
Abstract
Background
Familial hemiplegic migraine (FHM) is a rare, genetic form of migraine with aura. The severity of the aura imposes an effective prophylaxis that is currently based on standard anti-migraine drugs. To this concern, only short-term reports are currently available.
Methods
Eight patients from a multigenerational FHM type 1 family harbouring a T666M mutation in the CACNA1A gene were referred to our ataxia outpatient clinic. Medical history, general and neurological examination as well as therapeutic approaches were recorded regularly on a routine basis for an average period of 13 years (range 9–15 years). Brain imaging studies and EEG data were also collected.
Results
Our long-term follow-up revealed that ictal manifestations, which usually improve after the adolescence, may reoccur later in the adulthood. Permanent neurological signs as assessed by means of clinical evaluation as well as follow-up MRIs, EEGs and neuropsychological testing remained stable. Interval therapy with non-selective calcium antagonists reduced the burden of migraine attacks and was well tolerated in the long term.
Keywords
Introduction
Familial hemiplegic migraine (FHM) is a rare, genetic form of migraine with aura (1). FHM is characterised by the presence of motor symptoms during the aura in addition to the classical visual, sensory and dysphasic manifestations (1). Moreover, patients may experience severe attacks accompanied by drowsiness and coma. Full recovery after the attacks is usually achieved within hours to days. Later in the disease course a cerebellar syndrome may develop, which is believed to be independent from the severity of ictal manifestations (2).
FHM is inherited in an autosomal dominant manner associated with disease-causing mutations in three different genes (FHM1–3). FHM1 is the most frequent subtype caused by mutations in the CACNA1A gene, which encodes the pore-forming α1 subunit of the P/Q-type voltage-gated calcium channel (2). Mutations within this gene result in an enhanced channel activation and increased neurotransmitter release. More than 25 pathogenic mutations have been identified with T666M being the most frequent one (3).
Therapeutic management of FHM is based on classic migraine therapy (4), distinguishing treatment of acute attacks with common analgesics from prophylaxis of relapses. For the latter, current evidence supports the use of valproate, lamotrigine, verapamil, flunarizine and acetazolamide (for a recent review see (5)). To date, neither controlled trials nor reports on long-term observations on efficacy and side effects of FHM treatment are available.
Herein we describe the clinical course and treatment approaches in eight patients from a FHM1 family harbouring a T666M mutation with a follow-up of up to 15 years. The outcomes are discussed in light of current knowledge about FHM treatment.
Patients and Methods
The index patient was initially referred to the neurology outpatient clinic of the Medical University Innsbruck in 2001. Thereafter, seven more family members from three successive generations were examined (see Figure 1) and consecutively diagnosed with FHM1. All patients or their legal guardians gave written informed consent for genetic testing and bore a T666M mutation (gene variant c.1997C>T) on the CACNA1A gene. Investigations and assessments were conducted in accordance with the Declaration of Helsinki on ethical principles for medical research involving human participants.
The FHM1 pedigree with its four generations is illustrated. Black squares and black circles represent affected male and female patients, respectively. Diagonal line: deceased patient.
Seven patients were regularly followed up over an average period of 13 years (range 9–15 years). Baseline data are available for the eighth member who was recently diagnosed with FHM1. Regular clinical evaluations included detailed case history as well as general and neurological examination.
Six-monthly outpatient visits were performed. Assessment included frequency and severity of migraine attacks. Migraine attacks were defined as attacks with/without aura following the consensus definition (6). Severe attacks were defined by focal neurological symptoms with disturbance of consciousness like drowsiness or coma. Cerebellar signs were rated following the ‘Scale for the Assessment and Rating of Ataxia’ (SARA), a validated neurological scale with a score in the range of 0–40 points (7,8).
Seven patients underwent cerebral magnetic resonance imaging (MRI) on a 1.5 T whole-body scanner (Magnetom Avanto, Siemens Erlangen, Germany) at referral. Follow-up MRIs were performed in six patients. Functional brain imaging with Tc99m-Neurolite single-photon emission computed tomography was performed in one patient during an attack. Repetitive routine EEGs were performed in six patients. Baseline and follow-up neuropsychological assessments were performed in six patients as reported elsewhere (9).
Results
Patient I-1
The index patient (I-1) suffered from vertigo attacks since his early 40s. Triggered by a cerebral angiography, which was performed during diagnostic workup, he experienced a severe attack with hemiplegia, dysarthria and a 24-h coma at the age of 42 years. Similar attacks occurred over the following years, lacking an accurate diagnosis. Raising the suspicion of vascular events due to symptomatic carotid artery stenosis, surgery was performed.
Final diagnosis was made at the age of 71 years. He remembered 26 severe attacks with coma, postictal headache and reversible paresis, lasting from hours to days. Migraine attacks in his youth may have been present, but detailed disease history was not available. Neurological examination revealed horizontal and vertical gaze nystagmus, mild dysmetria and gait ataxia. MRI showed leukoencephalopathy due to known vascular risk factors and mild cerebellar atrophy. EEG demonstrated left temporal slowing.
Treatment and follow-up
At initial referral, he experienced a disease exacerbation with approximately five attacks/year. Flunarizine 5 mg daily was added to an ongoing treatment with 1000 mg valproate. No more severe attacks were reported within the next six years. After another severe migraine attack, treatment dosage was increased to valproate 2000 mg and flunarizine 10 mg daily. Thereafter, the patient remained free from disabling migraine attacks.
During follow-up, mild dementia (for detailed information see (9)) and a parkinsonian syndrome were diagnosed. Dopamine transporter imaging revealed a denervation pattern compatible with idiopathic Parkinson’s disease. The patient died at the age of 83 years.
Patient II-2
The first son of the index patient has had migraine since the age of five years. Some of his migraine attacks were accompanied by hemiparesis, aphasia and severe vertigo lasting for hours. Until the age of 15 years he remembers five severe attacks, followed by a free interval until the age of 42 years. From then on, he suffered about monthly severe attacks with loss of consciousness and severe vertigo. Urticaria and hypertensive crises often accompanied the migraine attacks. In the intervals, he suffers from a cerebellar syndrome with dysarthria, down-beat nystagmus, dysmetria and gait ataxia. Routine EEG in between the attacks revealed bilateral temporal intermittent slow activity (Figure 2). MRI shows atrophy of vermis cerebelli.
Patient II-2, 47 years old. Bipolar longitudinal montage. Intermittent bitemporal Theta.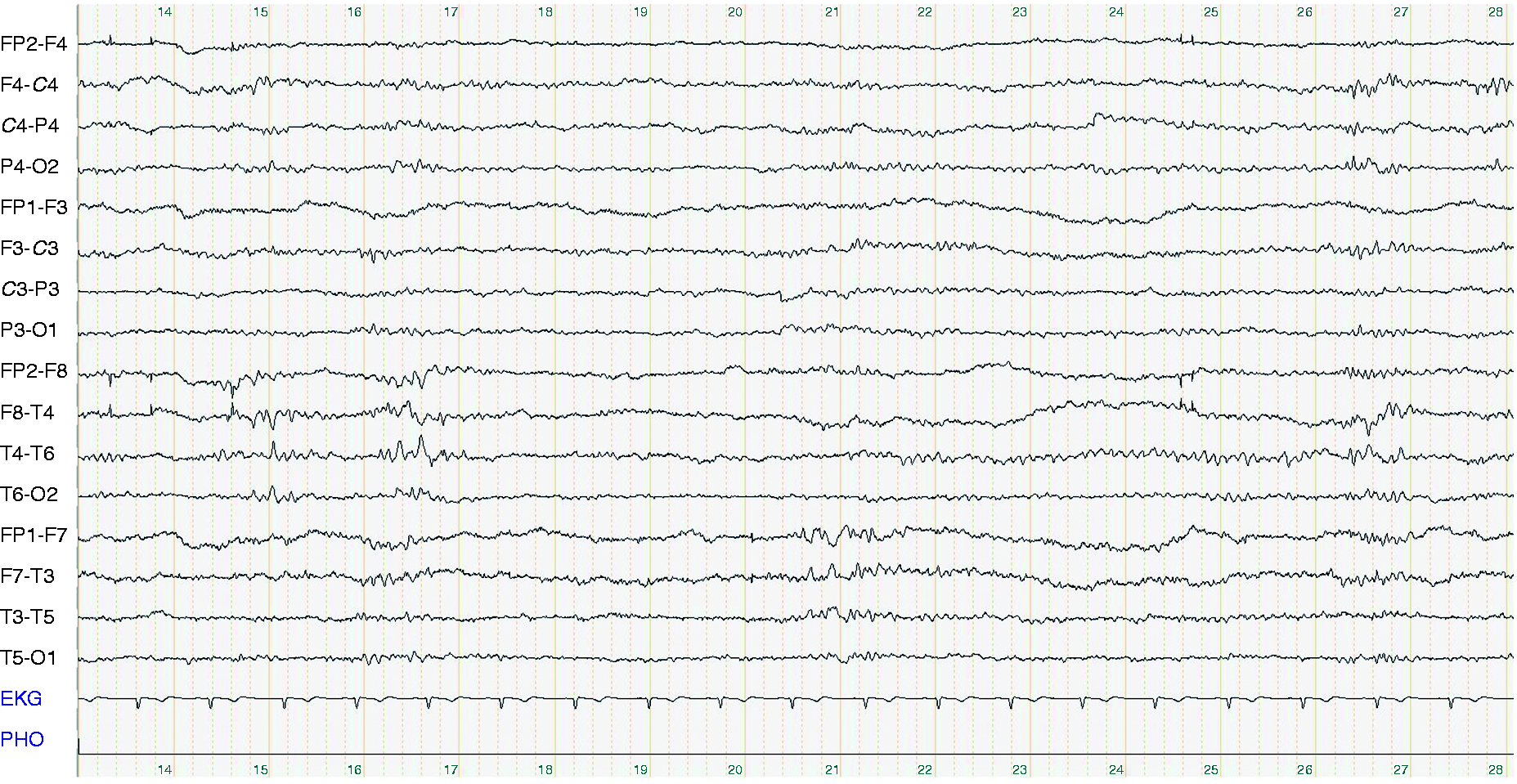
Treatment and follow-up
At the age of 47 years, acetazolamide was started but was soon terminated because of lack of benefit. Flunarizine 5 mg daily was then effective in preventing severe attacks. Abortive aura without impairment of consciousness or headache occurred once a month. Five years later, a disease exacerbation was followed by a dosage increase of flunarizine to 10 mg. Thereafter an attack-free interval occurred until the age of 57 years. Thus, prophylaxis was optimised adding metoprolol 50 mg in the light of elevated blood pressure and attack associated vegetative instability. Since then only occasional and mild attacks have been reported. Follow-up EEGs and MRIs showed no substantial changes.
Patient II-3
The second son of the index patient had his first symptoms at the age of 13 years. Until 17 years of age, he experienced three migraine attacks with motor, sensory and dysphasic aura, which lasted for hours. Mild head trauma triggered attacks. From the age of 30 years on, he developed progressive gait ataxia and dysarthria. At the first referral, he reported of migraine attacks (one or two episodes per month) without aura. Neurological examination at the age 40 years revealed a cerebellar syndrome with prominent downbeat nystagmus. MRI showed diffuse cerebellar atrophy. EEG showed phases with intermittent slowing.
Treatment and follow-up
The initial treatment with acetazolamide was stopped after a few weeks because of side effects (paraesthesia and dizziness). Flunarizine 5 mg daily was then started and showed benefit on the headache symptoms. The dose was increased to 10 mg and maintained to date. A temporary cessation of this therapy was accompanied by a substantial increase in headache frequency. One hemiplegic attack was recently reported (at 52 years). Consecutive MRI and EEG controls showed no significant dynamics.
Patient III-4
The first daughter of patient II-2 was first seen at our clinic at the age of 23 years. She reported hemiplegic attacks without impaired consciousness since her late first decade. Clinically, she had intermittent down-beat nystagmus and very mild limb dysmetria. MRI showed minimal cerebellar atrophy. Attacks with motor symptoms suspended at the age of 21 years, while migraine without aura still occur frequently.
Patient III-5
The second daughter of patient II-2 had a delayed motor development. She learned to sit by herself at the age of three years. After intensive physiotherapy, she was able to walk at about seven years of age. Cognition and intellect were unimpaired. At the first neurological examination (age 20 years), she had cerebellar ataxia with down-beat nystagmus and dysarthria, as well as mild dystonia in both upper limbs. MRI showed severe cerebellar atrophy while other brain areas were unremarkable. She never suffered from hemiplegic episodes, but had attacks with headache, vertigo and worsening of ataxia.
Treatment and follow-up
A prophylactic therapy with flunarizine 10 mg daily was prescribed and showed benefit on both vertigo and headache. After improvement of ictal manifestations in her early 20s, prophylactic treatment was stopped. SARA score at 30 years old was stable with 13 out of 40 points. MRI follow-up after ten years showed no progression of cerebellar atrophy.
Patient III-6
The first son of patient II-3 has been suffering from vertigo attacks since his early childhood. At first examination, at the age of 18 years, he reported frequent episodes of migraine without aura (four times per month). The patient was unable to report on severe attacks with hemiplegia, raising the suspicion of impaired memory for severe attacks. His mother, however, reported a first transient tetraparesis after falling down the stairs at four years of age. Clinically, he had prominent gaze nystagmus and perioral myokymia, as well as mild gait ataxia. EEG showed phases of reduced vigilance. MRI demonstrated mild cerebellar atrophy.
Treatment and follow-up
Flunarizine 5 mg daily reduced the frequency of migraine episodes. Under therapy, a severe attack with right side hemiplegia, anarthria, severe disturbance of consciousness and massive autonomic derangement occurred. Severe non-treatable supraventricular tachycardia occurred, together with fever of unknown origin and massive sweating. Verapamil was acutely administrated without benefit. A cerebral SPECT during the attack revealed pathological lateralisation of the cerebral blood flow without correlates in the MRI (see Figure 3). Ictal EEG was abnormal with continuous left hemispheric slowing (Figure 4). Clinically, the patient recovered slowly over several weeks. Flunarizine was later substituted with topiramate 100 mg daily because of weight increase. Under topiramate, the patient experienced another severe migraine attack, but at that time symptoms improved after acute administration of verapamil. Topiramate prophylaxis is currently ongoing. The patient is 31 years old and reported no more disabling attacks
SPECT and MR brain imaging of patient III-7 during an attack. (a) Reduced perfusion in the left frontal, left parietal lobes and in the left basal ganglia. (b) Reduced blood flow in right cerebellum. (c, d) T2-weighted and (e, f) diffusion-weighted scans showed no ischemic alterations in cerebral and cerebellar parenchyma. See text and Figure 4 for correspondent EEG findings. Patient III-6, 23 years old. Bipolar longitudinal montage. Continuous left hemispheric Delta–Theta slowing.

Patient III-7
The second son of patient II-3 has been having classical hemiplegic migraine since the age of seven years. Aura consists of motor, sensory and dysphasic manifestation and can last from hours to two days. Severe attacks were also reported. Trauma and emotional stress were pointed out as triggers. Except for nystagmus, he was clinically unremarkable. EEG showed intermittent diffuse slowing. MRI revealed mild vermis atrophy.
Treatment and follow-up
Flunarizine 5 mg daily was started and reduced both severity and frequency of attacks. After an attack-free interval of 1.5 years, the patient quitted prophylaxis at the age of 16 years.
In the subsequent controls, he reported weekly migraine without aura, treated with common analgesics.
No further hemiplegic episodes occurred until to date. Regular neurological evaluations revealed stable mild ataxia.
Patient IV-8
The daughter of patient III-4 was referred to our outpatient clinic when she was just 21 months old. Her mother reported a delayed motor development with first walking attempts at 18 months of age. Additionally, episodes of drowsiness with walking difficulties leading to falls and intermittent cervical dystonia were present. The mother had the impression that the child suffers from headache during these episodes. Episodes lasted in the range of 1–3 days and were followed by increased sleepiness. General and neurological examination as well as EEG were unremarkable.
Discussion
Assessment of the clinical course and treatment response in a multigenerational FHM1 family in our long-term observational study revealed: (i) after childhood onset of migraine with aura, symptoms remitted in adolescence and eventually recurred later in adulthood; (ii) early onset ataxia remained stable during follow-up; and (iii) interval treatment using non-selective Ca2+ channel blocker was well tolerated and efficacious in most patients with FHM1.
Migraine attacks were present in early childhood in all patients of our T666M cohort besides the index patient I-1. At first evaluation at the age of 71 years, he could not remember any obvious migraine attacks, which also may be explained by a recall bias. This has been reported earlier in sporadic hemiplegic migraine (10), where patients forgot having had hemiplegic attacks at a younger age. In patient IV-8, attacks with vertigo and neck dystonia occurred as early as 21 months. Six out of eight patients reported an improvement in frequency and severity of attacks in adulthood. This has been previously observed by Ducros et al. in several families (2). In addition, we found a reoccurrence of migraine with prolonged aura in three patients in adulthood, suggesting a ‘biphasic’ course of migraine in our cohort (Figure 5). To date, longitudinal data in FHM1 are lacking, therefore a biphasic disease course might have been overlooked. The peculiarity of FHM1 manifestations offers a considerable challenge in diagnostic allocation. In the absence of a precise diagnosis a sudden onset of transient neurological deficits raises the suspicion for vascular events or epilepsy. Indeed, our index case underwent an extensive work-up to address these preliminary diagnostic hypotheses including surgery for intended symptomatic carotid artery stenosis. Concerning epilepsy, the simultaneous presence of seizures and migraine attacks has frequently been reported (1). Notably, in many of these cases, EEG evaluation was either not available (11,12) or yielded normal findings (13–15). Conversely unspecific EEG abnormalities have been frequently reported and they were also found in our series. We documented diffuse or lateralised abnormal slow activity in repeated follow-up EEGs. Seizures were never observed. Involvement of the autonomic system occurred in two patients, who experienced cardiovascular instability and urticarial rash during severe migraine attacks. To date, the association between urticaria and headache has been reported only in one case of migraine without aura (16).
Clinical course of acute manifestation in patients I-1, II-2 and II-3. The migraine activity was classified in four levels of severity as follows: 0 = no attacks; 1 = attacks without hemiplegia; 2 = hemiplegic attacks; 3 = severe attacks with consciousness disturbances or high frequency of hemiplegic attacks. Time of FHM diagnosis and interval therapy is indicated.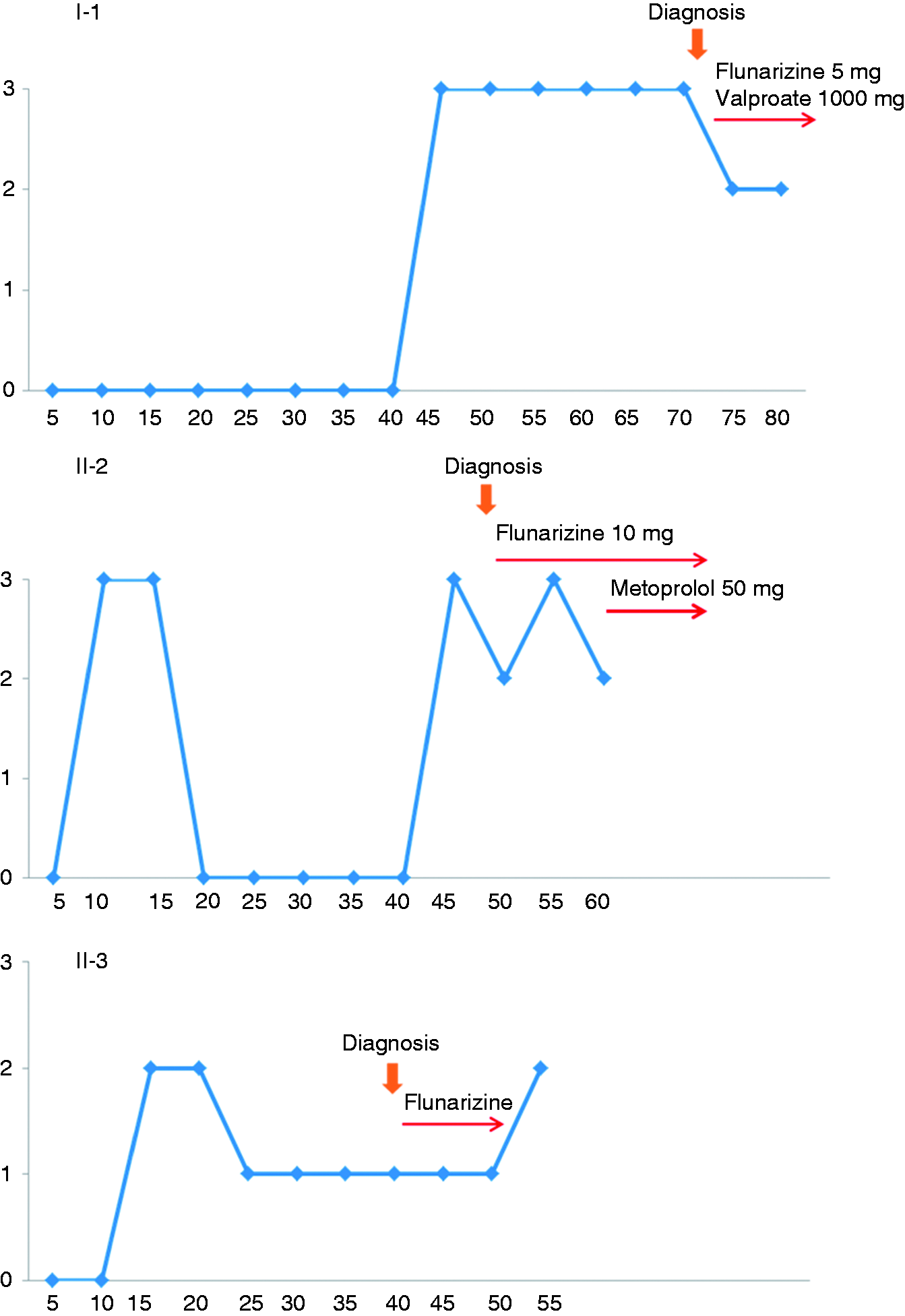
Clinical features of FHM1 family members.
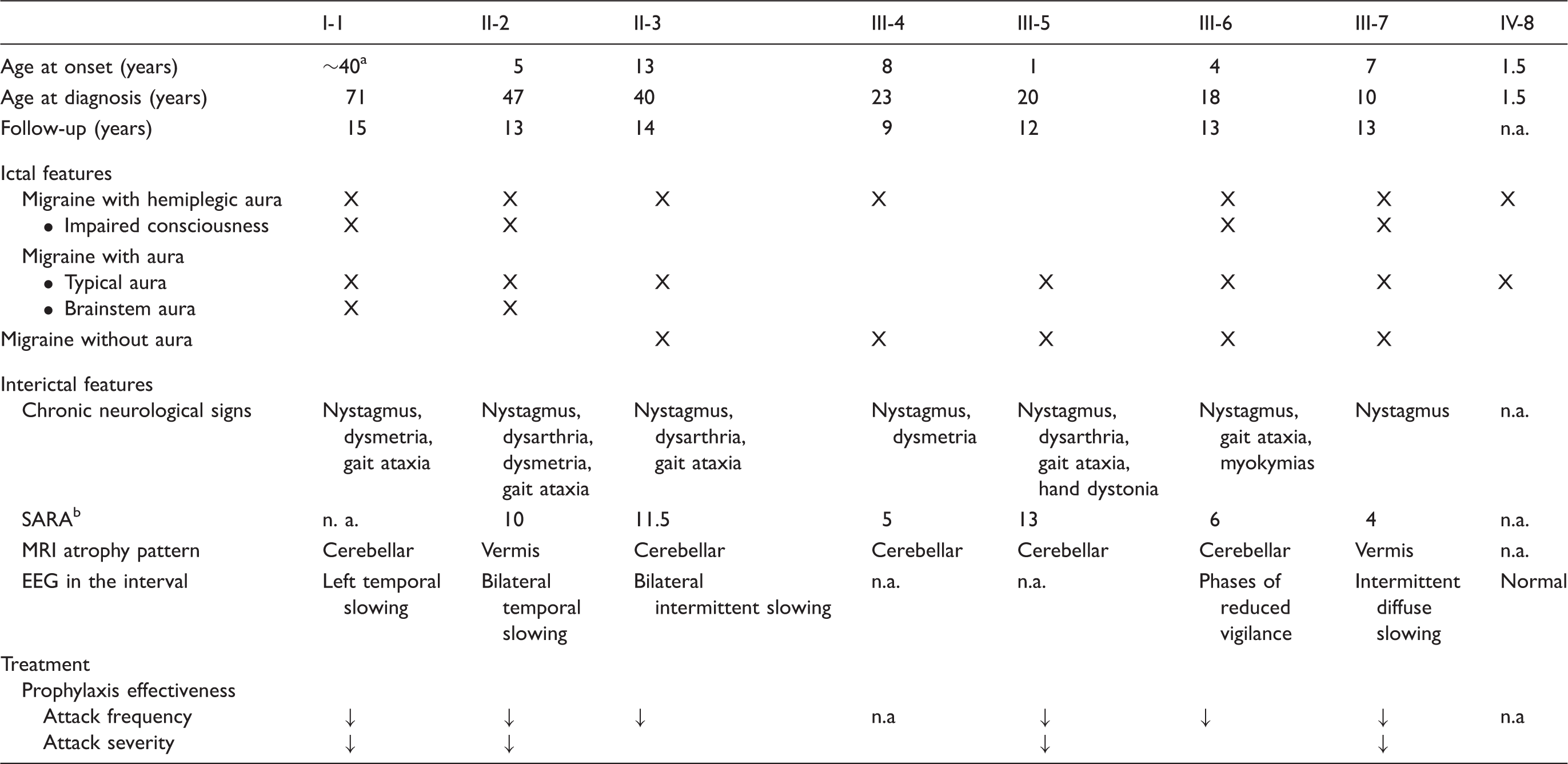
History of childhood attacks not available.
The most recent score is reported.
n. a.: not available/applicable.
Especially the presence of disabling up to life-threatening aura demands an effective migraine prophylaxis in FHM1. To date, a modifying therapy for migraine aura is not available (4).
Six out of seven FHM1 patients in our cohort received interval treatment for migraine. Frequency and severity of aura was markedly reduced in most of them, but severe attacks reoccurred in patient III-6 during follow-up. To the best of our knowledge, this is the first report about long-term management of FHM1. Current therapeutic strategies are based on standard migraine prophylaxis and studies from small case series (5). Besides the treatment with beta-blockers, non-selective Ca2+ channel blockers have been second-line therapy in migraine for decades (4). The T666M mutation in FHM1 affects the gating properties of neuronal P/Q calcium channels resulting in an enhanced cellular calcium influx (19). Non-selective Ca2+ channel blockers are supposed to modulate membrane excitability by inhibiting enhanced calcium influx in Purkinje cells (20). The use of flunarizine in FHM1 was documented earlier in single reports (21–23). Notably, in a retrospective study it appeared to be more effective in hemiplegic migraine than in common migraine in children (24). In only one case (patient III-6), non-selective Ca2+ channel blocker was suspended because of weight increase in a condition of pre-existing obesity. Besides, no other clear-cut side effects were observed. Some early reports showed benefit from acetazolamide in FHM treatment (25,26). Short-term experience with Acetazolamide in our FHM1 patients as an interval treatment was not successful. Acetazolamide is an effective treatment for episodic ataxia type 2, a disorder caused by CACNA1A missense mutations, which may show substantial overlap with FHM1 (26,27). It reduces bicarbonate levels by means of carbonic anhydrase inhibition and the resulting pH modulation is thought to affect the activity of ion channels (28). In one patient, metoprolol was successfully added to target migraine, hypertension and autonomic dysfunction.
The present observational study bears a number of shortcomings, as the small number of cases is limited to a single family harbouring a T666M mutation. Although the T666M mutation is the most frequent mutation in FHM1, numerous other mutations with an overlap to allelic disorders as spinocerebellar ataxia type 6 and episodic ataxia type 2 are known. It remains unclear if an interval treatment with low-dose non-selective Ca2+ antagonists is equally effective in all FHM1 mutations. It also has to be taken into account that the overall frequency of hemiplegic attacks is low and long attack-free intervals may occur independently from therapy (2). Moreover, frequency of attacks in FHM1 is extremely variable, even within patients bearing the same mutation.
Overall, our findings expand the current knowledge on FHM1 clinics and treatment. The clinical course may be biphasic with remission after adolescence and eventual recurrence later in adulthood, while permanent neurological signs show a substantially stable course. In terms of treatment, our experience shows that the prophylaxis with non-selective Ca2+ channel blockers is effective and well-tolerated in FHM1 long-term treatment, although severe attacks cannot completely be prevented. However, it remains speculative whether a reduction in attack frequency and severity by means of prophylactic treatment may have had beneficial effects on the progression of chronic neurological signs.
Clinical implications
The management of familial hemiplegic migraine 1 requires consequent interval treatment and management to reduce the frequency of attacks since intractable life-threatening neurological affection may occur during aura. Interval treatment with non-selective calcium antagonists was well tolerated in this T666M FHM cohort in a follow-up period of over ten years. Frequency and severity of migraine episodes could be reduced, although severe attacks were not completely prevented. Permanent neurological features remained stable during the follow-up as assessed by means of clinical evaluation, repeated MRI, EEG and neuropsychological testing.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.