
Abstract
Aim
To investigate the relationship between primary headache types and accomplished or attempted suicide in countries from all world regions.
Methods
Data were obtained using a questionnaire about suicide due to headache in a face-to-face interview with 203 physicians with expertise in headaches. They came from 48 countries, and from all continents.
Results
Primary headaches cause one suicide per 1,000,000 population each year (1% of the suicide rate due to all causes). Cluster headache and migraines account for 70–80% of them. Suicide attempts are 10 times more frequent than accomplished suicides. Cluster headache poses more risk than migraine. This risk is not often acknowledged, and is increased if there is previous psychiatric history. More than half of the physicians interviewed think it could be reduced with a more aggressive treatment of headaches.
Conclusions
Cluster headache and migraine are not always benign, and are the cause of the majority of suicides due to headache.
Aim
Suicide is a significant public health problem. Although primary headaches are considered benign conditions, the suicide risk may be underestimated as they are frequent, recurrent and severe: pain characteristics associated with suicide (1). Few studies have specifically addressed the relationship between headaches and suicide, and most of them are only concerned with suicide ideas or attempts in migraine (2). Our objective has been to estimate the size of the problem by collecting data on accomplished and attempted suicides related to different types of primary headache in a wide range of countries.
Methods
Number of physicians interviewed in regions of the world and in countries.

Countries in which the physicians interviewed had together a referral population of more than 100,000 people are underlined. Countries with more population per physician multiplied by number of physicians interviewed are ordered first into each world region.
Headache-associated (HA) suicide rates (SR); demographic and geographic data.

SR: (Suicide rate) number of suicides per 100,000 population per year; (SD): Standard Deviation.
If the outlier value of Japan (18) had been included, the SR would have been 0.22.
Includes the rest of the countries (Australia, New Zealand, Central Asia, Middle East, and Africa).
Results
Patient characteristics and data about the physician practice associated with suicide rate and suicide attempt rate.
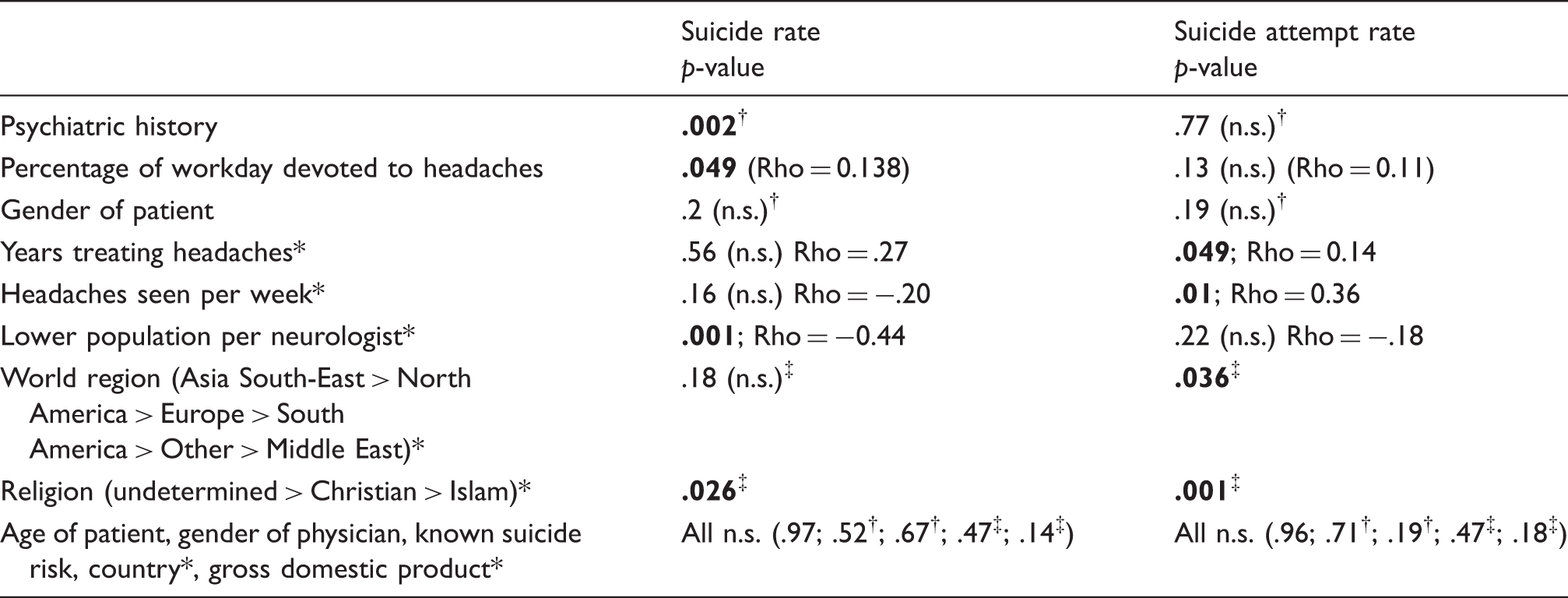
Associations were considered significant when p < .05 (bold figures); n.s.: not significant association. When variables are marked *, their value has been analyzed grouped by country. Analysis is with Spearman correlation coefficient when a Rho value is included, with Mann-Whitney (†) or Kruskal-Wallis tests (‡).
Globally, more than two-thirds of headaches associated with accomplished and attempted suicides were cluster headaches or migraines (Figure 1), while either tension-type headache or all the rest of the headaches grouped caused less than 11% of suicides or attempts. An exception was trigeminal neuralgia, which was associated with 26% of attempted suicides. The contribution to the global suicide rate (0.09/100,000 population-year) and global attempted suicide rate (1.04) of the different headache types was as follows: Cluster headache (0.04; 0.4); Migraine (0.04; 0.3); Other headaches (0.01; 0.06); Tension-type headache (0.01; 0.01); Trigeminal neuralgia (0.02; 0.3).
Contribution of each headache type to suicide rates.
Discussion
The global suicide rate due to headache reported by physicians was about one per million population-year, and while in South East Asia it was seven per million population-year, in the rest of world regions it was around 10 times less, being particularly low in Africa and the Middle East. These data should be considered provisional, due to the uneven distribution of the origin of interviewed physicians. Suicides increased between the age 30 and 40 and slightly predominated in women, albeit with variations between world regions (Table 2). This is at odds with suicide rate due to all causes, which worldwide is higher in men and in older people (4). The mean general population suicide rate due to all causes in the countries in this study was calculated as 12/100,000 population-year (5), around 100 times higher than headache-related suicide rate. Globally, suicide attempts motivated by headache were 1/100,000 population-year, 10 times more frequent than accomplished suicides (Table 2). Although, with wide variations among and within countries, an average of one suicide due to headaches, and nearly six suicide attempts, could be expected every 12.5 years of physician practice.
Only in North America, South America, and South East Asia was the suicide risk acknowledged before it happened in more than half of the cases. This can be related to more than half of the suicidal individuals having a psychiatric history in South America and South East Asia. Remarkably, half or more of the physicians in every world region judged that a more aggressive treatment of the headache or trigeminal neuralgia could have prevented the suicide or attempt. Suicide is not specifically recorded in headache clinical trials, but should be in the future. Its prevention could justify the emerging invasive therapies in selected cases. This underscores the need to detect suicide risk factors, in order to tailor treatment intensity of the headache. Not unexpectedly, psychiatric history is one of them (Table 3).
Some variables that may reflect more dedication by the physician to headache care are associated with more accomplished suicides (lower population per neurologist, higher percentage of workday devoted to headaches) or more attempted suicides (number of headaches seen per week and number of years treating headaches, Table 3). An over-detection bias due to closer follow-up cannot be excluded. The suicide attempts rate is also influenced by geographic region (South-East Asia > North America > Europe > South America > Other > Middle East). Both the accomplished and attempted suicide rate is higher in countries with undetermined or no predominant religion, intermediate where Christian religion prevails, and lowest in Islamic countries. This is in accordance with suicide rate due to all causes (4), whether for sociocultural influences or detection/reporting bias. Conversely, suicide or suicide attempt rates were not associated with patient age, with suicide risk being known by the doctor, with the particular country in which the patient lived, with its gross domestic product, or with the physician’s gender.
Among primary headaches, cluster headache and migraine each similarly encompass between 30–40% of suicide rates (Figure 1). Three general North-American population cohorts of migraine and severe non-migraine headaches reported increased suicidal ideas or suicide attempts (6), but to date we have found little information about accomplished suicides.
Cluster headache was nicknamed “suicide headache” shortly after its initial description, and between 15% and 21% of patients have suicidal ideation at some time, more in chronic (5.9–22% in different studies) than in episodic cluster headache (6.3–15%), and more than in migraine (4%) or controls (3%). Suicidal ideation is similar during bouts of episodic cluster headache, as well as between them (7). In other series, 55% of cluster headache patients had suicidal ideas, and 2% actually attempted suicide, men and women in the same proportion (8). But an increase of accomplished suicides in cluster headache has still not been generally accepted, because it is based on anecdotal reports (9).
Even if trigeminal neuralgia is the most severe pain that can be suffered and frequently elicits suicidal ideation, it was not the leading cause of suicide in any country, although it contributed to 25% of suicide attempts. While in a cluster headache episode there is restlessness and increased motor behavior, in trigeminal neuralgia bouts patients are usually motionless and auto-aggressive behavior may also be inhibited.
These findings of suicide risk for headache types need to take into account their very different prevalence. While migraine and tension-type headache have a prevalence in 3–12 months of 10 and 38 per 100 individuals respectively (10) in the general population, cluster headache has a one-year prevalence of 53 per 100,000 (11). Thus, if each group of headaches had a similar suicide risk, one single migraine would be four times, and one cluster headache 1000 times more lethal than one tension-type headache. Although cluster headache and migraine contribute similarly to the headache-related suicide risk of the population, as cluster headache is less prevalent, it carries more risk in the individual patient.
We also found that psychiatric history is associated with suicide. With depression being so prevalent in cluster headache and migraine, it is difficult to disentangle their relative contributions to suicide risk. Some data about migraine show that suicide risk appears to persist after controlling for depression only when migraine attacks are frequent or accompanied by aura (12).
The present data are retrospective and memory–based, with a low number of subjects, and due to these limitations they cannot be considered exact. It is rather a panorama of a problem difficult to study in registries, as suicides or their causes are not always reflected in some countries due to the stigma associated with suicide, and suicide attempts are not registered at all. Also, many headache sufferers do not seek specialized care, so the suicide rate is probably higher than the reported figures. Another limitation is that data cannot be replicated in the sample and they are based on recapitulation of the interviewed subjects, although the accomplished or attempted suicide of a patient in the last 10 years is difficult for a physician to forget. Also, European data are over-represented. There are also significant strengths in this study: Little variability in data collection (two interviewers, closed answers in questionnaire) from headache experts from 48 countries and, contrary to most published data, not about suicide ideation but about attempted and accomplished suicides. Some headache clinical practice data are presented.
Conclusions
Primary headaches are not always benign conditions and can provoke 1% of all suicides. Cluster headache and migraine are the main cause of headache-related accomplished and attempted suicides in a wide range of countries. Cluster headache poses the highest risk in the individual patient. Suicide risk is often not acknowledged in primary headaches, but physicians think that more effective treatment could prevent suicides. Psychiatric history should alert treating physicians.
Clinical implications
An interview conducted on 203 physicians with headache expertise from 48 countries shows that: 1% of all suicides are due to primary headaches, and suicide attempts are 10 times more frequent. 70–80% of headaches causing accomplished or attempted suicides are cluster headaches or migraines. In the individual patient, cluster headache poses more risk than migraine. A psychiatric history is an additional risk factor. More than half of physicians believe that a more effective treatment could prevent suicides.
Footnotes
Acknowledgements
We thank C Oyagüez for help with statistical analysis and the non-profit organization “Fundación Burgos por la investigación de la salud” for paying for four days of work of two interviewers, not related to the authors.
Ethical issues
As questionnaires were confidential and anonymous, with no names or personal data being asked and verbal approval before the interview was requested to each participant, evaluation by an ethics committee was not deemed necessary.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.