
Abstract
Background
Sleep disturbances are closely related to migraine. Nevertheless, information regarding the impact of short sleep duration and poor sleep quality on the clinical presentation of migraine at population level is limited.
Methods
This study was a nationwide population-based survey on adults aged 19–69 years. Headache frequency (attacks/month) and intensity (visual analogue scale, 0–10) were documented. Short sleep duration and poor sleep quality were defined as average sleep duration <6 h/day and Pittsburgh Sleep Quality Index score >5, respectively. The association of sleep parameters with headache frequency and intensity was analysed among migraineurs.
Results
Of 2695 participants, 143 (5.3%) had migraine. Headache frequency was significantly higher among migraineurs with short sleep duration (2.0 [1.0–12.0] vs. 1.0 [0.3–4.0], p = 0.048) and poor sleep quality (2.0 [0.6–4.7] vs. 1.0 [0.2–3.0], p = 0.009) than among those without. However, headache intensity was similar between migraineurs with short sleep duration and poor sleep quality. Multiple linear regression analyses revealed that short sleep duration was a significant contributing factor for headache frequency (β = 0.210, p = 0.015).
Conclusions
Self-reported short sleep duration (<6 h per day) is associated with an increased headache frequency among migraineurs in a population-based setting.
Introduction
Migraine and sleep disturbances are common conditions in the general population (1), and close associations between these two conditions have been reported in clinical and population-based studies (1–5). Both insufficient and excessive sleep are common triggers of migraine attacks (5). Furthermore, migraineurs have more sleep or sleep-related problems than non-migraineurs, such as insomnia, daytime sleepiness, sleep apnoea, and parasomnias (3,4). Moreover, sleep disturbances can increase the frequency and intensity of migraines (2).
Epidemiological studies have shown that sleep curtailment is common in the general population. Approximately 6–8% of adults in the general population sleep less than 6 h per night (6). Short sleep duration (less than 6 h within a 24 h period) is associated with an increased risk of cardiovascular disorders and psychiatric disease (7,8). In a clinic-based study, migraineurs with short sleep duration experienced more frequent and severe headaches than those with longer sleep duration (2).
As well as sleep duration, both sleep quality and quantity are related to health and wellbeing (9). Sleep studies among migraineurs have reported that sleep duration did not differ from that of non-migraineurs (10). Therefore, differences in sleep quality may explain why sleep disturbance is more common in migraineurs than in non-migraineurs. Indeed, poor sleep quality in migraineurs has been reported in a few clinical studies. These have consistently reported that migraineurs more frequently experience poor sleep quality than non-migraineurs (11,12). In addition, migraineurs with poor sleep quality had higher headache frequency and more frequent anxiety and depression symptoms than migraineurs without poor sleep quality (13). However, information regarding the prevalence and clinical impact of short sleep duration and poor sleep quality among migraineurs in a population-based setting is limited.
In this population-based study, we hypothesised that short sleep duration and poor sleep quality would increase the severity of headache attacks in migraineurs. To test this hypothesis, we analysed data from the Korean Headache–Sleep Study (KHSS), a nationwide, cross-sectional, and population-based survey on headache and sleep (14). We defined the prevalence of migraine, short sleep duration, and poor sleep quality, and assessed the effect of short sleep duration and poor sleep quality on the clinical presentation of headache among migraineurs.
Materials and methods
Survey
The KHSS included adults aged 19–69 years; the survey is described elsewhere in detail (14). Briefly, we adopted a two-stage clustered random sampling, which was proportional to the population distribution of Korea, except for Jeju island. To minimise interest bias, we informed candidates that the survey topic was “social health” rather than “headache and sleep”. All interviewers were employees of Gallup Korea, a multinational social research company. The survey was conducted by door-to-door visits and face-to-face interviews, using a structured questionnaire, between November 2011 and January 2012. The questionnaire was designed to identify headache type, sleep duration and quality, anxiety, depression, and insomnia. The study protocol was approved by the institutional review board/ethics committee of Hallym University Sacred Heart Hospital in Korea; written informed consent was obtained from all participants.
Assessment of migraine
Among participants who experienced headache during the previous year, we defined migraineurs according to the diagnostic criteria (a) to (d) for migraine without aura of the third edition beta version of the International Classification of Headache Disorders (ICHD), as follows: (a) five or more attacks in a lifetime; (b) attack duration of 4–72 h; (c) any two of the four typical headache characteristics (i.e. unilateral pain, pulsating quality, moderate-to-severe pain intensity, and aggravation by routine physical activity); and (d) attacks associated with at least one of the following: nausea, vomiting, or both photophobia and phonophobia (15).
The questionnaire used in the present study was found to have 75.0% sensitivity and 88.2% specificity when compared with physicians’ diagnosis (16). We did not define the type of migraine (migraine with or without aura) because it is difficult to assess this accurately using only a questionnaire (15). Clinical presentation of migraine was determined in terms of the frequency, intensity, and impact of the headache. To assess the intensity and impact of headache, we used visual analogue scale (VAS) and the Headache Impact Test-6 (HIT-6) scores. If a participant responded positively to the question, “In the past year, have you had at least one headache lasting more than 1 min?”, and was not diagnosed as having migraine, she or he was diagnosed as having non-migraine headaches.
Sleep duration and poor sleep quality
Participants were asked to report their usual sleep duration in terms of hours and minutes, separately for workdays and free days, during the past month. The average sleep duration was a weighted mean of the sleep duration on workdays and free days, calculated as [(workday sleep duration × 5) + (free day sleep duration × 2)]/7. Short sleep duration was defined as an average sleep duration of <6 h.
We assessed sleep quality using the Pittsburgh Sleep Quality Index (PSQI). If a participant’s total PSQI score was >5, she/he was classified as having poor sleep quality (17). We also calculated component scores of PSQI according to the guidelines, including subjective sleep quality, sleep latency, sleep duration, habitual sleep insufficiency, sleep disturbance, use of sleep medications, and daytime dysfunction (17).
Anxiety, depression, and insomnia symptoms
We used the Goldberg Anxiety Scale to investigate anxiety, which comprises four screening items and five supplementary items (18,19). Individuals who answered affirmatively for more than two items in the screening item and more than five items in the entire scale were identified as having anxiety. The Korean version of the scale has 82.0% sensitivity and 94.4% specificity for diagnosing anxiety (19) and correlates well with the State–Trait Anxiety Inventory, a validated tool for assessing anxiety (20).
For evaluating depression, the Patient Health Questionnaire-9 (PHQ-9) was applied. Participants who had scores of ≥10 were considered to have depression. The Korean version of the PHQ-9 has 81.1% sensitivity and 89.9% specificity (20).
We used the Insomnia Severity Index (ISI) to diagnose and classify insomnia symptoms (21). The ISI is composed of seven items that evaluate various aspects of insomnia. Individuals with an ISI score of ≥15.5 were classified as having significant insomnia symptoms.
Statistical analysis
For group comparisons among the no-headache, migraine, and non-migraine headache groups, we utilised the Student’s t-test or one-way analysis of variance for continuous variables, after confirming the normality of distribution using the Kolmogorov–Smirnov test. If the distribution was not normal, the Mann–Whitney U or Kruskal–Wallis tests were adopted. Chi-square tests were performed for categorical variables. We compared the headache frequency per month, the VAS, and HIT-6 scores between migraineurs with and without short sleep duration using the Mann–Whitney U test.
For assessing the contribution of short sleep duration and poor sleep quality to the frequency of headache, a multiple linear regression analysis that included short sleep duration, poor sleep quality, sociodemographic variables (age, sex, size of residential areas, and education level), insomnia symptoms (ISI score), anxiety (GAS score), and depression (PHQ-9 score), was performed. The significance level was set at p < 0.05 (two-tailed). The data were analysed using the Statistical Package for the Social Sciences 22.0 (SPSS 22.0; IBM, Armonk, NY, USA).
The 2695 participants responded properly to most of the items via a face-to-face interview. Nevertheless, non-responses occurred for some variables. In our study, we did not replace missing data with substituted values or delete data with missing values. Although this approach produces slightly larger standard errors in finite samples, the impact is minimised in large samples such as ours (14).
Results
Survey
Interviewers approached 7430 individuals, of whom 3114 agreed to participate (rejection rate: 58.1%); a total of 419 suspended participation during the interview, and thus 2695 subjects completed the survey (cooperation rate: 36.3%, Figure 1). There were no significant differences in the distribution of age, sex, size of residential area, and educational level between survey participants and the Korean general population (Table 1).
Flowchart depicting the participation of subjects in the Korean Headache-Sleep Study. Sociodemographic characteristics of survey participants, the total Korean population, and cases identified as having migraine, average sleep duration, and poor sleep quality. n: number; CI: confidence interval; SD: standard deviation; PSQI: Pittsburgh Sleep Quality Index. Variables are presented as number (%) or number (%) (95% confidence interval) and mean ± SD. Compared with gender, age group, size of residential area, and education level between the sample of the present study and the total population of Korea.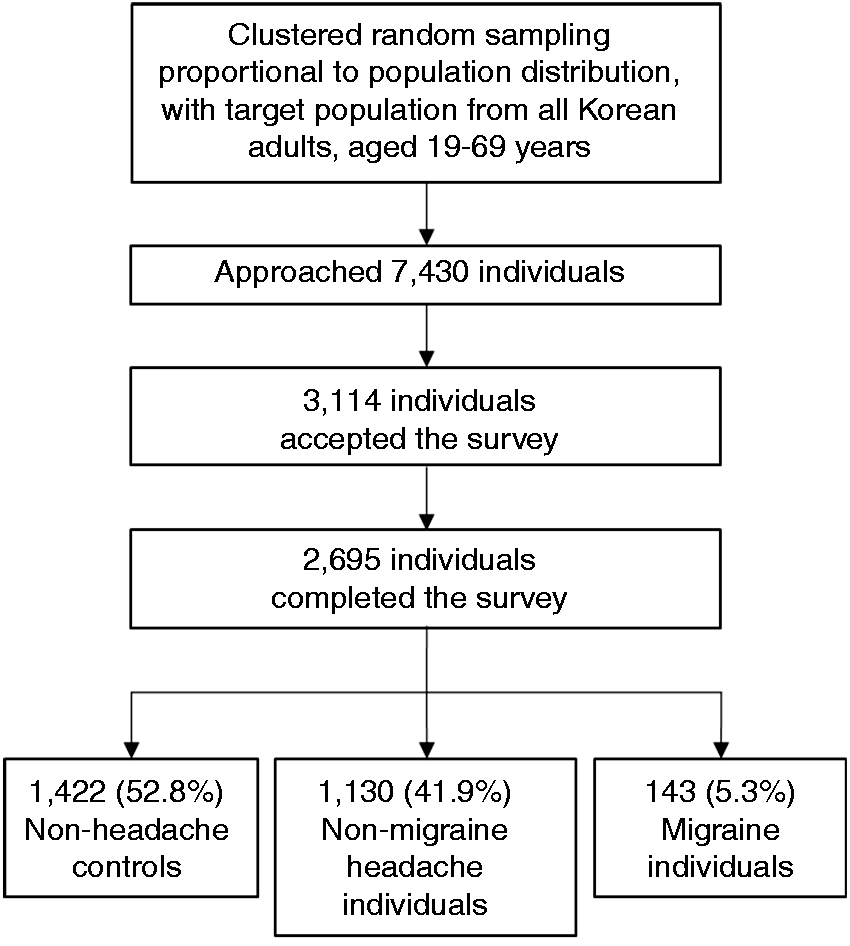

Prevalence and clinical characteristics of migraine
Of the 2695 participants, 1299 (47.2%) had had at least one headache attack during the previous year, and 143 (5.3%) were classified as having migraine. The remaining 1130 (41.9%) were classified as having non-migraine headache. The one-year migraine prevalence was highest in the 30–39 age group (7.0%). The mean headache frequency per month, the VAS score for headache intensity, and the HIT-6 score were 3.8 ± 6.3, 6.2 ± 1.9, and 54.3 ± 9.3, respectively.
Sleep duration and prevalence of short sleep duration
The mean sleep duration of all participants was 7.4 ± 1.3 h; 277 (10.3%) participants were classified as having short sleep duration. Of the 143 migraineurs, 17 (11.8%) had short sleep duration. Among the non-headache, non-migraine headache, and migraine group, sleep duration (7.3 ± 1.2 vs. 7.2 ± 1.2 vs. 7.3 ± 1.4, p = 0.207) as well as the prevalence of short sleep duration (9.2% vs. 11.4% vs. 11.2%, p = 0.154) were not significantly different. Sleep duration was negatively correlated with age (Pearson’s r = −0.151, p < 0.001), but did not differ according to sex, size of residential area, or educational level (Table 1).
Sleep quality and prevalence of poor sleep quality
In all included participants, 715 (26.5%) reported PSQI scores in excess of 5 and were classified as having poor sleep quality (Table 1). Among the 143 migraineurs, 68 (47.6%) were classified as having poor sleep quality. The prevalence of poor sleep quality was significantly higher in the migraine group compared with those of non-migraine headache and non-headache groups (47.6% vs. 30.9% vs. 21.0%, p < 0.001).
Total and component PSQI score according to headache diagnosis
Comparison of total and component score of Pittsburgh Sleep Quality Index score among study population.
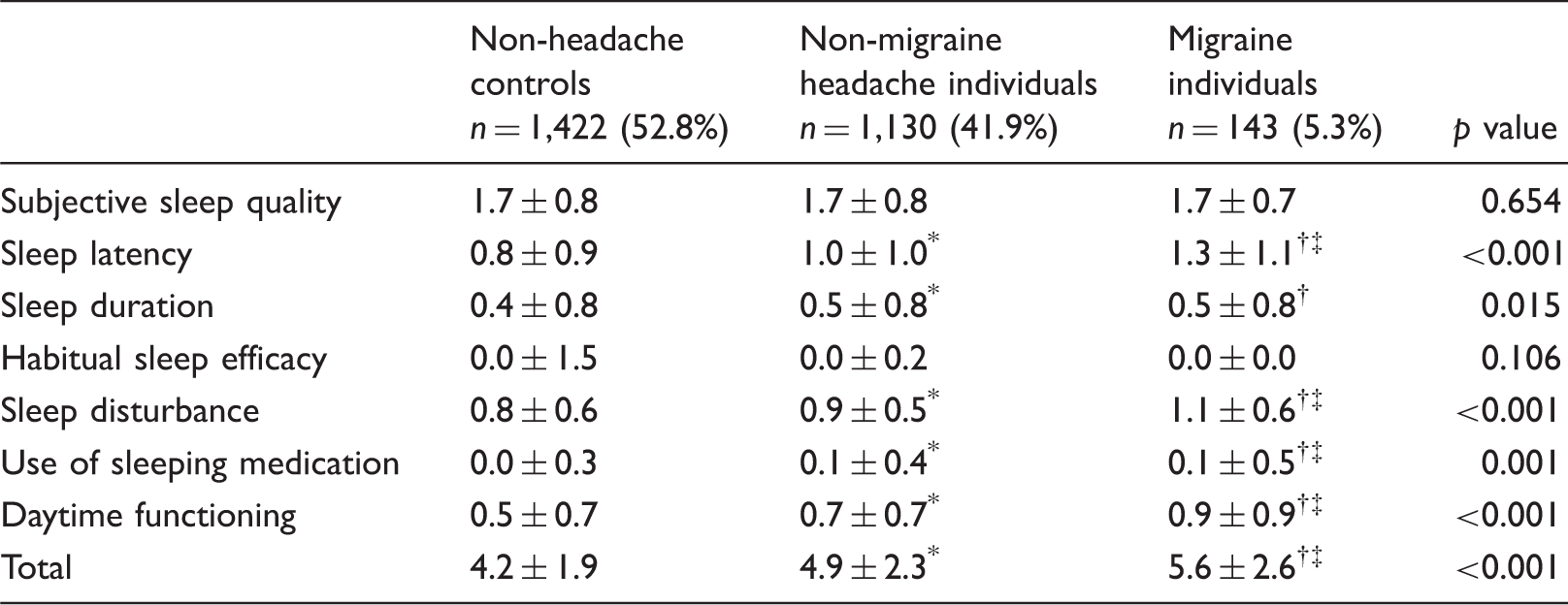
Data is presented as mean ± SD.
Each component scores of Pittsburgh Sleep Quality Index have a range of 0 – 3 points. Higher Pittsburgh Sleep Quality Index score indicates more severe difficulty.
p <0.05 compared non-headache controls with non-migraine headache individuals by Bonferroni’s post-hoc analysis.
p <0.05 compared non-headache controls with migraine individuals by Bonferroni’s post-hoc analysis.
p <0.05 compared non-migraine headache individuals with migraine individuals by Bonferroni’s post-hoc analysis.
Prevalence of anxiety, depression, and insomnia symptoms
Anxiety, depression, and insomnia were present in 268 (10.0%), 116 (4.3%), and 442 (16.4%) participants, respectively. The prevalence of anxiety (30.1% vs. 13.2% vs. 5.3%, p < 0.001), depression (16.8% vs. 5.9% vs. 1.8%, p < 0.001), and insomnia symptoms (37.8% vs. 22.7% vs. 9.2%, p < 0.001) was significantly higher in the migraine group compared to the non-migraine headache and non-headache groups.
Association of short sleep duration, poor sleep quality, and migraine severity
Headache frequency, visual analogue scale score for headache intensity, and Headache Impact Test-6 score of migraineurs, based on sleep duration and sleep quality.

Variables are presented as median (interquartile range).
Analysis of contributing factors for headache frequency among migraineurs
Analysis of contributing factors for headache frequency per one month among migraineurs (n = 143).

SE: Standard error, VIF: variation inflation factor.
Results of multiple linear regression analysis that included sociodemographic variables (age, sex, size of residential areas, and education level), short sleep duration (average sleep duration <6 hours per day), poor sleep quality (Pittsburgh Sleep Quality Index [PSQI] > 5) anxiety (Goldberg Anxiety Scale [GAS] ≥ 5), depression (Patient Health Questionnaire [PHQ]-9 ≥ 10) and insomnia symptom (insomnia severity index [ISI] > 15.5), with headache frequency set as dependent variable.
R2 = 0.194, adjusted R2 = 0.139.
Association of short sleep duration, poor sleep quality, and non-migraine headache severity
Within the non-migraine headache group, headache frequency per month (median, interquartile range [IQR] (short sleep duration: 1.0 [0.3–2.0], vs. longer sleep duration: 0.5 [0.3–2.0], p = 0.018), the VAS score for headache intensity (5.0 [3.0–6.0] vs. 5.0 [3.0–6.0], p = 0.019), and HIT-6 score (44.0 [40.0–52.0] vs. 43.0 [40.0–49.0], p = 0.008) were significantly higher in those with a short sleep duration. Poor sleep quality was associated with higher headache frequency per month (1.0 [0.3–3.0] vs. 0.4 [0.2–2.0], p < 0.001), VAS score for headache intensity (5.0 [4.0–6.0] vs. 5.0 [3.0–6.0], p < 0.001), and HIT-6 score (46.0 [42.0–53.5] vs. 42.0 [40.0–48.0], p < 0.001) compared with those without poor sleep quality.
Discussion
We conducted a population-based study to evaluate the impact of short sleep duration and poor sleep quality on the clinical presentation of headache among migraineurs. This study showed that the prevalence of migraine, short sleep duration, and poor sleep quality were 5.3%, 10.3%, and 26.5%, respectively, in a Korean general population sample. The average sleep duration and the prevalence of short sleep duration were not significantly different among the migraine, non-migraine headache, and non-headache groups. In contrast, the prevalence of poor sleep quality among migraineurs was significantly higher than among individuals in the non-headache and non-migraine groups. Furthermore, short sleep duration and poor sleep quality were significantly associated with increased headache frequency among migraineurs.
In European and USA population-based studies, poor sleep has also been associated with the presence of migraine (22,23). However, these studies did not show a relationship between sleep duration and headache frequency, and did not consider these together with the presence of psychological symptoms, including insomnia. Our results agree with a previous clinical-based study, which showed that those who slept for shorter durations had more frequent headaches than individuals who slept longer (2).
We assessed sleep duration, sleep quality, and insomnia using a questionnaire rather than objective assessments using devices such as polysomnography or actigraphy. Nevertheless, subjective and objective assessment for sleep duration showed good agreement with a previous study (24). PSQI and ISI scores were previously validated by comparing clinically definitive cases, and have been widely used in clinical and epidemiological studies (21,25). Objective assessment of sleep parameters in epidemiological studies is difficult owing to cost, accessibility to participants, and maintaining measuring devices, et al. Therefore, we assessed sleep duration and other sleep parameters using a questionnaire. Thus, further studies using actigraphy or polysomnography are needed to confirm the relationship between sleep duration and migraine severity in the general population.
The exact mechanism for the association between short sleep duration and increased headache frequency among migraineurs remains unclear. One possible mechanism is brain hyperexcitability. For instance, one previous study demonstrated that sleep deprivation was associated with increased brain hyperexcitability (26). Indeed, migraineurs showed higher brain excitability than individuals in the non-headache group (27). Therefore, short sleep duration may increase headache frequency by inducing brain excitability.
Another possible explanation is that the opioid system is disturbed by short sleep duration. Sleep deprivation may result in a hyperalgesic state by inhibiting opioid protein synthesis, which may increase headache frequency in migraineurs (28). Additionally, thalamic trigeminovascular neurons and the orexinergic neuronal pathway may play a role in the association between short sleep duration and exacerbation of migraine symptoms; thalamic trigeminovascular neurons play a role in the generation of headache during a migraine attack. They are regulated by a variety of neurotransmitters, some of which have relevance to sleep (29). Furthermore, orexin is a neuronal substance that is implicated in both migraine and sleep (30).
We defined short sleep durations as less than 6 h per day. Numerous population-based studies have shown that less than 6 h of sleep is significantly associated with pathological conditions, such as diabetes, obesity, and depression (31,32). In pain disorders, less than 6 h was prospectively linked with an increased next-day pain experience (33). Based on these previous studies, our study defined short sleep duration as less than 6 h per day.
In our study, short sleep duration was present in 10.3% of the study population. This proportion was somewhat higher than that noted in previous studies (7.8% in the USA (6) and 7.0% in China (34)). One possible explanation for this discrepancy may involve the method for measuring sleep duration. Most studies assessing sleep duration asked individuals about their average sleep duration without separating workdays and free days, and using 1 h intervals. In our study, we evaluated the typical sleep duration for workdays and free days separately, using both hours and minutes, and then calculated the average sleep duration. Considering the definition of our study, participants with an average sleep duration of 5 h 50 min might be classified as having short sleep duration, but this group might not be classified as having short sleep duration in other studies. If we set the cut-off point for short sleep duration to 5 h 30 min, with rounding off, the prevalence of short sleep duration in the present study was 7.7%, which was similar to previous studies.
Poor sleep quality is a frequent complaint among individuals with headache, especially migraineurs. Karthik et al. reported that 60% of 90 patients with migraine without aura had poor sleep quality, which was significantly higher than non-migraineurs (11). Another clinical study in Austria showed that the PSQI score of migraineurs was positively correlated with headache frequency (12). In our study, approximately half of the migraineurs experienced poor sleep quality. Therefore, our study confirms that poor sleep quality is a common problem in migraineurs.
Among the components of PSQI, the component scores of sleep latency, sleep duration, sleep disturbance, use of sleeping medication, and daytime functioning were significantly higher (i.e. worse) in migraineurs compared to individuals in the non-migraine headache or non-headache group. One interesting finding is that the component score of subjective poor sleep quality was not different among the three groups, which implies that migraineurs and individuals with headache did not report poor sleep quality, despite having various components of poor sleep quality. This indicates that a detailed assessment of sleep quality may be needed in patients with migraine, regardless of their self-reports.
The subcomponent score for sleep duration of PSQI of individuals in the non-headache group was shorter than that those with non-migraine headache and migraine in the present study. Sleep duration of individuals with non-migraine headache and migraine did not significantly differ. These findings contrast with our findings of no significant between-group difference in sleep duration based on average sleep duration. This discrepancy may be attributable to the scoring method of sleep duration in the PSQI. Namely, the subcomponent of PSQI scores sleep duration as >7 h = 0, 6–7 h = 1, 5–6 h = 2, and <5 h = 3 rather than in terms of hours and minutes.
Poor sleep quality is frequently noted in various study populations. At a primary care clinic based study in Africa, 68.7% of participants had poor sleep quality (35). Another study performed with Japanese white-collar workers showed a not infrequent (30–45%) prevalence of poor sleep quality (36). In Korea, a cross-sectional study of 1,406 young women (aged 18 to 40 years), who reported no clinically significant depression symptoms, revealed 22% of the total study population had a PSQI score of >5 (37). The similarity in the prevalence of poor sleep quality between the present study and these previous studies suggests that our study properly investigated poor sleep quality.
In the present study, headache frequency was higher in migraineurs with poor sleep quality than in those without poor sleep quality, even though we performed a univariate analysis. This finding is similar to previous clinical studies. For instance, high headache frequency correlated with poor sleep quality among migraineurs in an outpatient headache clinical study in China (13). Another case-controlled study in Austria revealed a positive association between headache frequency and poor sleep quality (12). The present and previous studies regarding the association between headache frequency and poor sleep quality were cross-sectional studies, and a causal relationship cannot, therefore, be confirmed. Further longitudinal studies are thus needed to confirm the exact relationship between these two conditions.
There are several limitations to the present study. First, although our study was conducted based on a survey of the general population and used a two-stage clustered random sampling with a low sampling error to represent the characteristics of the population, the small sample size of individuals with headache may have limited the subgroup analysis according to sociodemographics, longer sleep duration and accompanying insomnia, anxiety, or depression. Second, we did not investigate caffeine consumption and medications used. Caffeine overuse may not only negatively affect sleep duration but also increase headache frequency (38), and some medications have positive effects both for sleep duration and headache frequency of migraine such as antidepressants (39). Third, the overall response rate in the present study was not high. However, we used a two-stage clustered random sampling, proportional to the population distribution of Korea. Therefore, the distribution of age, sex, size of residential area, and educational level of our participants was not different from those of the Korean general population. In addition, the prevalence of migraine, anxiety, depression, and short sleep duration in the KHSS were similar to that of previous studies (14,40). Therefore, we could assure that we successfully investigated migraine and short sleep duration in the present study.
In conclusion, our study revealed important information about the prevalence of sleep duration, sleep quality, insomnia symptoms, anxiety, depression, and migraine characteristics in the general population. We simultaneously analysed insomnia symptoms, anxiety, and depression, which are closely associated with both sleep and migraine in the general population, using validated instruments such as the PHQ-9, GAS, and ISI. We found that short sleep duration (<6 h per day) is independently associated with an increased headache frequency among migraineurs. Further studies using objective methods to measure the duration and quality of sleep are necessary to assess the interaction of sleep and headache disorders, including migraine, in more detail.
Clinical implications
Although migraineurs had more sleep disturbances than non-migraineurs, average sleep duration and prevalence of short sleep duration were not significantly different among individuals with migraine, non-migraine headache and non-headache. In contrast, the prevalence of poor sleep quality was significantly higher in migraine participants compared with those of non-migraine headache and non-headache. Headache frequency per month was significantly higher in migraineurs with short sleep duration (average sleep duration <6 h) and poor sleep quality (total Pittsburgh Sleep Quality Index (PSQI) >5) than in those with relatively longer sleep duration (average sleep duration ≥6 h) and those without poor sleep quality (total PSQI ≤5). Visual Analogue Scale for headache intensity was not significantly different according to short sleep duration and poor sleep quality. Short sleep duration is an independent factor making a positive contribution to headache frequency after adjusting confounding factors. Our findings suggest that modulation of short sleep duration may be needed for better management of migraine.
Footnotes
Acknowledgements
The authors would like to thank Gallup Korea for providing technical support for the Korean Headache Survey.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a 2011-Grant from Korean Academy of Medical Sciences. This research was supported by grants of Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (2015R1D1A1A01057934).