be effective, but is often hampered by severe withdrawal symptoms. Here we assessed whether botulinum toxin A affords additional benefit in addition to acute detoxification.
Methods
We conducted an investigator-initiated, randomised, double-blind, placebo-controlled trial at the Leiden University Medical Centre Headache Clinic. Patients aged 18–65, with chronic migraine and medication overuse, were randomly assigned (1:1) to receive botulinum toxin A (155 units) or placebo (saline and 17ċ5 units botulinum toxin A only administered in the forehead, to prevent unblinding by facial relaxation). Participants in both groups were instructed to acutely refrain from using any acute anti-headache medication and to taper off any prophylactic agent they were using. Primary outcome was the relative change in number of headache days per month at 12 weeks. Secondary outcomes were: (A) Quality of Life during detoxification; (B) proportion of participants who succeeded to refrain from medication for at least three months; (C) change at 12, 24, 36 and 48 weeks of (i) cumulative headache duration; (ii) number of days with (moderate/severe) headache, migraine, or use of acute anti-headache medication. This trial was registered at the Netherlands Trial Register (NTR3440).
Results
According to a 90% power calculation to detect a 20% treatment difference, we included 179 participants (n = 90 botulinum toxin A; n = 89 placebo). The results are currently being analysed and will be presented at the meeting.
Conclusion
The study was successfully completed and results will be presented at the meeting.
Disclosure of Interest
None Declared
Migraine Preventive Therapy
PO-01-079
Cognitive Behavioral Therapy and Greater Occipital Nerve Blockade Combination in The Treatment of Chronic Migraine
Levent E. İnan1,*, Ceyla Ataç-Uçar1, Hanzade Ünal- Artık1, Gülçin Babaoğlu2, Nurten İnan3 and Tahir K. Yoldaş1
1Neurology
2Algology, Ankara Research and Training Hospital
3Algology, Gazi University School of Medicine, Ankara, Turkey
Objectives
Cognitive behavioral therapy(CBT) and greater occipital nerve (GON) block with local anesthetic effectiveness have been shown in the treatment of migraine separetly. We are applying CBT and GON blockade together in chronic migraine. We decided to present the results of two chronic migraine patients.
Methods
Patients with the diagnosis of chronic migraine according to the IHC 2013 had been followed with headache diary. CBT and GON blocks with bupivacaine had been done weekly.
Results
First patient's headache frequency was 17 headache days in 30 days, mean VAS score: 7.08, mean headache duration: 8.6 hours, Beck depresion score(BDS):7 and Beck anxiety score(BAS): 11 at baseline. At the end of four mounth. Headache frequency was 9 headache days in 30 days, mean VAS score:5.9, mean headache duration:7.7 hours, (BDS):0 and (BAS):0.
Second patient's headache frequency was 17 days in 30 days, VAS score:5.8, mean headache duration:7.7 hours, BDS:17 and BAS:25 at baseline after three mounts treatment headache freuency:0 in 30 days, BDS: 10 and BAS: 11.
Conclusion
As these results show combination of CBT and GON blockade with local anesthetics decreased headache frequency, VAS score, headache duration, BDS and BAS.
Disclosure of Interest
None Declared
Migraine Preventive Therapy
PO-01-080
Treatment-Induced Improvement in Migraine Classification in the Fremanezumab HFEM Study
Robert Noble1,*, Ernesto Aycardi2, Marcelo Bigal2 and Pippa Loupe3; Investigators of the Fremanezumab (TEV-48125) HFEM Study
1Statistics, Teva Global Medical Affairs, Hamilton OH
2Clinical Development, Teva Global Research and Development, Frazer PA
3Academic Affairs and Network, Teva Global Research and Development, Overland Park KS, United States
Objectives
Fremanezumab (formerly TEV-48125) is a fully humanized monoclonal antibody targeting the calcitonin-gene related peptide (CGRP) ligand, a validated target for migraine preventive therapy. Fremanezumab was found to be effective and well-tolerated as a preventive treatment for migraine in a high frequency episodic migraine (HFEM) phase 2 study. Study participants included patients with migraine with and without aura who were classified as having episodic migraine (EM) as per the International Classification of Headache Disorders (ICHD III beta). Herein, we determined whether there was a treatment induced shift in the number of patients who met the criteria for classification as having high frequency EM (HFEM) to moderate frequency episodic migraine (MFEM) and low frequency episodic migraine (LFEM) during the HFEM phase 2 study.
Methods
Patient classification in migraine categories during the HFEM study.

Shift in migraine category, worsen = HFEM to CM, stable = HFEM to HFEM, improve = HFEM to MFEM or HFEM to LFEM, discontinued = left study bn values indicate the patients per treatment group meeting HFEM classification at baseline
Results
Overall, the percent of patients in the fremanezumab arms showed significant improvement in migraine classification compared to placebo patients at month 3 (those on 225 mg 73% vs 49% for placebo, 95% CI: 0.098 to 0.358 and those on 675 mg 71% vs 49% placebo, 95% CI: 0.079 to 0.341, Table 1A). Chi square analyses indicated that the shift of migraine classification during the study was not independent of treatment, X2 = 31.64, p = 1.91E-05. As shown in Table 1B, 45% and 52% of patients on fremanezumab 225 mg and 675 mg showed a shift in migraine category from HFEM to LFEM in 3 months as compared to 20% of placebo patients.
Conclusion
As patients with migraine have more frequent migraine attacks, a central sensitization is facilitated, and a vicious cycle is created with a consequent increase on the frequency of migraine attacks. As treated patients were more likely to improve and less likely to worsen compared to those on placebo, this study suggests that fremanezumab may potentially prevent the progression of migraine to more chronic forms. Fremanezumab HFEM Study supported by Teva Pharmaceutical Industries Global Research and Development, Netanya Israel
Disclosure of Interest
R. Noble Conflict with: Teva Pharmaceutical Industries, Conflict with: Teva Pharmaceutical Industries, E. Aycardi Conflict with: Teva Pharmaceutical Industries, Conflict with: Teva Pharmaceutical Industries, M. Bigal Conflict with: Teva Pharmaceutical Industries, Conflict with: Teva Pharmaceutical Industries, P. Loupe Conflict with: Teva Pharmaceutical Industries, Conflict with: Teva Pharmaceutical Industries
Migraine Preventive Therapy
PO-01-081
Impact of Chronic Migraine on Health Resource Utilization, Quality of Life, and Work Productivity: Baseline Results from a Prospective, Observational Study (PREDICT)
Guy Boudreau1,*, Werner J. Becker2, Corrie Graboski3, May Ong-Lam4, Bradley Stewart5 and Goran Davidovic6
1Center de Traitement Neurologique, Quebec City
2University of Calgary, Alberta
3Island Health, Brentwood Bay
4St Paul Hospital, Vancouver
5600 Hys Centre, Edmonton
6Allergan plc, Ontario, Canada
Objectives
The PREDICT study aims to examine the long-term health-related quality of life (QoL) in patients being treated with onabotulinumtoxinA for chronic migraine (CM).
Methods
This is a multicenter, prospective, observational study in adult patients with CM naïve to onabotulinumtoxinA treatment (NCT02502123). Seven treatments of onabotulinumtoxinA are to be administered as described in the Canadian onabotulinumtoxinA product monograph (version July 7, 2014). The primary endpoint is the mean change at treatment 4 from baseline in the Migraine-Specific Quality of Life (MSQ). Secondary endpoints include healthcare resource utilization and work productivity. Data as of December 31, 2016 are summarized descriptively.
Results
Patients included in this analysis (N = 191) were on average 45 years of age (range = 19–72, n = 187); majority were female (85.1%, n = 160/188) and Caucasian (94.1%, n = 176/187). Average age at CM diagnosis was 39 years (range = 7–73, n = 178). The mean age at which the patient started experiencing headache on >15 days a month was 34 years (range = 4–69, n = 177). Patients reported an average 23.1 headache days per month (range = 12.0–30.6, n = 184) in the past 3 months and the majority (60.4%, n = 110/182) indicated a family history of CM. Majority of patients (95.1%, n = 176/185) had taken abortive medications for CM in the past 3 months; most commonly reported were simple analgesics (70.7%, n = 135/191) and triptans (67.0%, n = 128/191). Patients also indicated use of opioid combination analgesics (14.7%, 28/191) and/or opioids (2.6%, 5/191) in the past 3 months (patients taking opioid-containing products on more than 8 days per month were excluded from the study). Majority of patients (80.4%, n = 148/184) had taken a prophylactic medication for CM in the past 2 years; most commonly reported were antidepressants (47.1%, n = 90/191) and anticonvulsants (41.4%, n = 79/191). A total of 176 patients (96.7%) had visited a healthcare professional for treatment/evaluation of their headache and 32 patients (17.7%) indicated visiting an emergency room or urgent care clinic in the past 6 months; many (33.9%, n = 61/180) had received headache-related diagnostic testing. MSQ scores (lower scores indicate decreased QoL) revealed that migraine had the biggest impact on limiting the performance of daily activities (mean[SD] = 36.7[17.6], n = 185) and the lowest impact on preventing the performance of daily activities (mean[SD] = 51.1[22.6], n = 185). Patients employed at the time of screening (73.9%, n = 136/184) worked an average 27.4 hours (SD = 15.5) during the past 7 days and on average missed an additional 6.0 hours (SD = 9.7) of work due to problems associated with their headache. On average, patients indicated that their work productivity was 54% impaired and regular daily activities were 61% impaired due to headaches during the past 7 days.
Conclusion
Baseline data continue to demonstrate the social and economic burden of CM through the increased health-related costs and impairment in work productivity and regular daily activities. In addition, the observed gap in CM diagnosis, impact of headache on QoL, as well as the numerous medications prescribed, many of which have been shown to be ineffective, are all evidence of the unmet need. The PREDICT study may help to provide data on the longer-term impact of onabotulinumtoxinA on QoL in patients with CM.
Disclosure of Interest
G. Boudreau Conflict with: Amgen, Teva, Eli Lilly, W. Becker Conflict with: Allergan, Teva, St. Jude, and Amgen, Conflict with: Amgen, Allergan, Tribute, Electrocore, Conflict with: Serono, Allergan, Tribute, C. Graboski Conflict with: Allergan, Conflict with: Allergan, Conflict with: Allergan, Perdue, Eli Lilly, Sanofi, M. Ong-Lam Conflict with: Allergan, Eli Lilly, B. Stewart Conflict with: Allergan, G. Davidovic Conflict with: Allergan plc
Migraine Preventive Therapy
PO-01-082
Fremanezumab (formerly TEV-48125) decreases migraine symptoms such as nausea, vomiting, photophobia and phonophobia and reduces the need for acute medications in the first week of treatment in the HFEM study
Marcelo Bigal1, Mirna McDonald2, Ernesto Aycardi1,*, Pippa Loupe3, Robert Noble4 and Investigators of the Fremanezumab (TEV-48125) HFEM Study
1Clinical Development, Teva Global Research and Development
2Statistics, Teva Global Medical Affairs, Frazer PA
3Academic Affairs and Network, Teva Global Research and Development, Overland Park KS
4Statistics, Teva Global Medical Affairs, Hamilton OH, United States
Objectives
Migraines have a substantial impact on daily living, affecting productivity and impacting the quality of life for patients and their families. Patients frequently take acute medications to relieve migraine pain and reduce associated symptoms. Fremanezumab (formerly TEV-48125) was found to be effective and well-tolerated as a preventive treatment for migraine in a 3 month phase 2 high frequency episodic migraine (HFEM) study. The present analyses evaluated the efficacy of two doses of subcutaneous fremanezumab (225 mg and 675 mg) during the first three weeks of therapy in patients with high frequency episodic migraine (HFEM) to relieve symptoms associated with migraine pain such as nausea, vomiting, photophobia and phonophobia and the use of acute medications.
Methods
In this multicenter, placebo-controlled, parallel-group study, patients with HFEM
were first screened and trained to use an electronic headache diary during a 28 day
run-in period. After the run-in period, participants who met inclusion criteria and
were 80% compliant with daily diary intake were randomized, and treated once every
28 days for three months with either placebo, fremanezumab 225 mg or 675 mg.
Compared to placebo, both doses of fremanezumab significantly reduced the primary
endpoint of the HFEM study, change in the number of migraine days in month 3
relative to baseline; herein we performed post-hoc analyses to assess the efficacy
of each dose during the first 3 weeks of treatment to reduce migraine symptoms of
nausea, vomiting, photophobia and phonophobia. We also determined whether in the
first 3 weeks of therapy patients taking fremanezumab were able to reduce their
consumption of acute medications for migraine relative to patients taking placebo.

Results
The sample consisted of 296 study participants. Compared to placebo, decreases in days with nausea or vomiting occurred within 1 week of therapy for fremanezumab 225 mg and 675 mg doses (both p < 0.01), a benefit that was maintained through the second and third weeks of therapy (Fig.1 Panel A). Both doses decreased the number of days with photophobia and phonophobia at 1 week (p < 0.0001; Figure 1 Panel B), two weeks (p = 0.0003 and p = 0.0004) and 3 weeks (p = 0.0044 and p = 0.0047). For the weekly number of days taking acute medications, there were decreases for both fremanezumab doses compared to placebo during week 1 (p < 0.0001), week 2 (p < 0.0001) and week 3 (p < 0.0001 and p = 0.0002), shown in Fig. 1, Panel C.
Conclusion
In post-hoc analyses, fremanezumab treatment resulted in a rapid preventive response in patients with HFEM, with improvements seen in reducing migraine symptoms such as nausea, vomiting, photophobia and phonophobia within the first week of fremanezumab therapy. Patients also were able to rapidly reduce their use of acute medications to treat migraine attacks. The HFEM study was supported by Teva Pharmaceutical Industries Netanya Israel.
Disclosure of Interest
M. Bigal Conflict with: Teva Pharmaceutical Industries, Conflict with: Teva Pharmaceutical Industries, M. McDonald Conflict with: Teva Pharmaceutical Industries, Conflict with: Teva Pharmaceutical Industries, E. Aycardi Conflict with: Teva Pharmaceutical Industries, Conflict with: Teva Pharmaceutical Industries, P. Loupe Conflict with: Teva Pharmaceutical Industries, Conflict with: Teva Pharmaceutical Industries, R. Noble Conflict with: Teva Pharmaceutical Industries, Conflict with: Teva Pharmaceutical Industries
Migraine Preventive Therapy
PO-01-083
Body fat was associated to migraine in a sample of young university students of são paulo, brazil
Renata F. Viebig1,*, Kelly M. Isizuka1, Thaís R. Villa2 and Juliana M. Morimoto1
1Health and Biological Sciences Center, Mackenzie Presbiterian University
2Neurology, Universidade Federal de São Paulo, São Paulo, Brazil
Objectives
This study aimed to evaluate the association between nutritional status and the occurrence of migraine in University students from São Paulo-Brazil.
Methods
Cross-sectional study carried out with 46 students, men and women, over 18 years old, enrolled in different undergraduate courses of a private University. The students were invited to the nutritional status assessment consisted by the measurement of the following variables: weight, height and abdominal circumference. Body Mass Index (BMI) was calculated and the results were classified according to the cut-off points of World Health Organization (WHO) (1998). Cardiovascular risk, according to the abdominal circumference (AC) measurement, was either evaluated according to WHO (2000) cut-off points. To determine participants’ body composition, specially body fat percentage, and hydration status, bioelectrical impedance was performed. Body fat values were categorized by Lohman et al (1988) recommendations. Then the students answered a questionnaire about headache occurrence, for medical diagnosis, being the results evaluated by an experimented neurologist, according to the International Headache Society (2013) criteria for classification of migraine types. Statistical analyzes were performed using SPSS software, version 21. To investigate the associations between the occurrence of migraine and BMI categories, cardiovascular risk according to AC, fat percentage categories and hydration level chi-square test was used and to study differences in means between individuals with or without migraine, Student's t-test was performed, considering a 5% significance level. The Ethics Committee of the University approved this research (n.50839915.9.0000.0084).
Results
Sixty-one percent of the students were female (n = 28) and the mean age was 22.2 years old (min. 18; max. 32). Most of the students, 95.7%, reported at least one headache episode in the last 12 months, and 71.7% of the university students met the criteria for migraine, with a higher prevalence of migraine without aura (63.6%). Twenty-nine percent of the women were overweight according to BMI classification, and only 3.6% had a body fat percentage considered adequate. Half of male students presented body fat percentage above the average values reported by Lohman et al. Twenty-five percent of the women presented an increased risk of cardiovascular diseases, and of these, 7.1% presented a very high risk for metabolic diseases. The majority of the students, 80.4%, were well hydrated according to bioelectrical impedance. No associations were found between BMI and AC categories and migraine. This study showed a statistically significant association between body fat percentage and occurrence of migraine (p = 0.008), and individuals with migraine had mean values 6.22% higher than those without the condition (20.91% versus 14.69%). No differences in mean values of body hydration between students with or without migraine diagnosis were found (p = 0.070).
Conclusion
The results suggested that body fat percentage, but not hydration status, BMI or AC, was related to the occurrence of migraine in a Brazilian sample of University students.
Disclosure of Interest
None Declared
Migraine Preventive Therapy
PO-01-084
Migraine prevalence and environmental triggers in university students of são paulo-brazil
Kelly M. Isizuka1,*, Renata F. Viebig1, Thaís R. Villa2 and Juliana M. Morimoto1
1Health and Biological Sciences Center, Mackenzie Presbiterian University
2Neurology, Universidade Federal de São Paulo, São Paulo, Brazil
Objectives
This study evaluated the migraine prevalence and the triggers to this condition in young adults, students of a private University of São Paulo-Brazil.
Methods
A cross-sectional study was carried out with 197 students, men and women, enrolled in several courses of the University, with age above 18 years old. The students answered two questionnaires, one evaluating the presence of diagnostic criteria for migraine, recommended by the International Headache Society (2013) and the other on environment factors triggering migraine attacks, used by Rockett (2010), in southern Brazil. An experimented neurologist made the definitive diagnosis of migraine, using the questionnaire answers. Statistical analyzes were performed using SPSS software, version 21. For the investigation of associations between possible triggers and migraine, the chi-square test was used, and to study differences in triggering factors among individuals with migraine with aura or without aura, Student's t-test was used at a significance level of p < 0.05. All the participants were volunteers and this research was conducted based on the ethics in human research guidelines, with approval of the Ethics Committee of the University, under the number 51061015.0.0000.0084.
Results
The mean age of participants was 21.75 years old (SD = 4.82), most of them being women (70.7%). Among the participants, 35,6% reported that they were simultaneously students and workers. Fifty-six percent of the students reported that they usually practice physical activity, being 67 (50.4%) females. Ninety-five percent of the participants reported at least one headache episode in the last 12 months, and 72.3% met the diagnostic criteria for migraine. The prevalence of migraine with aura was higher, affecting 52.2% of the students. Female students had a significantly higher prevalence of migraine (79.4% versus 20.6%, p < 0.001). In addition, the prevalence of migraine was higher among the students who did not work (p = 0.010). It was also possible to observe that individuals with aura have vestibular migraine (56.3% versus 41.5%, p < 0.001). There was no association between physical activity or sleep hours and migraine. Some triggers of migraine attacks were statically significant, such as fasting or omitting meals (p < 0.001), smelling strong odours (p < 0.001), menstrual period (p < 0.023) and cola soft drinks intake (p = 0.04). Menstrual period showed a strong association to attacks in the female students who had migraine with aura (61.1% against 31.5%, p < 0.002).
Conclusion
The results showed that the prevalence of migraine in the University students of the present research was higher than the results observed in other Brazilian studies. This is a preoccupant fact, because the attacks could impair the student performance in University, and reduce their quality of life. Young women seem to be more affected by migraine, and besides all the environmental triggers found in this study, menstrual period appeared to be an important additional factor for female participants.
Disclosure of Interest
None Declared
Migraine Preventive Therapy
PO-01-085
Rational Design of a Monoclonal Antibody Inhibiting Calcitonin Gene-Related Peptide, ALD403 (Eptinezumab), to Provide Early Onset, High Efficacy, Extended Duration of Action, and Desired Safety for the Prevention of Migraine
Brian Baker1,*, Barbara Schaeffler1, Roger Cady1, John Latham1, Tim Whitaker1 and Jeff Smith1
1Alder BioPharmaceuticals, Bothell, United States
Objectives
To describe the rational design objectives and clinical trial results supporting the efficacy, safety, and durability of action for ALD403 (eptinezumab), a genetically engineered humanized anti-CGRP antibody, for migraine prevention.
Therapeutic mAbs currently in development that target the CGRP pathway may be differentiated by their unique characteristics relating to target selection, affinity, immunogenic recognition (Fcγ activity), route and schedule of administration, clearance mechanisms (FcRn activity and glycosylation pattern), formulation solubility, and bioavailability. Each of these characteristics was evaluated and intentionally selected during the ALD403 (eptinezumab) design process to achieve objectives for high efficacy, desirable safety profile, and patient adherence including optimal dose levels, a convenient treatment schedule (30 minutes intravenous [IV] infusion once every 12 weeks), early onset of migraine prevention, and a 12-week duration of activity.
Methods
The binding affinity for ALD403 to α-CGRP was evaluated by surface plasmon resonance. The pharmacokinetics, efficacy, and safety for ALD403 administration were evaluated in two Phase 2 clinical trials following single IV administration in patients with frequent episodic (FEM) or chronic migraine (CM), and one Phase 3 multi-dose trial in patients with FEM (PROMISE 1).
Results
ALD403 achieved high in vitro binding affinity, KD(M) = 1.5E −11, for the antagonism of soluble α-CGRP ligand, and a low concentration for the inhibition of capsaicin induced dermal vasodilation, IC50 = 0.5 µg/mL, in a Phase 1 trial Following a single IV administration of 1,000 mg ALD403 in FEM patients, the mean maximum concentration, Cmax, 336.4 µg/mL, was observed 4.8 hours, Tmax, after the start of the 1-hour infusion. The mean elimination half-life, T1/2, was 27.9 days and ranged from 19.9 to 46.5 days. The mean plasma concentration, Cmin, observed at Week 12 was 25.6 µg/mL. Significant differences from placebo were observed for reductions in mean migraine days from baseline over Weeks 1–4, 1.7 days (p < 0.001), and Weeks 5–8, 0.9 days (p = 0.033). In CM patients, following IV infusion of 10, 30, 100, or 300 mg, exposure to ALD403 increased proportionally as indicated by respective area under the curve, AUC0-inf, values of 3,000, 7,884, 26,395, or 80,980 µg*hr/mL and Cmax values of 4.3, 11.0, 37.3, or 108.7 µg/mL. Mean concentrations of ALD403 Cmin at 12-weeks post-infusion of 10, 30, 100, or 300 mg were 0.3, 0.7, 2.4, or 7.7 µg/mL, respectively. Aggregate migraine hours/day were decreased 24 hours following administration and significant differences from placebo were observed for reductions in mean migraine days from baseline over Weeks 1–12 following 300 mg, 2.9 days (p < 0.001); 100 mg, 2.4 days (p = 0.003); or 30 mg, 2.8 days (p < 0.001).
Conclusion
The rational design of mAbs enables selection of attributes important for achieving a desired clinical efficacy and safety profile. ALD403 (eptinezumab) was designed in this way and has demonstrated 100% bioavailability, early onset of migraine preventative action, high efficacy in reducing migraine frequency, and a 12-week duration of action following a single IV infusion. These observations suggest ALD403 (eptinezumab) has the potential to be an important new treatment option for migraine prophylaxis in patients with FEM and CM.
Disclosure of Interest
B. Baker Conflict with: Alder BioPharmaceuticals, Conflict with: Alder BioPharmaceuticals, B. Schaeffler Conflict with: Alder BioPharmaceuticals, Conflict with: Alder BioPharmaceuticals, R. Cady Conflict with: Alder BioPharmaceuticals, Conflict with: Alder BioPharmaceuticals, J. Latham Conflict with: Alder BioPharmaceuticals, Conflict with: Alder BioPharmaceuticals, T. Whitaker Conflict with: Alder BioPharmaceuticals, Conflict with: Alder BioPharmaceuticals, J. Smith Conflict with: Alder BioPharmaceuticals, Conflict with: Alder BioPharmaceuticals
Migraine Preventive Therapy
PO-01-086
Comparison of Propranolol versus Placebo Use in Reduction of Migraine Days by Frequency of Migraine Episodes, Systematic Review and Individual Patient Level Data Meta-Analysis
Ioana Medrea1,* and Suzanne Christie1
1Neurology, University of Ottawa, Ottawa, Canada
Objectives
Propranolol is one of the medications considered efficacious in episodic migraine prophylaxis. However, there are no randomized controlled trials of propranolol in chronic migraine prophylaxis. It is becoming more widely recognized that chronic migraine patients suffer from a different disease process, but recent data indicates that frequent episodic migraine patients (> = 10 headache days/month) are more alike to chronic migraine patients and as such may respond to similar medications.
We have undertaken a systematic review and individual patient level meta-analysis of trials that include a population of infrequent and frequent migraneurs to determine if the response to propranolol seen in episodic migraine is independent of frequency of attacks.
Methods
MEDLINE, EMBASE, Pubmed, were searched through to December 2016. Publications were also sought through a hand-search of journals and of the American Headache Society (AHS) and International Headache Society (IHS) conference proceedings and the references lists of identified trials were also reviewed to identify additional articles.
Studies were included if they were randomized controlled trials comparing propranolol
with placebo or an active comparator in adult migraineurs and had available
individual patient level data. Trials were assessed independently by two reviewers.
The pooled headache frequency on propranolol was the outcome measure, varying this
by headache frequency on placebo to determine if there was an effect of headache
frequency at baseline with response to propranolol. 
Results
Three randomized controlled trials (RCT) were included in the individual patient level meta-analysis, they were class III trials. The analysis was done by subgroups in each trial of infrequent and frequent episodic migraineurs as defined by headache days on placebo (likely an under-estimate of headache frequency). Our analysis shows that there is a treatment effect in reduction of mean headache frequency in each of these respective populations compared to placebo.
Conclusion
Propranolol is shown efficacious in reducing the headache frequency in frequent episodic migraineurs, a population that likely overlaps with chronic migraine patients. Although this analysis is limited by a small number of patients in the frequent migraine group, it raises the possibility that propranolol is useful in chronic migraine patients for migraine prophylaxis, and provides justification for a study looking at this question.
Disclosure of Interest
None Declared
Migraine Preventive Therapy
PO-01-087
Effect of anti-CGRP receptor antibody AA58 on CGRP receptor internalization and trafficking
Cen Xu1,*, Hong Sun2, Raffi Manoukian3, Bojiao Yin4, John Dunlop2, Zaven Kaprielian2 and Silke Miller2
1Neuroscience, Amgen Inc., Thousand Oaks
2Neuroscience
32Medical Sciences
4Therapeutic Discovery, Amgen Inc., Boston, United States
Objectives
Therapeutic antibodies that block the CGRP signaling pathway are a promising new drug class for migraine prevention. An anti-CGRP receptor antibody has demonstrated efficacy in clinical studies for the treatment of episodic and chronic migraines. To further understand the mechanism of action of the antagonist antibody, we measured the effects of anti-CGRP receptor antibody AA58 on the CGRP receptor internalization and trafficking in engineered cells.
Methods
We engineered a CHO cell line, which does not endogenously express CLR or RAMP1, by co-expressing His-tagged RAMP1 and myc/FAP-tagged CLR. The cells were used to directly measure both functional responses and receptor internalization after exposure to agonist alpha-CGRP (CGRP) alone or in combination with CGRP receptor antagonist antibody AA58. CGRP receptor signaling was measured by a cAMP accumulation assay and receptor internalization was monitored with a flow cytometric fluorogen-activating protein (FAP) assay. Immunofluorescence (IF) confocal microscopy was also used to visualize CGRP receptor internalization and trafficking in cells processed at fixed time points. cAMP responses and receptor internalization were compared to those in CHO cells expressing un-tagged CGRP receptor components. Functional cAMP responses were also measured in SK-N-MC cells expressing native CGRP receptors to confirm receptor pharmacology.
Results
Exposure to AA58 alone induced neither cAMP accumulation nor internalization of the CGRP receptor.
Exposure to agonist CGRP led to comparable dose-dependent cAMP accumulation in CHO cell lines expressing tagged or un-tagged CGRP receptors. In all cell lines tested, responses to agonist CGRP were blocked by co-incubation with an antagonist peptide CGRP8–37 or with AA58.
Prior to the application of agonist or antagonist, CGRP receptor immunoreactivity was confined to the cell membrane. As measured by flow cytometry, CGRP induced internalization of the receptors within minutes of application. IF confocal microsocopy visually confirmed immunoreactivity of CGRP receptor on both membrane and intracellular vesicles 5 minute after CGRP application. Following 10 min of agonist application, most of the CGRP receptor immunoreactivity was localized to the intracellular compartment. At the 30 min time point, immunoreactivity was observed in perinuclear bodies that colocaized with LAMP2 immunostaining (a marker of lysosomal membrane protein) suggesting that CGRP receptor was targeted for lysosomal degradation. Co-incubation with AA58 blocked CGRP induced internalization of the CGRP receptors.
There was no indication of apoptosis based on nuclear morphology indicating that AA58 blockade is not detrimental to cell health.
Conclusion
Using an engineered CHO cell line expressing tagged, functional CGRP receptors, we demonstrate that exposure to anti-CGRP receptor antibody AA58 alone did not induce any cAMP response and the internalization of the receptor. However AA58 inhibits agonist-induced cAMP accumulation and receptor internalization. These findings suggest that therapeutic antibodies act by inhibiting the CGRP-induced functional cAMP response and delaying receptor internalization and trafficking.
Disclosure of Interest
C. Xu Conflict with: Amgen Inc., H. Sun Conflict with: Amgen Inc., R. Manoukian Conflict with: Amgen Inc., B. Yin Conflict with: Amgen Inc., J. Dunlop Conflict with: Amgen Inc., Z. Kaprielian Conflict with: Amgen Inc., S. Miller Conflict with: Amgen Inc.
Migraine Preventive Therapy
PO-01-088
Postural correction and orthopedic massage decrease migraine episodes and reduce headache attributed lost time
Doris Vahtrik1, Ingrid Vanahunt2, Kristi Tamela3 and Mark Braschinsky3,*
1Institute of Sport Sciences and Physiotherapy, University of Tartu
2Sports Medicine and Rehabilitation Clinic
3Neurology Clinic, Tartu University Hospital, Tartu, Estonia
Objectives
Due to controversial information about the effect of different physiotherapy methods used in the treatment of migraine patients, the aim of the study was to assess postural correction and the effect of orthopedic massage to upper body posture; the frequency of migraine attacks; headache attributed lost time; head, neck and shoulder girdle muscles tone and active range of cervical motion in migraine patients before and after five week therapy program.
Methods
The purpose of the postural correction therapy program was to instruct and guide subjects to maintain good upper body alignment during sitting, standing or walking in everyday activities. The program consisted of five sessions administered once a week. The duration of each therapy session was one hour. Every session included postural correction and the orthopedic massage, lasting 55 minutes.
Upper body alignment from anterior, posterior and lateral view was assessed with observation (New York Posture Rating Chart). Score of posture was formed of the head, shoulders and thoracic spine evaluation results (free evaluable structures in free view, 0–3 indicating poor, 4–7 fair and 8–10 good posture). Based on the subjects headache diary and the question “On how many days in the last month did you have a headache” from The Headache Under-Response to Treatment (HURT) Questionnaire migraine episodes during the past months were recorded. Headache attributed lost time was assessed with HALT questionnaire. Muscles tone was assessed bilaterally using the Total Tenderness Score (TTS) in subject's supine and prone position for m. trapezius pars descedens, m. splenius capitis, linea nuchalis superior, m. levator scapulae, m. sternocleidomastoideus, m. masseter, m. temporalis, m. deltoideus pars anterior. Active range of cervical motion (caROM) was assessed in six directions by cervical goniometry.
This study was approved by the Research Ethics Committee of the University of Tartu.
Results
Ten consented patients (9 women, 1 man) with migraine diagnosis (2 with aura and 8 without aura) were included in a five-week postural correction and orthopedic massage therapy. The patients’ mean age was 41.6 years (SD 10.78 years, range 23–58 years) and the mean body mass index 24 kg/cm2 (SD 3.8 kg/cm2, range 18–30 kg/cm2). The average period of migraine symptoms was 14.6 years (SD 12.17, range 2–36 years). Before therapy, during the past month migraine episodes were reported on 10.3 days (SD 5.59, range 3–16).
After the therapy subjects’ upper body posture was 10.4% more correct in every three assessed views than before therapy (respectively before therapy 25.1 and after therapy 28.0 points; p < 0.01). The caROM values increased by 9.5% in flexion (53.7 and 59.3 degrees; p < 0.01), 12.8% in extension (61.1 and 70.1 degrees; p < 0.05), 13.8% in rotations to the right (67.3 and 78.1 degrees; p < 0.05) and 11.5% to the left (72.8 and 82.3 degrees; p < 0.05). Lateral flexion to the right (35.3 and 39.7 degrees) and to the left (40.3 and 45.3 degrees) were also increased (both 11.1%), but not significantly (p > 0.05). Migraine days per month decreased 35.9% (10.3 and 6.6 days; p < 0.05). HALT and Total Tenderness scores were significantly lower compared to the baseline (51.3%, 24.2 and 11.8 HALT score; p < 0.01, and 49.9%, 24.5 and 12.4 TTS score p < 0.001 respectfully).
Conclusion
Postural correction and orthopedic massage are effective in decreasing migraine days, probably leading to an improved quality of migraine patients’ life. Physiotherapy methods used in current study were effective also in improving upper body functionality related with upper body posture, head, neck and shoulder girdle muscles tone and cervical mobility.
Disclosure of Interest
None Declared
Migraine Preventive Therapy
PO-01-089
Hull Prospective Analysis of OnabotulinumtoxinA (Botox) in the treatment of Chronic Migraine; a real-life data in 742 patients; updated results on over six years of experience
Fayyaz Ahmed1, Ali J. Ghabeli2, Alina Buture2,* and Modar Khalil2
1Spire Hesslewood Clinic and Hull York Medical School, Elloughton
2Neurology, Spire Hesslewood Clinic and Hull York Medical School, Hull, United Kingdom
Objectives
To evaluate the efficacy and safety of OnabotulinumtoxinA in adult patients with Chronic Migraine (CM) in real-life settings.
Methods
Adult patients with CM attending the Hull Migraine Clinic were treated with OnabotulinumtoxinA based on clinical needs. Patients were treated as per PREEMPT protocol. Patients were asked to maintain a headache diary for at least 30 days prior to and continuously after treatment. Patients with medication overuse were included based on the expert opinion. Data were extracted for headache days, migraine days, crystal clear days (headache-free) as primary outcome; also analgesic consumption, adverse events and quality of life using HIT-6. Responder was defined as per Hull criteria (50% reduction in either headache or migraine days or increment on headache free days twice the baseline) for treatment in the first cycle.
Results
Of a series of 742 patients (July 2010 – February 2017) full data were available on 626 patients (112 male, median age 48 years; range 19–77 years, 514 female, median age 45 years; range 18–91 years). A total of 3368 cycles were given. 611 (97.6%) had failed three preventive treatments. 363 (57.9%) patients were overusing analgesics. Patients had CM for a median of 4 years (Range 0.5–67 years). 363 (58.4%) responded based on Hull Criteria and reported improved health related quality of life outcome. 82 (13.0%) reported adverse events mainly stiffness in the neck with 50 (7.9%) reporting mild ptosis.
Conclusion
We report on a large cohort of real life patients receiving OnabotulinumtoxinA for chronic migraine.
Disclosure of Interest
F. Ahmed Conflict with: Allergan, Eneura, Electrocore, Novartis as Advisory Board member paid to British Association for the Study of Headache and the Migraine Trust, Conflict with: Educational Officer for British Association for the Study of Headache, Trustee of Migraine Trust, IHS Board Member, A. Ghabeli: None Declared, A. Buture: None Declared, M. Khalil: None Declared
Migraine Preventive Therapy
PO-01-090
Does Medication overuse matter? Response to OnabotulinumtoxinA in Chronic Migraine (CM) patients with or without medication overuse; update from real-life data
Modar Khalil1,*, Alina Buture1, Ali J. Ghabeli1 and Fayyaz Ahmed1
1Neurology, Spire Hesslewood Clinic and Hull York Medical School, Hull, United Kingdom
Objectives
Introduction: CM affects 2% of the general population with substantial impact on quality of life. Medication overuse in CM is seen in around two third of patients in specialist headache clinics. There is lack of consensus on whether preventive treatment be initiated before or after the analgesic withdrawal. We analysed the response to OnabotulinumtoxinA in patients with CM with or without analgesic overuse treated at the Hull Migraine Clinic.
Objectives
To compare the efficacy of OnabotulinumtoxinA in adults with Chronic Migraine with or without medication overuse.
Methods
Methods: Adult patients with CM were offered OnabotulinumtoxinA based on clinical need and were injected based on the PREEMPT treatment paradigm. Headache diaries were maintained for 30 days prior to and continuously after treatment. Data were extracted for headache, migraine and headache-free days and responders were defined based on Hull Criteria (50% reduction of either headache or migraine days or increment in headache free days twice that of the baseline).
Results
Results: Of 742 patients, full data for the first cycle was available on 626 patients [363 (57.9%) with analgesic overuse and 263 (42.1%) without overuse]. The responder rate based on Hull criteria was 59.8% in patients with analgesic overuse compared to 56.8% in patients without overuse. 50% reduction in Migraine days was 41% and 44% respectively. There was significant reduction in days with analgesic consumption in both groups.
Conclusion
Conclusion: Patients with CM respond equally well to OnabotulinumtoxinA irrespective of analgesic consumption at baseline.
Disclosure of Interest
M. Khalil: None Declared, A. Buture: None Declared, A. Ghabeli: None Declared, F. Ahmed Conflict with: Allergan, Eneura, Electrocore, Novartis as Advisory Board member paid to British Association for the Study of Headache and the Migraine Trust, Conflict with: Educational Officer for British Association for the Study of Headache, Trustee of Migraine Trust, IHS Board Member
Migraine Preventive Therapy
PO-01-091
Long term outcome for OnabotulinumtoxinA therapy in Chronic Migraine; a two year follow up of 403 patients from the Hull Migraine Clinic
Alina Buture1,*, Ali J. Ghabeli1, Modar Khalil1 and Fayyaz Ahmed1
1Neurology, Spire Hesslewood Clinic and Hull York Medical School, Hull, United Kingdom
Objectives
Introduction: The long-term outcome for patients with CM treated with OnabotulinumtoxinA remains uncertain. The National Institute for Health and Care Excellence (NICE) recommends discontinuing treatment if there is no response to two consecutive cycles (negative stopping rule) or when the migraine becomes episodic (positive stopping rule). However, this is based on consensus only.
Objectives: To determine the long term outcome of patients with CM treated with OnabotulinumtoxinA.
Methods
Methods: All patients treated with OnabotulinumtoxinA at the Hull Migraine Clinic were prospectively followed. Treatment was delivered as per the PREEMPT paradigm. Responders were defined as per NICE or Hull criteria. Treatment was stopped if there was no response to two consecutive cycles or until the headache days were less than 10 for three consecutive months (modified positive stopping rule).
Results
Results: Of a series of 742 patients treated between July 2010 and February 2017 and received 3368 cycles, full data was available on 626 patients. Treatment data for at least two years (range 24–54 months) was available on 403. 234 (58.06%) patients fulfilled either NICE (48%) or Hull criteria for responder at cycle 2 and continued treatment. 169 patients (41.9%) stopped treatment at cycle two. Of the 234 patients 94 (40.17%) patients continued treatment for two years or more and 140 (59.8%) were able to stop the treatment within two years; 32/140 (22.8%) relapsed after stopping, 15/140 (10.7%) got resistant after initial response and 88/140 (62.85%) remained episodic.
Conclusion
Conclusion: At two years, 40% of initial cohort of responders will still require therapy with OnabotulinumtoxinA.
Disclosure of Interest
A. Buture: None Declared, A. Ghabeli: None Declared, M. Khalil: None Declared, F. Ahmed Conflict with: Allergan, Eneura, Electrocore, Novartis as Advisory Board member paid to British Association for the Study of Headache and the Migraine Trust, Conflict with: Educational Officer for British Association for the Study of Headache, Trustee of Migraine Trust, IHS Board Member
Migraine Preventive Therapy
PO-01-092
Analysis of patterns of response to OnabotulinumtoxinA in Chronic Migraine in predicting long-term outcome
Alina Buture1,*, Ali J. Ghabeli1, Modar Khalil1 and Fayyaz Ahmed1
1Neurology, Spire Hesslewood Clinic and Hull York Medical School, Hull, United Kingdom
Objectives
Introduction: The efficacy of OnabotulinumtoxinA for Chronic Migraine (CM) is established; however, long term outcome data is limited and need for ongoing treatment remains uncertain.
Objectives: The study aims to identify patterns of response to OnabotulinumtoxinA that predict successful conversion to episodic migraine.
Methods
Methods: Adult patients receiving OnabotulinumtoxinA for CM at the Hull Migraine Clinic were prospectively followed. All patients maintained headache diary continuously during treatment. Data was extracted on headache and migraine days to identify patterns of response and need for ongoing treatment at two years.
Results
Results: Of 403 patients followed up for at least two years 234 fulfilled NICE or Hull Criteria for responder and continued treatment beyond cycle 2. Of the 234 responders, 94 patients were still obtaining positive response at year 2 and 88 were successfully converted to episodic migraine. Others were either lost to follow up, relapsed, became resistant or stopped treatment for other reasons. Our study analysed patterns of response and outcome in the cohort of 182 responders. We found two distinct patterns of response with 100 (54.9%) patients having a fluctuating ‘wearing off’ pattern with an increase in headache frequency prior to their next treatment; 82 (45.05%) having a steady decline on headache days without significant fluctuation between treatments. We found that the ‘wearing off’ pattern predicted those patients who would remain in chronic migraine with only 12/100 (12%) patients converting to episodic migraine compared to 63/82 (76.8%) with stable non-fluctuating response.
Conclusion
Conclusion: We observed two distinct patterns of response that help to predict long-term outcome.
Disclosure of Interest
A. Buture: None Declared, A. Ghabeli: None Declared, M. Khalil: None Declared, F. Ahmed Conflict with: Allergan, Eneura, Electrocore, Novartis as Advisory Board member paid to British Association for the Study of Headache and the Migraine Trust, Conflict with: Educational Officer for British Association for the Study of Headache, Trustee of Migraine Trust, IHS Board Member
Migraine Preventive Therapy
PO-01-093
OnabotulinumtoxinA in Chronic Migraine; Predicting response to treatment based on headache days at baseline
Alina Buture1,*, Ali J. Ghabeli1, Modar Khalil1 and Fayyaz Ahmed1
1Neurology, Spire Hesslewood Clinic and Hull York Medical School, Hull, United Kingdom
Objectives
OnabotulinumtoxinA is an established preventive treatment for Chronic Migraine (CM). Predicting response to treatment is unknown, although potentially duratuion of CM, frequency of headache or migraine days may have some bearing on the response rate.
To establish whether the number of headache days at the baseline predict response to treatment with Botox in adult patients with CM.
Methods
Patients receiving OnabotulinumtoxinA at the Hull Migraine Clinic were prospectively followed up. The treatment was delivered as per PREEMPT protocol and patients were asked to maintain a headache diary at least four weeks before and continuously after treatment. Data was extracted for headache and migraine days and headache free days before and after treatment. Patients were divided into three frequency groups based on the number of headache days pre-treatment as low frequency (15–20), moderate frequency (21–25) or high frequency (26–30). The response to treatment in the three groups were compared.
Results
Of a series of 742 patients treated between July 2010 and February 2017, full data was available on 626 patients receiving 3368 cycles in total. 125 (19.9%) had low frequency, 144 (23%) had moderate frequency and 357 (57%) had high frequency headache days.
Patients with low or moderate frequency of headache days at baseline tend to respond better than those with high frequency headache days before treatment. However, the improvement in severity (migraine days) was similar in the three groups. Achievement of headache free days was more in those with high frequency at baseline.
Applying Hull Criteria that considers headache, migraine and headache free days to identify response, patients with moderate frequency seem to respond better.
Conclusion
Patients with low or medium frequency of headache days at baseline seem to respond better than those with high frequency headache days before treatment.
Disclosure of Interest
A. Buture: None Declared, A. Ghabeli: None Declared, M. Khalil: None Declared, F. Ahmed Conflict with: Allergan, Eneura, Electrocore, Novartis as Advisory Board member paid to British Association for the Study of Headache and the Migraine Trust, Conflict with: Educational Officer for British Association for the Study of Headache, Trustee of Migraine Trust, IHS Board Member
Migraine Preventive Therapy
PO-01-094
A Multicenter, Prospective, Single Arm, Open Label, Post-Market, Observational Study to evaluate the use of sTMS in reduction of Migraine Headache (ESPOUSE Study)
Amaal J. Starling1,*, Stewart J. Tepper2, Michael J. Marmura3, Ejaz A. Shamim4, Matthew S. Robbins5, Nada A. Hindiyeh6, Andrew C. Charles7, Peter J. Goadsby8, Richard B. Lipton5, Stephen D. Silberstein3 and David W. Dodick1
1Neurology, Mayo Clinic, Phoenix
2Neurology, Dartmouth, Hanover
3Neurology, Jefferson Headache Center, Philadelphia
4Neurology, Mid-Atlantic Permanente Medical Group (Kaiser), Rockville
5Neurology, Montefiore Headache Center, Bronx
6Neurology, Stanford Headache Program, Stanford
7Neurology, UCLA Headache Research and Treatment Program, Los Angeles, United States
8Neurology, NIHR-Wellcome Trust King's CRF, London, United Kingdom
Objectives
Single pulse transcranial magnetic stimulation (sTMS) is an FDA-approved acute treatment for migraine with aura. Open label patient experience in the United Kingdom has suggested a possible preventive benefit in migraine. The objective of this clinical trial was to evaluate the efficacy and tolerability of sTMS for the treatment of migraine.
Methods
The ESPOUSE Study was a multicenter, prospective, single-arm, open label, observational study to evaluate sTMS for the preventive treatment of migraine with or without aura. From December 2014 to March 2016, 263 patients with migraine were consented to complete a 1-month baseline headache diary followed by 3 months of treatment. The full analysis set (FAS) included patients who completed the baseline headache diary, met the inclusion criteria including 5–25 headache days per month, and used the device at least once. The treatment protocol consisted of both preventive (4 pulses twice daily) and acute treatment (3 pulses at 15 minute intervals repeated up to 3-times for each attack). The primary effectiveness endpoint (PEE), mean reduction of headache days compared to baseline, was measured over the 28-day period ending at 12 weeks. In the absence of a placebo control group, the PEE was compared to the performance goal, which is a statistically-derived, estimated placebo effect size, based on historical controls, of −0.6 day reduction of headache days from baseline.
Results
A total of 263 subjects were consented, 229 completed a baseline diary, 220 subjects were found to be eligible based on the number of headache days, and 217 were assigned a device (safety data set). 132 subjects met the strict inclusion criteria based on the protocol definition of a headache day (4 or more hours of headache reaching moderate to severe pain), comprising the FAS. FAS baseline characteristics include: mean age of 42.8 years; 80.3% female; 85.6% Caucasian, 8.3% African American, 5.3% Hispanic, and 0.8% other. The PEE analysis was assessed in the FAS dataset. The mean reduction of headache days from baseline compared to the performance goal was statistically significant. There was −2.8 ± 0.4 mean reduction of headache days from baseline (9.1 days) in the FAS compared to the performance goal of −0.6 days (p < 0.0001). 19.4% of subjects reported adverse events that were determined as “definitely”, “probably”, or “possibly” device-related. There were no serious adverse events. The top three adverse events were lightheadedness (4.5%), tingling (3.9%), and tinnitus (3.9%). 9 patients withdrew from the study because of adverse events.
Conclusion
This open label study suggests that sTMS may be an effective, well-tolerated treatment option for migraine prevention.
The ESPOUSE Study was supported by eNeura Inc.
Disclosure of Interest
A. Starling Conflict with: Amgen, Lily, eNeura, S. Tepper Conflict with: ATI, Conflict with: Alder, Allergan, Amgen, ATI, Avanir, Electrocore, eNeura, Scion Neurostim, Teva, Zosano, Conflict with: Acorda, Alder, Allergan, Amgen, ATI, Avanir, BioVision, Dr. Reddy's, Electrocore, Eli Lilly, eNeura, Kimberly-Clark, Pernix, Pfizer, Scion Neurostim, Teva, Zosano, M. Marmura Conflict with: Teva, eNeura, Conflict with: Teva, Supernus, E. Shamim Conflict with: Kinetics Foundation, CD PROBE (Allergan), COMPEL(Allergan), Myorisk (NIEHS), eSPOUSE (eNeura), NIH intramural support NINDS and NIEHS, Mid-Atlantic Permanente Research Institute. I have not received any personal compensation from Allergan but have received research funding, M. Robbins Conflict with: eNeura, N. Hindiyeh: None Declared, A. Charles: None Declared, P. Goadsby Conflict with: Grants and personal fees from Allegan, Amgen and Eli-Lilly and company. Personal fees from Akita Biomedical, Alder Biopharmaceuticals, Autonomic Technologies Inc, Avanir Pharma, Cipla Ltd, Colucid Pharamceuticals Lrd, Dr Reddy's Laboratories, eNeura, Electrocore LLC, Novartis, Pfizer Inc, Promius Pharma, Quest Diagnostics, Scion, Teva Pharmaceuticals, Trigemina Inc., Scion; and personal fees from MedicoLegal work, Journal Watch, Up-to-Date, Oxford University Press and in addition, Dr Goadsby has a patent Magnetic stimulation for headache pending assisgned to eNeura., R. Lipton Conflict with: He receives research support from the NIH: 2PO1 AG003949 (Program Director), 5U10 NS077308 (PI), 1RO1 AG042595 (Investigator), RO1 NS082432 (Investigator), K23 NS09610 (Mentor), K23AG049466 (Mentor). He also receives support from the Migraine Research Foundation and the National Headache Foundation. He serves on the editorial board of Neurology and as senior advisor to Headache. He has reviewed for the NIA and NINDS, holds stock options in eNeura Therapeutics; serves as consultant, advisory board member, or has received honoraria from: American Academy of Neurology, Alder, Allergan, American Headache Society, Amgen, Autonomic Technologies, Avanir, Biohaven, Biovision, Boston Scientific, Colucid, Dr. Reddy’s, Electrocore, Eli Lilly, eNeura Therapeutics, GlaxoSmithKlein, Merck, Pernix, Pfizer, Supernus, Teva, Trigemina, Vector, Vedanta. He receives royalties from Wolff’s Headache, 8th Edition, Oxford Press University, 2009, Wiley and Informa., S. Silberstein: None Declared, D. Dodick Conflict with: Dr Dodick has served on advisory boards and/or has consulted within the past five years for Allergan, Amgen, Alder, Arteaus, Pfizer, Colucid, Merck, Neura, NuPathe, Eli Lilly and Company, Autonomic Technologies, Ethicon J&J, Zogenix, Supernus, Labrys, Boston Scientific, Medtronic, St Jude, Bristol Myers Squibb, Lundbeck, Impax, MAP, Electrocore, Tonix, Novartis, Teva, Alcobra, Zosano, Insys, GBS/Nocira, Acorda. Dr. Dodick owns equity in Epien, GBS/Nocira and Second Opinion. Dr. Dodick has received funding for travel, speaking, editorial activities or royalty payments from: IntraMed, SAGE Publishing, Sun Pharma, Allergan, Oxford University Press, American Academy of Neurology, American Headache Society, West Virginia University Foundation, Canadian Headache Society, Healthlogix, Wiley, Universal Meeting Management, WebMD, UptoDate, Medscape, Oregon Health Science Center, Starr Clinical, Decision Resources, Synergy.
Migraine Preventive Therapy
PO-01-095
Case report: treatment of sporadic hemiplegic migraine with propranolol and non invasive vagal nerve stiumlation (nvns) in a young woman through pregnancy
Anne-Marie Logan1,* and Niran Nirmalananthan1
1Headache Service, Neurology Department, St George’s University Hospital NHS Foundation Trust, London, United Kingdom
Objectives
Sporadic hemiplegic migraine (SHM) is a rare form of migraine with aura associated with motor weakness defined by its absence in the first or second degree relatives of the probands. Treatment is based on case reports only and the young age of onset in women complicates treatment during child bearing years. This case report adds to the evidence for prophylaxis and acute treatment for hemiplegic migraine.
Methods
A 32 year old doctor presented with a two year history of SHM. She had episodes of unilateral hemisensory progressing to hemiplegic aura lasting upto 48 hours. She continued to have regular migraines without aura. Imaging and investigations were normal over multiple admissions. Triptans were unsuccessful in treating the attacks. Pizotifen which she used previously was not controlling her symptoms. Due to the severe functional impact the motor aura and headache were causing on her work and family and her wish to conceive, Propranolol 80 mg bd was used. Acute treatment was changed to nVNS at the onset of sensory aura with headache along with simple analgesics. nVNS was used twice daily for one month and then acutely for sensory attacks. She was able to abort hemisensory attacks including those progressing distally into her limbs which would previously have resulted in motor aura, by using nVNS acutely along with the low dose simple analgesics. She noticed that 30 minutes after using her acute treatment her symptoms would start to resolve in a way that she had not previously experienced. She became pregnant 6 months later and continued with the Propranolol and nVNS/ Paracetamol. The dose of Propranolol was lowered to 40 mg bd through her late pregnancy without change to her migraine symptoms.
Results
A pragmatic approach to treatment using several interventions was tried due to the severity of her symptoms. The combination of Propranolol with nVNS/simple analgesia reduced her total MIDAS score from 104 to 22 before her pregnancy, with the HIT6 reducing from 66 to 60. nVNS and low dose simple analgesia was successfully used acutely and stopped the patient's normal progression of symptoms to motor aura from the initiation of prophylaxis and through the subsequent months. The initiation of nVNS improved the effectiveness of her acute treatment with the result that this combination was sufficent through pregnancy. The treatment continued thoughout her pregnancy and breastfeeding with good effect.
Conclusion
There is only one case report to our knowledge of Propranolol being used as prophylaxis for hemiplegic migraine. This case report adds to evidence for treatment of SHM which has largely been limited to case reports of prophylaxis and acute medicine which are contraindicated in pregnancy. The treatment was well tolerated and enhanced the patient’s quality of life as shown in the improvements in quality of life measures. The difference in improvement between the MIDAS and HIT6 highlights the improvement in the work related impact of the hemiplegic migraine which was more identifiable in the MIDAS scale. We suggest that Propranolol should be considered for treatment in women of childbearing age with SHM and further work should be undertaken into the use of nVNS for acute treatment of hemiplegic migraine.
Disclosure of Interest
None Declared
Migraine Preventive Therapy
PO-01-096
OnabotulinumtoxinA for Chronic Migraine during pregnancy; experience from Hull Headache Clinic, United Kingdom
Ali J. Ghabeli1,*, Kalyan Peddada1, Fan Cheng1, Alina Buture1, Modar Khalil1 and Fayyaz Ahmed1
1Neurology, Spire Hesslewood Clinic and Hull York Medical School, Hull, United Kingdom
Objectives
The use of OnabotulinumtoxinA during pregnancy is restricted due to the lack of adequate and well-controlled studies. While women who are pregnant, nursing or planning a pregnancy are excluded from clinical trials, many women treated with OnabotulinumtoxinA for axillary hyperhidrosis, chronic migraine and cosmetic indications are of reproductive age. A 24–year retrospective review of the Allergan safety database on 574 pregnancies demonstrated that the prevalence of fetal defects in OnabotulinumtoxinA-exposed mothers to be comparable to background rates in the general population. Most of these patients were treated for cosmetic reasons or movement disorders. There are no reports regarding patients with Chronic Migraine exposed to OnabotulinumtoxinA therapy during pregnancy.
Methods
Adult patients treated with OnabotulinumtoxinA for prophylaxis of Chronic Migraine at the Hull Headache Clinic received prospective follow-up. Female patients of reproductive age were asked to report on pregnancy before each treatment. Pregnant patients were advised against further treatment unless they chose to continue following an informed discussion about the uncertain impact of treatment on the fetus.
Results
Of the 15 patients who reported pregnancy (8–16 weeks), 12 wished to continue with further treatment at three-monthly intervals. 3 patients did not continue further treatment. All 15 patients had normal vaginal delivery, live births and no fetal malformations were reported.
Conclusion
We report no adverse outcome in 15 pregnant patients with CM exposed to OnabotulinumtoxinA. There is need to collect further data before establishing its safety.
Disclosure of Interest
A. Ghabeli: None Declared, K. Peddada: None Declared, F. Cheng: None Declared, A. Buture: None Declared, M. Khalil: None Declared, F. Ahmed Conflict with: Allergan, Eneura, Electrocore, Novartis as Advisory Board member paid to British Association for the Study of Headache and the Migraine Trust, Conflict with: Educational Officer for British Association for the Study of Headache, Trustee of Migraine Trust, IHS Board Member
Migraine Preventive Therapy
PO-01-097
Novel formulation of nasal oxytocin for the treatment of migraine
David C. Yeomans1 and Shashi Kori2,*
1Anethesia, Stanford University, Stanford
2Trigemina, Moraga, United States
Objectives
Objective: We have shown that nasal administration of oxytocin (OT) in rats produced a clear craniofacially limited analgesic effect that is mediated through transport along trigeminal nerve to act at OT receptors on trigeminal neurons. Mg++ has been shown to enhance binding affinity of OT for its receptor. This aim of this study was to test whether formulations of OT which include a magnesium (Mg) salt would enhance the effect of nasal OT on trigeminal nerve associated pain.
Methods
Methods: We have previously shown that craniofacial inflammation induced by electrocutaneous (EC) stimulation of the face of anesthetized rats induces an 5–10 fold upregulation of oxytocin (OT) receptors on trigeminal ganglia neurons. Thus, we pretreated rats with EC 24 hours prior to testing for nociceptive withdrawal responses to noxious heating of the face. We then nasally administered either OT, Mg, or one of a series of concentration combinations of 1 of 3 Mg salts and OT in solution. We then measured the effects of this administration on withdrawal latencies over the next 3 hours.
In separate studies, rats were given CFA injection in the cheek in order to induced inflammation and receptor upregulation. 24–48 hours thereafter, rats were euthanized and trigeminal ganglia removed, dissociated and neurons prepared for whole-cell patch clamp electrophysiology. The effects of OT and OT plus Mg solutions on excitability of neurons was then tested by current injection. Action potential current thresholds, suprathreshold action potential number, and effects on sodium and potassium currents were determined.
Results
Results: Both OT delivered alone as well as any of the Mg salts produced significant elevation of the withdrawal latency in response to noxious heat. The combination of the two produced a clear supraadditive effect at many dose ratios, demonstrating pharmacologic synergy between OT and Mg. The superiority of OT formulation with Mg++ was confirmed in the electrophysiologic study, in that it produced distinctly greater inhibition of TG neuron excitability, AP generation and sodium current.
Conclusion
Conclusion: Addition of Mg++ via Mg salt synergistically enhanced the analgesic effect of oxytocin when applied nasally to rats. This effect appears to be mediated, at least in part, through an enhanced direct inhibition of the excitability of trigeminal ganglia neurons, likely through enhancing binding of OT to its trigeminal ganglia OT receptors.
Disclosure of Interest
D. Yeomans Conflict with: Trigemina, Inc., S. Kori Conflict with: Trigemina, Inc., Conflict with: Trigemina, Inc, Conflict with: Trigemina, Inc
Migraine Preventive Therapy
PO-01-098
Efficacy of diet restriction on migraine
Akçay Övünç Özön1, Ömer karadaş2 and Aynur Özge3,*
1Neurology, Kemerburgaz University, Istanbul
2Neurology, Gülhane Training and Research Hospital, Ankara
3Neurology, Mersin University School of Medicine, Mersin, Turkey
Objectives
Migraine type headache is a very common headache, but its pathogenesis is still not fully understood. It varies from person to person, and there are many factors that trigger a migraine. Foods take an important place among these factors. In this study, the efficacy of food limitations triggering migraine in the prevention of migraine attacks was investigated
Methods
Patients diagnosed with a migraine without aura according to International Classification of Headache were included in the study. 50 migraine patients stating that migraine attack started after the intake of certain foods were evaluated. The patients were divided into 2 groups randomly. The foods triggering migraine identified for patients were excluded from the diet of the patients both in group 1 (N = 25) and group 2 (N = 25). Attack frequency in a month, attack duration and attack severity (by using the Visual Analogue Scale) were recorded before starting the diet restriction and 2 months after the diet restriction. Diet restriction was removed in the patients in group 1 after the second month; however, diet restriction continued in group 2, and in the fourth month, attack frequency in a month, attack duration and attack severity (using the Visual Analogue Scale) were determined in both groups
Results
A total of 50 patients consisting of 9 males and 41 females were evaluated in this study. In both groups, in the 2nd month after the diet application, attack frequency in a month, attack duration and attack severity were detected to be statistically lower to a significant extent compared to the period before diet implementation (p < 0.05). In the evaluation in the fourth month, it was observed that this significance continued only in group 2
Conclusion
The results of the study reveal that if the foods triggering migraine attacks are identified in migraine patients, restricting these foods from the diet can be an effective and reliable treatment method to reduce migraine attacks
Disclosure of Interest
None Declared
Migraine Preventive Therapy
PO-01-099
The clinical efficacy of short-lasting ketogenic diet in migraine is due to a general normalization of cortical hyperresponsivity rather than to a direct modulation of the brainstem activity
Cherubino Di Lorenzo1,*, Gianluca Coppola2, Martina Bracaglia3, Ilaria Bove3, Davide Di Lenola3, Mariano Serrao3, Vincenzo Parisi2 and Francesco Pierelli4
1Department of Neurology, Don Carlo Gnocchi Foundation, Milan
2Research Unit of Neurophysiology of Vision and Neurophthalmology, G. B. Bietti Foundation IRCCS, Rome
3Department of medico-surgical sciences and biotechnologies, Sapienza University of Rome Polo Pontino, Latina
4Headache Clinic, INM Neuromed IRCCS, Pozzilli, Italy
Objectives
We previously reported that a short-lasting period of ketogenic diet (KD) regimen can help to prevent migraine and can normalize its interictal abnormal cortical hyperresponsivity. Here, we aimed to verify whether cerebral cortex is the primary site of KD-related changes or if the latter are the expression of ketones ability to modulate brainstem subcortical structures.
Methods
We simultaneously recorded the nociceptive specific blink (nBR, a marker of the brainstem trigeminal activity) and cortical pain-related evoked potentials (PREP) elicited by the stimulation of right the supraorbital division of the trigeminal nerve in 18 migraine without aura patients before and after 1-month of KD, during ketogenesis. We measured nBR R2 component as well as PREP amplitude habituations over 2 blocks of 5 averaged responses.
Results
We confirmed the ability of 1-month KD of significantly decreasing mean attack frequency and duration. KD significantly induced normalization of the interictally reduced PREP habituation (pre: +1.8, post: −9.1), while nBR habituation remained unchanged.
Conclusion
The results of the present study suggest that the clinical efficacy of a short-lasting KD regimen in migraine can be primarily due to a general normalization of the interictal cortical dysfunction, and not to a direct modulation of the subcortical brainstem activation.
Disclosure of Interest
None Declared
Migraine Preventive Therapy
PO-01-100
75% responder rate provides greater improvement in domain scores of the SF-36 than the historically accepted 50% responder rate
Richard Lipton1,*, Joel Saper2, Jeff Smith3, Peter J. Goadsby4, David Dodick5, Roger Cady3 and Joe Hirman6
1Neurology, Montefiore Headache Center, Department of Neurology, Albert Einstein College of Medicine, Bronx
2Michigan Head Pain & Neurological Institute, Ann Arbor
3Alder BioPharmaceuticals, Bothell, United States
4NIHR-Wellcome Trust King's Clinical Research Facility, London, United Kingdom
5Neurology, Mayo Clinic, Phoenix
6Pacific Northwest Stats, Bothell, United States
Objectives
Historically, successful prophylactic therapy in migraine is defined as a 50% reduction in migraine days, paralleling the efficacy of many available preventive medications. Patients with chronic migraine (CM) experiencing a 50% reduction of migraine often continue with frequent migraines and potential impairment of quality of life (QOL). The Short-Form Health Survey (SF-36) questionnaire is a widely used validated measure of disease burden. ALD403 (eptinezumab) is a genetically engineered humanized anti-CGRP antibody, for migraine prevention. In a Phase 2b clinical trial in patients with CM, a single intravenous (IV) administration of ALD403 (eptinezumab) demonstrated a reduction in migraine days with efficacy maintained from week 1 through 12 weeks. We compare the impact of different responder rates for weeks 1–12 on SF-36 scores following infusion of 300 mg and 100 mg of ALD403 or placebo in that trial.
Methods
Domain; Mean SF-36 Domain Scores at Week 12 Among ≥75% Responders Baseline/12 Week/Change (n = 93)

Results
Chronic migraine had a unique pattern of disease impact as measured by the SF-36. Baseline domain scores with the greatest impact were role physical (RP), bodily pain (BP), and social functioning (SF). Persons achieving a ≥75% RR for weeks 1–12 showed improvement in all SF-36 domain scores with mean scores being >50 for all domains and average increases ranging from 1.9–7.1. Greatest improvement was noted in the domains most impacted by migraine. Patients with a ≥50% RR improved to a lesser degree and those with <25% RR showed a low degree of change. More subjects achieved ≥75% RR with ALD-403 than placebo (33.3%, 31.4% and 20.7% for 300 mg, 100 mg and placebo respectively, one-sided, p-values 0.016 and 0.039).
Conclusion
SF-36 domain scores provided a unique pattern of impact with the RP, BP, and SF being the most impacted SF-36 domains. ≥75% RR resulted in improvements in all SF-36 domain scores with mean scores being >50 for all domains for the weeks 1–12 analysis. The domains most impacted by migraine showed the most improvement. ≥50% RR improved to a lesser degree and <25% RR resulted in an even lower degree of improvement. These data suggest that SF-36 may be a valuable outcome tool for CM and that a ≥75% RR tends to normalize all SF-36 domains, with significantly more subjects achieving a ≥75% RR with ALD403 (eptinezumab) than placebo.
Disclosure of Interest
R. Lipton Conflict with: Alder BioPharmaceuticals, J. Saper Conflict with: Alder BioPharmaceuticals, J. Smith Conflict with: Alder BioPharmaceuticals, Conflict with: Alder BioPharmaceuticals, P. Goadsby Conflict with: Alder BioPharmaceuticals, D. Dodick Conflict with: Alder BioPharmaceuticals, R. Cady Conflict with: Alder BioPharmaceuticals, Conflict with: Alder BioPharmaceuticals, J. Hirman Conflict with: Alder BioPharmaceuticals
Migraine Preventive Therapy
PO-01-101
Predicting treatment response to candesartan in migraine patients
Roberta Messina1,* and Peter J. Goadsby2,3
1Headache Group, Department of Basic and Clinical Neuroscience, King’s College London
2Headache Group, Department of Basic and Clinical Neuroscience, King’s College London
3NIHR-Wellcome Trust King’s Clinical Research Facility, King’s College Hospital, London, United Kingdom
Objectives
Recent randomised studies reported a positive effect of candesartan, an angiotensin II receptor antagonist, in migraine prevention. The aim of our study was to identify response predictors to candesartan in a sample of migraine patients.
Methods
We retrospectively reviewed the clinical records of patients who have attended the Headache Clinic from February 2015 to December 2016, looking specifically at their response to candesartan. Univariate and multivariate logistic regression models were used to assess for predictors of outcome. Odds ratios (OR) with confidence intervals (CI) 95% were also calculated.
Results
The clinical history of 118 migraine patients was reviewed. A total of 104 patients (84 females, 81%), with a mean age of 43 (range: 17–77), were included in the final analysis. Fourteen patients were excluded cause to missing data. Thirty-two (31%) patients reported a positive response to candesartan, while 72 (69%) did not have any significant therapeutic effect. In the univariate logistic regression analysis, no one of the predictors was associated with the outcome. In the multivariate logistic regression model including a positive history of triptan-overuse headache, the number of migraine days per month, disease duration, presence of aura, presence of allodynia, presence of cranial autonomic symptoms and the total number of preventive therapies tried by patients, a positive history of triptan-overuse headache was associated with higher odds of a positive response to candesartan (OR 6.37, 95% CI 1.73–23.46, p = 0.03).
Conclusion
Patients with triptan-overuse headache might benefit from taking candesartan. On the other hand, neither the disease activity or migraine associated symptoms nor the number of preventive treatments tried by patients can help us to predict the response to candesartan in migraine patients.
Disclosure of Interest
R. Messina: None Declared, P. Goadsby Conflict with: Allergan, Amgen, and Eli-Lilly and Company., Conflict with: Allergan, Amgen, Eli-Lilly and Company, Akita Biomedical, Alder Biopharmaceuticals, Autonomic Technologies Inc, Avanir Pharma, Cipla Ltd, Colucid Pharmaceuticals, Ltd, Dr Reddy's Laboratories, eNeura, Electrocore LLC, Novartis, Pfizer Inc, Promius Pharma, Quest Diagnostics, Scion, Teva Pharmaceuticals, Trigemina Inc., Scion; and in addition, Dr. Goadsby has a patent Magnetic stimulation for headache pending assigned to eNeura, Conflict with: MedicoLegal work, Journal Watch, Up-to-Date, Oxford University Press
Migraine Preventive Therapy
PO-01-102
Long term results for occipital nerve stimulation in refractory chronic migraine
Pedro E. Bermejo1,* and Cristina del Pozo2
1Neurology
2Puerta de Hierro, Majadahonda (Madrid), Spain
Objectives
Although some prophylactic medications have been proposed to treat chronic migraine (CM) there are still many refractory patients and other treatments are warranted. Occipital nerve stimulation is a potentially promising therapy for CM patients, although long term experience is scarse.
The aim of this study is to evaluate the long term efficacy and tolerability of occipital nerve stimulation for the treatment of refractory CM.
Methods
Twenty eight patients (12 men, 16 women, average age 53.9 ± 12.1) meeting the IHS criteria for refractory CM were enrolled in this study and implanted with a neurostimulation device near the occipital nerves. The primary endpoint was the reduction in Analogical Visual Scale (AVS). Patient satisfaction, migraine frequency, side effects and reasons for discontinuation were also studied. Significance level was set at P < 0.05.
Average follow up period was 6.7 ± 2.2 years.
Results
Headache severity according to the AVS was reduced from 8.7 ± 0.2 before occipital nerve stimulation to 3.6 ± 2.8 after treatment initiation. There was also a significant difference in reduction of number of headache days and 80% of the patients were satisfied or very satisfied with the procedure. The most common adverse event was persistent implant site pain and only one patient required to be explanted due to inefficacy. Good efficacy and tolerability were maintained after the follow-up period.
Conclusion
Occipital nerve stimulation has been explored as a possible treatment option in selective drug-resistant primary headache disorders and, according to our results, this technique may be effective, safe and well tolerated in treating refractory CM. These good results seem to remain stable after several years.
An increasing experience and a more routine use of these techniques can be forecasted in the near future.
Disclosure of Interest
None Declared
Neuromodulation for Headache
PO-01-103
Novel use of Radiofrequency Ablation in a case of a severely refractory New Daily Persistent Headache
Matthew Chung1,*, Emil Gaitour1, Olga Fermo1 and Charles Brock2
1Neurology
2University of South Florida, Tampa, United States
Objectives
New daily persistent headache (NDPH) is a severely refractory headache disorder with a chronic, daily persistence from date of onset without specific guidelines for treatment. Despite management of NDPH being aimed towards treatment of the predominant headache phenotype, this headache disorder continues to be resistant to the most aggressive measures implemented by headache providers. Radiofrequency ablation is an neuro-ablative procedure implemented by interventional pain physicians that has been commonly applied to the treatment of chronic disorders including the neck, back, joint as well as intercostal neuralgia. There are multiple studies and growing use of RFA in the headache community in the management of other headache disorders including cervicogenic headache, trigeminal neuralgia, hemicranias continua, and occipital neuralgia that have shown promising results. We present a case in a veteran with NDPH who was refractory to all treatment modalities over the last two decades until RFA was introduced and has since provided significant and long lasting relief over the last years.
Methods
Conventional RFA utilizes alternating currents to create a thermal lesion along a targeted nerve via an intricately placed needle. The targeted nerve is isolated under image guidance (with use of anatomical landmarks, ultrasound or fluoroscopy) and is followed by generating a temperature between 80–85 degrees at the tip of the uninsulated needle via an alternating current for approximately 60–90 seconds to create an adequately sized lesion. Creation of this lesion involves the disruption of the neuronal architecture without compromising the fascicular structure itself. The incurred lesion serves as a temporizing block, preventing transmission of nociceptive signals along the target nerve. We targeted the greater occipital, the lesser occipital and the supraorbital nerve as sites for neuromodulation in this case.
Results
We present a 47-year-old male veteran with migraine variant NDPH, whose initial headache presentation began following an incident while active duty wherein he was enveloped with an unknown chemical from an overhead missile and subsequently lost consciousness with no injuries to report of otherwise. His headaches over the next two decades were unsuccessfully treated with numerous ablative therapies (including sumatriptan, NSAIDs, and methadone), preventative therapies (including propranolol, metoprolol, topiramate, valproate, gabapentin, pregabalin, levetiracetam, lamotrigine, amitriptyline, nortriptyline, paroxetine, venlafaxine, indomethacin, and onabotulinum toxin A) as well as cervical branch blocks. This patient’s daily headache was debilitating, requiring daily and frequent high dose opiate use and becoming functionally dependent on his family. With the introduction of conventional RFA on a biannual basis 6 years from present day, he has tapered himself from these opiates, is back to work on a full time basis with regained independence. He is pain free for a most of the days of the month with occasional mild headaches and at most, three severe headache days in a month. Additionally, he has not experienced nor encountered any side effects or neurologic sequelae on exam since starting this ablative therapy.
Conclusion
Thermal lesions created along targeted nerves as facilitated by conventional RFA can serve as a potentially safe, effective, and alternative means for treatment of NDPH as demonstrated in the case of this veteran. RFA has been similarly applied with success to other refractory chronic headache disorders, but to the knowledge of our authors, there are no published reports using conventional RFA to treat NDPH.
Disclosure of Interest
None Declared
Neuromodulation for Headache
PO-01-104
Prevention of frequent episodic migraine and chronic migraine with a supraorbital transcutaneous stimulator in Japan
Daisuke Danno1,*, Miho Iigaya2, Noboru Imai3, Hisaka Igarashi4 and Takao Takeshima5
1Division of Neurology, Department of Internal Medicine, Hyogo College of Medicine, Hyogo
2Department of Neurology, Kitasato University, Kitasato Institute Hospital, Tokyo
3Department of Neurology, Japanese Red Cross Shizuoka Hospital, Shizuoka
4Headache Care Unit, Fujitsu Clinic, Kanagawa
5Department of Neurology, Headache Center, Tominaga Hospital, Osaka, Japan
Objectives
To examine the preventive effect for frequent episodic migraine and chronic migraine of a supraorbital transcutaneous stimulator (Cefaly®; Cefaly Technology, Grâce-Hollogne, Belgium) in Japan.
Methods
Patients were prospectively collected from four headache units in Japan between April 7 and September 6, 2016. The inclusion criteria for the study were as follows: age 18–65 years old, migraine with and without aura (International Headache Classification 3rd Edition beta version Code 1.1, and 1.2.1.1), and at least two attacks per month. The patients who started or changed their prophylactic treatment and had received botulinum toxin type A or a nerve block injection within the previous three months were excluded. The migraine patients with secondary headache except for medication overuse headache were also excluded. After four weeks of a run-in phase, the patients started the active phase for 12 weeks, in which they were stimulated by Cefaly® with the following characteristics: square wave, pulse width 300 µsec, frequency 60 Hz, maximum 16 mA, and 20 minutes every 24 h. The headache status was recorded every day in an electronic headache diary (Zutsuclick®; J-MAC SYSTEM, INC., Sapporo, Japan). We analyzed the change in the number of migraine days between the run-in month and the second and third months. We also evaluated the comprehensive effectiveness as the following three degrees: improved, no change, and deteriorated. Furthermore, we measured the patients’ satisfaction using a questionnaire.
Results
A total of 100 patients (19 males, 81 females) were analyzed; 95 completed the study in accordance with the protocol. The average age at the study initiation was 43.5 years in males and 44.7 years in females. Seventy-four cases were diagnosed with migraine without aura, 40 with chronic migraine, 9 with migraine with aura, and 5 with chronic migraine with medication overuse. Regarding the effectiveness, 74 cases improved (highly improved in 20 cases, moderately improved in 31 cases, mildly improved in 23 cases), 24 saw no change, and 2 deteriorated. Regarding the satisfaction, 63 were satisfied, 24 were dissatisfied, and 9 had no opinion. Adverse events were reported in seven patients: pain or discomfort at the site of stimulation in three patients, sleepiness in two patients, fatigue in one patient, and headache in one patient. All of the adverse events were mild to moderate, and there were no severe adverse events.
Conclusion
Supraorbital transcutaneous stimulation for frequent episodic migraine and chronic migraine is thought to be an effective and relatively safe treatment. In this study, the supraorbital transcutaneous stimulator (Cefaly®) was offered by IMI Co., Ltd. (Saitama, Japan). We also received technical cooperation with the J-MAC SYSTEM for the electronic headache diary (Zutsuclick®).
Disclosure of Interest
D. Danno Conflict with: In this study, the supraorbital transcutaneous stimulator (Cefaly®) was offered by IMI Co., Ltd. (Saitama, Japan). We also received technical cooperation with the J-MAC SYSTEM for the electronic headache diary (Zutsuclick®)., M. Iigaya Conflict with: In this study, the supraorbital transcutaneous stimulator (Cefaly®) was offered by IMI Co., Ltd. (Saitama, Japan). We also received technical cooperation with the J-MAC SYSTEM for the electronic headache diary (Zutsuclick®)., N. Imai Conflict with: In this study, the supraorbital transcutaneous stimulator (Cefaly®) was offered by IMI Co., Ltd. (Saitama, Japan). We also received technical cooperation with the J-MAC SYSTEM for the electronic headache diary (Zutsuclick®)., H. Igarashi Conflict with: In this study, the supraorbital transcutaneous stimulator (Cefaly®) was offered by IMI Co., Ltd. (Saitama, Japan). We also received technical cooperation with the J-MAC SYSTEM for the electronic headache diary (Zutsuclick®)., T. Takeshima Conflict with: In this study, the supraorbital transcutaneous stimulator (Cefaly®) was offered by IMI Co., Ltd. (Saitama, Japan). We also received technical cooperation with the J-MAC SYSTEM for the electronic headache diary (Zutsuclick®).
Neuromodulation for Headache
PO-01-105
Anodal transcranial direct current stimulation over the left temporal pole restores normal visual information processing in migraine patients
Francesca Cortese1,*, Gianluca Coppola2, Ilaria Bove1, Vincenzo Parisi2 and Francesco Pierelli1,3
1Department of Medico-Surgical Sciences and Biotechnologies, Sapienza University of Rome Polo Pontino, Latina
2Department of Neurophysiology of Vision and Neurophthalmology, G. B. Bietti Foundation-IRCCS, Rome
3IRCCS-Neuromed, Pozzilli (IS), Italy
Objectives
Many neuroimaging studies have implicated the temporal pole (TP) in migraine pathophysiology; its morphology and function were reported to change per the so-called migraine cycle. The link between TP morphology changes and the electro functional abnormalities of the migraine brain is unknown. In humans, the TP serves as a multimodal neural hub that receives and integrates all sensory modalities except for somatosensory information. Here, we aim to verify whether a non-invasive enhancement of TP excitability by means of anodal transcranial direct current stimulation (tDCS) may change the interictal abnormal multimodal sensory processing in migraine.
Methods
Thirty-two interictal migraineurs underwent visual (VEPs, 600 sweeps, 3.1 Hz reversal rate, 15 min of arc check) and median nerve somatosensory (SSEPs, 200 sweeps, 4.4 Hz) evoked potentials before and immediately after 20-minute real anodal tDCS (N = 16) or sham (N = 16) delivered over the left TP (2 mA, cathode placed on the right arm). We measured VEPs N1-P1 and SSEPs N20-P25 amplitudes respectively in 6 and in 2 sequential blocks of 100 sweeps as well as habituation as the slope of the linear regression between block 1 to 6 for VEPs or between 1 to 2 for SSEPs.
Results
Before tDCS or sham, migraine patients lacked habituation in response to both visual (+0.09, +0.05 respectively in the tDCS and sham group) and somatosensory (+0.5, +0.2) repetitive stimulations. After anodal tDCS but not sham stimulation, migraine patients showed normalization of the interictal habituation deficit in response to visual (−0.25, p = 0.01), but not to somatosensory (+0.3) repetitive stimulations.
Conclusion
Our study shows for the first time that excitability enhancer tDCS over the TP could significantly normalize the interictal abnormal visual information processing in migraine, and that this was not so for the somatosensory modality. This distinct cortical finding in response to tDCS could be related to the fact that the temporal pole belongs to the so-called ventral stream of the visual pathway.
Disclosure of Interest
None Declared
Neuromodulation for Headache
PO-01-106
Neuromodulation by electroacupuncture for migraine without aura Analysis using Diffusion Tensor Imaging
Sumire Ishiyama1,*, Yasushi Shibata2,3, Satoshi Ayuzawa4, Akira Matsushita5 and Akira Matsumura2
1Department of Neurosurgery, Graduate School of Comprehensive Human Sciences, University of Tsukuba
2Department of Neurosurgery, University of Tsukuba, Tsukuba
3Neurosurgery/Headache clinic, Mito kyodo general hospital, Mito
4Faculty of Health Sciences, Tsukuba University of Technology, Tsukuba
5Department of Neurology, Ibaraki Prefectural University of Health Sciences Hospital, Ami, Japan
Objectives
Migraine is one of the most common diseases. Medication therapy is the first choice for primary headache, but some patients show resistance for medical therapy. Recently, neuromodulation such as peripheral nerve field stimulation (PNfS) is used for the treatment of migraine and neuralgia. Further more, in the group of patients with fibromyalgia PNfS for Cervical 2 area (C2 PNfS) is reported as effective for headache, trunk pain and depression. However, PNfS requires implantation surgery, so some complications such as infection and hardware erosion were reported. In addition, the mechanism of PNfS has not yet been fully understood. In this study, we investigated whether electro-acupuncture could reproduce the effects of C2 PNfS (EAP-C2-PNfS).
Methods
A board accredited headache physician diagnosed the headache using the International Classification of Headache Disorders 3rdβ edition (ICHD-3β). The 36 patients were diagnosed as migraine without aura (MWoA) (4 men, 32 women, mean age 46.2 ± 13.2 years-old) and they underwent 3.0T MRI (SIEMENS, Erlangen, Germany) with 32-channel head coil including Diffusion Tensor Imaging(DTI) before and after EAP-C2-PNfS. We assessed headache intensity using Numerical rating scale (NRS). We measured the impact of headache on daily disability using Short-form 36 (SF-36) and Headache Impact Test (HIT-6). We used self-rating depression scale (SDS) as the depression assessment tool. Each scale was evaluated before and after EAP-C2-PNfS.
The acupuncture needles (50 mm length, 0.18 mm diameter, SEIRIN JSP-type, Shizuoka, Japan) were subcutaneously inserted into the bilateral occipital scalp about 15 to 20 mm and biphasic electrical pulse waves were applied for 15 minutes using electrical stimulator. The EAP-C2-PNfS was performed once per a week for 3 months.
The DTI were acquired by single-shot echo planar imaging (EPI) (TR = 6800 ms, TE = 75 ms, Nex = 1, GRAPPA factor = 2, b values is 0 and 1000 s/mm2, 20 motion proving gradient) with 50 axial slices (slice thickness = 3 mm, no gap, field of view = 230 × 230 mm2, matrix size = 128 × 128 mm2). The DTI scan time was 5 minutes 21 seconds.
For imaging analysis, we used tract-based spatial statistics (TBSS) in Oxford Centre for Functional MRI of the Brain (FMRIB) Software Library (FSL). Using this software, we analyzed Fractional anisotropy (FA) in whole brain.
Results
Clinical indexes of NRS, HIT-6, SF-36 and SDS significantly improved after 3 months of EAP-C2-PNfS. On the other hand, FA decreased at some brain regions such as right thalamus, right minor forceps, right internal capsule and bilateral corpus callosum. All subjects showed no adverse event with EAP-C2-PNfS.
Conclusion
Recently some reports suggest that functional dysfunction and central sensitization are present in pathology of chronic headache such as migraine. In DTI studies for MWoA, the patients at interictal phase showed increased FA in bilateral thalamus compared with those of healthy control. On the other hand, there are studies that report no significant difference of FA values among 3 groups: chronic, episodic migraine and healthy control.
Right hemisphere is involved in cognitive aspect of pain. Our study showed that FA decrease in right hemisphere, so EAP-C2-PNfS may be effective by inhibiting neural activity in right hemisphere.
In this study, clinical indexes of headache and depression were significantly improved and right hemisphere FA decreased after EAP-C2-PNfS for 3 months. EAP-C2-PNfS is low invasive and safe procedure. This study indicated that EAP-C2-PNfS is effective by neuromodulation for MWoA.
Disclosure of Interest
None Declared
Neuromodulation for Headache
PO-01-107
Effects of Occipital Nerve Stimulation on Cerebral Blood Flow in Patients with Medically Intractable Chronic Cluster Headache
Ilse F. De Coo1,*, Jasper van der Aart2,3, Leopoldine A. Wilbrink1, Patty G. Doesborg1, Hannan Abrabi3, Maqsood Yaqub3, Adriaan A. Lammertsma3 and Michel D. Ferrari1
1Neurology, Leiden University Medical Center
2Centre for Human Drug Research, Leiden
3Radiology & Nuclear Medicine, VU Medical Center, Amsterdam, Netherlands
Objectives
Pilot studies have suggested that occipital nerve stimulation could be effective in medically intractable chronic cluster headache. It is currently not known how occipital nerve stimulation affects cerebral blood flow (CBF) and whether clinical outcome is related to changes in CBF. Here, we assessed the effects of occipital nerve stimulation on both attack frequency and CBF.
Methods
CBF was measured using dynamic [15O]H2O PET scans before (‘baseline’) and after six months treatment with occipital nerve stimulation in 17 medically intractable chronic cluster headache patients. A low-dose CT scan was performed immediately before each [15O]H2O scan to correct the latter for attenuation. Emission data were acquired for 10 minutes following intravenous injection of 800 MBq [15O]H2O. In addition, arterial blood was sampled continuously during this scan. A co-registered cerebral structural T1 weighted MRI scan was used for segmentation of volume of interest. CBF was obtained by fitting region of interest time-activity curves to the standard single tissue compartment model for [15O]H2O using the arterial blood curve as input function.
The primary outcome was the effect of the absolute change in attack frequency on the CBF in our regions of interest (i) associated with pain processing (ACC, insula, thalamus, cerebellum, pons), as well as (ii) the area near the occipital nerve stimulator: occipital lobe, and (iii) the hypothalamus associated with cluster headache attacks.
Results
At baseline, age correlated significantly with CBF (p = 0.02). Cluster headache attacks were significantly reduced from 64.4 at baseline to 32.4 after 6 months occipital nerve stimulation (p = 0.01). An increase in CBF in the contralateral ACC (p = 0.001) and ipsilateral hypothalamus (p = 0.035) were significantly associated with a reduction in absolute attack frequency corrected for age, gender and baseline attack frequency. Change in CBF in other regions of interest did not correlate with a change in cluster headache attacks.
Conclusion
This is the first report of changes in CBF following occipital nerve stimulation in medically intractable chronic cluster headache. Reduction in attack frequency was associated with an increase in CBF in both ipsilateral hypothalamus and contralateral ACC.
Disclosure of Interest
None Declared
Neuromodulation for Headache
PO-01-108
Long term experience in peripheral nerve stimulation in drug-resistant cranial neuralgias
Pedro E. Bermejo1,* and Cristina del Pozo1
1Puerta de Hierro, Majadahonda (Madrid), Spain
Objectives
Cranial neuralgias are distinct, treatable syndromes which comprise one of the possible causes of facial pain. Although some prophylactic medications and techniques have been proposed as treatments, there are still many refractory patients and other therapeutic options are warranted. Peripheral nerve stimulation (PNS) has been proposed as a promising therapy for these patients although long term experience is scarse.
The aim of this study is to evaluate the long term efficacy and tolerability of PNS for the treatment of refractory cranial neuralgias
Methods
Sixteen patients (5 men, 11 women, average age 51.0 ± 11.3) suffering from different drug-resistant cranial neuralgia were enrolled and implanted with a neurostimulation device. Six suffered from occipital neuralgia, 6 had postherpetic neuralgia and 4 had trigeminal neuralgia. The primary endpoint was the reduction in Analogical Visual Scale (AVS). Patient satisfaction, side effects and reasons for discontinuation were also studied. Significance level was set at P < 0.05.
Average follow-up period was 6.1 ± 1.3 years.
Results
Pain severity according to the AVS was reduced from 8.7 ± 1.1 before PNS to 4.9 ± 2.7 after treatment initiation. 55% of treated patients were satisfied or very satisfied with the procedure. The most common dverse event was persistent implant site pain and three patients required to be explanted due to inefficacy. There were not differences between different subgroups.
Efficacy and tolerability remained stable during the follow-up period.
Conclusion
PNS has been explored as a possible treatment option in selective drug-resistant cranial neuralgias and, according to our results, this technique may be effective, safe and well tolerated in treating them in the long term. More studies are warranted to confirm these results.
Disclosure of Interest
None Declared
Other Primary Headache Disorders
PO-01-109
Subjective Hyperosmia in Burning Mouth Syndrome: The Burn and the Smell
Rohin Dhir1,*, Wannapak Richter2 and Alan R. Hirsch3
1Aureus University School of Medicine, Oranjestad, Aruba
2Ramathibodi Hospital, Mahidol University, Bangkok, Thailand, Thailand
3Neurology, Smell and Taste Treatment and Research Foundation, Chicago, United States
Objectives
While hypogeusia (Grushka, 2002) and hyposmia (Yakov, 2010) have been noted in those with burning mouth syndrome (BMS), neither subjective nor true hyperosmia heretofore have been described. Such a case is presented.
Methods
A 45 year old woman, six weeks after beginning treatment with duloxetine, quetiapine and alprazolam for an episode of Major Depression and Generalized Anxiety Disorder, noted a gradual onset of oral irritation while eating spicy foods. This progressed over the following year to a constant burning sensation in the anterior tongue and palate, independent of eating. Initially mild, this became more severe (10/10 at night), and she was diagnosed with BMS. One and a half years after burning onset, she perceived hyperosmia, whereby smells were more intense than normal. For instance, the aroma of perfume, cleaning supplies, spices, dog feces, tomato sauce, pizza, orange juice and other citrus scents were 200% greater than the normal smell; cinnamon, onions, and shampoo were 120% greater than normal.
Results
Abnormalities in neurological examination: Cranial Nerves: III: Left ptosis. Motor: Drift testing: Left abductor digiti minimi sign. Reflexes: 3+ throughout. Positive jaw jerk. Chemosensory testing: Olfaction: Brief Smell Identification Test: 3 (anosmia). Quick Smell Identification Test: 1 (anosmia). Alcohol Sniff Test: 3 (anosmia). Pocket Smell Test: 3 (normosmia). Sniff Magnitude Test: ratio 1.49 (anosmia). Odor Memory Test: 0 at 10 seconds, 4 at 30 seconds, 2 at 60 seconds. Total 6 (hyposmia). SNAP Phenylethanyl Olfactory Threshold Test: Left > −2.0, Right > −2.0 (anosmia). Olfactometer Identification test: Left 18 (normosmia), Right 14 (hyposmia). Sniffin’ Sticks Threshold: Left < 1, Right < 1, Bilateral <1 (anosmia); Bilateral Discrimination test: 8 (hyposmia); Bilateral Identification test: 10 (hyposmia). Suprathreshold Amylacetate Odor Intensity Test: Normosmia. Suprathreshold Amylacetate Odor Hedonic Test: Crossed pattern (abnormal). Retronasal Olfaction: Retronasal Smell Index: 6 (normal). Gustation testing: Propylthiouracil Disk Taste Test: 2 (hypogeusia). Taste Threshold and Suprathreshold Testing: Normogeusia to urea and phenylthiocarbamol; hypogeusia of 10–30% to sodium chloride, sucrose and hydrochloric acid. Taste Quadrant Test: Sucrose impaired throughout the tongue and palate. Reduced ability to taste anteriorly to all modalities. Alcohol and carbonated water: Normal. Fungiform papillae count: Right 24, Left 18. Piesethesiometry: Tongue normal. Saxon test: 3 (normal). Electrogustometry testing: Left palate >34, Right palate >34, Left anterior tongue: 22, Right anterior tongue: 24, Left posterior tongue: 14, Right posterior tongue: 14. Neuropsychiatric Testing: Clock Drawing Test: 4 (normal), Animal Fluency Test: 27 (normal). Center for Neurological Studies Lability scale: 10 (normal). Zung Anxiety scale: Anxiety Index: 46 (minimal to moderate anxiety). Beck Depression Inventory type II: 15 (probable depression).
Conclusion
Burning pain often causes depression, which may induce the patient to focus more on the chemosensory system (Lorig, 1988). With concentrated attention, there is activation of afferent sensory systems, inducing sensory stimuli to be perceived as more intense (Hummel, 2006). Furthermore, odors may worsen BMS (Hirsch, 2004), and thus the patient may be focused on odors to avoid precipitating BMS. Moreover, patients with BMS are often supertasters and supersmellers (Bartoshuk, 1998), and a supersmelling patient may actually perceive smell as greater than others. Query as to subjective hyperosmia in those with BMS is warranted.
Disclosure of Interest
R. Dhir: None Declared, W. Richter: None Declared, A. Hirsch Conflict with: Institute for Personal Development; Advance Psychiatry and Counseling, Conflict with: Nestle Health Science - Pan Lab Inc., Conflict with: CRC Press
Other Primary Headache Disorders
PO-01-110
Sumatriptan Responsive Olfactory Hallucinations: Treatment of Phantosmia of Amigrainous Migraine
Brittany Avonts1,*, Kamran Hanif2 and Alan R. Hirsch3
1Neuropsyciatry, Lake Forest College, Lake Forest, United States
2Neuropsychiatry, Carribean Medical University, Willestamd, Curaçao
3Neuropsychiatry, Smell and Taste Treatment and Research Institute, Chicago, United States
Objectives
While olfactory hallucinations have been described as an aura to migraine (Podoll, 2004; Henkin, 2013) it is not a recognized type of migraine aura according to the International Classification of Headache Disorders (Mainardi, 2015). Olfactory hallucinations have been described persisting into the headache phase and even as a manifestation of migraine without headache (Henkin, 2013). No patients with phantosmia as a manifestation of amigrainous migraine responsive to treatment with sumatriptan, has heretofore been described.
Methods
Methods: Case study: A 27-year-old left handed (pathological) female, 7 years prior to presentation noted intermittent olfactory hallucinations of dried blood and rotten sour eggs, which was reduced with lacrimation. The phantosmia occurred several times per week. Once it is present it will persist the entire day and it has progressed in frequency to every day. It is made worse with stress and 70% of the time it is precipitated with sneezing. It is made better with holding her breath or occluding her nostrils. She admits to getting ice cream headaches, bloating with her menses and frequently fainted as a child. The headaches are holocephalgic, associated with light-headedness and nausea. The phantosmia would usually accompany the light-headedness and nausea even when the headaches were not manifest. She is not impaired by the headaches and there is no dirurnal variation to the headaches. Phantosmias are usually level 8/10 in intensity. She was unresponsive to lamotrigene, carbamazepine, gabapentin, zinc, acupuncture, and aromatherapy. Trial of sumatriptan 25 mg reduced the intensity to 5/10 a half hour later and after another 5 mg reduced the intensity to a level 2/10 which remained reduced for 5 hours until she fell asleep, returning the next day. Recurrent trial on sumatriptan had a similar effect.
Results
Abnormalities in Physical Examination: General: bilateral palmar erythema. Neurological Status Examination: Mental Status Examination: Memory testing: Immediate recall: 5 digits forwards and backwards. Proverbs (concrete). Cranial Nerve Examination (CN): CN IX and X: gag absent, uvula deviated to left. Motor Examination: Drift Testing: left upward drift and bilateral abductor digiti minimi sign. Reflexes: 3+ bilateral brachioradialis and quadriceps femoris. ankle jerks bilateral delayed return, bilateral positive Hoffman’s Reflexes. Chemosensory Testing: Olfactory Testing: Alcohol Sniff Test: 14 (hyposmia). Brief Smell Identification Test: 10 (normosmia). Retronasal Olfaction: Retronasal Smell Index: normal. Gustatory Testing: Propylthiouracil Disc Taste Test: 10 (normoguesia). Neuropsychiatric testing: Clock Drawing Test: 4 (normal), Animal Fluency Test: 21 (normal), Go-No-Go Test: 6/6 (normal). Other: normal 72-hour EEG, MRI, and fiberoptic endoscopy.
Conclusion
Phantosmia have been reported to respond to a variety of different medications including anticonvulsants (Majumdar, 2003), anti-depressants, anti-psychotics (Henkin, 2013), beta blockers and calcium-channel blockers (Coleman, 2011). This is the first recorded case of phantosmia responsive to sumatriptan. While the patient’s response to sumatriptan strongly suggests it is of a migrainous nature, other possibilities should be considered. The phantosmia may be a manifestation of serotonergic imbalance which sumatriptan modulates. Since, sumatriptan has been demonstrated to affect the chemosensory system (Doty, 2004) it may be acting on the olfactory system independent of its effects on headaches. This case suggests that trial with anti-migraine drugs or with other serotonergic agonists may be useful with treatment of phantosmia. Such an effect warrants further study.
Disclosure of Interest
None Declared
Other Primary Headache Disorders
PO-01-111
Evaluation of electroencephalogram using eLORETA during photic stimulation in patients with migraine
Tomohiko Shiina1,*, Ryotaro Takashima1, Roberto D. Pascual-Marqui2 and Hirata Koichi1; Department of Neurology, Dokkyo Medical University
1Neurology, Dokkyo University School of Medicine, Shimotsuga, Tochigi, Japan
2The KEY Institute for Brain-Mind Research, Zurich, Switzerland
Objectives
Migraine patients indicate various type of abnormal information processing. Photophobia may be one of abnormal information procession. In electroencephalograms(EEG), photic driving is known as a reaction to visual stimulation. Both photophobia and the photic driving response are similar to appear during light stimulation. We considered that evaluation of migraine patients photic driving response may lead to elucidation of the mechanism of their sensitive condition. Our study aimed to investigate EEG photic driving responses with a source-localizing method.
Methods
We recruited 50 migraine patients (migraine with aura (MWA) 21;migraine without aura (MWOA) 29). We recorded spontaneous eyes-closedresting EEG from 20 electrodes on the scalp during the interictal phase. Afterrecording, each photic stimulation was separately selected. We also analyzedEEG by fast Fourier transform and observed the spectrum frequency peaks andtopographies in response to photic stimulationWe recruited 50 migraine patients (migraine with aura (MWA) 21; migraine without aura (MWOA) 29). We recorded spontaneous eyes-closed resting EEG from 20 electrodes on the scalp during the interictal phase. After recording, each photic stimulation was separately selected. We also analyzed EEG by fast Fourier transform and observed the spectrum frequency peaks and topographies in response to photic stimulation.
Results
Photic stimulation at frequencies 5, 8, 15, 20 showed significant difference between the subtypes with and without aura. MWOA always had stronger response to photic stimulation than MWA. In all cases the differential response is located in visual cortex, except for 20 Hz stimulation, where the difference at subharmonic 10 Hz was located in parietal cortex (BA 7).
Conclusion
High incidences of photic hypersensitivity and photic drivingresponses in migraine patients were confirmed. It is considered that corticalfunction may be suppressed by repeated occurrence of CSD in MWA with lowactivity in the occipital region.
Disclosure of Interest
None Declared
Other Primary Headache Disorders
PO-01-112
New Daily Persistent Headache (NDPH): possible triggers for remission and relapsing
Yoshio Asano1,*, Yuichi Maruki1, Tomokazu Shimazu1, Chiaki Yanagisawa1, Masaaki Matsuzaki1 and Fumihiko Sakai2
1Neurology, Saitama Neuropsychiatric Institute
2Saitama International Headache Center, Saitama, Japan
Objectives
New daily persistent headache (NDPH) has two subforms: a self-limiting subform that typically resolves within several months and a refractory form that is resistant to pharmacological treatment. Previous studies showed that the prognosis of NDPH is poor and is resistant to treatment. We studied clinical features of NDPH to know the factors which may influence the prognosis of the disease.
Methods
A retrospective study was conducted at our headache center during the period of April 2014 to August 2015. All the patients with NDPH fulfilled the ICHD-3β. Secondary headaches were excluded by clinical and MRI studies. All the patients received pharmacologic treatment of various combination. The usefulness of integrated headache care including psychological counseling, acupuncture, daily life planning, physical therapy and yoga was also evaluated.
Results
Conclusion
We categorized NDPH patients in two group: non-persistent group (remission, remission/relapsing) and persistent group (continuous). Remission occurred more in the group of early clinic visit. Possible triggers were reported by the patients but we could not identify any specific triggers common to the onset of all the NDPH. Non-pharmacologic treatment or lifestyle ingenuity may also be considered as useful therapeutic option.
Disclosure of Interest
None Declared
Other Primary Headache Disorders
PO-01-113
Our current experience in infiltration in a series of patients with trigeminal neuralgia
Ane Minguez-Olaondo1,2,* and José Miguel Láinez1,3
1Neurology, Hospital Clínico Universitario de Valencia, Valencia
2Neurology, Clínica Universidad de Navarra, Pamplona
3Neurology, Universidad Católica de Valencia, Valencia, Spain
Objectives
Pharmacological treatment is first choice for the prophylactic management of trigeminal neuralgia (TN), but in some cases is ineffective or has unacceptable side effects. Botulinum Toxin A has been reported as effective in patients with TN. We represent our experience in a cohort of patients with TN.
Methods
Twelve patients (7 men, 5 women; age: 61–84 years-old) suffering from drug-refractory TN were treated. We injected 25–50 UI reconstituted Botulinum Toxin A solution in the trigger zone (V2-V3). The injection was repeated after 3 months depending on the clinical response.
Results
In 8 patients a decrease of more than 75% of the pain was obtained with a reduction also of prophylactic medication. Two patient's response was of 50% and the other two were no responders. Adverse events were no more than esthetical changes in face appearance in 7 patients. The duration of the efficacy was from 3 to 6 months.
Conclusion
Infiltration with Botulinum Toxin A is an alternative therapeutic treatment for patients with TN refractory to drugs. Adverse events are frequents but reversibles.
Disclosure of Interest
None Declared
Other Primary Headache Disorders
PO-01-114
Chronic paroxysmal hemicrania in paediatric age: report of four cases
Laura Papetti1,*, Samuela Tarantino1, Barbara Battan2, Federico Vigevano3 and Massimiliano Valeriani1
1Neuroscience, Bambino Gesù Children Hospital
2Neuroscience
3Bambino Gesù Children Hopsital, Rome, Italy
Objectives
Chronic paroxysmal hemicrania (CPH) is a rare and well-characterised headache, classified amongst the trigeminal autonomic cephalgias (TACs). CPH has been only rarely and incompletely described in the developmental age. The objective of the present report was to describe the features of chronic paroxysmal migraine in four pediatric patients.
Methods
MBCT-M Adaptation

Results
We detected 4 patients with CPH. Clinical features are reported in table 1. Our children presented with a long history of severe and unilateral pain, which occurred in the fronto-orbital region without side shift. Attacks were accompanied by at least one autonomic symptom, ipsilateral to pain. During the attacks, besides conjunctival injection, eyelid oedema and rhinorrhea and all children showed a dramatic response to indomethacin.
Conclusion
Here, we describe four patients with short-lasting, recurrent headache combined with cranial autonomic features. The clinical features of our children’s headache and the positive response to indomethacin led us to propose the diagnosis of CPH. Clinical symptoms and pain characteristics of our children are similar to those found in typical adult CPH. However in line with the previous cases of CPH reported during developmental age, our patients showed some atypical features, not fully meeting the ICHD-III beta criteria. First, although the ICHD criteria require an attack frequency higher than 5 attacks per day, in our patients, the attack frequency was lower. Second, attack duration was variable in all our children, but in three of four children it was sometimes longer than 30 min, which represents the maximal duration for a CPH attack. However, several reports showed CPH patients with attack duration longer than 30 min in both adults and children. Frequency and duration of the attacks, nevertheless, are commonly different between paediatric and adult population also in more common primary headaches, such as migraine and tension-type headache. If attack duration and frequency can make the diagnosis more difficult, especially in paediatric age, the absolute response to indomethacin represents the diagnostic key for CPH in both adults and children (indotest).
In conclusion, the characteristics of our children’s headache, particularly the positive response to indomethacin, led us to consider the diagnosis of CPH. However, the frequency and duration of our patient attacks did not fulfil the ICHD-III beta criteria. These elements suggest that a revision of the current CPH diagnostic criteria, possibly with the inclusion of special notes for developmental age, would be necessary.
Disclosure of Interest
None Declared
Other Primary Headache Disorders
PO-01-115
Vitamin D deficiency is associated with the severity of migraine: a case-control study
Laura Rapisarda1,*, Maria Rosaria Mazza1, Aldo Quattrone1 and Francesco Bono1
1Headache Group, Institute of Neurology, Magna Graecia university of Catanzaro, Catanzaro, Italy
Objectives
It is well recognized that vitamin D deficiency may occur in patients with headache. However, if the serum vitamin D levels correlate with severity of migraine remains uncertain. The aim of this study was to investigate if the severity of vitamin D deficiency correlates with the frequency of headaches in migraine patients.
Methods
In this prospective study we enrolled 140 consecutive headache suffers (18 men, 122 women; mean age: 42 ± 13,4 years) and 41 healthy controls (18 men, 23 women; mean age 43,1 ± 14,2 years). Each patient underwent a neurological evaluation, and migraine was diagnosed according to IHS diagnostic criteria. The frequency of headaches was measured by using a monthly headache diary recorded for three months from the headache sufferers. All participant underwent a venous blood sampling for 25-hydroxyvitamin D.
Results
According to serum vitamin D levels we grouped patients into 3 groups: Group 1 included 28 patients with 25-(OH) vitamin D level between 20 and 30 ng/ml; Group 2 included 71 patients with 25-(OH) vitamin D levels between 10 and 20 ng/ml; Group 3 included 41 patients with 25(OH) vitamin D levels lower than 10 ng/ml. Serum 25-(OH) vitamin D levels of migraine patients revealed that the most severe vitamin D deficiency was associated with higher frequency of headaches. Indeed, Group 3 had a mean serum 25-(OH) vitamin D levels of 7,3 ± 1,7 ng/ml and a mean number of monthly headache days of 26,7 ± 7,5; Group 2 had mean serum 25-(OH) vitamin D levels of 14,7 ± 2,6 ng/ml and mean frequency of monthly headache days of 20,1 ± 10; Group 1 had mean serum 25-(OH) vitamin D level of 23,4 ± 2,9 ng/ml and a mean frequency of monthly headache days of 17 ± 9,5. Whereas, all subject in control group had serum vitamin D levels above 20 ng/ml.
Conclusion
Our data indicate that severe vitamin D deficiency is associated with higher frequency of headaches in migraine patients, suggesting that serum vitamin D levels correlate with severity of migraine. Since low vitamin D levels are implicated in descending modulation of endogenous pain control, we speculated that severe vitamin D deficiency may ease the headache attacks in migraine patients.
Disclosure of Interest
None Declared
Other Primary Headache Disorders
PO-01-116
Linear headache: clinical and algometric characteristics of 3 new cases
Marina Ruiz Piñero1,*, María Palacios-Ceña2,3, María Pedraza Hueso1, Ana Juanatey García1, Pascal Madeleine3, Ángel Luis Guerrero Peral1 and César Fernández de las Peñas2
1Headache Unit, Hospital Clínico Universitario, Valladolid
2Fisioterapia, Terapia Ocupacional, Rehabilitación y Medicina Física, Universidad Rey Juan Carlos, Alcorcón, Madrid, Spain
3Health Science and Technology, Aalborg University, Aalborg, Denmark
Objectives
Linear headache has been recently described as a headache of variable duration and intensity, located in a well circumscribed antero-posterior lineal trajectory. Its characteristics and accompanying symptoms may resemble migrainous or epicranial features. We describe three cases of linear headache including an analysis of pressure pain sensitivity to suggest a potential pathogenesis of this new entity.
Methods
We considered all patients attending a headache office at a tertiary hospital from January 2016 to March 2017. We identified three cases with a clinical picture comprised under previous descriptions of Linear Headache. In all of them we gathered demographic and clinical characteristics. A complete neurological exam and magnetic resonance study ruled out underlying disease. We evaluated pressure pain thresholds (PPT) over 21 points distributed over the scalp, based on the standard positions of 10/20 system for electroencephalogram recordings: 8 points on the right side (Fp2, F4, F8, C4, T4, P4, T6 and O2), 8 points on the left (Fp1, F3, F7, C3, T3, P3, T5 and O1) and 5 points along the mid-sagittal line (Fpz, Fz, Cz, Pz, and Oz). Topographical pressure pain sensitivity maps were constructed.
Results
CASE 1: A 65-year-old woman with arterial hypertension. She came to our office due to a one year history of a continuous mild pain, rated 2 out of 10 on a Visual Analogue Scale (VAS) described as oppressive, and located in a 2 centimeters-width band, extending from right supraciliary to ipsilateral occipital scalp. Pain increased with pressure and was not accompanied by any other symptom. Relief was obtained with occasional analgesia and our patient did not require preventive therapy. CASE 2: A 33-year-old female complained of almost daily episodes, triggered by stressful events, of pain located in a linear trajectory of 2 centimeters in width over left parasagittal region. Pain was either oppressive or stabbing and was rated as 7/10 on VAS. Episodes lasted hours and related to allodynia. No response was achieved with topiramate, gabapentin and lamotrigine as preventive therapies. CASE 3: 16-year-old male consulted due to the presentation 20 days a month during the previous year of oppressive pain, rated 7 out of 10 on VAS, located over a 1 centimeter-width band from forehead to occipital right parasagittal scalp, accompanied with photophobia and intolerance to physical exercise; partial response to analgesia. Topographical pressure pain sensitivity maps showed a decrease in PPT over the painful area in patients 2 and 3. In none of the 3 cases, the common pattern of frontal and temporal hyperalgesia previously described in migraine was evident.
Conclusion
In these patients with linear headache, and although clinical features of the pain sometimes suggest migraine characteristics, topographical pressure sensitivity maps would correspond epicranial headaches.
Disclosure of Interest
None Declared
Other Primary Headache Disorders
PO-01-117
Cephalalgia as an enantiopathy to salty hypogeusia: Restoration of salty taste concomitant with headache
Dayana M. Dominguez1,*, Neil Sondhi2 and Alan R. Hirsch3
1Caribbean Medical University, Willemstand, Curaçao
2Aureus University School of Medicine, Oranjestad, Aruba
3Smell & Taste Treatment and Research Foundation, Chicago, United States
Objectives
Heightened sensation in auditory and visual spheres, during the aura or headache phases of migraine is well described in the literature (Hupp, 1989). While headaches have been associated with hyposmia (Hirsch, 1992) osmophobia (Hirsch, 2005) and undefined taste abnormalities (Kelman, 2005), restoration of taste during the headache has not heretofore been described. Such a case is presented.
Methods
A 36 year-old right handed male, two weeks prior to presentation, struck his head without loss of consciousness, resulting in a 40% reduction in smell and taste, with no ability to taste salt and sour, and a constant salty phantageusia. Four days after this event he began to experience headache which presents, altering sides, in both temples but always is unilateral, with a severity of 8/10, at times dull and at times sharp in nature. His headaches are associated with neck stiffness and improves with neck stretching. They occur every 3 days and last two minutes in duration. There is no warning or aura to the headache. He has a history of headaches, which began in the 1st grade, ice cream headaches, and car sickness as a child. He does snore. During the headache phase he states that his taste remains impaired except for salty taste that recovers to totally normal. After the headache resolves, the ability to taste salt diminishes to the impaired baseline level.
Results
Normal neurologic and psychiatric examinations. Chemosensory Testing: Olfaction: Alcohol Sniff Test: 17 (normosmia), Brief Smell Identification Test: 12 (normosmia). Pocket Smell Test: 3 (normosmia). Retronasal Smell Testing: Retronasal Smell Index: 9 (normal). Gustation: Propylthiouracil Disc Taste Test: 10 (normogeusia). Neuropsychiatric testing: Clock Drawing Test: 4 (normal). Animal Fluency Test: 21 (normal). Center for Neurologic Study-Lability Scale: 14 (abnormal). Other: MRI of head and neck: normal.
Conclusion
The mechanisms for the restitution of salty taste associated with the headache is unclear. Possibly the same physiologic dysfunction which is inducing the headache is concomitantly inducing the taste sensation abnormality. (Hutchins, 2016). Thalamocortical discharges could be inducing the cephalalgia as well as the salty taste (Marmura, 2014; Small, 2006). While taste inhibits pain (Gibbs, 2013), in this case pain may actually reduce taste threshold, allowing greater taste to salt. However, the short duration of the headache is inconsistent since disturbances of taste correlate with longer duration of cephalalgia (Kelman, 2005). It may not be the taste which is affected but rather the smell. With headache, parasympathetic activation induces nasal mucosal engorgement (Marmura, 2014). This may act to disinhibit odor induced inhibition of taste, thus intensifying the true salty taste. What is also unknown is why salty taste is specifically involved in contrast to other tastes. Possibly this represents activation of the trigeminal nerve inducing both cephalalgia and also savory discharge, since palatal trigeminal nerve fibers are responsive to sapid stimuli (Kelman, 2005).
In those who suffer from headache, taste sensation should be queried and medication used in the management of cephalalgia might also influence gustatory ability. Investigation of this is warranted.
Disclosure of Interest
None Declared
Other Primary Headache Disorders
PO-01-118
Seasonal headache associated with sexual activity. A case report
Alexandre Kaup1,* and Maurice Vincent2
1Neurology, Hospital Israelita Albert Einstein, São Paulo
2Neurology, Universidade Federal do Rio de Janeiro, Rio de Janeiro, Brazil
Objectives
To describe a patient who presents a primary headache associated with sexual activity for the last 23 years occurring only between November and January, every year since it started, determining a seasonal pattern. This seems to be the first description of such a case.
Methods
A 40 y-o white male patient describes an orgastic (through masturbation or sexual intercourses) headache for the last 23 years. The pain is explosive, always starts few seconds before the orgasm (grade 5 in a 0–10 intensity scale), and reaches grade 8 within one minute following orgasm. The pain is always frontal, bilateral, usually lasting 2 hours when treated with combined analgesics, or 8 hours if untreated. He insisted his sexual-related headache occurs only between the end of November and the end of January, with a maximum bout duration of 6 to 8 weeks. Sexual headaches are absent for the rest of the year, except when related to 5 mg Tadalafil occasional use. During the bout all orgasms are followed by headache. Normal brain MRI and MRA scans were obtained twice during the symptomatic period. No autonomic phenomena of any kind was ever noted. Surprisingly, he presented last year HSA in July, prompting him to see a neurologist. He suffers from co-morbid, low frequency episodic migraine without aura. His medical history includes hypertension since his early 30's, insulin resistance, and dyslipidemia, treated with Valsartan HCT 160/25, 850 mg Metformin bid, and 5 mg Rosuvastatin qd.
Results
The International Classification of Headache Disorders (ICHD 3rd edition, beta version) diagnostic criteria considers two possible forms of primary HSA: definitive, with at least two episodes of HSA; and probable, for patients with only one episode. Exclusion of a secondary cause is firmly advised at the first manifestation. Episodic, chronic or paroxysmal forms are not recognized in the ICHD.
Frese et al, noted that HSA may occur in bouts lasting 3.3 ± 5.2 months. Most of
their patients presented only one bout during a mean
Overlapping of headache characteristics as well as co-occurrence of two or more primary headaches is often observed in headache practice. Migraine with seasonal variation, side-locked migraine with autonomic symptoms, and association of trigeminal-autonomic symptoms with trigeminal neuralgia; and cluster-tic and CPH-tic syndromes are well recognized possible forms of “mixed” primary headaches.
Orgasm is a needed condition to consider the occurrence of HSA. Both orgasm and CH show hypothalamic activation in functional MRI studies, allowing us to considerer that a common pathophysiological mechanism.
The described patient could be classified as having a chronic primary HSA with seasonal variation.
Conclusion
The case presented here is the first case of seasonal headache associated with sexual activity. The previous descriptions observed the fact that headache associated with sexual activity may present in bouts, but no seasonal aspect has been described until now. Long term follow up of these patients may help us understand the pathopshysiological mechanism involved in such headache type.
Disclosure of Interest
None Declared
Other Primary Headache Disorders
PO-01-119
Kleine Levin Syndrome: An Episodic Syndrome that may be associated with Migraine?
Harry Donnelly1, Alexander D. Nesbitt2,*, Juana C. A. Marin3, Peter J. Goadsby4 and Guy D. Leschziner2
1King's College London
2Sleep Disorders Centre, Guy's and St Thomas' NHS Foundation Trust
3Headache Group, Department of Clinical Neuroscience, Institute of Psychiatry, Psychology and Neuroscience, King's College London
4Headache Group, Department of Clinical Neuroscience, Institute of Psychiatry, Psychology and Neuroscience, London, United Kingdom
Objectives
To phenotype headache and associated symptoms in patients with Kleine-Levin Syndrome (KLS), a rare sleep disorder characterised by fully reversible, recurrent episodes of hypersomnia, behavioural, perceptual and cognitive disturbances.
Methods
Consecutive patients with KLS presenting to a tertiary sleep neurology service over a 24-month period were asked about a range of symptoms associated with primary headache disorders using a semi-structured interview approach.
Results
Of 17 patients identified, 11 were interviewed. Of these, eight patients (73%) received a concurrent diagnosis of migraine, with the majority complaining of a symptom complex consistent with a migraine attack during their KLS episodes, as well as separate migraine attacks in between KLS episodes.
Conclusion
The high frequency of migraine in this small and rare illness cohort alludes to either a strong co-association, or shared pathophysiological mechanisms, between KLS and migraine; both being disorders of episodic neurological dysfunction. Indeed, KLS could potentially be considered an “episodic syndrome that may be associated with migraine”, a group of disorders representing a sub-category of migraine defined by the International Classification of Headache Disorders (3rd Edition). Even without definitive proof, using this hypothesis as a novel frame of reference could lead to a better mechanistic understanding of the disorder, as well as allow testing of simpler, and more effective treatment options, for it.
Disclosure of Interest
None Declared
Other Primary Headache Disorders
PO-01-120
Features of chronic primary headaches (CPH) in children and adolescents referred to two third level headache centers
Irene Salfa1, Laura Papetti1, Beatrice Bartoli2, Barbara Battan1, Cristiano Termine2 and Massimiliano Valeriani1,*
1Neuroscience, Bambino Gesù Children Hospital, Rome
2Infantile Neuropsychiatry, Insubria University, Varese, Italy
Objectives
Chronic migraine (CM), Chronic tension-type headache (CTTH) and new daily persistent headache (NDPH) are the main forms of CPH reported in the ICHD-III beta version. Medication-overuse headache (MOH) is classified among secondary headache but it generally affects patients with a pre-existing primary headache. CPH have been well described in adults and their diagnostic criteria were designed based on the clinical characteristics in the adult population. However, CPH are not a rare condition in children and adolescence with negative impact on their quality of life.
Our aim was to investigate the clinical features of CPH in a cohort of pediatric patients.
Methods
We retrospectively reviewed the charts of patients attending the Headache Centre of Bambino Gesú Children and Insubria University Hospital. The ICHD-III criteria were used for diagnosis. Statistical analysis was conducted by SPPS version 22.0 and χ2 test was used to study possible correlations between: - CPH and population features (age and sex); - CPH and headache qualitative features; - CPH and risk of MOH; -CPH and response to prophylactic therapies.
Results
We included 377 patients with CPH (66.4% female, 33.6% male, age between 0 and 18 years). The most frequent CPH type was CM (73.5%), followed by CCTH (13.5%) and NDPH (13%). MOH was detected in 10.9% of total patients. CPH are less frequent under 6 years of age (0.8%; p < 0.05); significant greater frequency in females than in males was found in the age group between 0–6 years (23/31 F, 8/31 M) and between 15–18 years (41/51 F, 10/51 M) (p < 0.05). No correlations between age/sex and different CPH types were detected. We found a more frequent incidence of vegetative symptoms (photo/phonophobia and vertigo) in female sex (p < 0.05). Nausea and vertigo are the two most frequent vegetative symptoms under 10 years of age (p < 0.05) while photo/phonophobia are more frequently in patients older than 15 years (p < 0.05). Possible development of MOH has been found correlated with CM types (p < 0.05) and age above 15 years (p < 0.05).
Conclusion
Our results showed that CPH presented a correlation with patients’ age and sex. No significant differences were found between CPH types and population/pain features. Development of MOH was related with CM onset and adolescent age. Amitriptyline and topiramate had the best effectiveness. However, it is to be underlined that follow up data could not be issued from a moderate percentage of patients. It will be useful in the future to reduce the number of missing patients by improving patients’compliance and promoting the concept of migraine as a disease that can cause relevant disability.
Disclosure of Interest
None Declared
Other Primary Headache Disorders
PO-01-121
Cell phone associated headache: Is it new variant of chronic daily headache?
Devashish Ruikar1,*, Sita Jayalakshmi2 and Surath Mohandas2
1Medicine, MIMSR MEDICAL COLLEGE, Latur
2Neurology, KIMS, Hyderabad, India
Objectives
There are more than three billion cellphone uses across the globe across all socio economics standards of population. Health related issues related to mobile or cellphone are topic of active debate and under active evaluation. There is hardly any data on headache associated with cellphone use in pubmed.
Here we present atypical cases who reported chronic daily headache related only with cellphone use
There are more than three billion cellphone uses across the globe across all socio economics standards of population. Health related issues related to mobile or cellphone are topic of active debate and under active evaluation. There is hardly any data on headache associated with cellphone use in pubmed. Here we present atypical cases who reported chronic daily headache related only with cellphone use
Methods
this is case report of 4 patients from tertiary centre from India. We followed patients from opd basis from 2013 to 2016 prospectively for six months or more. There MRI and other lab parameters were normal and no evidence of secondary headache ethology.
Results
In 2013 to 2016 patients out patients basis follow up we have noted avoidance of cellphone during migraine episode is new avoidance behaviour(60%)
Here we report four patients who had stereotypical pattern of headache related to use of cellphone only. They reported use of cellphone for at least six hours per day for more than 3 years on regular basis.
The reported headache pattern was more than fifteen days headache per month for more than six months, mostly dullaching in nature but disturbing the work and activities of daily living. There was no photo or phonophobia or nausea associated with headache. Dullaching headache satisfies IHS chronic daily criteria. Two reported starting associated with stress and two denied any form of stress. There was no significant relief with routine treatment and counselling. Two patients changed job which involves less or no use of mobile phone
In 2013 to 2016 patients out patients basis follow up we have noted avoidance of cellphone during migraine episode is new avoidance behaviour(60%)
Here we report four patients who had stereotypical pattern of headache related to use of cellphone only. They reported use of cellphone for at least six hours per day for more than 3 years on regular basis. The reported headache pattern was more than fifteen days headache per month for more than six months, mostly dullaching in nature but disturbing the work and activities of daily living. There was no photo or phonophobia or nausea associated with headache. Dullaching headache satisfies IHS chronic daily criteria. Two reported starting associated with stress and two denied any form of stress. There was no significant relief with routine treatment and counselling. Two patients changed job which involves less or no use of mobile phone
Conclusion
Use of cellphone is part of everyday life for most of adults worldwide. Excessive use of cellphone with possible underlying stress may trigger a form of chronic daily headache in few patients, this form are tough to treat as wel.
This entity needs further evaluation, follow up and more assessment. In patients of chronic headache use of cell phone and its association should be actively searched for.
Use of cellphone is part of everyday life for most of adults worldwide. Excessive use of cellphone with possible underlying stress may trigger a form of chronic daily headache in few patients, this form are tough to treat as wel. This entity needs further evaluation, follow up and more assessment. In patients of chronic headache use of cell phone and its association should be actively searched for.
Disclosure of Interest
None Declared
Other Primary Headache Disorders
PO-01-122
Episodic cluster headache responsive to orgasm. Case presentation and considerations
Maurice Vincent1 and Alexandre Kaup2,*
1Neurology, Universidade Federal do Rio de Janeiro, Rio de Janeiro
2Neurology, Hospital Israelita Albert Einstein, São Paulo, Brazil
Objectives
To describe a male cluster headache patient who achieves relief from his cluster attacks through orgasms.
Methods
LMP, male, 53 years old, with attacks initiated in 1994, when bouts of Cluster Headache lasting 1–2 months occurred every 6–18 months. The duration was around 10–15 minutes, always on the right fronto-temporal-retrocular area. There may be a combination of ipsilateral conjunctival injection, tearing, nasal obstruction, and mild reduction of the inter palpebral fissure during attacks. Symptoms have always occurred to the right side, but in february 2014 he experienced attacks on the left. He noticed that the left inter palpebral fissure became permanently shorter after these late attacks. Two weeks before his first visit, October 2014, the attacks returned at the right side, up to three times a day, stoping two days prior to the visit. The cluster attacks are almost immediately and effectively aborted by orgasm, either during sexual intercourse or masturbation. Frequently he asks her wife for a sexual intercourse if possible, or masturbates to get rid of the pain. He mentioned entering once in a public restroom in a shopping mall to masturbate in order to abort an imminent attack. Orgasm has been effective in 100% of the pain episodes. He sufferes from gout and takes allopurinol regularly. No other present or past diseases were reported. The neurological examination was hormal except for an assimetry in the left palpebral slit.
Patient perception is that orgasm acts fast than sumatriptan nasal spray or subcutaneous.
Results
Sexual related headache is known since mid seventies. Primary headache associated with sexual activity was first described by Kriz in 1970, followed by the classic publication of Lance in 1976. More recently few reports have been published showing that sexual activity can relief or even resolve a headache attack, either migraine or cluster headache.
Male CH patients seem to found more pain relief than women. Differences between men and women in reaching an orgasm, as well as the sexual habits may explain the observed diferences.
Possible explanations for the sexual activity headache relief include distraction from pain, endorphins release, and postorgasmic relaxation. Both CH and orgasm show hypothalamic activation in studies of Function MRI studies, increasing the possibility of the influence of one condition on the other in both directions. Probably, orgasm may be the first noninvase treatment for CH directed to act in hypothalamus.
Conclusion
Sexual activity can interact with headache in many ways, trigerring, changing the behavior of a previously diagnosed headache, and even be able to treat it, aborting a acute headache attack.
We present a case of a male cluster headache patient who responde unequivocally to orgasm, as a treatment for his attacks. Both CH and orgasm show hypothalamic activation, leading us to consider that orgasm may act like a hypothalamic target treatment for some patients, being even faster that sumatriptan in abort a cluster headache attack.
Disclosure of Interest
None Declared
Other Secondary Headache Disorders
PO-01-123
Stroke-Like Migraine Attacks after Radiation Therapy (SMART): A Case Report
Anand Diwan1,* and Sanjay Vekhande2
1Medicine-Neurology, Dr Vasantrao Pawar Medical college
2Neurosurgery, Nashik hospital, Nashik, India
Objectives
To report uncommon cause for secondary headache.
Image:

Pt rceovered fully with symptomatic management and antiepileptic therapy. He followed up after 3months with complete recoverey from his left hemiparesis and was headache-free and seizure free.
Conclusion
SMART is a syndrome considered to be a delayed and sometimes reversible complication of whole-brain irradiation. Recurrent attacks of migrainous headaches, seizures (with or without prior history of migraine and seizure), complex neurological deficit (hemiparesis, hemianopia, dysarthria) and characteristic imaging findings are noted. The underlying pathophysiology is unknown. It is differentiated from Post-Ictal pseudo regression by less headache, milder deficit and quicker recovery favouring latter. Recognition of SMART syndrome is important to safeguard against misdiagnosis and prevention of aggressive treatment like cerebral angiography or Brain biopsy.
Disclosure of Interest
None Declared
Other Secondary Headache Disorders
PO-01-124
Headache improvement after intracranial endovascular procedures in Chinese patients with unruptured intracranial aneurysm: A Prospective Observational Study
Linjing Zhang1, Ruozhuo Liu2,*; on behalf of China International Headache Center, Shengyuan Yu1; on behalf of China International Headache Center
1Neurology, Chinese PLA General Hospital
2Neurology, Chinese PLA General Hospital, Hainan Branch of Chinese PLA General Hospital, Beijing, China
Objectives
To investigated whether there is long-term improvement in headache of patients with unruptured intracranial aneurysms (UIAs) treated with intracranial endovascular procedures.
Methods
Using a prospective design, consecutive patients with unruptured intracranial aneurysms (UIAs) with neuroendovascular treatment from January 2014 to December 2014 were asked to participated in. Headache outcomes were established prior to aneurysm treatment and for 6 months following treatment. Factors associated with different headache outcomes were investigated.
Results
Ultimately, fifty-eight patients completed the 6-month follow-up. In total, 29 patients had preoperative headache. Six months after the intracranial endovascular procedure, thirteen patients (44.8%) stated that their headaches were relieved after endovascular treatment; headache in one patient improved slightly, and six reported disappearance of headache and marked improvement. Overall, the mean headache scores of 29 patients improved on the self-reported Numeric Rating Scale (NRS) after endovascular treatment (6.00 vs. 2.30; p < 0.001). Patients with pretreatment tension-type headache, more severe headaches, stent-assisted coiling and stent implantation of the aneurysm were the important disadvantage for patients in improvement of post-procedure headache.
Conclusion
Treatment of unruptured intracranial aneurysms resulted in relief of headaches in about half of patients who had headaches pre-operatively.
Disclosure of Interest
None Declared
Other Secondary Headache Disorders
PO-01-125
Orthostatic Headache- Etiologies different than CSF Hypovolemia
Ryan Smith1,*, Ivan Garza2 and Carrie E. Robertson2
1Headache Neurology, St. Luke's Health System, Boise
2Neurology, Mayo Clinic, Rochester, United States
Objectives
To report on possibly clinically relevant features other than CSF hypovolemia that may contribute to orthostatic headache.
Methods

Results
Sixty patients met inclusion criteria. Of those, 37 were suspected to have a spontaneous CSF leak despite neuroimaging (MRI brain, MRI entire spine, CT myelogram, and nuclear cisternography) failing to identify a causal leak. No other etiologies were found to cause the orthostatic nature of their headaches.
The orthostatic headaches in the remaining 21 patients were of unclear etiology, but many had potentially significant comorbidities to which the treating physician attributed their headaches. These are listed in Table 1. Thirteen of 21 had some form of autonomic dysfunction diagnosed clinically or with formal autonomic diagnostic procedures such as autonomic reflex screen and/or thermoregulatory sweat test.
Conclusion
In patients presenting with orthostatic headache where a thorough evaluation for CSF hypovolemia has been negative, there may be other potentially relevant comorbidities contributing to the headaches. It appears that autonomic dysfunction may account for a sizeable number of patients with orthostatic headache who do not have CSF hypovolemia. This is consistent with previous reports on orthostatic headache in postural orthostatic tachycardia syndrome and the so called “coat hanger headache” with orthostatic hypotension2. A few of our patients appeared to have a paradoxical orthostatic headache in the setting of presumed increased intracranial pressure. Despite thorough evaluation, there remain a considerable number of patients for whom no etiology for orthostatic headache can be identified, creating a diagnostic and therapeutic challenge.
References
1Smith, Ryan M., Carrie E. Robertson, and Ivan Garza. “Orthostatic headache from supratentorial meningioma.” Cephalalgia 35.13 (2015): 1214–1214
2Martin, V. T., & Neilson, D. (2014). Joint hypermobility and headache: The glue that binds the two together–Part 2. Headache: The Journal of Head and Face Pain, 54(8), 1403–1411.
Disclosure of Interest
R. Smith Conflict with: Avanir, I. Garza Conflict with: Contributes to UpToDate Inc, C. Robertson Conflict with: UpTo Date, Amgen
Other Secondary Headache Disorders
PO-01-126
Characterising the effect of lumbar puncture on headache in IIH
Andreas Yiangou1,2, James Mitchell1,3, Keira Annie Markey1,2, William Scotton1,2, Susan Mollan1,4 and Alexandra Sinclair1,3,*
1Institute of Metabolism and Systems Research, University of Birmingham, Edgbaston, B15 2TT
2Centre for Endocrinology, Diabetes and Metabolism, Birmingham Health Partners, B15 2TH
3Department of Neurology
4Birmingham Neuro-Ophthalmology Unit, Ophthalmology Department, University Hospitals Birmingham NHS Foundation Trust, B15 2TH, Birmingham, United Kingdom
Objectives
This study aimed to evaluate the temporal change in headache severity in the week following lumbar puncture (LP) in patients with active Idiopathic Intracranial Hypertension (IIH). Furthermore we characterised the likelihood of headache improving or deteriorating following LP, depending on baseline headache severity. Finally, we evaluated the factors which influenced headache severity post LP.
Methods
Patients with IIH (diagnosed according to the modified Dandy criteria) were prospectively recruited from University Hospitals Birmingham NHS foundation Trust, a UK tertiary referral hospital. All patients recruited had active IIH (papilloedema with a Frisén grade >1, LP pressure >25cmCSF). Exclusion criteria included significant comorbidity and previous CSF diversion procedure.
Headache severity was prospectively recorded using a verbal rating scale (VRS) 0 (no pain) to 10 (most severe pain) immediately prior to LP and following the LP (at 1,4 and 6 hours and then daily to 7 days). Headache severity was further categorised into mild (VRS 1–3), moderate (VRS 4–6), severe (VRS 7–10). Demographic data and variables hypothesised to impact on the post LP headache severity were recorded.
Results
37 IIH patients were recruited, 20 had LP’s performed on 2 occasions with mean age 31 ± 6.5, BMI 40.5 ± 10.4 Kgm−2, LP opening pressure 33.5 ± 6.3 cmCSF, CSF drainage 10.8 ± 1.6mls.
A deterioration in headache severity at some point in the week post LP was noted in 65% with 28% experiencing an exacerbation of pain by ≥4 points on the VRS.
Overall, headaches improved as early as 1 hour in 60% (33% reduction in VRS (p < 0.001)) and this was maintained at 7 days in 51% (38% reduction in VRS (p = 0.005)). There was no significant variability in the headache VRS between 1 hour through to 7 days post LP. In those with severe headaches pre LP, 82% improve at 1 hour (p = 0.043) and 73% improved at 7 days (p = 0.018) whilst the likelihood of deterioration over the week was 36%. In patients with moderate headaches pre LP, 90% improve at 1 hour (p < 0.001) and 62% improved at 7 days (p = 0.005), with a likelihood of deterioration of 67%. In those with mild headaches pre LP, 46% improved at 1 hour (p = 0.924) and 62% improved at 7 days (p = 0.811), with a likelihood of deterioration of 92%. Patients with no headache at the time of LP, 17% develop headache at 1 hour (p = 0.157) and at 7 days 25% will have developed headache (p = 0.18), whilst the overall likelihood of developing headache at some point during the week was 58%.
The only factor which influenced the post LP headache severity was pre LP headache severity (p < 0.001). There was no relationship between the response of the headache severity post LP and BMI, height, skin to dura depth, LP opening or closing pressure, CSF volume withdrawn, number of LP attempts, CSF red blood cell count, acute analgesics, acetazolamide use and Frisén grade.
Conclusion
The majority of IIH patients will experience deterioration in headache at some point during the week post LP. Headache severity pre-LP significantly influenced the likelihood of improving or deteriorating after LP. Additionally, we noted that the improvement at 1 hour post LP was maintained at 7 days. This characterisation of headache outcomes post LP in IIH patients has relevance when counselling patients about the procedure.
Disclosure of Interest
None Declared
Other Secondary Headache Disorders
PO-01-127
Invasive spinal interventions for the treatment of head pain outside of occipital nerve distribution
Vladimir Gorelov1,*
1Pain Management, Spire Elland Hospital, Halifax/Huddersfield, United Kingdom
Objectives
Head pain outside of the distribution of occipital nerves, i.e. in the face or eye, can stem from a source in the neck and, vice versa, primary headaches can be accompanied by neck symptoms. The anatomy of this phenomenon is described in terms of trigeminocervical convergence (1). Its clinical implications are not fully understood, nor sufficiently reflected in the literature. In a recent review the neck and cervical spine were absent among the recognised sources of facial pain (2), although Fredriksen et al.'s description of cervicogenic headache featured facial pain with a periorbital component in all reported cases (3). Our objective is to demonstrate that facial pain can respond to invasive interventions in the neck and such treatment may be employed with consistently successful outcomes.
Methods
We analysed retrospectively all consecutive headache cases referred to our Pain Clinic over a period of 6 years. There were no recent-onset cases (less than 3 months). Inclusion criteria: We selected cases where all or part of head pain affected the face and/or eye irrespective of their ICHD-3 beta class. Pain stemming from the neck (cervicogenic headache ICHD-3 beta 11.2.1 and occipital neuralgia ICHD-3 beta 13.4) was included and represents the majority of the cases. Other secondary headaches (ICHD-3 beta groups 6–12 except neck-related) and trigeminal neuralgia were excluded as well as minor headaches that were not among the main complaints. Definition of outcomes: The outcomes are presented categorically as either success or failure (4). Success is defined as sustained, complete/near-complete resolution of the headache with functional recovery and remission uninterrupted or, in case of recurrence, reinstated. Patients who had a clinically significant, but non-complete/non-sustained improvement were not counted as a success and are presented as failures. Clinical management consisted of a combination of cervical spinal exercises, repeat cervical medial branch and/or occipital nerve blocks performed with bupivacaine and no steroids. 13 patients underwent RF neurotomy of C2–4 medial branches (5).
Results
48 cases were selected, aged 25–81, median age 54 years. In all cases except one headache was strictly or predominantly unilateral. 40 patients (83%) had signs of ipsilateral neck involvement, the remaining 8 but one had a characteristic occipital trajectory of the pain. Distribution of pain: periorbital/ocular/retroocular - 69% of cases, temple - 36%, maxilla and mandible - 30% each. Occipital trajectory was present in 69% of all cases. Outcome: Of the 48 cases 8 are ongoing and 6 were lost to follow-up (some with good initial response). Of the remaining 34 cases, 26 (76%) had a successful outcome and 8 failed.
Conclusion
A cervical source of facial pain is common, although not always apparent, and in a clinically significant proportion of cases responds to invasive spinal interventions with a meaningful, sustained remission. It is our impression, both from practice and literature, that the significance of spinal origin is underestimated.
References:
1. Goadsby PJ and Bartsch T. On the functional neuroanatomy of neck pain. Cephalalgia 2008; 28 (suppl1):1–7
2. Zakrzewska JM. Differential diagnosis of facial pain and guidelines for management. BJA 2013; 111:95–104
3. Fredriksen TA, Hovdal H, Sjaastad O. “Cervicogenic headache”: clinical manifestations. Cephalalgia 1987; 7:147–60
4. MacVicar J, et al. Cervical medial branch radiofrequency neurotomy in New Zealand. Pain Med 2012; 13:647–54
5. Gorelov V. Bipolar radiofrequency denervation for treatment of cervicogenic headache: a case report. WIP 8th World Congress, New York 2016/ Abstract. Pain Pract 2016; 16, S1:80–1
Disclosure of Interest
None Declared
Other Secondary Headache Disorders
PO-01-128
Sildenafil-Related Cerabral Venous Sinus Thrombosis and Papilledema: A Case Report of a Rare Entity
Dilek Top Karti1,*, Omer karti2, Dilara Aktert3, Nese Celebisoy3 and Figen Gokcay3
1Neurology
2Ophthalmology, bozyaka Training and Research Hospital
3Neurology, Ege University, izmir, Turkey
Objectives
We present a rare case of cerebral venous sinus thrombosis associated with long-term and high dose use of sildenafil.
Methods
case report
Image:

Results
A 29-year-old man was referred to our neuroophthalmology clinic for bilateral visual deterioration and severe headache. He had stage 2 papilledema and other clinical and neurological examinations were normal. He had used the drug for nearly two years, two to three times a day. All laboratory parameters including blood count cell, coagulation panels and genetic tests including methylene-tetrahydrofolate reductase and factor V Leiden mutation were unremarkable. Brain magnetic resonance imaging result confirmed transevers cerebral venous sinus thrombosis (CVST) (figure 1). The opening pressure of cerebrospinal fluid (CSF) was 43 cm H2O with normal biochemistry and no cells.
Conclusion
Clinicians must be aware of the possibility of CVST when the patient use sildenafil.
Disclosure of Interest
None Declared
Other Secondary Headache Disorders
PO-01-129
Topiramate is as effective as Acetazolamide at lowering intracranial pressure in healthy rodents
William Scotton1,*, Hannah Botfield1, Maria Uldall2, Connar Westgate1, James Mitchell1, Rigmor Jensen3 and Alex Sinclair1
1Institute of Metabolism and Systems Research, University of Birmingham, Birmingham, B15 2TT, United Kingdom
2Danish Headache Center, Clinic of Neurology, Rigshospitalet-Glostrup, University of Copenhagen, Glostrup
3Danish Headache Center, Clinic of Neurology, Rigshospitalet-Glostrup, University of Copenhagen, Birmingham, B15 2TT, Denmark
Objectives
Management of Idiopathic Intracranial Hypertension (IIH) aims to reduce intracranial pressure (ICP). Acetazolamide is the most commonly used drug, with class 1 evidence demonstrating modest improvement in patients with mild visual loss. Other drugs used include Topiramate, Furosemide, Amiloride and Octreotide, despite little mechanistic or clinical evidence to support their use.
The aim of this study was to ascertain which of these drugs has the greatest effect on lowering ICP in-vivo.
Methods
Using a validated epidural ICP recording method we measured changes in ICP in conscious female rodents after subcutaneous administration of these drugs at clinically equivalent and supra-clinical doses over 2 hours (peak plasma concentrations).
Results
At clinical doses, Topiramate lowered ICP by 32% (p = 0.0009) compared to a 25% reduction for Acetazolamide (p = 0.0081). Post-hoc analysis showed no significant difference between the two (p = 0.85). Furosemide, Amiloride and Octreotide had no significant effect.
Conclusion
Our in-vivo studies have demonstrated that, at clinically equivalent doses, Topiramate significantly lowers ICP and is as effective as acetazolamide. Topiramate may have additional advantages in IIH, including its migraine prevention properties and weight loss effects. These findings support the need for future randomised controlled trials evaluating the therapeutic efficacy of topiramate in IIH.
Disclosure of Interest
None Declared
Other Secondary Headache Disorders
PO-01-130
The prevalence rate, risk factors, and surgical treatment of cervicogenic headache in patients with cervical spine disorders requiring surgery
Keiko Shimohata1,*, Kazuhiro Hasegawa2 and Takayoshi Shimohata3
1Departmet of Anesthesiology, Kameda- Daiichi hospital
2Department of Spine Surgery, Niigata Spine Surgery Center
3Department of Neurology, Brain Research Institute, Niigata Unuversity, Niigata, Japan
Objectives
Cervicogenic headache (CEH) is caused by cervical spine disorders that was first identified by Sjaastad (1983). Surprisingly, 86–88% of patients with cervical myelopathy or radiculopathy requiring anterior cervical surgery presented headache in 2 prospective studies, although these studies did not diagnose headache according to the International Classification of Headache Disorders criteria. The International Classification of Headache Disorders-Third Edition beta (ICHD-3beta) CEH criteria represents the first instance of verification of cervical spondylosis as causing disorder of CEH. However, it remains unknown about the prevalence rate, risk factors of CEH in patients with cervical spine disorders requiring surgery. The aim of the present study was to clarify the prevalence rate, clinical features and risk factors of CEH as diagnosed according to ICHD-3beta in patients with cervical spine disorders requiring surgery.
Methods
In this single hospital-based prospective cross-sectional study, we enrolled 70 consecutive patients with cervical spine disorders such as cervical spondylotic myelopathy (CSM), ossification of the posterior longitudinal ligament (OPLL), cervical spondylotic radiculopathy (CSR), and cervical spondylotic myeloradiculopathy (CSMR) who had been scheduled to undergo anterior cervical fusion or dorsal cervical laminoplasty between June 2014 and December 2015. All patients were asked structured interview and headache was diagnosed according to ICHD-3beta pre-operatively. Limited cervical range of motion, identification of the spinal lesion levels and intramedullary high signal intensity on T2-weighted MRI, the Japanese Orthopaedic Association Cervical Myelopathy Evaluation Questionnaire, Neck Disability Index (NDI), and a 0–100 mm visual analog scale (VAS) of headache and neck pain were used to evaluate clinical features, and scores were compared between preoperatively and 3, 6, and 12 months post-surgery. We also compared clinical difference between patients with CEH and those without CEH.
Results
We enrolled 70 patients (M:F = 46:24, 64.5 ± 11.5 years old) with CSM (53 patients), OPLL (7 patients), CSM (5 patients), and CSMR (5 patients). The prevalence rate of CEH in our population was 15/70 (21.4%; 95%CI: 11.8% to 31.0%). 12 patients were diagnosed with CH, 2 with CH and tension-type headache, and 1 with CH and psychogenic disorder. The main clinical features were dull and tightening/pressing headache sensations in the occipital region. All our patient with CEH had cervical lesion below C4. Headache severity was mild (VAS, 32 ± 11 mm). The CEH group had a higher frequencies of neck pain (87% vs.51%; P < 0.05), cervical range of motion limitation (67% vs. 38%; P < 0.05), and higher NDI score (14 vs.3; P < 0.001). Among the different cervical spine disorders, the prevalence of CEH was highest in CSMR patients (60%), being ≤20% for all other disorders. Surgical treatments including cervical laminoplasty produced initial improvements in CEH that slightly diminished by 12 months post-surgery. The headache VAS at 3, 6month and 12month after surgery was lower than that before surgery (P < 0.001, F = 9.728, 9 ± 15,11 ± 18,12 ± 15). The neck pain VAS at 3, 6month and 12month after surgery also significantly reduced than before surgery (P < 0.001, F = 6.69).
Conclusion
We demonstrated that the prevalence rate of CEH (21%) was much lower than the previous report. Potential risk factors for CEH included neck pain, limited cervical ROM, high NDI score and a diagnosis of cervical spondylotic myeloradiculopathy.
Disclosure of Interest
None Declared
Other Secondary Headache Disorders
PO-01-131
Acute ischemic stroke with prominent headache symptom: A case series study
Jinyoung Ahn1,* and Byungkun Kim2
1Neurology, Seoul Medical Center
2neurology, Eulji university hospital, Seoul, Korea, Republic Of
Objectives
Headache in stroke is usually caused by cerebral hemorrhages such as subarachnoid hemorrahge (SAH), subdural hemorrhage (SDH) and lobar hemorrhages. Acute ischemic stroke can also show headache with various neurological signs and symptoms and usually managed in emergency room. But some patient with acute ischemic stroke walks in outpatient clinic with isolated headache. We retrospectively analyzed clinical and radiological characteristics in such patients.
Methods
We conducted a retrospective review of 18 patients (male = 5, female = 13) who showed isolated headache diagnosed as acute ischemic stroke in outpatient clinic. We investigated their clinical features, neurological findings and radiologic findings.
Results
All patients showed abrupt onset headache that was disappeared within 7 days. The mean age of patients was 65 year-olds. Characteristics of headache was mostly dull-aching pain(n = 12) followed by throbbing pain(n = 5). Thunderclap headache was presenting mode in one patient. One patient showed very mild limb weakness and 3 patients showed hemianopia. But none of the patients noticed such symptoms. The location of infarction were temporal(n = 12), occipital(n = 10), cerebellar(n = 5) and pons(n = 1) infarction in posterior circulation of brain.
Conclusion
In case of newly developed sudden onset headache without any other prominent neurological symptoms in outpatient clinic, we have to consider acute ischemic stroke, especially in elderly patients.
Disclosure of Interest
None Declared
Other Secondary Headache Disorders
PO-01-132
Headache as the only symptom of atypical tuberculous meningitis
Asel Jusupova1,*
1Neurology and Med Genetics Dept, Kyrgyz State Medical Academy, Bishkek, Kyrgyztan
Objectives
TB meningitis - a secondary disease, specific inflammatory process primarily localized on meninges in the base of the brain, which leads to the typical picture basilar tuberculous meningitis. There are some atypical forms of tuberculosis of the brain, which are due to inadequate application of anti-TB drugs.
Methods
Patient M., 52 years, during 6 months of 2016 was delivered four times through the ambulance in different neurological department of Bishkek. And each time with monotonous complaints: chronic headaches in the parietal-occipital areas Expander nature radiating to the eyeballs, accompanied by nausea, repeated vomiting. According to his son, occasionally marked by episodes of “thought and pour”, during which he did not immediately respond to a verbal appeal.
Last deterioration observed 1 December 2016, when the headaches became severe, he could not talk, by the ambulance he was admitted to the angioneurology department with the DS: Supratentorial aneurysm of the left internal carotid artery. On MRA: the restriction and intermittent progress of both the middle cerebral artery in M2 segments, thinning A1segment both anterior cerebral arteries, aplasia of the right vertebral artery, the depletion of the vascular pattern of the terminal branches of both pools of blood supply to the brain. Blood sugar, common blood and urine tests, kidney tests, ECG were within normal limits.
Then he was transferred to the Department of Neurosurgery to exclude the aneurysm supratentorial department of the left internal carotid artery. In the neurological status: apathetic, slightly retarded, face pained, pale skin. Questions answered in monosyllables. Convergence weakness on the left side. Trigeminal point slightly painful. Palpable occipital pain points, the spinous processes of the cervical localization. Meningeal symptoms negative
Angiography of cerebral vessels: aneurisms were excluded. Markers for viral hepatitis, blood for HIV, Wasserman - Neg. Blood sugar, prothrombin index, total protein serum within the normal range. Ultrasound of the internal organs: cholecystitis, a cyst of the left kidney. Chest x-ray: lungs roots extended with the presence of small calcifications on the left. Optometrist: VOD = 0,8; VOS = 0,8. Optic disc more bloodshot, efface the border narrowed artery, veins slightly expanded. Antibodies to Mycobacterium tuberculosis - Neg.

Results
He was transferred to the National TB Center. The patient was scheduled for TB therapy first category DOTS (isoniazid, pyrazinamide, ethambutol, rifampicin, kanamycin) and symptomatic treatment. During the time spent in the department noted regression of headaches, nausea, vomiting.
Conclusion
Thus, this clinical example shows that the diagnosis and treatment of TB meningitis problem can not be considered solved, even with greatly increased the arsenal of diagnostic and therapeutic agents. TM Early diagnosis is very difficult. In this described case, symptoms were stable nature, which were assessed by experts as a vascular process. It is necessary to pay attention to soft course over 6 months, with an extension of each phase of the disease. This, apparently, can be explained by the appointment of broad-spectrum antibiotics while another hospitalization in the form of symptomatic treatment. In conclusion, we can say about the evolution of the modern course of infection, which is caused by the active use of drugs as a symptomatic therapy, which brings change for the seemingly classical infectious diseases.
Disclosure of Interest
None Declared
Other Secondary Headache Disorders
PO-01-133
Characteristics of headache in the patients with anti-neutrophil cytoplasmic antibody associated disorders
Takayuki Kosaka1,*, Mari Watari1, Makoto Nakajima1 and Yukio Ando1
1Neurology, Kumamoto University, Kumamoto, Japan
Objectives
Anti-neutrophil cytoplasmic antibody (ANCA) is one of autoantibodies detected in some autoimmune disorders. The characteristics of headache due to ANCA associated disorders remains to be elucidated. The aim of this study was to elucidate the characteristics of headache in patients with ANCA associated disorders.
Methods
We retrospectively reviewed the medical records of 10 Japanese patients with ANCA associated disorders (7 men, and 3 women), who were admitted to our hospital between January 2014 and December 2016. We investigated clinical, radiological, and serological profiles including myeloperoxidase (MPO)-ANCA and proteinase 3 (PR3)-ANCA in these patients.
Results
MPO-ANCA alone-positive patients was found in 8, PR3-ANCA alone-positive patient in 1, and both of them-positive patient in 1, respectively. Three patients complained headache as the chief complaint. Those patients were all positive for MPO-ANCA and had lesions limited to the intracranial space without systemic organ disorders. The location of headache in each patient was forehead, temporal, and occipital, respectively. The comorbidities were diverse (otitis media in 2, cranial polyneuropathy in 1, chronic sinusitis in 1, and mastoiditis in 1). MRI demonstrated that all patients with headache had no brain parenchymal involvement and two of three patients were radiologically diagnosed as hypertrophic pachymeningitis. Great efficacy was observed in immunosuppressive therapy including prednisolone in two patients.
Conclusion
Previous reports had been demonstrated MPO-ANCA positivity was predominant in Asian countries, whereas PR3-ANCA positivity was predominant in northern Europe. In this study, we elucidated that the prevalence of otitis media in patients suffering from headache due to MPO-ANCA associated disorders was high. Otitis media might be an important clue in diagnosis of headache with MPO-ANCA associated disorders and we should take into consideration for MPO-ANCA associated disorders in differential diagnosis of headache in Japanese patients with refractory otitis media.
Disclosure of Interest
None Declared
Other Secondary Headache Disorders
PO-01-134
10-year follow-up of CSF leakage by serial neuroimages in a patient with protracted spontaneous intracranial hypotension
Yu Cheng Chu1,*, Jong-Ling Fuh1, Yen-Feng Wang1, Shih-Pin Chen1, Jiing-Feng Lirng2 and Shuu-Jiun Wang1
1Neurology, Taipei Veterans General Hospital, Taipei
2Radiology, Taipei Veterans General Hospital, Taipei, Taiwan, Republic of China
Objectives
Protracted spontaneous intracranial hypotension (SIH) is uncommon. Long-term follow-up of these patients is rare in the literature. The pathophysiology of protracted SIH and the relationship between clinical symptoms and neuroimaging in these patients are not clearly understood.
Methods
A 52-year-old female had a protracted course of SIH and received 3 epidural blood patches within 2 years (at 1 month, 2.5 months, and 10 months). Her symptoms improved gradually over a period of 4.5 years. During the 10-year follow-up, we serially evaluated her neuroimaging of brain magnetic resonance imaging (MRI) and heavily T2-weighted magnetic resonance myelography (HT2W MRM). The correlation between clinical symptomatology and neuroimaging was analyzed.
Image:

Results
During the 10-year follow-up, nine brain MRIs and 15 HT2W MRMs were done. The patient's orthostatic headache resolved at 4.5 years, while her brain MRI was normalized at 10 months. In contrast, her HT2W MRM at 10 years still showed anterior epidural CSF collections at T9 to T11. The length of her anterior epidural CSF collections was 6–8 segments of vertebrae when she was symptomatic, while it shortened to but remained 3 segments when her symptoms improved.
Conclusion
With the advent of the non-invasive technique, long-term imaging follow-up for patients with protracted SIH becomes feasible. This protracted case provides us insight that HT2W MRM might be more sensitive than brain MRI in the circumstances of SIH. In addition, there could be discrepancy between clinical symptomatology and imaging findings, and both should be taken into considerations in determining the treatment strategies.
Disclosure of Interest
None Declared
Other Secondary Headache Disorders
PO-01-135
Clinical and psychological factors associated to medication-overuse headache
Michele Viana1,*, Sara Bottiroli1, Grazia Sances1, Daniele Martinelli1,2, Giorgio Sandrini1,2, Giuseppe Nappi1 and Cristina Tassorelli1,2
1Headache Science Center, National Neurological Institute C. Mondino
2Dept of Brain and Behavioural Sciences, University of Pavia, Pavia, Italy
Objectives
To identify clinical and psychological factors associated to MOH
Methods
The study was conducted at the Headache Science Center of “Mondino” Institute, Pavia, Italy. We enrolled consecutive patients with long-term episodic migraine (EM, with a history of illness >10 years who never had Medication Overuse MO) and patients with chronic migraine and MO (MOH). We compared socio-demographical, clinical and psychological variables between EM and MOH patients. Clinical variables included lifestyle habits, migraine characteristics/history, endocrino-gynecological history, familiar pathological history, and general medical history. Psychological assessment included psychopathological history, Toronto Alexithymia Scale (TAS-20), Hospital Anxiety and Depression Scale (HADS), Childhood Trauma questionnaire and stressful life-events questionnaire. Univariate and multivariate logistic regressions were applied in order to determine predictors of MOH. The criterion for variable inclusion in the multivariate model was based on statistical significance at the level of p < 0.10 as obtained by univariate analysis.
Results
Three hundred and eighteen patients were enrolled: 156 with EM and 162 with MOH. The mean age was 42.1 ± 10.3, 80.8% of subjects were female. The duration of migraine (before MOH onset in the case of MOH patients) was not significantly different between the two groups (24.0 yrs EM vs 24.6 yrs MOH; p = 0.57). After the multivariate analysis the factors associated to MOH were: age of onset of migraine [OR 0.94 (0.89–0.98) p = 0.016], use of at least one migraine preventive medication [OR 2.36 (1.18–4.71), p = 0.014], marital status [married vs unmarried OR 3.65 (1.63–8.19) p = 0.002; separated/divorced/widowed versus unmarried OR 4.19 (1.13–15.47) p = 0.031], physical activity [0.42 (0.19–0.91) p = 0.029], history of depression [2.91 (1.25–6.73) p = 0.012], insomnia [insomnia associated to use of hypnotics versus absence of insomnia OR 5.59 (1.65–18.93) p = 0.006], traumatic head injuries [OR 3.54 (1.57–7.99), p = 0.002] snoring [OR 2.24 (1.05–4.79), p = 0.036], and higher score at Childhood Trauma questionnaire [OR 1.48 (1.09–2.02), p = 0.012].
Conclusion
The factors associated to the development of MOH are elusive. Few studies have attempted to answer this question, although with some limitations (i.e. diagnosis made with questionnaires, a small number of variables considered, impossibility to compare duration of illness between groups). In this study run in a headache center, we evaluated and compared a high number of clinical and psychological variables between two large and well characterized groups of patients suffering from EM or MOH. In this frame, it is worth noting that the similar duration of illness in the two groups strongly speaks against a possible overlap between them. The present study is interesting as it considered together several aspects that can be involved in MOH development. Multivariate analysis identified 9 factors belonging to 4 different areas, indicating that MOH derives from a mixture of factors. This is useful to know as MOH can be optimally treated by considering perspectives and strategies (medical, social/lifestyle, psychological).
This work was supported by grants of the Italian Ministry of Health to RC 2013–2015.
Disclosure of Interest
None Declared
Other Secondary Headache Disorders
PO-01-136
Evaluating the use of spectral domain optical coherence tomography to measure retinal nerve fibre layer thickness in idiopathic intracranial hypertension
Anuriti Aojula1, Susan Mollan2, John Horsburgh2, Keira Markey3, James Mitchell3, William Scotton3, Pearse A. Keane4 and Alexandra Sinclair1,3,*
1Institute of Metabolism and Systems Research, University of Birmingham
2Department of Ophthalmology
3Department of Neurology, University Hospitals Birmingham NHS Foundation Trust, Birmingham
4NIHR Biomedical Research Centre for Ophthalmology, Moorfields Eye Hospital NHS Foundation Trust and UCL Institute of Ophthalmology, London, United Kingdom
Objectives
Identification and monitoring papilloedema is an essential aspect to managing patients with idiopathic intracranial hypertension (IIH). Direct inspection to quantify papilloedema is subjective and prone to inaccuracy and inter-rater variability. Spectral domain optical coherence tomography (SD OCT) can quantify peripapillary retinal nerve fibre layer (RNFL) thickness, a measure of papilloedema. This has been a major advance in the field as it enables quantification of optic disc oedema and can track changes over time. Consequently, OCT imaging of the RNFL is being increasingly used in both the clinical and research setting to monitor IIH patients. We have noted that the automated OCT RNFL measurements are not consistently accurate in IIH. Here we aim to conduct an in depth analysis of the extent and location of the automated RNFL segmentation error in a cohort of IIH patients and provide a practical paradigm for clinicians to review SD-OCT scans to improve the reliability.
Methods
Baseline SD OCT scans of patients with IIH (active papilloedema) and controls with no retinal or optic nerve pathology were examined. In each patient, the OCT RNFL of the most severely affected eye was assessed for errors with the automated segmentation values. The automated segmentation errors were then manually corrected as needed. The distribution, around the optic disc (superior, temporal, inferior, nasal) of RNFL errors were qualitatively assessed. The difference between the original automated area of the RNFL and the manually adjusted RNFL area were quantified using ImageJ and also reanalysed with the Heidelberg Eye Explorer software, version 1.9.1. (Heidelberg Engineering, Heidelberg, Germany). The percentage change was determined.
Results
46 IIH and 14 control subjects were recruited. Significantly greater segmentation error (p = 0.009) was present in RNFL total area, assessed using ImageJ, in IIH patients (error 5% ± 0–58%) compared to controls (error 1% ± 0–6%). This was particularly evident in patients with moderate to severe papilloedema (n = 23, 10% ± 0–58%, p < 0.001). Automated re-analysis of the adjusted average RNFL indicated that the superior retina was predominantly affected (error 20% in IIH v 3% in control) with least error noted in the temporal region (error 5% in IIH v 2% in controls). Qualitative analysis also highlighted that the error was predominantly located in the superior retina of 50% of IIH patients. Finally, in those with very severe papilloedema the RNFL thickness was so inaccurate that it could not be quantified.
Conclusion
Clinicians should be cautious when interpreting SD OCT RNFL in IIH patients with papilloedema as automated segmentation values can be significantly inaccurate, especially in the superior retinal quadrant. Importantly, errors in the automated RNFL values are greatest in those with moderate to severe papilloedema. We suggest that SD OCT RNFL scans are systematically reviewed in IIH patients with moderate to severe papilloedema. Scans should be evaluated particularly in the superior retinal quadrants and manually adjusted and then re-segmented to allow corrected values to be generated and utilised for monitoring papilloedema in IIH.
Disclosure of Interest
None Declared
Other Secondary Headache Disorders
PO-01-137
Effect of SSRI treatment on the prognosis of patients with medication overuse headache
Yang Zhang1,*, Ning Chen2 and Li He3
1Sichuan University West China Hospital, Chengdu, China
2Neurology Department, Sichuan University West China Hospital, Chengdu
3Neurology Department, Sichuan University, No.17 Renmin Road, China
Objectives
In this study, patients with MOH were treated and followed up to explore the role of SSRIs in the treatment of MOH patients and the risk factors for relapse in patients with MOH
Methods
In this cohort study, we were followed up for MOH patients diagnosed at the West China Hospital at an average follow-up duration of 1.5 years to analyze patient outcomes and relapse. We used logistic regression to assess the relationship between patient medication and withdrawal treatment success rate. We used COX regression analysis to assess the relationship between withdrawal treatments and relapse rate in patients with MOH.
Results
A total of 72 MOH patients were enrolled in this study, of which 14 (19.4%) were discontinued. In the successful treatment of patients, there are 13 (20.7%)relapse patients. SSRIs treatment can increase the effect of withdrawal therapy (odds ratio [OR] 0.016, 95% confidence interval [CI] 0.003,0.091, p < 0.001). No significant association was found between SSRIs treatment and the risk of relapse.
Conclusion
SSRIs can increase the therapeutic effect in MOH withdrawal therapy.
Disclosure of Interest
None Declared
Other Secondary Headache Disorders
PO-01-138
Headache and neck pain in vertebral artery dissection
Hisao Tachibana1,*, Yoshiaki Tatsumi1, Tadashi Nakajima1, Takashi Tokunaga1 and Hiroji Miyake2
1Neurology
2Neurosurgery, Nishinomiya Kyoritsu Neurosurgical Hospital, Nishinomiya, Japan
Objectives
Headache and neck pain are frequent symptoms in spontaneous vertebral artery dissection(VAD). VAD is being increasingly diagnosed because of magnetic resonance imaging(MRI) and magnetic resonance angiography(MRA). The purpose of this study was to analyse the clinical features of VAD.
Methods
We reviewed medical records of 34 consecutive patients who showed VAD and were diagnosed between 2014 and 2016. Headache topography, severity and quality, presence of migraine or vascular risk factors such as hypertension, diabetes mellitus, dyslipidemia and smoking and outcome were examined.
Results
The mean age was 52 years. Twenty-seven of 34 patients presented with headache. Of them, 6 had brainstem infarcts, 3 had subarachnoid hemorrhages and 18 had neither infarction nor bleeding(Headache group). Onset of headache was progressive in 9, acute in 11 and thunderclap-type in 7 patients. Headache was throbbing in 21 and constrictive in 6. Neck pain was present in 10 patients. Neck pain was constrictive in all patients. Pain was unilateral in 23 and bilateral in 4 who showed bilateral VAD. All patients were pain free at 2 months. Headaches were distributed posteriorly in all patients. Migraine was present in 3 patients. There were no significant differences in age, dynamics and quality of headache, and rates of vascular risk factors between Headache group and brain ischemia patients. Antithrombotic therapy was administered to the patients with brain ischemia. In the Headache group, no antithrombotic therapy was administered, but no reattacks were noted in the follow-up period.
Conclusion
Pain may be the only symptom in VAD, but pain dynamics, quality and duration were heterogenous. Present study shows that imaging study should be necessary in patients with newly-developed unexplained headache or neck pain.
Disclosure of Interest
None Declared
Other Secondary Headache Disorders
PO-01-139
Moyamoya syndrome in a patient with hemiplegic migraine type 1: A case report
Nicolas Vandenbussche1,* and Robin Lemmens1
1Department of Neurology, UZ Leuven, Leuven, Belgium
Objectives
We present an association between moyamoya syndrome and sporadic hemiplegic migraine type 1. Moyamoya syndrome is a rare cerebrovascular condition characterized by the progressive stenosis of proximal intracranial vessels. Stroke is the most feared complication of this disease. Many patients complain of headaches although an association between moyamoya and migraine syndromes has not been described. The patient had multiple episodes of headache associated with transient neurological deficits. She was diagnosed with probable moyamoya syndrome based on intracranial vessel imaging. However not all symptoms could be attributed to the stenosis observed and therefore hemiplegic migraine was considered. A pathogenic heterozygous mutation in the CACNA1A gene was indeed identified confirming this diagnosis.
Methods
Case report.
Image:

Results
A 43 year old Caucasian woman without relevant prior medical history experienced sudden transient loss of consciousness followed by headache without any other neurological deficit during several hours. More than one year later similar symptoms occurred although this episode was complicated with a transient left sided hemiparesis which lasted for one day. She presented to an outside hospital in which magnetic resonance (MR) imaging revealed a recent ischemic lesion in the right frontal lobe. Six months later she developed transient neurological symptoms with dizziness, a right sided hemiparesis and visual disturbances of the right eye during mulitple hours. In the outside hospital a cardiac etiology for the loss of consciousness was excluded by implanting a continuous cardiac monitoring device (REVEAL) which did not show any cardiac arrhythmias.
Thereafter she visited our outpatient clinic for medical advice on the episode of transient neurological deficits and chronic symptoms of headache. She described chronic daily headache for many years, with episodic exacerbations characterized by severe, pulsating and uni/holocranial headache associated with photophobia, sonophobia, nausea and vomiting. These severe headaches were not preceded by auras. Severe headache we present simultaneously with the transient neurological symptoms or started even before these symptoms occurred. Familial history was negative for migraine or other neurological syndromes.
On clinical examination, there was a mild right sided sensorimotor hemiparesis. Comparing the neuro-imaging performed following the second event versus a MR angiography few months prior a progressive narrowing of the right M1 segment of the middle cerebral artery was identified. The recurrent episodes of headache with associated transient, but prolonged neurological deficits suggested a diagnosis of hemiplegic migraine. This was confirmed by genetic analysis of the CACNA1A gene which identified a heterozygous pathogenic mutation: rs16024 c.3043G>A (p.Glu1015Lys).
Conclusion
To our knowledge and after reviewing available literature, this is the first case report of moyamoya syndrome in a patient with (sporadic) hemiplegic migraine type 1. We also did not find a current link between CACNA1A and moyamoya disease as a causative or involved gene. Headache is a very common symptom in patients with moyamoya disease with frequent migraine-like phenotype. Therefore, we suggest that CACNA1A might play a role in the pathophysiology or symptomatology of moyamoya disease. Because we cannot confirm its relevance in moyamoya disease with this sole case study, further research is needed to elaborate this hypothesis.
Disclosure of Interest
None Declared
Other Secondary Headache Disorders
PO-01-140
Can secondary thunderclap headache be transformed into primary headache? 9-year follow up study – a Georgian case
George Gegelashvili1,*, Khatuna Gugulashvili1,2 and Ketevan Kobakhidze1,2
1Headache Center
2Health Institute of Georgia, Tbilisi, Georgia
Objectives
To report a case of long period observation of recurrent thunderclap headache and analyze possibilities of transformation of secondary headache into primary one.
Methods
A 62-year-old healthy female, caucasian, doctor first time in her life in 2008 suffered from excruciating occipital headache after taking the shower. The patient recalls: “pain became unbearable in seconds as if somebody was hitting hammer into my head, I thought it was about to split and I began screaming”. Initial blood pressure was 260/120 mmHg. Pain lasted 10–15 minutes and the same day in 1,5–2 hours it “came back” again. Neurological examination was normal. During next two days she felt general discomfort, arterial pressure periodically increased (>180/100 mmHg) and she experienced analogical pain 4 times. CT (day 4) and MRI (day 6) showed SAH and 9 ml hematoma in parasagittal area of the left parietal lobe. Brain MRA/MRV, carotid and vertebral arteries ultrasound, MRA and 4-vessel angiography (day 6–7) didn’t reveal any abnormalities. CBC, ESR, CRP, full biochemistry, serum cardiac enzymes, thyroid panel were normal (day 4 and 7). Ultrasound of heart, thyroid and abdomen were normal. Treatment was provided by nimodipine, antihypertensives, analgesics. During one month the patient has been complaining of mild-moderate, dull holocranial pain. According to MRI hematoma has disappeared after 1.5 months and the patient was back to her active lifestyle apparently healthy. Arterial pressure has been periodically slightly increasing during the period of 9 years (<180/100 mmHg) and had rare episodes of mild “simply” headache. After 7 and 9 years stereotypical attacks of thunderclap headache have renewed. In 2015 (6 attacks during 3 days) trigger was witnessing the car crash (child was hit by car and she ran for help) and in 2017 (5 attacks during 3 days) - her close friend’s death. In both cases in acute period brain CT, gadolinium-enhanced MRI, MRA and MRV, carotid and vertebral arteries ultrasound/MRA and lab excluded any acute pathology. In the last episodes patient has been feeling herself well. No other types of headache were presented neither between thunderclap headaches nor after. Treatment was provided according to the same chart.
Results
Patient has been suffering from 17 purely stereotypical high-intensity abrupt onset and short (10–15 min) headache attack during the period of 9 years. In 2008 thunderclap headache (6 attacks) was developed after non-traumatic intracranial haemorrhage of unknown etiology. In 2015 and 2017 thunderclap headache was triggered by emotional stress, but during this period general discomfort and mild-moderate headache was not presented any more. Blood pressure was elevated (>180/100 mmHg) only during 10 attacks out of 17. If admitted that all the researches were provided on timely and adequate basis - last 11 headache attacks by ICHD-3 beta may be classified as “Primary thundeclap headache” (code 4.4).
Conclusion
Thunderclap headache resulted from intracranial lesion (e.g. haemorrhage of unknown etiology) may later become recurrent primary one According to the analysis of our case complete stereotypeness of severe headache in the late period with the absence of other type (between or after attacks) headaches, patient’s good general condition, normal instrumental and lab researches make us to think that maybe at early stage in case of intracranial hemorrhage “clap of thunder pattern” was saved somewhere in “pain memory” which may play the role of “generator” of “nonorganic” headache triggered by psychological stress. It is necessary to continue recurrent stereotypical thunderclap headache analysis in the future.
Disclosure of Interest
None Declared
Other Secondary Headache Disorders
PO-01-141
Headache attributed to craniocervical dystonia
Marcos Eugenio Ramalho Bezerra1 and Pedro Augusto Sampaio Rocha Filho2,3,*
1Universidade Federal de Pernambuco, RECIFE, Brazil
2Neuropsychiatry, Universidade Federal de Pernambuco
3Hospital Universitário Oswaldo Cruz, Universidade de Pernambuco, Recife, Brazil
Objectives
We studied the prevalence, characteristics and impact of headache attributed to craniocervical dystonia in cervical dystonia patients.
Methods
24 consecutive patients had been evaluated regarding the dystonia and headaches clinical characteristics and followed for about 4 months after botulinum neurotoxin type A injections. Patients had been evaluated in three distinct moments by a neurologist with experience in treating movement disorders and headaches: 1- first baseline visit, when they had taken their scheduled botulinum toxin A injections; 2- second revaluation visit, approximately four-weeks later; 3- third visit, expected sixteen-weeks later than the first visit. Semistructured interviews, headache diaries, Hospital Anxiety and Depression Scale (HADS), Headache Impact Test-6 (HIT-6) and Toronto Western Spasmodic Torticollis Rating Scale (TWSTRS) were used. Reported headaches were classified at baseline visit in accordance with the diagnostic criteria established by the third edition beta of the International Classification of Headache Disorders. According to the identified headaches characteristics, the patients were assigned to one of the cohort groups: headache attributed to craniocervical dystonia group, “other headaches” group and “without headaches” group. All patients had given their informed consent. The Universidade Federal de Pernambuco’s Research Ethics Committee had provided ethics approval (ethics report number 777.590/2014).
Results
19 patients (79%) had cervical dystonia associated pain, 18 (75%) had headaches. Seven patients (29%) had headache attributed to craniocervical dystonia, all of them with migraine-like headaches, mean HIT-6 score: 60.1 ± 9.9. These patients had more disability related to dystonia compared to those without headaches (TWSTRS; Kruskal-Wallis test; p = 0.02). Headache impact did not vary significantly through the time in the “other headaches” group. Those with headache attributed to craniocervical dystonia had a significant improvement in HIT-6 scores between first and second visits, followed by a significant worsening of HIT-6 scores between second and third visits (MANOVA; p < 0.05). Considering the analysis of HADS scores through the visits, no statistical significant differences were found among the groups (MANOVA; p > 0.05).
Conclusion
Headache attributed to craniocervical dystonia is commonly prevalent among cervical dystonia patients, have a high impact and have different behavior from other headaches presented by these patients.
Disclosure of Interest
None Declared
Other Secondary Headache Disorders
PO-01-142
A Pain From The Neck: Hemicrania Continua-Like Headache After Carotid Dissection
Jennifer Wax1,*, Anusha Mannava1, Melissa Schorn1 and Natalia Murinova1
1Neurology, University of Washington, Seattle, United States
Objectives
Hemicrania continua is a rare primary headache subtype characterized by unilateral, constant pain, autonomic features, and responsiveness to indomethacin. The condition is frequently subject to diagnostic error, leading to significant delay in appropriate diagnosis and treatment. The objective of this report is to present a case of hemicrania continua-like headache occurring secondary to carotid dissection with immediate response to sphenopalatine ganglion (SPG) blockade.
Methods
A 44-year-old right-handed man was referred to the University of Washington Headache Clinic for a second opinion on “uncontrolled headaches,” previously diagnosed as migraine prior to his referral. A thorough headache history and neurologic exam were performed. The patient had developed a spontaneous left carotid dissection two years ago, and the headache had been constantly present since. He did not have any headache history prior to the dissection. His pain was determined to be unilateral, moderate-to-strong in intensity with spikes of more severe discomfort, and associated with left-sided tearing and ptosis. His extensive previous medication trials were reviewed and included many acute and prophylactic agents, though never indomethacin. General and neurologic exam were unremarkable with exception of left-sided miosis and ptosis. His previous vessel imaging and MRI in 2014 were reviewed, and revealed left carotid dissection. Follow-up MRI in 2016 showed resolution of the dissection.
Results
The patient was diagnosed with hemicrania continua-like headache secondary to carotid dissection. He underwent same-day bilateral sphenopalatine ganglion blockade, with immediate, full response. He was unable to tolerate indomethacin uptitration, but continued weekly SPG blocks for three weeks, followed by biweekly SPG blocks over the following months. He continued to have excellent results, with full pain relief following each block.
Conclusion
Hemicrania continua-like headache may occur after carotid dissection, and should be a diagnostic consideration. In this case, secondary hemicrania continua responded to sphenopalatine ganglion blockade, potentially via suppression of unopposed parasympathetic activity. SPG blockade may be a useful modality for secondary hemicrania continua treatment in the future, particularly for patients who cannot tolerate or who do not have complete response to indomethacin.
Disclosure of Interest
None Declared
Other Secondary Headache Disorders
PO-01-143
Intracranial hypertension after massive blood transfusion
Kyung-Hee Cho1,* and Kyungmi Oh2
1Neurology, Korea University Anam Hospital
2Neurology, Korea University Guro Hospital, Seoul, Korea, Republic Of
Objectives
Idiopathic intracranial hypertension is an uncommon syndrome presenting with chronic headache, papilledema, diplopia, tinnitus and other neurological symptoms. However, the pathophysiology of the syndrome is unknown, although many hypotheses have been proposed, including hormonal change, cerebrospinal fluid (CSF) dynamics, and cerebral venous blood pressure change. We experienced a patient with idiopathic intracranial hypertension after rapid massive blood transfusion, who had chronic anemia due to multiple uterine myomas.
Methods
CASE: A 38-year-old woman presented to the emergency department with uncontrolled vaginal bleeding for 2days. She had history of uterine myoma operation in 2007, otherwise there was no relevant medical or family history. The body mass index was 20.78. Initial vital signs were stable. She had mild dizziness and anemic conjunctiva, however her mental status was alert and the neurologic exam showed no focal deficits. Anemia with uterine myoma was considered as a possible cause. The hemoglobin level was 2.4 g/dl, mean cell volume (MCV) 51.5 fL, mean cell hemoglobin (MCH) 14.3 pg, mean cell hemoglobin concentration (MCHC) 27.7 g/dL, Fe < 10 ug/dL, total iron binding capacity (TIBC) 468 ug/dL, ferritin 2.4 ng/mL and laboratory findings were compatible with iron deficiency anemia. She had 7 pints of red blood cell transfusion for 2days and follow up hemoglobin level was 10.8 g/dl. Three days after last transfusion, she started to suffer severe pulsatile headache from occipital area radiating to frontal area with visual analog scale score of 10. She also had nausea and excessive daytime somnolence. The CSF study through lumbar puncture was done, the pressure was 25.0 cmH2O and the other profiles were within normal range. The magnetic resonance imaging with angiography and venography showed suspicious leptomeningeal enhancement without any vessel abnormalities. She had multiple retinal hemorrhages on both eyes but no papilledema on the ophthalmic exam.
Results
In this case, the papilledema was absent and the CSF pressure was not high enough to diagnose idiopathic intracranial hypertension, however, suddenly developed severe headache and multiple retinal hemorrhages on both eyes suggested idiopathic intracranial hypertension. She was treated with 20% intravenous dextrose mannitol and oral acetazolamide. The headache was improved gradually for next 7 days and no other complications occurred. The multiple uterine myomas were confirmed on sonography and myomectomy was done 1month later. Her hemoglobin level was stable and the headache has resolved completely.
Conclusion
The chronic iron deficiency anemia is well known as risk factor of idiopathic intracranial hypertension with young, obese women. In this case, the severe chronic anemia was present before headache and the onset of headache was the time after massive rapid blood transfusion was done. We made a hypothesis that the sudden blood transfusion in chronic anemia patient might damage cerebral vascular endothelium, releasing free radicals, resulting in vasogenic cerebral edema. Finally, the massive rapid blood transfusion might be the cause of idiopathic intracranial hypertension. Therefore, it is important to investigate carefully when the chronic anemia patient have sudden headache after blood transfusion.
Disclosure of Interest
None Declared
Other Secondary Headache Disorders
PO-01-144
Minimum important difference of the Headache Impact test Questionnaire (HIT-6) in subjects with temporomandibular disorders and concomitant headache
Letícia B. Calixtre1,*, Ana Beatriz Oliveira1, Corine M. Visscher2 and Susan Armijo-Olivo3
1Physical Therapy, Federal University of São Carlos, São Carlos, Brazil
2Oral Kinesiology Department, Academic Center for Dentistry Amsterdam, Amsterdam, Netherlands
3Faculty of Rehabilitation Medicine, University of Alberta, Edmonton, Canada
Objectives
The prevalence of pain-related Temporomandibular Disorders (TMD-pain) in adults is estimated to range from 5–10%, while there is a high prevalence of primary headaches. The two disorders often co-occur; up to 70% of TMD patients also present with headache. The Headache Impact Test questionnaire (HIT-6) covers domains of pain, social functioning, role functioning, vitality, cognitive functioning, and psychological distress. It has been used in clinical trials to verify the effect of treatments regarding headache impact. However, the Minimum Important Difference (MID) of the HIT-6 has not been reported for subjects with TMD and concomitant headache (TMDH). Therefore, this study aims to estimate the MID of the HIT-6 to measure changes of headache impact after an intervention in subjects with TMDH.
Methods
Mean change in HIT-6 scores between baseline and 5-week follow up for subjects classified according to the GRS.

Results
At baseline, the mean scores of the HIT-6 were 62.5 ± 6.1 for the CG and 61.4 ± 6 for the IG. Data from the classification of subjects according to the GRS are described in Table 1. All strong responders were on the IG as were 3 (out of the 17) moderate responders and 3 (out of the 29) non-responders. The area under the ROC curve (AUC) was 0.749 and the MID of the HIT-6 to discriminate between responders and non-responders was 3.5 (with sensitivity of .72 and specificity of .76).
Conclusion
According to the AUC, sensitivity and specificity values, HIT-6 has a reasonable responsiveness to variations on headache impact in the population with TMDH and the MID should be considered to verify the effect of future interventions.
Disclosure of Interest
None Declared
Other Secondary Headache Disorders
PO-01-145
Handl syndrome in pediatric age
Irene Salfa1, Laura Papetti2, Barbara Battan2, Federico Vigevano2 and Massimiliano Valeriani2,*
1Pediatric
2Neurology, Children's Research Hospital Bambino Gesù, Rome, Italy
Objectives
The syndrome of transient headache and neurologic deficits with cerebrospinal fluid lymphocytosis (HaNDL) is a rare syndrome of unclear pathogenesis characterized by one or more episodes of severe headache, transient neurologic deficits and lymphocytic pleocytosis in the cerebrospinal fluid, seldom reported in paediatric age. In most cases it is a benign and self limited disorder, although it may mimic various serious, including life-threatening, diseases, such as stroke and meningoencephalitis, which is why vigorous tests should be sought before this diagnosis of exclusion can be reached.
Methods
We report three cases of HaNDL occurred in 2 boys (14 years and 10 years old) and in a 17 years old girl.
Results
Each patient presented with headache, altered conscious state and papilledema associated with different neurological symptoms such as dysarthria, hemiplegia, pernicious vomiting, ideomotor slowing and psychomotorr agitation. None of them had fever and there was no evidence of meningeal irritation.
They received Ceftriaxone, Aciclovir, and Dexamethasone for possible encephalitis and/ or autoimmune disorders. Clinical manifestations were compatible with a variety of disorders including structural brain lesions, meningitis, seizures, autoimmune, vasculitic and paraneoplastic disorders. We performed neuroimaging examinations (CT scan and MRI of the brain), EEG and serum/CSF studies for infectious, autoimmune and vasculitic diseases. All of these aetiologies were ruled out. In one case, a complete tox screen was added and it resulted negative. The laboratory finding common to all three cases was a clear CSF lymphocytic pleocytosis and an elevated opening pressure during lumbar puncture. The intracranial hypertension treated in all three cases with acetazolamide per os with complete remission. In one case, it was necessary the admission in the intensive care unit because of the worsening of psychomotorr agitation of the patient, requiring sedation and endotracheal intubation. All three patients recovered without any neurological sequelae during the follow up.
Conclusion
The possibility of HaNDL should be considered in patients presenting with unusual patterns of headache and transient neurological symptoms. It is most commonly diagnosed in the third or fourth decades of life and is rare in the paediatric population. However, awareness of HaNDL existence also in children and adolescents can avoid unnecessary and potentially harmful investigations and therapies.
Disclosure of Interest
None Declared
Other Secondary Headache Disorders
PO-01-146
Hypertensive Posterior Reversible Leukoencephalopathy with Spinal Cord Involvement Presenting as Migraine like Headaches in a Young Child
Ankur Gupta1,*, Debashish Chowdhury1 and Geeta A. Khwaja2
1Neurology, Headache Clinic, GB Pant Institute of Post Graduate Medical Education and Research, Delhi, India
2Neurology, GB Pant Institute of Post Graduate Medical Education and Research, Delhi, India, Delhi, India
Objectives
Posterior reversible encephalopathy syndrome with spinal cord involvement (PRES-SCI) is a rare entity with only about 15 cases being reported in the literatures so far. The Aim is to present a case of 7-year-old girl who presented with complaints of migraine like headache and was later found to be hypertensive with features of PRES-SCI.
Methods
A 7-year-old girl presented with recurrent episodic, bilateral fronto-temporal throbbing headache since 3 months. Headaches occurred every 3–4 days, lasting for 2–3 hours with nausea, vomiting, vertiginous sensations and phonophobia and used to subside after a bout of vomiting or sleep. There was no history of aura. There was no significant past history. Her initial evaluation by a GP revealed no abnormality including fundus examination. However, no record of her BP measurement was available. She was referred to our centre as her headaches became continuous for the past 7 days. On examination, patient was conscious but jittery. She was well oriented but her sustained attention was impaired. Her pulse was 106/min and BP 240/130 mm of Hg. Peripheral pulses were normal, without any radio-femoral delay. Eye examination showed bilateral grade-4 hypertensive retinopathy with bilateral exudative retinal detachment. Neurological examination revealed bilateral hyper-reflexia, dysdiadochokinesia and impaired tandem gait. Planters were flexors. There was no neck rigidity. A diagnosis of malignant hypertension with hypertensive encephalopathy was entertained which was treated immediately with tablet Amlodipine followed by addition of tablet Telmisartan and Clonidine hydrochloride.
Her routine biochemistry including KFT was normal. She had albuminuria without any pyuria or casts. Both her spot urinary protein and 24-hour urinary protein were raised. ANA, rheumatoid factor were negative. MRI brain showed patchy areas of signal alteration (hyper-intense in T-2/FLAIR and iso-intense to hypo-intense signals in T-1 images) involving cortical, sub-cortical white matter of bilateral frontal, temporal, parietal and occipital lobes, bilateral basal ganglia, cerebellum, pons, medulla and upper cervical spinal cord. There were focal intramedullary patchy areas of similar signal alteration with swelling of cervical, dorsal, lumbar cord and conus without any significant post-contrast enhancement. Her ECG and ECHO revealed concentric LVH thereby suggesting chronic hypertension. USG showed bilateral loss of renal cortical medullary differentiation suggestive of medical renal disease. CT angiography of thoracic and abdominal aorta and renal vessels was normal. Her urinary VMA was normal. Subsequent DPTA renal scan was also normal without any evidence of reflux uropathy. CSF examination showed clear fluid, normal pressure with 3 cells (all mononuclear)/field, glucose was 91 mg/dl, protein was 137 mg/dl. CSF stains and culture for bacteria, AFB, and fungus were negative. Pan-neurotropic virus panel for different viral nucleic acids (by PCR) was negative. Thus based on above investigations a diagnosis of medical renal disease with malignant hypertension, hypertensive encephalopathy with exudative retinal detachment was made.
Results
Over next 6 weeks, her BP normalized on treatment and repeat MRI brain and spine became absolutely normal thereby confirming the diagnosis of PRES-SCI. Her headaches improved dramatically. Her retinal detachment also improved on conservative management by 8 weeks.
Conclusion
BP measurement should be an integral part of headache evaluation even in young children. PRES-SCI although rare can present with migraine like headaches.
Disclosure of Interest
None Declared
Other Secondary Headache Disorders
PO-01-147
Clinical evaluation of dissection of the cerebral arteries with headache
Yoshiko I. Unno1,2,*, Tatsuo Iwashita3 and Teruyuki Hirano1
1Stroke and Cerebrovacular Medicine, Kyorin University
2Neurology, Roppongi Hills Clinic
3Neurology, Inagi Municipal Hospital, Tokyo, Japan
Objectives
Arterial dissections are recognized as an important cause of stroke in young person. Some patients with cerebral artery dissecition shows no signs and symptoms except for headache. It remains unclear how we treat these patients with cerebral artery disseciton without ischemic signs.
The purpose of our study is to evaluate clinical characteristics of disseciton of the cerebral arteries with headache.
In serial 27 patients (21men, 6women, 50.0 years) who admitted Kyorin University Stroke Center between October 2013 and July 2016 because of cerebral artery disseciton were evaluated.
Methods
Information about clinical characteristics, history about headache, imaging study and clinical course were obtained from medical records retrospectively. Twenty-seven patients with dissection of the cerebral artery, comprising 21 man and 6 women with a mean age of 50.0 years were studied. We assessed the difference between Group H (patients without ischemic sign) and Group I (patients with ischemic sign).
Results
Lesions of dissection were anterior circulation in 5 (ICA:2, ACA:2, MCA:1) cases and posterior circulation in 22 (BA:2, BA + VA:1, VA:19) cases. Ten of 27 patients show no signs and symptoms except for headache. Fourteen of 27 patients had subjective symptoms, vertigo was most frequent. Nine of 27 patients had objective neurological findings, dysarthria was most frequent.
Group H (without ischemic lesion) were 15 patients (12 men, 3 women, mean age of 49.5years) and group I (with ischemic lesion) were 12 patients (9 men, 3 women, mean age of 50.5years). The ratio of negative neurological findings of group H was significantly higher than group I (p < 0.001).
About risk factors of cerebrovascular disease (history of hypertension, diabetes mellitus, hyperlipidemia, hyperuricemia, chronic kidney disease, and smoking), clinical character of headache, region and shape of dissection, and blood pressure at first visit, there were no differences between group H and group I.
Two patients (one in group H and one in group I) developed asymptomatic ischemic stroke during hospitalization.
Conclusion
Fifty-six percent of cerebral artery disseciton patients with headache had no ischemic lesion at onset. Except for objective neurological findings, there were no difference between group H and group I. In this study, we were not able to clarify the factors to be related to development of ischemic lesion. Careful neurological examination and appropriate neurological imaging study were recommended for patients with disseciton of cerebral arteries with headache.
Disclosure of Interest
None Declared
Other Secondary Headache Disorders
PO-01-148
Cerebral blood flow changes after withdrawal from medication overuse in patients with chronic migraine
Soo-Kyoung Kim1, Min Won Park1,*, Sangkyeong Yoo1, Heeyoung Kang1, Nack-Cheon Choi1, Oh-Young Kwon1 and Byeonghoon Lim1
1Neurology, Gyeonsang National University School of Medicine, Jinju, Korea, Republic Of
Objectives
Cerebral blood flow (CBF) changes in chronic migraine patients with medication overuse (CM-MO) before and after withdrawal and theirs relationship to the clinical outcomes are yet unknown. In this study, we aimed to evaluate CBF changes before and after stopping overused drugs in CM-MO by transcranial Doppler (TCD).
Methods
Patients with CM-MO (code 1.3 and 8.2 of the international classification of headache disorders-3beta) included and were followed-up for 1 month. After withdrawal of the overused medication, patients were treated with prophylactic treatments. Headache diaries, the headache impact test (HIT-6), the migraine disability assessment (MIDAS), and the Beck Depression Inventory (BDI) were administered before withdrawal and at 1 month after. The mean CBF velocities of the bilateral middle and anterior cerebral arteries (MCA and ACA) and basilar artery (BA) were measured by TCD.
Results
A total of 21 patients participated in the study, with the average age being 58.5, average headache frequency/month was 22.1, and average monthly medication intake was 20.7 pills. Headache Frequency (approximately 8–10 days reduction), use of Medication (approximately 3 intakes reduction), MIDAS, HIT-6 and BDI showed significant improvement after withdrawal with prophylactic treatments. The mean CBF velocities of the BA and MCA were found to be significantly increased before withdrawal when compared with those at 1 month after (p < 0.05). No significant differences in CBF velocities of the ACA were observed (p > 0.05).
Conclusion
Our results show that medication overuse increased CBF velocities via vasoconstriction, especially of the BA and MCA in patients with CM-MO. Withdrawal of the overuse medication could lead to vasodilation.
Disclosure of Interest
None Declared
Other Secondary Headache Disorders
PO-01-149
Diagnosis of a primary brain tumor after a woman developed a holocranial headache post-partum
Tara Von Kleist1 and Fawad Khan1,*
1Neuroscience, Ochsner Clinic Foundation, New Orleans, United States
Objectives
Women experience significant physiologic and anatomic changes associated with pregnancy. These adaptations involve most organs, and are largely driven by hormonal fluctuations. After delivery there is a sudden adjustment in physiology that can take up to eight weeks to normalize, while the woman returns to her pre-pregnancy state. While robust research about brain tumors during pregnancy is limited, it has been suggested that these changes during pregnancy can both promote and delay tumor growth depending on the type of tumor1. The pathophysiology has yet to be fully understood, though theories exist regarding the role of growth hormones and angiogenesis1. We present the case of a young woman who developed post-partum headaches that were found to be secondary to a large primary brain tumor.
Methods
Case report
Image:

Results
A healthy 23 year-old woman presented two weeks post-partum with worsening headache. She became pregnant via in-vitro fertilization and had an uneventful pregnancy, though did complain of occasional mild headaches that were self-limiting. She had a normal vaginal delivery at 40 weeks with intact placenta. Post-partum course was complicated by severe preeclampsia that resolved with medical management. She was also given three units of packed red blood cells for excessive bleeding.
The patient developed a holocranial pressure-like headache the night of delivery. She reported associated bilateral tinnitus, lightheadedness and blurry vision with minimal relief from over-the-counter medications. She had no history of migraines but had mild headaches in the past. Neurologic exam exhibited bilateral papilledema, but was otherwise unremarkable. CT head showed a right temporal cystic mass with associated vasogenic edema and midline shift. She was treated with steroids, and underwent neurosurgical intervention with a temporal craniotomy and tumor resection. Post-operatively she had no neurologic deficits. She remained stable and was discharged home four days after craniotomy.
Conclusion
Pregnancy causes various physiologic changes, which then reverse following delivery. While sex hormones have been suggested to influence the progression of some brain tumors, the role of pregnancy is unclear2. One study of fourteen pregnant women used MRI before and after delivery to evaluate for change in brain and ventricle volume. They found that both healthy and preeclamptic women had a statistically significant decrease in brain size and increase in ventricle size during pregnancy3. They then displayed that these changes had reversed within six weeks of delivery. While preeclampsia has not been implicated in affecting tumor growth, the pathophysiology involves generalized endothelial dysfunction. This may result in a sudden increase in blood pressure and vascular permeability, contributing to accelerated vasogenic edema. This case suggests that pregnancy provides some form of neuro-protection, and that delivery or preeclampsia resulted in a sudden physiologic change in our patient causing rapidly increasing edema.
Disclosure of Interest
None Declared
Other Secondary Headache Disorders
PO-01-151
A case-study of cavernous sinus thrombosis manifested with headache in young woman in Kyrgyzstan
Inna L. Lutsenko1,*
1Neurology, Kyrgyz State Medical Academy, Bishkek, Kyrgyztan
Objectives
To display an unique course of headache in Tolosa-Hunt syndrome (THS), which include episode(s) of unilateral orbital pain for an average of 8 weeks if untreated, with associated paresis of one or more of the third, fourth, and sixth cranial nerves.
Methods
We present a case of Tolosa-Hunt syndrome with bacterial thrombosis of cavernous sinus manifested with intense headache in 39 y.o. female. Patient was interviewed about headache intensity according to visual analog scale (VAS), general neurological observation was made and diagnose was confirmed with MRI with MR venography.
Results
The patient experienced intensive stabbing headache in the left orbita, 9 scores according to VAS. Headache was paralysing and disabling with acute onset, followed in 2 days with left ptosis and midriasis. MRI and MR-venography demonstrated a stasis of venous blood in the left cavernous sinus with perifocal edema and infarction in left temporal lobe. The combination of several chronic inflammatory diseases (hepatitis, pancreatitis, duodenitis, uteritis, adnexitis, gastritis, cholecystitis, mastoiditis, periodontitis) lead to septicemia, latent disseminated intravascular coagulation syndrome, and later to severe complication - bacterial cavernous sinus thrombosis. Prescription of wide spectrum antibacterial drugs and corticosteroid antiplatelets lead to full relief of headache and focal oculomotor symptoms.
Conclusion
Tolosa-Hunt syndrome must not be overlooked taking into account high rate of complications such as strokes. Anticonvulsants showed inefficacy compared to steroids leading to immediate relief of pain till 2 scores according to VAS
Disclosure of Interest
None Declared
Post-Traumatic Headache
PO-01-152
Lifestyle and Behavioral Occupational Therapy Treatment for Post-Concussive Syndrome Headache: Case Reports
Lindsey Reeves1,* and Ashley Uyeshiro Simon1
1Chan Division of Occupational Science & Occupational Therapy, University of Southern California, Los Angeles, United States
Objectives
According to the Centers for Disease Control, an estimated 2.5 million people in the United States sustain a traumatic brain injury (TBI) annually, and about 75% are classified as concussions or other forms of mild TBI. An estimated 15–30% of people who have a concussion may develop post-concussion syndrome (PCS), which is characterized by the persistence of symptoms including headaches, dizziness, fatigue, irritability, insomnia, concentration or memory difficulty, and increased risk for depression. Treatment of PCS focuses on gradual activity reintegration, functional rehabilitation, and learning how to cope, manage and prevent symptom onset. Evidence demonstrates that patient education, compensatory cognitive strategies, graded physical activity, and mental health interventions can improve symptoms of PCS and related headaches. Occupational therapists (OTs) are typically involved in acute concussion treatment for physical and cognitive rehabilitation, but OTs can also provide lifestyle and behavioral treatment for management and rehabilitation of PCS with headache (PCSH). To demonstrate the methodology and efficacy of lifestyle behavioral OT for managing PCSH, clinical outcomes for a group of patients with PCSH who attended individual outpatient OT treatment is presented.
Methods
Lifestyle Redesign® (LR) is a module-based behavioral OT technique that facilitates the development of health-promoting habits and routines, and has been shown to improve health management and slow disease progression. LR OT treatment for PCSH focuses on helping patients understand the disease process, gradually reintegrate into functional daily activities, and manage persistent symptoms through active participation in self-management habits. Treatment topics can include eating routines, activity pacing, energy management, body mechanics, sleep hygiene and positioning, physical activity, stress and depression management, and community/work reintegration.
Clinical outcome data for a small sample of patients with PCSH receiving LR OT outpatient clinic-based treatment as part of their typical plan of neurological care were collected to determine efficacy of treatment. Inclusion criteria was diagnosis of PCSH, and attendance of 3 or more sessions of OT. Outcome measures were completed at initial evaluation and discharge, and included the SF-36 Quality of Life Scale, Canadian Occupational Performance Measure (COPM), Headache Impact Test-6 (HIT-6), Headache Management Self-Efficacy Scale (HMSE), Migraine Specific Quality of Life Questionnaire (MSQL), and Migraine Disability Assessment Questionnaire (MIDAS).
Results
Seven patients’ clinical outcomes were collected (two male, five female). The average age of the patients was 36 years, and the average number of OT sessions had between evaluation and discharge was 7.14. On average, patients demonstrated improvements in almost all outcome measures, with the most substantial gains noted in certain SF-36 subscales (role limitations due to physical or emotional problems, energy and fatigue, social function), COPM Performance and Satisfaction scores, HMSE score, and MIDAS number of headache days.
Conclusion
These clinical case studies contribute to the evidence that lifestyle and behavioral OT treatment can be used to successfully help patients with PCSH improve their self-management abilities, symptoms, quality of life, and function. More research with a larger sample size of patients is needed to further investigate the significance to which lifestyle and behavioral OT can improve PCSH.
Disclosure of Interest
None Declared
Post-Traumatic Headache
PO-01-153
Hidden Disability: Mild Traumatic Brain Injury
Maureen A. Moriarty1,*
1Peripheral Nerve Institute, Georgetown University Hospital, District of Columbia, United States
Objectives
Purpose: Through systematic review of the literature, describe interprofessional interventions for post-traumatic syndrome following mild traumatic brain injury.
Methods
The World Health Organization reports that 70–80% of traumatic brain injury (TBI) is mild with a yearly incidence of 600 per 100,000. Minor sport, combat or accidental head trauma may go unnoticed. Often, emotional pressure is applied to return to activity by coaches, peers, or one’s self. In addition to pain, patients may experience somatic, psychological and cognitive symptoms. Dizziness, tinnitus, light or sound sensitivity, blurred vision, decreased smell, decreased libido and fatigue may trouble patients. Common psychological complaints of depression, anxiety, irritability, apathy and insomnia are seen. Cognitive changes include impaired attention, concentration and memory. This constellation of symptoms coupled with headache pain after a seemingly inconsequential injury affects areas of thinking, mood and emotional control. Appearing physically “normal”, anxiety, depression and irritability lead to occupational difficulties and interpersonal stress. This hidden disability reduces meaningful participation in work, family or social events and predisposes those injured to second impact syndrome increasing the possibility for lasting cognitive, somatic or emotional changes associated with mild TBI.
Results
This literature review explores genetic and environmental risk factors in development of mild traumatic brain injury. Using pathophysiologic changes following mild TBI as a framework, cognitive, somatic and emotional alterations are discussed. Successful symptom identification and interprofessional collaboration are fundamental best practices in improving quality of life in the mild traumatic brain injured patient Effective treatment requires a comprehensive approach with pharmacotherapy, physical therapy, biofeedback and counseling for patients and significant others.
Conclusion
It’s essential that clinicians recognize and understand physical, cognitive and emotional manifestations that may occur with mild traumatic brain injury. These manifestations are a result of trauma induced pathophysiology. Interprofessional team approach with collaborative documentation and clinical decision making promotes a multifaceted recovery in patients with this hidden disability.
Disclosure of Interest
None Declared
Post-Traumatic Headache
PO-01-154
Post-Traumatic Stress Disorder and Depression in relation to the Different Phenotypes of Post-Traumatic Headache and comparison with matched controls
James R. Couch1,* and Kenneth Stewart2,2
1Neurology, OklahomaUniversity Health Sciences Center
2Biostatistics, Universityof Oklahoma Health Sciences Center, Oklahoma City, United States
Objectives
Post-Traumatic Headache (PTH) is classified as a headache of any type following a TBI. This study evaluates the occurrence of Post-Traumatic Stress Disorder (PTSD) and Depression in relation to the various phenotypes of PTH following a deployment-related TBI (DTBI) for Veterans of the Iraq (OIF) and Afghanistan (OEF) wars with comparison to matched controls.
Methods
All subjects were Veterans who had been deployed to OEF/OIF and subsequently joined Operation New Dawn (OND), a VA program to assist in re-entering civilian life after discharge. OND Veterans were screened for possible DTBI and screen positive subjects were referred to our TBI clinic to confirm presence of a DTBI. A recruitment pool was established by taking the first 500 confirmed DTBI subjects (TBIS) and matching them to OND participants without DTBI (CS) by age, sex, race and time of deployment, Subjects were recruited from this pool and were interviewed by telephone. All subjects received the same questionnaires (QS) including: (a)TBI QS, (b) Headache QS, (c) Beck Depression Inventory 2 (BDI), and (d) Brief PTSD QS consisting of 7 “yes/no” questions. For depression, BDI score categories were: (a) Minimal/none – 0–11, (b) Mild – 12–19, (c) Moderate – 20–28, (d) Severe – ≥29. For PTSD, categories included: (a) none (0–3 yes answers), (b) possible (4–5 yes),and definite (6–7 yes). Headache phenotypes included: Migraine with (MA) and without (MO) aura, Tension/Probable Migraine (T/PM) and No Headache (NoHA). Statistics included Fisher’s Exact and Odds Ratio tests.
Image:

Results
There were 84 TBIS (81 male) and 85 CS (82 male). These subjects suffered their TBI 2-11 years before interview. Results are presented in the Table showing the distribution of PTSD and Depression categories for each headache phenotype. For the TBIS, 77 (92%) had migraine of which 70% had MA and 30% had MO. For MA and MO there was no significant difference in the distribution of PTSD or Depression categories with 59% having definite PTSD and 46% severe Depression. For their controls, only 16% had definite PTSD and 8% had severe Depression. For T/PM, There were 6 TBIS and 30 CS. For TBIS, 4 (67%) had definite PTSD, but only 1 (17%) had severe Depression. There were 30 CS with T/PM phenotype of which 3(10%) had definite PTSD and 2 (7%) had severe Depression. Differences between overall distribution of PTSD categories and Depression- categories between TBIS and CS were highly significant (p < .001).
Conclusion
There is a strong propensity for PTSD to occur in conjunction with PTH whether this is MA, MOM or T/PM in phenotype. For Depression, the propensity is limited to MA and MO. There are too few subjects in the T/PM group to allow a judgement. The results suggest a co-morbidity or even a causal link between these entities. Further research is needed in this regard.
Disclosure of Interest
None Declared
Psychological and Behavioural Factors and Management
PO-01-155
Inpatient Headache Therapy at the Berolina Clinic, Germany
Zoltan Medgyessy1,*, Gerhard Schmid-Ott1, Rolf Süllwold1 and Kai Lorenz2
1Psychosomatic
2Cognitive behavioral Therapy for orthopedics, Berolina Clinic, Loehne, Germany
Objectives
Headache disorders are third cause of disability worldwide (Stovner et al. 2015). The annual cost of treating migraine in Germany has been estimated at €478 million, the indirect costs at €6.237 million (Neubauer 2002). Evidence-based guidelines recommend a multi-modal approach that combines drug therapy, educational programs in disease and stress management, biofeedback, relaxation techniques, and aerobic exercise.
The German healthcare system has an extensive network of rehabilitation facilities where persons with present or impending work disabilities can receive inpatient or outpatient treatment for up to six weeks. The Berolina Clinic is one of these facilities. It specializes in psychosomatic disorders and chronic pain including migraine and headache and cognitive-behavioral therapy for orthopedics and utilizes a treatment program that follows evidence-based guidelines.
Methods
The clinic’s three-week inpatient treatment program for headache includes: medical supervision by a physician specialized in the treatment of headache, CBT in groups and in individual sessions, headache lectures, relaxation techniques, biofeedback, medical setting, detoxification of headache medicine, various forms of exercise with variable levels of intensity, art therapy, TENS therapy, and employment counseling.
Headache patients are treated either in the department of psychosomatics or of cognitive behavioral therapy for orthopedics depending on comorbidity. Over the past eight years, 4800 headache patients have been treated in the Berolina Clinic.
Results
The Berolina Clinic participates in an extensive quality assurance program mandated by the German statutory pension insurance scheme that includes reviews of patient satisfaction, therapy concepts, and treatment results. The results are communicated to the participating clinics after ca. 12 months. In the national scoring system, the quality score for subjective treatment success for 2015 was 70,9 -out of 100- for the department of psychosomatic medicine, compared to 67,3 for 146 other German psychosomatic clinics. The department of cognitive behavioral Therapy for orthopedics attained a score of 78,2, as compared to 72,2 for 254 other German orthopedics clinics.
Conclusion
Possible causes of this relatively high patient-reported satisfaction are the strict adherence to treatment guidelines, our multidisciplinary approach, a highly qualified team, and supervised care by experienced rehabilitation physicians specialized in psychosomatic medicine, neurology, orthopedics as well as physical and rehabilitative medicine and psychiatry.
Disclosure of Interest
None Declared
Psychological and Behavioural Factors and Management
PO-01-156
Self-reported triggers vs prospectively statistically determined factors associated with attacks in individuals with episodic and chronic migraine
Stephen Donoghue1,*, Gabriel Boucher1, Francesc Peris1, Alec Mian1 and Paul R. Martin2
1Curelator Inc., Cambridge, United States
2School of Applied Psychology, Griffith University, Queensland, Australia
Objectives
Migraine attacks may be triggered by combinations of internal and external factors which differ markedly between individuals (1). Most migraineurs suspect a range of triggers (2), usually based on (unreliable) retrospective recall which is subject to misinterpretation and recall bias. Previously we reported that less than 20% of suspected self-reported triggers could be shown to be statistically associated with attacks when using individuals’ prospective data collected using a digital platform (Curelator HeadacheTM) (2). Here we compare in groups of individuals with episodic or chronic migraine their self-reported triggers and attack risk factors identified statistically.
Methods
Individuals with migraine registered to use Curelator Headache via website or the App Store (iOS only) and completed a questionnaire about personal suspected triggers and their importance (1 = low; 10 = maximal). They then used Curelator Headache daily for 90 days, entering details about headaches and tracking factors that may affect migraine attack occurrence. After 90 days all factors were analyzed for each individual (3) and those significantly associated with attacks were compared with self-reported triggers
Results
Of 528 individuals, 429 (81%) were classed as episodic and 99 (19%) chronic migraine. Mean age (SD) was 43.5 (13.8) years and the majority (90%) were female: there were no major demographic differences between groups. Overall, individuals each suspected between 3 and 47 different triggers; mean (SD) = 23.6 (12.7). The most frequently suspected at all by both groups were: neck pain, stress, eyestrain, bright light, menstruation, fatigue, odors, dehydration, missed meals, travel, sleep duration, and sleep quality. The triggers most frequently strongly suspected (7 − 10 on the rating scale) were similar but alcohol and tiredness were proportionately more often strongly suspected.
Of self-reported triggers, on average (SD) only 3.4 (2.8) (14%) were shown to be statistically associated with attack occurrence. A further 12.5 (7.7) (53%) were shown to have no statistical association to attacks and for 5.5 (4.6) (23%) there was not enough data to determine an association. The proportion of self-reported triggers also identified statistically was similar in the two groups (14.1% vs 15.4%). In both groups ≥ self-reported triggers also identified statistically by 20% individuals were neck pain, anxiety, sadness, stress, bright light, menstruation, irritability and skin sensitivity: in addition were eyestrain, tiredness and loud noise in the episodic group and odors and angriness in the chronic group. In both groups, for the majority of factors, a relationship was seen between strength of suspicion as a trigger and statistical confirmation of an association with attack occurrence.
Conclusion
Individuals vary greatly in the factors statistically associated with their attacks but, as groups, there are no clear differences between those with episodic or chronic migraine in terms of self-reported triggers or the proportion of those confirmed statistically. This may be because 1) all individuals are guessing their risk factors with very low accuracy (essentially random guessing or based on the same lists of triggers circulated by media and internet) or 2) risk factors for episodic or chronic migraine are indeed similar, suggesting shared aspects of pathophysiology.
References
1 Spierings ELH et al. Curr Pain Headache Rep (2014) 18:455.
2 Donoghue S et al. Headache (2016) 56 (Supp 1): 35
3 Peris F et al. Cephalagia 2016; DOI: 10.1177/0333102416649761
Disclosure of Interest
S. Donoghue Conflict with: Curelator Inc., G. Boucher Conflict with: Curelator Inc., F. Peris Conflict with: Curelator Inc., A. Mian Conflict with: Curelator Inc., P. Martin Conflict with: Curelator Inc.
Psychological and Behavioural Factors and Management
PO-01-157
Mindfulness for Chronic Migraine with Medication Overuse: Clinical Results and Biological markers at 12 Month Follow-up after withdrawal
Licia Grazzi1,*, Frank Andrasik2, Domenico D'Amico1, Elena Corsini1, Emilio Ciusani1, Giovanni D'Andrea3, Andrea Bolner3, Matilde Leonardi1, Alberto Raggi1 and Emanuela Sansone1
1Neurological Institute C. Besta IRCCS, Milano, Italy
2University of Memphis, Memphis, United States
3Research & Innovation, Pafova, Italy
Objectives
Chronic migraine (CM) arises from a complex mixture of interconnected biological, psychological and social factors. CM is a disabling condition, worsened when associated with medication overuse. Mindfulness is emerging as a helpful treatment for pain, but it has yet to be explored fully for CM accompanied by Medication Overuse (MO). We report initial clinical findings from an on-going trial exploring the feasibility and utility of mindfulness as a primary treatment for this condition. We also investigated whether mindfulness (and medication treatment as well) produced meaningful changes in key hematological parameters, IL-6 and specific biological markers of tyrosine metabolism which have been revealed altered in chronic migraine patients.
Methods
Forty-four patients, diagnosed as CM with MO (IHS-III-beta 2013 criteria), were
enrolled. All patients completed a standardized medication withdrawal in a
day-hospital setting and were then assigned to 1 of 2 conditions: Prophylactic
Medication Alone (MED) or Mindfulness Training Alone (MT)
Results
Twenty patients in MT-group and nineteen in Med-group reached the 12-month follow-up assessment. Significant decreases were reported in clinical parameters and disability from BL to 12 months: 1) Headache Days/Month-MED: 19.6 ± 7.4 vs 9.8 ± 7.3(50% reduction); MT: 18.5 ± 7.5 vs 12.4 ± 8.5 (33% reduction). 2) Medications Intake/ Month-MED: 17.5 ± 6.4 vs 8.1 ± 5.08 (54% reduction); MT: 17.9 ± 6.3 vs 10.3 ± 5.3 (43% reduction). 3) MIDAS Score-MED: 81.1 ± 37.5 vs 51.5 ± 50.2 (36% reduction); MT: 65.2 ± 41.3 vs 53.7 ± 52.5 (18% reduction). 4) Values of STAI Y1-STAI Y2, HIT-6 and Beck decreased, but not significantly in both groups. 5) Hematological parameters: WBC count-MED: 7549 vs 6282; MT: 7037 vs 6082. Changes that did occur were chiefly due to decreases of neutrophils. CD3/microlt, CD4/microlt, CD19/microlt decreased too, but not significantly. 6) Interleukin 6 decreased in both groups, significantly in MT-group only (Il-6 MT-group 2.52 ± 4.4 vs 0.7 ± 2.0; Il-6 Med-group 0.75 ± 1.91vs 0.5 ± 1.16). 7) Biological markers: NE, DA and E changed significantly in both groups (NE MT-Group: 323.4 ± 94.8 vs 440.8 ± 117.5; NE Med-group 320.7 ± 86.6 vs 535.6 ± 123.9; DA MT-Group 12.4 ± 13.8 vs 19.9 ± 15.9; DA Med-Group 4.1 ± 2.23 vs 20.3 ± 14.8; E MT-Group 22.95 ± 9.8 vs 42.6 ± 15.5; E Med-Group 22.6 ± 18.5 vs 55.1 ± 22.7). TYR, OCT, SYN did not change significantly.
Conclusion
Our results provide initial evidence of sustained similar effects for MED and MT with
respect to key headache outcomes (but not for psychological variables). Mindfulness
as well as pharmacological treatment seems to influence significantly specific
biological markers of tyrosine metabolism: they changed significantly in both groups
after treatment by indicating a possible restore of the original
unbalance
Disclosure of Interest
None Declared
Psychological and Behavioural Factors and Management
PO-01-158
Comorbidity of migraine and mood episodes in a population-based study in north-eastern Iran
Ali Ghabeli Juibary1,*, Payam Sasannejad1, Kaveh Bahrami1 and Mohammadreza Sobhani1
1Neurology, Mashhad University of Medical Sciences, Mashhad, Iran, Islamic Republic Of
Objectives
Migraine has been found to be comorbid with bipolar disorder and major depressive disorder in clinical and population-based samples. However, significant variability in findings between studies has been found and this proposes that mood episodes examination may be useful in determining which of these mood episodes are specifically associated with migraine and clarify the burden of this problem in population.
Methods
Using a cross-sectional, population-based sample, a group of Iranians at city of Mashhad (North-eastern Iran) have been studied. In this observational study, data on all 450 adult participants, were analyzed. Sociodemographic and clinical correlates of migraine were examined in each combination of mood episodes as well as controls. The relationships between self-reported migraine, perceived mental health, and mood/anxiety disorders were modeled using univariate and multivariate logistic regression. The migraine-depression association was also explored in a subset of participants using the Farsi version of Composite International Diagnostic Interview-Short Form (CIDI-SF) depression scale.
Results
Compared with controls, the adjusted odds ratio of having migraine was 1.8 (95% confidence interval [CI] 1.3–2.9) for manic episodes alone, 1.9 (95% CI 1.6–2.1) for depressive episodes alone, and 3.0 (95% CI 2.3–3.9) for subjects with both manic and depressive episodes. By using CIDI-SF depression scale, the migraine-mood disorders association was significant. The odds of migraine were higher among those with anxiety disorders. The was inverse association between high perceived mental health and the odds of migraine.
Conclusion
Migraine comorbidity seems to outline a subset of individuals with earlier onset of affective illness and more psychiatric complications, suggesting that migraine assessment in mood disorder patients may be useful as an indicator of clinical severity and possible poor response to treatment. Surveillance for mood disorders and comorbid migraine is necessary in clinical settings.
Disclosure of Interest
None Declared
Psychological and Behavioural Factors and Management
PO-01-159
Modeling chronic migraine-like headache in mice using a conditioned place aversion paradigm
Qing Lin1,*, Saurabh Kokane1, Cherith Naig1, Anh Ngo1 and Feng Tao2
1University of Texas at Arlington, Arlington
2Texas A&M University College of Dentistry, Dallas, United States
Objectives
Current animal models of chronic migraine-like headache involve activating nociceptors of the trigeminal afferents present on the meninges by repeatedly administering a mixture of inflammatory mediators into the cisterna magna or via direct topical application on the dura. These models utilize repeated artificial recreation of the pathophysiological changes that induce migraine-like headaches to establish chronicity. The pain of migraine is commonly determined by assessing the development of facial allodynia due to sensitization of trigeminal nociceptors and central neurons in trigeminocervical complex. Conditioned place aversion (CPA) is a commonly used paradigm that uses classical conditioning to pair environment with a motivationally aversive stimulus (pain or foot-shock). This pairing leads to induction of the negative affective state whenever the animal is exposed to the environment. CPA has been used to study neural circuits involved in negative affective components of pain. In this study, we have proposed a novel method involving the use of complete Freund's adjuvant (CFA) as an inflammatory mediator in conjunction with the CPA paradigm to induce an animal model of chronic migraine-like headache.
Methods
Experiments were performed in C57BL/6 mice at ages of 3–4 months of either sex. Under a brief anesthesia by isoflurane, 5 µl of CFA was injected into the dura. Cutaneous allodynia was determined by using von Frey filaments applied to the craniofacial region. The CPA paradigm was used to establish a pain-paired compartment where the animal was conditioned for facial pain state. The effect of the conditioning on the prolongation of CFA-induced acute migraine-like pain was tested and evaluated.
Results
We observed that cutaneous allodynia persisted for 72 hours after single CFA application. After 72 hours, thresholds for mechanical stimuli in the craniofacial regions reverted back to baseline. Interestingly, after conditioning the animals using the CPA paradigm, we found that the mice that had been conditioned continued to demonstrate facial allodynia induced by CFA administration for as long as they were exposed to the pain-paired environment. We were able to maintain the facial allodynic pain state induced by CFA administration for up to 10 days.
Conclusion
These results indicate that although pathophysiological effects of single CFA application persisted for acute stages, the negative affective component associated with migraine pain facilitated by CPA paradigm persisted for much longer. Thus, our pilot study demonstrates a potential use of CPA paradigm in the development of a chronic migraine model, which mimics a feature of chronic migraine-like headache.
Disclosure of Interest
Q. Lin Conflict with: NIH R01 Grant NS040723, S. Kokane: None Declared, C. Naig: None Declared, A. Ngo: None Declared, F. Tao Conflict with: NIH R01 Grant DE022880
Psychological and Behavioural Factors and Management
PO-01-160
Headache worsened by mri
Veselina Grozeva1,2,* and Ivan Milanov1,2
1Medical University Sofia
2MHATNP “St. Naum” Sofia, Sofia, Bulgaria
Objectives
Imaging is not always required when a primary headache diagnosis such as migraine can be set. Imaging in primary headache disorders is performed to exclude a secondary headache with similar phenotype. Physicians must be aware that incidental and clinically insignificant findings might worsen the patient's condition.
Methods
We report a 41-year-old lady with a migraine started at the age of 22, which
chronified after 35 years of age and worsened significantly after a huge arachnoid
cyst was revealed by MRI. 
Results
Our patient used to have menstrually related migraine attacks in her twenties. Pain was pulsating in character, with intensity of VAS = 7. Headache started from the left or right side of the forehead and irradiated occipitally. The pain could spread also towards the ear, or upper teeth. The patient experienced photo- and phonophobia during the attacks and she was unable to perform any tasks. Sometimes the headache was accompanied by nausea and vomiting. Frequency was around 5 attacks monthly. She aborted the severe ones by oral sumatriptan. In patient's late 30s, the number of headache attacks per month raised to 10. She had a concomitant chronic sinusitis and mother with migraine. Brain MRI showed a huge inborn arachnoid cyst in the left temporal region with mild dislocation of the ventricular system. After the patient was informed, headache complaints worsened, despite the fact that the incidental finding was not progressive, not clinically significant. The neurological and cognitive status were both normal. EEG had no abnormalities. Headache was not triggered by exertion, neither by cough. Frequency of the severe attacks raised to 16 per month. She began to use paracofdal (paracetamol 200 mg, metamisol natrium 300 mg, codeine phosphate 20 mg, caffeine 30 mg) and coffergamine (ergotamine tartrate 1 mg, caffeine 100 mg) frequently: two to three tablets of each daily. Depression and insomnia were diagnosed together with a milder persistent daily headache in the vertex and occipital area.
Conclusion
The case report serves as a clear example of how an imaging study performed in the absence of additional worrying symptoms and signs can worsen the condition and the quality of life of a patient with a primary headache. The brain cyst should be monitored in time, but we believe the discomfort and stress that the MRI finding caused to our patient cannot be justified.
Disclosure of Interest
None Declared
Psychological and Behavioural Factors and Management
PO-01-161
The Headache Triggers Sensitivity and Avoidance Questionnaire (HTSAQ-G) – Psychometric Evaluation of a German Adaptation
Anna Caroli1, Timo Klan1,*, Charly Gaul2, Eva Liesering-Latta2, Lyn A. Lücke1, Kirsten K. Wischnewski1, Janine Lüthi1, Judith May1 and Michael Witthöft1
1Department of Psychology, University of Mainz, Mainz
2Migraine and Headache Clinic, Königstein im Taunus, Germany
Objectives
This study aims to develop and validate a German version of Kubik and Martin’s Headache Triggers Sensitivity and Avoidance Questionnaire (HTSAQ, [1]). The HTSAQ was established with regard to the Trigger Avoidance Model of Headaches, which suggests that the avoidance of headache triggers may lead to developing a primary headache disorder. Similar to anxiety disorders, avoidance behavior may generate sensitization and thus an increase in trigger potency. This model has led to a novel approach in the behavioral treatment of primary headache disorders, i.e., the Learning to Cope with Triggers (LCT). While traditional counseling aims at the avoidance of all triggers, the LCT proposes a more differentiated handling of potential triggers. To examine the effectiveness of LCT, the HTSAQ was developed including 24 of the most commonly reported triggers (e.g., stress, odors, lack of sleep) and two open-ended questions for two individual triggers that can be added.
Methods
Like in the original version, respondents are asked to rate for each trigger on a 5-point Likert-scale (a) whether it is a trigger for the respondent’s headaches, (b) how sensitive the respondent is to the trigger compared with other people, (c) how sensitive the respondent is to the trigger compared with the time of least sensitivity, and (d) how hard the respondent tries to avoid the trigger. A sample of N = 99 consecutive patients (75% female; age: M = 44.4, range 15–83; diagnosed with either migraine, tension-type headache, cluster headache or a combination of two or more headache disorders) completed a battery of measures (including the HTSAQ-G and the Depression, Anxiety and Stress Scales, Headache Impact Test-6, Headache Disability Inventory and Chronic Pain Acceptance Questionnaire) at admission for a residential treatment in a headache clinic. With an interval of approx. 4 weeks (at discharge), N = 93 patients completed the battery of tests for a second time.
Results
The HTSAQ-G showed excellent reliability evaluated through internal consistency (alpha = .88) and test-retest reliability (r = .85) over a period of approx. 4 weeks. As first evidence of construct validity, headache patients reporting higher triggers sensitivity and more avoidance behavior showed higher levels of depression (r = .31 to .38), anxiety (r = .33 to .45), stress (r = .29 to .44), and impairment due to pain (r = .31 to .45), and concurrently lower levels of acceptance of pain (r = −.24 to −.41). As the Trigger Avoidance Model of Headache would predict, correlations between the HTSAQ-G Sensitivity scales and the Avoidance scale were strong (r = .69 to .76).
Conclusion
The results of this study support the use of the German adaptation of the HTSAQ as a reliable and valid measure of sensitivity to headache triggers and avoidance of headache triggers. The HTSAQ-G will be of use investigating the effectiveness of novel behavioral treatment approaches to migraine. Future studies should examine the factor structure of the HTSAQ-G using exploratory and confirmatory factor analysis in order to identify possible different types of triggers.
References
1 Kubik, S. U., & Martin, P. R. (2017). The Headache Triggers Sensitivity and Avoidance Questionnaire: Establishing the Psychometric Properties of the Questionnaire. Headache: The Journal of Head and Face Pain, 57, 236–254.
Disclosure of Interest
None Declared
Psychological and Behavioural Factors and Management
PO-01-162
An Integrative Cognitive Behavioral Therapy Program for Adults with Migraine: A Pilot Study
Timo Klan1,*, Eva Liesering-Latta2, Charly Gaul2 and Wolfgang Hiller1
1Department of Psychology, University of Mainz, Mainz
2Migraine and Headache Clinic, Königstein im Taunus, Germany
Objectives
Behavioral therapy (BT) is efficacy in the treatment of migraine [1]. There are different approaches to behavioral treatments for migraine, including relaxation therapy, biofeedback, cognitive-behavioral therapy (CBT) to enhance stress-management, the concept of “learning to cope with triggers” (LCT, [2]), and counselling. It is still unknown, which approach fits to which patient or if a combination of all approaches is superior. The aim of our study was to evaluate the feasibility, acceptability, and preliminary effects of a specific CBT-program for adults with migraine. The program integrates several important approaches (except biofeedback) and comprises 7 sessions: (1) psychoeducation, (2) life-style counselling, (3) coping fear of migraine-attacks, (4) coping the current migraine-attack, (5) LCT, (6) stress-management and (7) relapse prevention. Every session includes a brief relaxation exercise.
Methods
A pilot nonrandomized trial was conducted with N = 10 adults with migraine (age: M = 40,7; SD = 16,7; 80% female; 50% Migraine without aura, 20% Migraine with aura, 30% Chronic migraine). After each of the 7 outpatient group therapy sessions, evaluation questionnaires (5 point scale from 1 = “disagree” to 5 = “agree“) were filled out as a primary outcome measure. Secondary outcome measures were the German Version of the Headache Disability Inventory (IBK), the German Version of the Headache Management Self-Efficacy Scale in a short form (HMSE-G-SF) and the Depression-Anxiety-Stress Scales (DASS). A daily headache e-diary using smartphone and web-based application technology was conducted during the treatment.
Results
The group intervention was feasible and highly accepted. Only N = 1 dropped out (after one session, a further participation was not possible due to repeated migraine attacks ahead of the subsequent sessions). The following results refer to the completer sample (N = 9). The compliance was good (total participation rate of the sessions was M = 86%, SD = 14%). The evaluation of the 7 sessions by the patients showed a high acceptability for every session: contents were comprehensible (M = 4.75; SD = 0.24), session was supporting the coping (M = 4.22; SD = 0.42), and session was satisfying (M = 4.74; SD =0.35). Pre-Post-Effect-sizes were large (IBK: d = 0.84; HMSE-G-SF: d = –0.86), or small (DASS-Depression: d = –0.09; DASS-Anxiety: d = 0.10; DASS-Stress: d = .29).
Conclusion
Our idea to combine several approaches of BT into a specific therapy program for adults with migraine seems to be feasible and promising. The acceptability for the novel approaches (session 3, 4, and 5) including LCT was as good as for the traditional approaches (session 1, 2, and 6). Effect sizes showed a reduced disability and an enhanced self-efficacy. Effect sizes referring to the emotional impairment showed no clear trend, which may be due to the small sample. A randomized controlled trial with headache frequency as a primary outcome to determine the efficacy of our program is now warranted.
References
1 Kropp, P., Meyer, B., Dresler, T., Fritsche, G., Gaul, C., Niederberger, U., ... & Straube, A. (2016). Relaxation therapy and cognitive behavioural therapy for treatment of migraine. Nervenheilkunde, 35, 502–515.
2 Martin, P. R., Reece, J., Callan, M., MacLeod, C., Kaur, A., Gregg, K., & Goadsby, P. J. (2014). Behavioral management of the triggers of recurrent headache: a randomized controlled trial. Behaviour research and therapy, 61, 1–11.
Disclosure of Interest
None Declared
Psychological and Behavioural Factors and Management
PO-01-163
Alterations in attention, fatigue and alertness associated with the premonitory and postdrome stages of triggered migraine attacks
Nazia Karsan1,2,*, Pyari Bose1,2, Charlotte Thompson1 and Peter J. Goadsby1,2
1Headache Group, Department of Basic and Clinical Neuroscience, Institute of Psychiatry, Psychology and Neuroscience, King's College London
2NIHR-Wellcome Trust King's Clinical Research Facility, King's College Hospital, London, United Kingdom
Objectives
Despite increasing awareness that non-painful symptoms can manifest at any time during a migraine attack, there is little quantitative evidence to support the severity of such symptoms.
We aimed to understand the differences in fatigue (Daily Fatigue Impact Scale- DFIS), attention (Sustained Attention to Response Task- SART) and alertness (Karolinska Sleepiness Scale- KSS) at baseline and during the premonitory and postdrome stages of nitroglycerin-triggered migraine attacks, using validated psychological tests.
Methods
Subjects aged 18–50 years with spontaneous migraine with or without aura were pre-screened over the telephone and if deemed eligible for the study, invited to a screening appointment. Following informed consent, detailed migraine history taking, observations, an electrocardiogram, a pregnancy test where applicable and a physical examination, each subject was exposed to a 0.5 mcg/kg/min nitroglycerin (NTG) infusion over 20 minutes, to attempt to trigger premonitory symptoms and headache.
Following the development of headache, where applicable, headache was treated with either 1 g intravenous aspirin (the premonitory patients) or 6 mg subcutaneous Sumatriptan (the postdrome patients).
Baseline (symptom free) scores for all tests for each subject (n = 21) were collected prior to any drug administration. The same tests were conducted in the premonitory (n = 9) or postdrome (n = 12) phases of triggered attacks, following display of symptoms after NTG infusion and when appropriate, after effective headache treatment. Subjects were chosen for which arm of the study they were put into, based on their usual attacks and which symptomatology was dominant and which treatment they usually responded to with spontaneous attacks.
The premonitory phase was defined as the presence of three or more non-headache symptoms which started before the onset of headache, which the subject would usually associate with successfully predicting the onset of headache. The postdrome phase was defined as the presence of three or more symptoms following headache resolution, which the subject would associate with headache freedom but not feeling completely back to normal.
Statistical analyses were performed using Pearson correlation and paired t-tests. P < 0.05 was considered significant.
Results
There were statistically significant increases in scores on the DFIS in the premonitory stage compared to baseline (tX = −3.76, 95% CI −17.465 – −4.090, p = 0.006) and in the postdrome stage compared to baseline (tX = −3.668, 95% CI −3.635 – −3.688, p = 0.004). There were statistically significant increases in scores on the KSS in the premonitory stage compared to baseline (tX = −3.255, 95% CI −3.796 – −0.648, p = 0.012) and in the postdrome stage compared to baseline (tx = −6.402, 95% CI −5.515 – −2.667, p < 0.001). No statistically significant differences in SART scores in the premonitory phase or postdrome phase were observed compared to baseline. There was no significant correlation between the baseline DFIS, KSS and SART scores and headache days at baseline.
Conclusion
Despite a small sample size, we have demonstrated notable changes in alertness and fatigue in the premonitory and postdrome stages of a migraine attack. This is an area that warrants increased clinical and research attention.
Disclosure of Interest
N. Karsan Conflict with: Dr Karsan is an Association of British Neurologists/Guarantors of Brain Clinical Research Training Fellow, P. Bose: None Declared, C. Thompson: None Declared, P. Goadsby Conflict with: Dr. Goadsby reports grants and personal fees from Allergan, Amgen, and Eli-Lilly and Company; and personal fees from Akita Biomedical, Alder Biopharmaceuticals, Autonomic Technologies Inc, Avanir Pharma, Cipla Ltd, Colucid Pharmaceuticals, Ltd, Dr Reddy's Laboratories, eNeura, Electrocore LLC, Novartis, Pfizer Inc, Promius Pharma, Quest Diagnostics, Scion, Teva Pharmaceuticals, Trigemina Inc., Scion, Conflict with: personal fees from MedicoLegal work, Journal Watch, Up-to-Date, Oxford University Press; and in addition, Dr. Goadsby has a patent Magnetic stimulation for headache pending assigned to eNeura
Psychological and Behavioural Factors and Management
PO-01-164
A Multidisciplinary Team Approach for Chronic Migraine Treatment: A Clinical Case Study
Lindsey Reeves1,*, Lori Ginoza1 and Lauren Green1
1University of Southern California, Los Angeles, United States
Objectives
Chronic migraine (CM) affects up to 5% of the global population and negatively impacts a person’s quality of life and ability to engage in daily activities. While primary care physicians and neurologists frequently treat CM with pharmacological interventions, lifestyle, behavioral and physical rehabilitation provided by occupational therapists (OT) and physical therapists (PT) can be effective for treating and managing CM. At the USC Keck Medical Center a multidisciplinary team including neurologists, OTs, PTs and pain psychologists has been established to treat patients with head, neck and facial pain disorders, including CM.
The aim of this study is to understand how a multidisciplinary treatment approach can be used for CM, explain the role of neurology, OT and PT, and present a case study to demonstrate the effectiveness of a multidisciplinary approach.
Methods

Results
A 36 year-old female patient who works as a chef with a diagnosis of CM without aura was used for this case study. She had worsening of headaches for 8 months and was experiencing left-sided neck tightness and jaw pain. Neurology evaluated the client, implemented pharmacological changes, and referred the patient to OT and PT. LR OT and PT treatment was provided at outpatient clinics where the patient was seen for 8 sessions, by each discipline, over the course of 3 months. OT treatment topics included sleep hygiene and positioning, activity pacing, stress management, trigger identification, ergonomics and time management. PT prescribed exercises to improve strength of deep neck flexors, scapular stabilizers, and core muscles and spine flexibility to improve postural mechanics and tolerance to complete daily and work-related tasks. PT treatment also included manual therapy to reduce neck and jaw symptoms. Clinical outcomes are included in Table 1.
Conclusion
This case study demonstrates the effectiveness of using a multidisciplinary approach for treating chronic migraine and improving a patient’s symptoms, quality of life and function.
Disclosure of Interest
None Declared
Psychological and Behavioural Factors and Management
PO-01-165
Decision-making in Medication Overuse Headache under ambiguity and under risk
Sara Bottiroli1,2,*, Grazia Sances1, Elena Cavallini2, Alessia Rosi2, Riccardo Russo2, Viana Michele1, Vito Bitetto1, Marta Allena1, Giorgio Sandrini3,4 and Cristina Tassorelli1,2
1Headache Science Centre, C. Mondino National Neurological Institute
2Department of Brain and Behavioral Sciences, University of Pavia
3Department of Brain and Behavioral Sciences, C. Mondino National Neurological Institute
4Headache Science Centre, University of Pavia, Pavia, Italy
Objectives
To evaluate whether Medication Overuse Headache patients (MOH) (progressed from migraine) differ from episodic migraine patients (MIG) as regards decision making and whether, within MOH patients, this ability is influenced by the duration of chronification.
Methods
In order to to explore whether possible differences between groups were attributable to the type of decision-making situation, we used two different tasks: 1) ambiguous information is provided and the outcome of choices is not defined by clear probabilities (decision under ambiguity), 2) explicit information is provided and the outcome is defined by probabilities (decision under risk). We recruited 47 patients, n. 22 suffered from MOH evolved from migraine (chronic migraine + MOH) (77.3% female, Age: 46.7 ± 11.1, Years of education:12.4 ± 3.7), while 25 suffered from MIG (68.0% female; Age: 41.9 ± 13.9, Years of education:14.3 ± 3.8). The diagnosis in the 2 groups was operationally defined according to ICHD-IIIβ. Within the MOH group, 12 patients suffered of chronic headache since at least 10 years (long-lasting MOH, 83.3% female, Age: 51.8 ± 8.2, Years of education:12.6 ± 3.5, Chronification duration: 20.3 ± 9.6), whereas 10 since less than this duration (short-lasting MOH, 70.0% female, Age:44.5 ± 11.8, Years of education:12.7 ± 3.9, Chronification duration: 7.1 ± 2.6). All individuals were recruited at the Headache Center of Neurological National Institute “Mondino”, Pavia. All patients completed the two different tasks being comparable in terms of intrinsic characteristics of the game: one decision-making task under risk, the Game of Dice Task (GDT), and one decision task under ambiguity, the Iowa Gambling Task (IGT). Demographic and clinical information was collected as well.
Results
As regards the decision task under ambiguity, interesting differences resulted between the MOH group and the MIG group as the MOH made significantly more disadvantageous and risky choices than the MIG group: IGT net score for MOH group −6.2 ± 22.6, for MIG group 12.0 ± 22.2; F(1,44) = 7.54, p = .009. No significant difference emerged between MOH and MIG patients as regards the decision task under risk: GDT net score: MOH 4.9 ± 11.6; MIG 7.4 ± 9.4; F(1,45) = 0.66, p = .42. Interestingly, when evaluating the impact of MOH duration on the decision-making performance, we found that patients with the longer duration of disease made significantly more disadvantageous and risky choices at the task under risk: GDT net score: long-lasting −0.5 ± 12.3; short-lasting 11.46.7; F(1,20) = 7.48, p = .013. No difference was instead detected as regards the task under ambiguity: IGT net score long-lasting −4.3 ± 19.1; short-lasting −8.7 ± 27.7; F(1,19) = 0.18, p = .67.
Conclusion
Patients with chronic pain conditions such as chronic migraine have to face important and complex decisions with respects to their health care. For this reason, the ability to make advantageous decisions may have a relevant impact on different steps of management, such as intake of medications and adherence to treatment. Our data are very interesting as they show two different patterns of decision making according to the kind of patients considered. MOH group as a whole showed a reduced performance in decision-making under ambiguity. When the duration of disease is long (≥10 years) also the performance in decision-making under risk becomes affected in this group of patients. Though preliminary, these findings highlight an important component in the complex approach to MOH.
Disclosure of Interest
None Declared
Psychological and Behavioural Factors and Management
PO-01-166
The Women’s Health and Migraine Trial (WHAM): A Randomized Controlled Trial of Behavioral Weight Loss as a Treatment for Migraine in Women with Overweight/Obesity
Dale S. Bond1,*, J G. Thomas1, Richard B. Lipton2, Jelena M. Pavlovic2, Kevin C. O'Leary1, Julie Roth3, Lucille Rathier4, E W. Evans1 and Rena R. Wing1
1The Miriam Hospital/Brown Alpert Medical School Weight Control and Diabetes Research Center, Providence
2Montefiore Headache Center, Albert Einstein College of Medicine, Bronx, NY
3Rhode Island Hospital/Brown Alpert Medical School
4The Miriam Hospital/Brown Alpert Medical School, Providence, United States
Objectives
Research suggests that obesity is both a risk and exacerbating factor for migraine, particularly in reproductive-aged women. Additionally, uncontrolled studies suggest that weight loss has potential to reduce migraine frequency and severity in the context of obesity. The present study is the first to test the efficacy of a standardized behavioral weight loss (BWL) intervention for decreasing headache frequency and severity in women with comorbid migraine and overweight/obesity within a randomized controlled trial.
Methods
A total of 108 women aged 18–50 years who had neurologist-confirmed migraine with or without aura, 4–20 headache days/month and body mass index (BMI) between 25 and 49.9 kg/m2 were randomly assigned to 16 weekly in-person group sessions of either: 1) BWL (n = 52), that aimed to produce weight loss via instruction in behavioral strategies targeting physical activity and diet (but did not address migraine); or 2) Migraine education control (ME; n = 56), involving didactic information on migraine headaches and evidence-based pharmacological/non-pharmacological management approaches (but did not address weight loss). Both groups used a smartphone diary to record headache activity for 4 weeks at both baseline, prior to randomization, and the end of treatment (16 weeks). The primary outcome measure was change in number of migraine headache days. Analyses focused on changes in body weight, migraine headache days, and other variables of interest controlled for baseline values and employed the intention-to-treat principle with no change imputed for missing data.
Results
Retention rate at the primary end point was 77.8% and similar between groups. BWL and ME did not differ in age (39.2 ± 7.2 years), BMI (35.2 ± 6.7 kg/m2), monthly migraine days (8.3 ± 4.5), and % using preventive (20.2%) medications at baseline (ps > .30). BWL achieved significantly greater mean (±SD) weight loss than ME at 16 weeks (−3.2 ± 4.4 vs. +0.6±2.3 kg, p < .001). Number of monthly migraine days decreased significantly between baseline and end-of-treatment in both BWL (8.1 ± 3.9 to 6.0 ± 4.3 days/month; p < .001) and ME (8.6 ± 4.8 to 5.3 ± 4.8 days/month; p < .001), but did not differ from each other (p = .11). A similar pattern of findings with significant (p < .05) decreases between baseline and end-of-treatment occurring in both the BWL and ME groups, but no significant between-group differences (BWL vs. ME), was shown for average headache intensity (5.8 ± 1.4 to 5.1 ± 2.2 vs. 5.8 ± 1.6 vs. 5.0 ± 2.4 on 0–10 scale, p = .61), attack duration (20.4 ± 17.6 to 19.6 ± 20.6 hours/attack vs. 19.8 ± 14.4 to 15.4 hours/attack, p = .13), and disability measured via the Headache Impact Test−6 (65.7 ± 4.3 to 61.5 ± 6.4 vs. 63.9 ± 4.2 to 60.8 ± 5.3, p = .62).
Conclusion
Intensive, 16-week long BWL and ME control interventions produced significant but similar reductions in migraine frequency and severity among women who with both migraine and overweight/obesity. Further research in this population is needed to determine whether: 1) mechanisms of migraine improvement differ between BWL and ME; 2) either intervention is superior in maintaining migraine improvements over time; and 3) combining BWL and ME yield greater migraine improvements than either treatment alone.
Disclosure of Interest
D. Bond Conflict with: National Institutes of Health, Agency for Healthcare Research and Quality, Grace K. Alpert Award in Clinical Neurosciences, The Miriam Hospital Foundation, Weight Watchers International, Inc., Conflict with: Covidien/Medtronic, Conflict with: American Headache Society, J. Thomas Conflict with: National Institutes of Health, Weight Watchers International, etc., R. Lipton Conflict with: eNeura Therapeutics, Conflict with: National Institutes of Health, National Headache Foundation, Boston Scientific, Conflict with: Alder, Allergan, American Headache Society, Amgen, Autonomic Technologies, Avanir, Boehringer-Ingelheim, Boston Scientific, Bristol-Meyers Squibb, Colucid, Dr. Reddy's, Electrocore, Eli Lilly, eNeura Therapeutics, Merck, Novartis, Pfizer, Teva, Vedanta, Conflict with: Royalties from Wolff's Headache, 8th Edition, Oxford Press University, 2009 and Informa, J. Pavlovic Conflict with: Allergan, Inc., Conflict with: American Headache Society, K. O'Leary: None Declared, J. Roth: None Declared, L. Rathier: None Declared, E. Evans: None Declared, R. Wing Conflict with: National Institutes of Health
Psychological and Behavioural Factors and Management
PO-01-167
The effect of emotional and cognitive aspect of pain perception on headache related disability in migraine patients
Dae Woong Bae1,* and Jeong-Wook Park1
1Neurology, Catholic university of Korea, Seoul, Korea, Republic Of
Objectives
Disability due to migraine can be influenced by emotional and cognitive aspect of pain perception. This study aims to evaluate the difference on pain perception between migraine patients and normal population. Secondly, this study aims to examine the effect of distorted pain perception on headache related disability in migraine patients.
Methods
A normal control of 106 health care professionals and their relatives without pain completed questionnaires on pain perception, the Korean version of the Pain Anxiety Symptoms scale (PASS), the Pain Catastrophizing Scale (PCS), and the Pain Sensitivity Questionnaire (PSQ). 145 migraine patients aged 19 to 70 years who visited outpatient neurology clinics in two hospitals were also requested to complete questionnaires on pain perception. Both normal control and migraine patients also fulfilled questionnaires on general psychological distress, the Hospital Anxiety and Depression Scale (HADS). Next, migraine patients completed questionnaires on disability due to migraine, in this case the Korean version of the Headache Impact Test-6 (HIT-6) and the Migraine Disability Assessment (MIDAS). The pearson correlations analysis among each variable and stepwise backward multiple regression analysis were used by R-statistics.
Results
Migraine patients showed significantly higher scores on PASS, PCS, PSQ and HADS, compared to normal control. In migraine patients, PASS, PCS, PSQ showed correlation with each other, especially strong correlation between PASS and PCS (Pearson’s r = 0.746, P < 0.000). However, PASS, PCS, PSQ showed no significantly strong correlation with pain characteristics. Migraine patients also demonstrated correlation between questionnaires on pain perception (PASS, PCS, PSQ) and questionnaires on general psychological stress (HADS). After adjusting for pain characteristics and all questionnaires, stepwise backward multiple regression analyses demonstrated that PASS, HADS-A, headache frequency were an independent predictor associated with HIT-6 (p = 0.001, p = 0.020, p = 0.006). Associated with MIDAS, headache frequency and PASS were an independent predictor (p = 0.000, p = 0.027).
Conclusion
These study suggested that migraine patients have distorted emotional and cognitive aspect of pain perception, independently of pain characteristics itself. PASS showed the most important contribution to HIT-6 among variables, implying effect of distorted pain perception on headache related disability in migraine patients.
Disclosure of Interest
None Declared
Psychological and Behavioural Factors and Management
PO-01-168
Circadian phase typing in episodic and chronic migraine: dim light melatonin onset and pattern of melatonin secretion
Roberto De Icco1,*, Maria C. Berri1, Raffaele Manni2, Silvia Cerri3, Marta Allena4, Vito Bitetto1, Daniele Martinelli1, Giorgio Sandrini1, Giuseppe Nappi4, Cristina Tassorelli1 and Grazia Sances4
1Dept. of Brain and Behavioral Sciences, Headache Science Center, C. Mondino National Neurological Institute
2Unit of Sleep Medicine and Epilepsy, C. Mondino National Neurological Institute
3Laboratory of Functional Neurochemistry, C. Mondino National Neurological Institute
4Headache Science Center, C. Mondino National Neurological Institute, Pavia, Italy
Objectives
A strong association between primary headaches and sleep disorders is well described in literature, although the dynamics underlying this interaction are not known. Sleep disturbances are indicated among trigger factors for migraine and seem to favor its progression toward chronification. It is also possible that a central neural dysfunction in migraine leads to an imbalance in sleep-wake regulation or that the two disorders share common pathophysiological mechanisms (i.e. chronobiological dysfunction). The Dim Light Melatonin Onset (DLMO) is a reliable marker of the endogenous circadian phase and it is defined as the time of the nychtemeron when the salivary melatonin reaches and maintains the 3 pg/mL concentration. The aim of our study was to investigate subjective and biological components of the chronotype in patients with episodic and chronic migraine.
Methods
We enrolled 8 patients with episodic migraine (EM), 19 patients with chronic migraine and medication overuse headache (MOH), and 22 healthy controls (HC). We evaluated the following parameters: All subjects were evaluated with: 1) DLMO, melatonin concentration of the first post-DLMO salivary sample (ELISA method), melatonin surge in the 30-minute interval after DLMO; under-the-curve area of the post-DLMO semicurve; 2) sleep interview aimed to assess mean sleep times, midsleep (midtime between sleep onset and sleep end) on work days (MIDwd), on free days (MIDfd), corrected for sleep duration (MIDc), social jet lag (SJL); 3) subjective chronotype by means Morningness–Eveningness Questionnaire (MEQ); 4) sleep quality by means of Pittsburgh Sleep Quality Index (PSQI); 5) headache disability measured by MIDAS, day of headache/month and days of drugs intake/month.
Results
The mean sleep onset and offset times on work days and free days, the MIDwd, the MIDfd and the MIDc occurred significantly earlier in MOH as compared to HC. In particular MIDc was 3:16 ± 0:40 in MOH, 4:03 ± 0:48 in EM and 4:29 ± 0:54 in HC. We did not find significant differences between MOH and EM regarding other sleep parameters. The mean MEQ score was significantly higher in the MOH group (59.44 ± 8.04) than in the HC group (54.88 ± 8.77, p = 0.001), with the percentage of morning type being was 61.1% in MOH, 37.5% in EM and 18.2% in HC (p = 0.04). The mean PSQI score was higher in the MOH group as compared to controls (p = 0.018). DLMO occurred at 20:43 ± 00:58 in MOH, 20:41 ± 00:48 in EM and 21:18 ± 01:11 in HC, without any significant difference between groups. Similarly distributed among groups was the percentage of morning, intermediate and evening types according to DLMO. The pattern of after-DLMO melatonin secretion was comparable in all groups.
In both MOH and EM the MIDc significantly correlated with days of headache/month (p = 0.01), days of drug intake/month (p = 0.008), age (p = 0.034), MEQ (p = 0.001) and DLMO (p = 0.001). The MIDAS and the PSQI significantly correlated in both MOH and EM groups.
Conclusion
MOH patients are more morning-oriented than HC as measured by MEQ and by MIDc. However MOH patients did not show an early circadian phase as measured by DLMO. Several factors may account for the observed discrepancy, including the impact of the disease chronicity on the patients’ lifestyle. Moreover this discrepancy could represent a predictor of migraine chronification.
Acknowledgements: This study was supported by a grant of the Italian Ministry of Health to Institute C. Mondino (RC 2016).
Disclosure of Interest
None Declared
Psychological and Behavioural Factors and Management
PO-01-169
Do Headache Patients require more care in between visits than other Neurology outpatients?
Roland Brilla1,* and Susanne Seeger1
1Neurology, Universit of Wisconsin Madison, Madison, United States
Objectives
To establish whether headache patients require a high level of care in addition to clinic visits, based on the quantity of remote encounters (phone calls and secure email communication to the clinics), in comparison to other neurologic subspecialty clinics.
Methods
In an academic referral clinic, a total of 3164 established patients were included in this retrospective analysis, 275 from the Headache clinic, the remainder from the Epilepsy clinic, Movement disorder clinic, the MS/neuroimmunology clinic, the neuromuscular clinic and the General Neurology clinic. Patients presenting for a follow up visit between January 2014 and April 2016 were observed for a 12 month period during which the number of telephone and secure email (Mychart) encounters was recorded; in addition, the number of entries related to each of these encounters was registered. This analysis did not require IRB approval as per institutional guidelines.
Results
Based on preliminary analysis of available data, Headache Clinic patients required a high intensity of remote encounters (composite of both telephone- and email messages), this is only surpassed by the MS/neuroimmunology Clinic. Usage of secure email messaging (mychart) was much higher in the Headache Clinic compared to the other clinics. There was no convincing negative correlation of email messaging usage to age.
Conclusion
Patients in a headache clinic in an academic tertiary care setting require a high intensity of remote outpatient care, more so than patients in other neurology subspecialty clinics and general neurology clinic, with the exception of the Neuroimmunology/MS clinic that has an even higher intensity of remote encounters (and related medical record entries). This was to a large extent secondary to the use of secure email linked to the electronic medical record by headache patients. Reconfirmation of these findings by other clinics/centers and investigation of possible predictive patient factors (e.g. psychiatric comorbidity, as has been suggested by others) is warranted.
Disclosure of Interest
None Declared
Psychological and Behavioural Factors and Management
PO-01-170
The role of subjective meaning and cognitive beliefs about sensations in the provocation of sensations in head and neck
Elena Rasskazova1, Yulia Migunova1,* and Aleksandr Tkhostov1
1Psychology, Lomonosov Moscow State University, Moscow, Russian Federation
Objectives
Psychological factors play in important role in both triggering and perpetuation of somatic symptoms (Leventhal et al., 2003, Rief et al., 1998) including pain and headache (Nash et al., 2006, Smitherman et al., 2015, Ak et al., 2004). Psychological model of body function regulation (Rasskazova et al., 2014) suggests that negative subjective meaning of symptoms is associated with higher general level of sensations in the situations requiring bodily functions monitoring especially in those with dysfunctional cognitive beliefs. Positive meaning could lead to higher risk of specific head-related sensations under these tasks.
The aim of this study is to reveal the role of subjective meaning and cognitive beliefs about sensations in the provocation of head-related sensations in healthy participants.
Methods
36 healthy students (21 male, 15 female) without history of headaches participating in the biofeedback training were randomly assigned to one of three instructions. Under the neutral instruction they were told that during this task people typically have bodily sensations, mainly in head and neck. Negative instruction added that such symptoms are typical for neurotic people with psychological problems while positive instruction portrayed people with sensations as attentive and talented. All participants filled Screening for somatoform symptoms (Rief, Hiller, 2003) and Cognitions About Body and Health Questionnaire (Rief et al., 1998).
Results
24 participants (66.7%) reported some bodily sensations during training. 15 participants (41.7%) reported sensations in the head and neck (pain, pressure, tingling, tickling, dizziness). Under negative instruction most participants reported head-unrelated or no sensations (N = 5, 33.3% and N = 8, 53.3%, consequently). Under both neutral and positive instructions they more frequently (χ2 = 9.5, p < .05, V = .36) reported head-related sensations (under neutral instruction: 50.0%, OR = 6.5; under positive instruction: 36.4%, OR = 3.7).
Comparing to both negative (OR = 2.3) and neutral (OR = 4.5) conditions participants under positive instruction more frequently reported any sensations.
The likelihood of any sensations was higher in those believing that their body is weak and vulnerable to environmental factors (F = 4.3, p < .05) and marginally related to the rate of unexplained somatic symptoms (F = 3.3, p < .08). Catastrophization was related to higher risk of sensations under negative and positive but not neutral instructions (F = 4.2, p < .05) while low level of health habits was related to no sensations under positive instruction comparing to the negative and the neutral ones (F = 3.2, p < .06). Patterns of results were the same for both head-related and head-unrelated sensations.
Conclusion
In line with a cognitive approach the frequency of head-related sensations in the task requiring attention and monitoring of the bodily functions is high under neutral condition and is related to belief about bodily weakness and general level of unexplained somatic symptoms.
According to the psychological model of body function regulation data suggests that negative meaning of head-related sensations leads to their lower frequency but higher level of head-unrelated sensations due to efforts to prevent head-related sensations. Positive meaning of head-related sensations could provoke head-related sensations especially in those concentrating of their health and health behavior. Catastrophization seems to be a risk factor of bodily sensations only under specific subjective meaning of these symptoms.
Research was supported by the Russian Foundation of Fundamental Research, project 17-06-00849.
Disclosure of Interest
E. Rasskazova Conflict with: Research was supported by the Russian Foundation of Fundamental Research, project 17-06-00849, Y. Migunova Conflict with: Research was supported by the Russian Foundation of Fundamental Research, project 17-06-00849, A. Tkhostov Conflict with: Research was supported by the Russian Foundation of Fundamental Research, project 17-06-00849
Psychological and Behavioural Factors and Management
PO-01-171
Illness representation as a moderator of the relationship between headache severity and quality of life in patients with migraines and tension-type headaches
Yulia Migunova1,*, Elena Rasskazova1, Alisa Andrushenko2 and Alla Spivakovskaja1
1Lomonosov Moscow State University
2I.M. Sechenov First Moscow State University, Moscow, Russian Federation
Objectives
According to common-sense model (Leventhal et al., 2003) illness representation regulates patients’ coping with somatic illnesses from both cognitive and emotional levels affecting their quality of life. Research demonstrated the role of anxiety sensitivity (Ocanez et al., 2016), catastrophization (Holroyd et al., 2007), perception of pain (Mongini et al., 2009, Vowles et al., 2016) in headache severity and perpetuation while cognitive behavioral therapy (CBT) suggest strategies of effective pain management (McCracken, Turk, 2002).
The aim of this study was to reveal a role of illness representation on quality of life in patients with chronic headaches.
Methods
75 patients (62 females, mean age 42.0 ± 14.3 years old) with chronic migraines and tension-type headaches filled Migraine Disability Assessment Test (Stewart, 2001), revised version of Illness Perception Questionnaire (Moss-Morris et al., 2002) and a brief version of Quality of Life and Enjoyment Questionnaire (Ritsner et al., 2005).
Results
Headache severity negatively correlated with satisfaction with health and emotions (r = –.26, p < .01) but not with leisure time activity and communication. After statistical control for headache severity (R2 = 13.0%), satisfaction with health was higher (ΔR2 = 23.1%) in those who believed in their personal control (β = .31, p < .05) and had less emotional reactions to the illness (β = –.33, p < .05). There was marginally significant interaction between headache severity and emotional representations (β = .18, p < .08, ΔR2 = 3.0%): emotional reactions to illness better predicted dissatisfaction with health in those with less severe headache.
Satisfaction with emotions adjusted for headache severity (R2 = 12.9%) was additionally related (ΔR2 = 20.6%) to lower emotional representations (β = –.34, p < .05). The effect of headache severity was moderated by beliefs about illness length and personal control (ΔR2 = 10.3%, p < .01, β = –.38 – –.24): higher headache severity was related to dissatisfaction only in those who believed that their illness is long-term. The relationship was paradoxically stronger for patients believing in their control under headaches.
Belief in negative consequences of illness was related to dissatisfaction with leisure time activity (ΔR2 = 20.6%, p < .05, β = -.31). Satisfaction with communication was unrelated to both headache severity and beliefs about illness but there was an interaction effect between belief about illness length and headache severity (ΔR2 = 7.6%, p < .05, β = -.29): only in those with more severe headaches belief that illness is long-term correlated with dissatisfaction with communication.
Major patterns of relationships remained after controlling for headache type (migraines versus tension-type headaches).
Conclusion
From the CBT perspective, data supports that work with patients’ beliefs about illness length, consequences, personal control and especially emotional representations could be helpful for quality of life regardless of headache severity. Patients are more satisfied with health and emotions if they have less emotional reactions to the illness and more satisfied with health if they believe that they can control their headache. Also patients with lower beliefs in the negative consequences of their headache are more satisfied with leisure time activity. Moreover, beliefs that headache is long-term and controllable seem to strengthen negative effect of headache severity on satisfaction with emotions while emotional representations could strengthen negative effect of headache severity on satisfaction with health.
Research was supported by the Russian Foundation of Fundamental Research, project 17-06-00849.
Disclosure of Interest
Y. Migunova Conflict with: Research was supported by the Russian Foundation of Fundamental Research, project 17-06-00849, E. Rasskazova Conflict with: Research was supported by the Russian Foundation of Fundamental Research, project 17-06-00849., A. Andrushenko: None Declared, A. Spivakovskaja: None Declared
Psychological and Behavioural Factors and Management
PO-01-172
Identification of herbal plants for the treatment of headaches
Vikas Sharma1,* and Sukrat Sinha1
1Biotechnology, Guru Gobind Singh Indraprastha University, New Delhi, India
Objectives
Herbs have been used in traditional medicine for several thousand years. The knowledge of medicinal plants has accumulated in the course of time in different medicinal systems such as Ayurveda, Unani and Siddha. The objective of this study was to interact with local traditional healers and document the medicinal plants effective in treating headaches.
Methods
Details regarding traditional herbal medicine were acquired from indigenous with local traditional healers and document their knowledge on medicinal plants. Prepared questionnaires were used for this purpose.
Results
Our study showed that there are 11 herbs traditionally to treat headaches. Because of the importance of these medicinal plants it is necessary to determine the distribution and availability of these herbs. Also there is need to further study the effect of these medicines.
Conclusion
The study indicated that there are plenty of medicinal plants to treat headache. Extensive study should be designed to identify the mode of action and other important aspects of these herbs.
Disclosure of Interest
None Declared
Tension-Type Headache
PO-01-173
Neurophysiological mechanisms in tension-type headache chronification
Kostiantyn Stepanchenko1,*
1Neurology, KHARKIV MEDICAL ACADEMY OF POSTGRADUATE EDUCATION, Kharkiv, Ukraine
Objectives
Aim of the study - to determine the EEG patterns of adolescents with tension-type headache (TTH) and differences in EEG patterns in various forms of TTH.
Methods
105 adolescents with TTH were examined. Four groups: 1st (46 pers.) - patients with infrequent episodic tension-type headache (IETTH), 2nd (40 pers.) - patients with frequent episodic tension-type headache (FETTH), 3d (19 pers.) - patients with chronic tension-type headache (CTTH), 4th (20 pers.) - healthy adolescents (control group) were formed. EEG study included visual, spectral, and nonlinear multidimensional analysis (deterministic chaos, calculated Kolmogorov-Sinai entropy) EEG.
Results
Patients with TTH had increased activity of both arousal-1 system (A-1 - mesencephalic reticular formation of the brainstem), and arousal-2 (A-2 - hippocampal cortex and septum pellucidum) system. Patients with IETTH had increased activity of A-1, and patients with FETTH and CTTH - A-2. The compensatory synchronizing influence on the cerebral cortex had been associated with an increase in the functional activity of thalamocortical system (C-2) in the patients with IETTH and FETTH, and reticulocortical system (C-1) in the patients with CTTH. Imbalance between activating systems (switching A-1 to A-2) and synchronizing systems (reducing the activity of C-2 and the relative increase of the activity of the C-1) has been associated with clinical signs of transformation of FETTH to CTTH. The value Kolmogorov-Sinai entropy decreased simultaneously with increasing frequency of TTH.
Conclusion
Complex changes of cortical-subcortical relationships, such as activation of the limbic structures; lack of the activity of the synchronization thalamocortical system; the relative increase of the activity of the reticulocortical system; the formation of stable pathological dominant (‘central sensitization’) in key limbic structures are associated with transformation of EEG pattern of “paroxysmal” headache to pattern of “chronic” headache in adolescents with tension-type headache.
Disclosure of Interest
None Declared
Tension-Type Headache
PO-01-174
“How do Italian osteopaths treat and manage tension-type headache? A qualitative study”
Alessio Iacopini1,2,*, Francesco Cerritelli2 and Jorge Esteves3,4
1Research Department, CROMON, Rome
2Clinical-Based Department, Come Collaboration, Pescara, Italy
3Research Department, Instituto Piaget, Lisbona, Portugal
4Osteopathic Health Centre, Dubai, United Arab Emirates
Objectives
This qualitative study explored the attitudes, beliefs and values of osteopaths practising in Italy regarding the evaluation, treatment and management of patients with tension-type headache (TTH).
Methods
Ten osteopaths were recruited by theorethical sampling from the teaching faculty of an osteopathic college in Italy. In-depth, individual semi-structured interviews were conducted; the interviews were audiorecorded and verbatim transcribed. Data were coded and analysed using Thematic Analysis with elements of Grounded Theory to identify common trends reported by osteopaths with experience in treating and managing people with TTH. The consolidated criteria for reporting qualitative research checklist (COREQ) was used to improve the transparent reporting of qualitative data. Researcher bias/trustworthiness were mitigated using a researcher, with experience in qualitative research, checking 20% of interview transcripts. Transcripts were checked and edited by participants. Member-checking was used to control for accuracy. Finally, peer debriefing including colleagues, researchers and educators not involved directly in the study, was used to consider different aspects of the findings model of interpretation.
Results
Four main themes were identified: 1) osteopathy and its alternative perspective on patients’ perception 2) the osteopaths’ decision making process regarding the selection of treatment approaches; 3) the person’s management through and individualized case treatment model; 4) a renewed person-centred approach setting the treatment in a environment to find fulfilment of individual potential. The participants tailored TTH management to suit patients’ needs and preferences. Treatment strategies resulted highly individual, giving the headache patient a central role within the care process.
Conclusion
Osteopaths endorsed a person-centred renewed approach. Although the clinical conditions and disabilities associated with TTH were considered carefully, osteopaths reported how, a more targeted approach at improving and promoting the individual’s wellbeing and symptomatic relief of their symptoms, should be the main aim of osteopathic treatment. Moreover, our findings highlighted the active role of the patient in the process of care and how the osteopath-patient relationship is crucial to create a robust therapeutic alliance.
Disclosure of Interest
None Declared
Tension-Type Headache
PO-01-175
Dynamic Mechanical Hypersensitivity in the Trigeminal Area in Tension Type Headache
María Palacios-Ceña1, Ángel Guerrero-Peral2,*, Marina Ruíz2, Cesar Fernandez-De-Las-Peñas1 and Lars Arendt-Nielsen3
1Fisioterapia, Terapia Ocupacional, Rehabilitación y Medicina Física, UNIVERSIDAD REY JUAN CARLOS, ALCORCON
2Headache Unit, Hospital Clínico de Valladolid, Valladolid, Spain
3Health Science and Technology, Aalborg University, Aalborg, Denmark
Objectives
To explore the association of dynamic algometry for evaluating dynamic mechanical hyperalgesia with headache clinical features and widespread pressure pain sensitivity in subjects with tension-type headache (TTH).
Methods
One hundred eighty-eight individuals with TTH (70% women) participated. They were diagnosed of TTH according to the International Classification of Headache Disorders (ICHD-III) criteria. Exclusion criteria included other primary headaches, whiplash, medication overuse headache, fibromyalgia or any neurological disorder. A 1-month headache diary was used to collect clinical data and preventive medication intake Dynamic hyperalgesia was assessed with a dynamic pressure algometry set (Aalborg University, Denmark©) consisting of 11 different rollers with fixed levels from 500 g to 5300 g. Each roller was moved at a speed of 0.5 cm/sec over a 60 mm horizontal line covering the temporalis muscle. Dynamic pain threshold (DPT-level of the first painful roller) was determined. As golden standard, static pressure pain thresholds (PPTs) were assessed over temporalis muscle, C5/C6 zygapophyseal joint, second metacarpal and tibialis anterior.
Results
Side-to-side consistency between DPT (r = 0.843, P < 0.001) was observed. DPT was moderately associated with widespread PPTs (0.526 > r > 0.656, all P < 0.001).
Conclusion
DPT was associated with widespread pressure sensitivity supporting that dynamic pressure hyperalgesia within the trigeminal area is consistent with generalized pressure pain hyperalgesia. These results suggest that dynamic pressure algometry may be a valid tool for assessing dynamic mechanical pain sensitivity in TTH. Therefore, assessing both static and dynamic deep somatic tissue pain sensitivity may provide new opportunities for differentiated diagnostics and new tool for assessing treatment effects.
Disclosure of Interest
None Declared
Tension-Type Headache
PO-01-176
The use of Preventive Pharmacological Treatment is Associated with Local Pressure Pain Hyperalgesia in Tension Type Headache
María Palacios-Ceña1, Ángel Guerrero-Peral2, Marina Ruíz2,*, Elena Benito-González1, Lars Arendt-Nielsen3 and Cesar Fernandez-De-Las-Peñas1
1Fisioterapia, Terapia Ocupacional, Rehabilitación y Medicina Física, UNIVERSIDAD REY JUAN CARLOS, ALCORCON
2Headache Unit, Hospital Clínico de Valladolid, Valladolid, Spain
3Health Science and Technology, Aalborg University, Aalborg, Denmark
Objectives
To investigate the differences in clinical features and widespread pressure sensitivity according to the use of preventive medication in individuals with tension type headache (TTH).
Methods
Individuals with TTH diagnosed according to the International Classification of Headache Disorders (ICHD-III) criteria participated. Exclusion criteria included other primary headaches, medication overuse headache, whiplash, fibromyalgia or any neurological disorder. A 1-month headache diary was used to collect clinical data and preventive medication intake. Pressure pain thresholds (PPTs) over the temporalis, C5-C6 zygapophyseal joint, second metacarpal, and tibialis anterior were assessed.
Results
One hundred and forty-four (n = 144) patients (72% women; mean age: 45 ± 13 years; headache frequency: 16 ± 9 days per month; headache intensity: 6.1 ± 1.1; headache duration: 7.4 ± 4.3 hours/attack) participated. Fifty-nine (41%) reported use of preventive medication (62% amitriptyline). Patients taking preventive medication reported longer headache duration and higher headache frequency, but similar intensity, than those not taking medication (P < 0.001). Similarly, those patients taking preventive medication had lower PPT over the temporalis muscle and C5-C6 zygapophyseal joint (P < 0.05) than those patients not taking preventive medication. No significant differences in PPTs over the second metacarpal and tibialis anterior muscles were observed.
Conclusion
The current study found that preventive medication intake was related to worse headache frequency and duration and higher local pressure pain hypersensitivity in the trigemino-cervical area in patients with TTH. Future studies should investigate if the use of preventive medication intake is able to reduce sensitization mechanisms in TTH.
Disclosure of Interest
None Declared
Tension-Type Headache
PO-01-177
Comparison of clinical characteristics between chronic tension-type headache patients diagnosed by ICHD-3β original and stricter alternative criteria
Chun Pai Yang1, Jong-Ling Fuh2, Wei-Ta Chen2, Shih-Pin Chen2, Yen-Feng Wang2 and Shuu-Jiun Wang2,*
1Departments of Neurology, Kuang Tien General Hospital, Taichung
2Department of Neurology, Neurological Institute, Taipei Veterans General Hospital and National Yang-Ming University School of Medicine, Taipei, Taiwan, Republic of China
Objectives
The purpose of this study was to compare the clinical characteristics of chronic tension-type headache (CTTH) patients diagnosed by International Classification of Headache Disorders-3β (ICHD-3β) original criteria code 2.3 and stricter alternative criteria code A2.3.
Methods
Of the 12,920 outpatients in a headache clinic seen by neurologists from 2004 to 2016 in one tertiary teaching hospital in Taipei, Taiwan, 225 (1.7%) patients were diagnosed as CTTH. Among them, all patients fulfilled the ICHD-3β original criteria (ICHD-3β original group), whereas, only 67 (29.8%) fulfilled the stricter alternative criteria. In order to compare these two criteria, this field testing study compared these two groups of CTTH patients, i.e. those who did not fulfill stricter criteria (non-stricter group, n = 158) vs. those who fulfilled stricter criteria (stricter group). The comparisons included the following data if available: demographics, headache profiles, comorbidities, and a battery of rating scales including Hospital Anxiety and Depression Scale (HADS), Migraine Disability Assessment (MIDAS), Pittsburgh Sleep Quality Index (PSQI), and fibromyalgia (FM) questionnaires based on the modified 2010 American College of Rheumatology preliminary diagnostic criteria. Categorical data was performed by chi-square test and continuous data was performed by independent t-tests.
Results
Demographic data showed no difference between 2 groups except that the non-stricter group had a higher family history (1st degree relatives) of headache (49.7% vs. 28.8%, p = 0.005) than stricter group. In headache profiles, non-stricter group had higher intensity of the worst headache in the past year (6.8 ± 2.1 vs. 6.0 ± 2.3, p = 0.01), higher intensity of the average headache in the past year (5.4 ± 2.1 vs. 4.4 ± 1.9, p = 0.03), and higher frequency of posterior neck pain (43.9% vs. 25.4%, p = 0.01) than the stricter group. The non-stricter group had higher frequency of coffee or tea or coke drinking than the stricter group (45.8% vs. 27.3%, p = 0.04). Moreover, non-stricter group had higher HADS score (7.2 ± 6.1 vs. 5.4 ± 3.9, p = 0.01), higher wide spread pain index (2.8 ± 2.9 vs. 1.9 ± 2.0, p = 0.001), and higher symptom severity score (4.9 ± 2.6 vs. 3.9 ± 2.8, p = 0.02) than stricter group but not for the scores of the MIDAS or PSQI.
Conclusion
Our findings suggested that compared to ICHD-3β original criteria, CTTH patients identified by the stricter criteria appear to have less headache severity and comorbidities. Further study needs to identify this unique headache group.
Disclosure of Interest
None Declared