
Abstract
Background
Migraine is highly prevalent in women (18%). Peak morbidity affects their most productive years, coinciding with peak fertility. Hormonal contraception is often tailored for migraine prevention. Estrogen-containing contraceptives may be contraindicated in women experiencing migraine with aura due to the risk of vascular events. While improvements in migraine with a progestin-only pill (POP), which inhibits ovulation are documented, the strength and quality of evidence has not been formally evaluated.
Objectives
To determine the effectiveness of progestin-only contraceptives for migraine treatment by systematic review and meta-analysis.
Data sources and selection
MEDLINE, EMBASE and Cochrane Libraries were searched (1980 to September 2016) for studies on progestin-only treatments for migraine. Studies in English on >4 non-menopausal women aged 18–50 with migraine diagnosed by formal criteria were included.
Data extraction and analysis
Data were quality-assessed using the GRADE system. A random effects model was used for pooled analyses.
Results
Pooled analyses of four studies demonstrated that desogestrel 75 mcg/day, POP significantly but modestly reduced the number of migraine attacks and migraine days. Reduced intensity and duration, reduced analgesic and triptan use were observed, along with improved headache-related quality of life. GRADE analysis indicated evidence was low to very low for each outcome measure. Adverse effects resulted in treatment cessation for <10% of participants. Two studies compared desogestrel POP to a combined oral contraceptive, demonstrating similar migraine outcomes for both treatments.
Conclusions
The desogestrel POP shows promise in improving migraine in women. Current evidence is observational and based on small samples of women using only one oral progestin-only formulation. Further randomized trials on additional progestin-only contraceptives are required to confirm their role in migraine management.
Abbreviations
Combined oral contraceptive pill Grading of Recommendations Assessment, Development and Evaluation Migraine with aura Migraine without aura Menstrually-related migraine Non-menstrual migraine Non-steroidal anti-inflammatory drugs Pure menstrual migraine Progestin-only pill
Introduction
Description of the condition
Migraine is common, affecting approximately 18% of women and 6% of men (1), translating to its ranking as the third most prevalent disorder and seventh highest specific cause of disability in the Global Burden of Disease Survey of 2010 (2). Migraines in women are a significant health issue, not just because of their high prevalence, but also because of their distinct relationship with hormonal changes (3). Migraines typically worsen or begin with the onset of menarche and they commonly occur with menstruation (known as menstrual migraine) for up to 60% of women (4). This peak in incidence coincides with a woman’s most productive years, affecting her personal relationships and having a notable economic burden due to a loss of productivity and work absenteeism, long term need for medications and recurrent visits to health care professionals (5,6).
Available treatments for migraine
Conventional management of migraine involves symptomatic treatment for acute attacks and consideration of daily preventative medication for those with frequent migraine. For acute migraine, agents such as non-steroidal anti-inflammatory drugs (NSAIDs), triptans and anti-emetics in varying combinations may be effective (7,8). For patients experiencing frequent migraine and/or migraine causing impairment, the use of daily preventative treatments such as propanolol, amytriptyline, pizotifen or topiramate, are recommended (1).
Ovarian hormones are likely to modulate the nociceptive and anti-nociceptive pathways involved in migraine pathogenesis (9,10). Furthermore, menstruation appears to be one of the most prominent factors implicated in the occurrence or persistence of headache and migraine (11). As mentioned above, 60% of women with migraine have menstrual exacerbation. Both ovulation and menstrual bleeding patterns can be potentially manipulated by the use of hormonal therapies, thereby potentially altering migraine. Hence, whilst not first-line management, a clinician may also consider tailoring a female migraineur’s choice of contraception or gynaecological treatment, particularly if hormonal sensitivity of migraine is evident.
A recent systematic review documented low-level evidence for the use of various combined oral contraceptive pills (COCs), oestrogen gel and gonadotropin-releasing hormone agonists (12) in the treatment of menstrual migraine. However, there are significant limitations to the use of COCs documented in WHO and international guidelines (13,14), particularly the two to four-fold increased risk of stroke in women who experience migrainous aura (15) and prevalent comorbidities such as advancing age over 35 and smoking status (13,14). One third of women with migraine experience aura, therefore the cohort of patients unable to use the COC is sizeable (16). Furthermore, COCs have been reported to have a variable impact on migraine, worsening migraine in some women (4).
Progestin-only treatments for migraine
Given the contraindications to combined hormonal contraceptive (CHC) use in a significant proportion of female migraine sufferers, including all women with migraine with aura (MA), progestin-only contraceptives are increasingly considered as an alternative for patients with migraine, particularly those experiencing migraine with aura. World Health Organisation and UK Faculty of Sexual and Reproductive Health Medical Eligibility Criteria state that progestin-only contraceptives are generally considered safe for use in women with risk factors for stroke including MA (13,14). Recent clinical reviews report improvements in migraine symptoms with a relatively high-dose progestin-only pill (POP), the desogestrel 75microgram/day pill (17,18). Despite this, the strength and quality of evidence on POPs for migraine treatment has not been formally evaluated. The mechanism of progestin in reducing migraine frequency and intensity is largely unknown, but may relate to inhibition of ovulation and modulation of nociceptive pathways (17).
Study objective
To determine the effectiveness of POPs for migraine treatment in pre-menopausal women aged 18–50 by systematic review and meta-analysis.
Method
The systematic review and meta-analysis were prepared using the Meta-analysis Of Observational Studies in Epidemiology checklist (19), Preferred Reporting Items for Systematic Reviews and Meta-Analyses (20) and Review Manager 5.3 software (21).
Search strategy
A comprehensive literature search of Cochrane library, MEDLINE AND EMBASE was performed by two investigators (SW, CR). Search terms were across three categories and included 1) migraine or headache, 2) progesterone, progestin, progestogen, or desogestrel and 3) treatment or contraceptive. The MEDLINE searching procedure is included in Appendix A (Supplementary material). Additional relevant studies were identified in Scopus and Google Scholar as well as reference lists of treatment and review articles.
Inclusion and exclusion criteria
Inclusion and exclusion criteria as well as outcome measures were selected prior to the literature search, based on the International Headache Society’s Guidelines for controlled trials of drugs in migraine (22), where appropriate. Excluded studies including reason for exclusion are listed in Appendix B (Supplementary material).
Types of studies
All prospective and retrospective studies published in English (1980 – September 2016), in which progestin-only contraceptives were used for the management of migraine in women, were included. Studies in a language other than English were included if a reliable English translation could be obtained. Review articles and case series with less than four participants were excluded.
Type of participants
Studies on women (aged 18–50) with MA, migraine without aura (MO) and menstrual migraine were included. Study participants were diagnosed with migraine by any edition of the International Headache Society criteria (23) or another reasonable criterion, by a physician. Studies on pregnant women and participants on hormone-replacement therapy for menopausal symptoms were excluded.
Type of interventions
Studies with at least one arm investigating progestin-only contraceptives for migraine management were included. Comparator arms, such as groups receiving no treatment, or treatment with CHCs or other medical treatments for migraine, were acceptable. For all study groups, use of acute analgesia or rescue medications was permitted, but these needed to be recorded.
Types of outcome measures for use in meta-analysis
To determine treatment effectiveness, studies needed to include one of the outcome measures of interest. The primary outcome measure was the number of migraine attacks following 180 days of treatment with a progestin-only treatment. Secondary outcome measures included 1) number of days with migraine; 2) duration of migraine; 3) average headache intensity; 4) number of symptomatic pain medications and triptans used; 5) Headache-related quality of life scores; and 6) rates and types of adverse events.
Data extraction and quality assessment
Studies were reviewed by two authors (SW, CR) to determine eligibility for the study based on the inclusion and exclusion criteria. The Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach (24) was used, as recommended by the Cochrane Collaboration (25) to evaluate the quality of evidence for each outcome measure. The GRADE rating was also performed by two authors (SW, CR) and discrepancies were resolved by consensus.
Meta-analysis
Point estimates at baseline and at 90 days and 180 days post-initiation of treatment were extracted for all outcome measures. To perform the meta-analysis for each POP pre- and post-treatment outcome, a random effects generic-inverse variance model was used to combine point-estimates in RevMan, specialist software produced by the Cochrane Collaboration (21). Tau-squared was calculated using the DerSimonian and Laird method (26). Correlations between results at baseline and 90-day and 180-day point estimates were not reported in any included studies, so these were assumed to be zero to produce the most conservative results. p-values are reported with no adjustment for multiplicity of analyses.
Rates of adverse effects associated with desogestrel POP use were computed from study data and 95% confidence intervals were calculated using Wilson’s method in OpenEpi (27). For adverse effects of desogestrel compared to the COC, risk differences were calculated using a Mantel-Haenzsel random effects model and days with bleeding analysis was performed with a continuous random effects model, both in RevMan (21).
Results
Included studies
Six studies met the inclusion and exclusion criteria for the study and were considered eligible for the systematic review. However, upon further correspondence with the authors of the Swiss studies, it was confirmed that one study (28) was an extension of two 2013 studies (29,30) so these earlier studies were excluded to avoid biasing pooled analyses with duplicated participant data. One eligible study in German was also excluded as no translation could be obtained from the authors. Details of the searching process and application of inclusion and exclusion criteria are shown in Figure 1. Characteristics of the four included studies (28,31–33) are shown in Table 1. All studies reported pre- and post-treatment data for a desogestrel 75microgram/day POP. Two of the included studies (32,33) additionally compared the POP to a COC (containing desogestrel 150 micrograms and ethinylestradiol 20 micrograms) after 90 and 180 days’ treatment. Nappi et al. (31) examined two different groups with MA, one with previous COC use and one without. Results for both groups were eligible for inclusion, so have been reported separately in the meta-analysis.
PRISMA flowchart detailing data identification, screening, eligibility and inclusion. Characteristics of studies identified for inclusion systematic review and meta-analysis. P: prospective; R: restrospective; CS: case series (with pre and post-test data); cohort: cohort study; MO: migraine without aura, MA: migraine with aura; pre: pre-treatment; post: post-treatment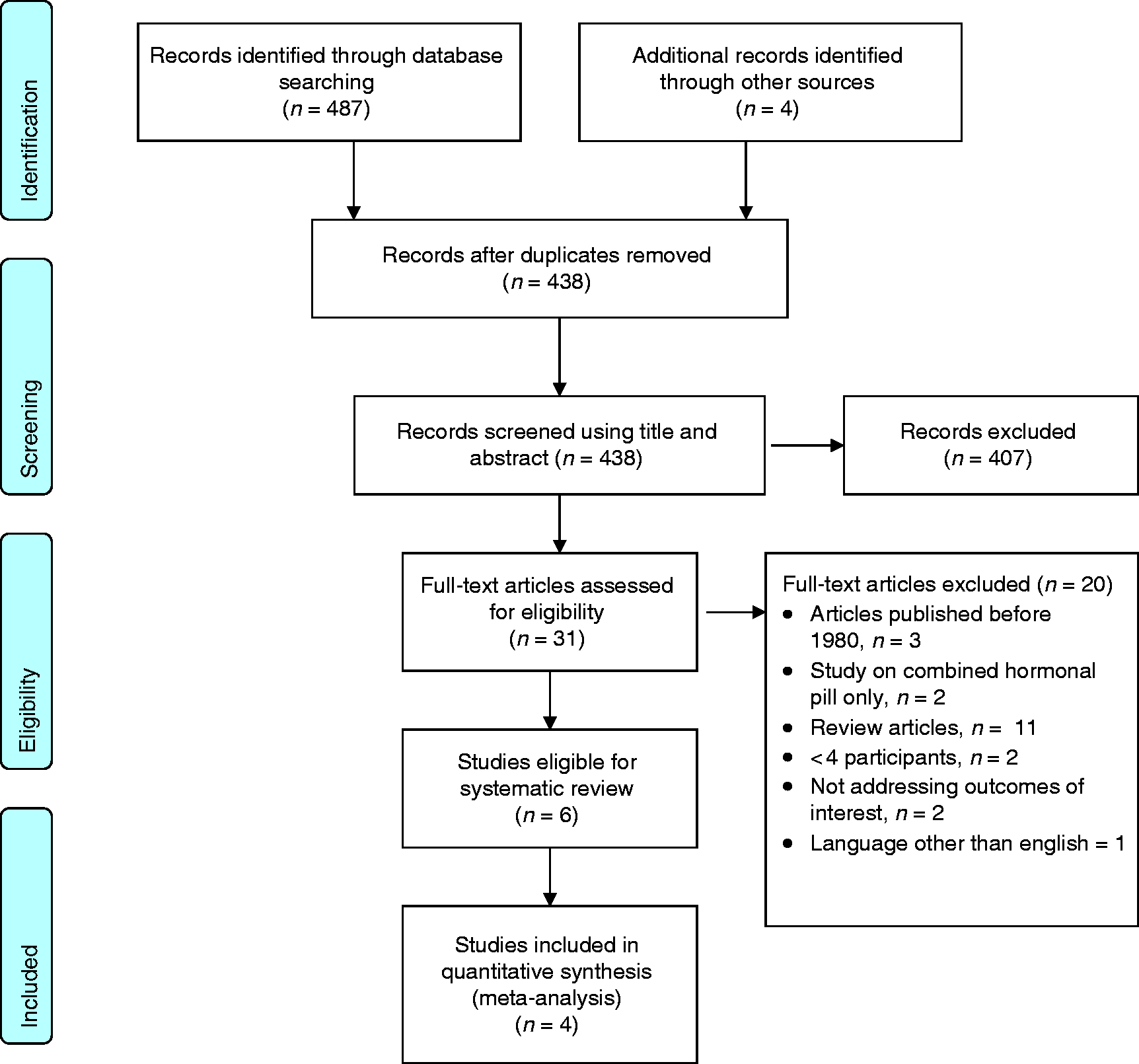

GRADE evaluation
Summary of findings table and GRADE analysis for all outcomes measures at 180 days.

For all studies, headache intensity was rated on a scale of zero to four. In Merki-Feld, 2015 and Morotti, 2014a, the average monthly headache intensity as calculated as: the sum of the last 90 days of severities divided by three. This produced an average headache intensity measure that was also dependent on migraine/headache frequency.In Morotti, 2014b (35), the authors used the same four-point scale to measure headache intensity as Morotti, 2014a and Merki-Feld, 2015, but their method for averaging the headache intensity was not clearly described. Therefore results were not included in the meta-analysis.
See Appendix C (Supplementary material) for further detail on how GRADE rating was performed.
Nappi, 2011 (31) reported analgesic use as the number of analgesics required per attack and found no significant decrease in use of pain medications after POP treatment in both groups.
Primary outcome measure: POP pre-treatment vs. post-treatment
Forest plots for each outcome measure are presented in Appendix D, Figures 1–13 (Supplementary material) and mean differences with p-values for each outcome measure at 180 days are presented in Table 2. Pooled analysis showed that the number of attacks of migraine per month was significantly decreased at 180 days post-treatment, compared with baseline. However, the size of this mean random effect was modest, with 0.64 fewer migraine attacks per month at 90 days and 0.96 fewer migraine attacks per month at 180 days. The women had a mean migraine frequency of 4.43 migraines per month in the pre-treatment period.
Secondary outcome measures: POP pre-treatment vs. post-treatment
Pooled analyses found small but significant reductions in the number of days with migraine per month, average headache intensity and number of pain medications used per month at both post-treatment time points. Significant reductions in duration of migraine and use of triptans following 180 days of POP use were also observed, compared with the pre-treatment baseline. However, random effects for these outcomes were not significant 90-days post-treatment.
Quality of life scores at 90 days and 180 days
Merki-Feld et al. (28) examined the effects of the POP on participants’ Migraine Disability Assessment (MIDAS) scores at 90 days and 180 days post-treatment. A mean change (improvement) in total MIDAS score of −18.00 (p < 0.001) was observed, as well as a significant reduction in all individual MIDAS items (p < 0.001 – p = 0.046). Morotti et al. (32,33) also reported significant improvements in quality of life, related to POP use, measured using two subscales of the Short Form-36 version 2 (SF36v2) questionnaire (34) (p < 0.001 for both subscales in both studies). However, insufficient data were reported to facilitate meta-analysis of these results.
Adverse events at 180 days
Adverse effects leading to treatment cessation, related to use of desogestrel 75 mcg/day.

Effects of interventions: Desogestrel 75 mcg/day POP vs. a desogestrel-containing COC
Two included studies also compared the desogestrel POP to a COC containing desogestrel 150 mcg and ethinylestradiol 20 mcg. Pooled analysis of most outcomes could not be performed as the studies used differing outcome measures and differing COC regimes. In both studies, there were no significant differences in baseline demographic characteristics between the POP and COC groups.
Morotti et al. (32) examined the effects of the desogestrel POP, compared to continuous use (i.e. with no pill-free interval) of the desogestrel-containing COC in women with MO. The POP and COC group had no differences in migraine days per month, average headache intensity, pain medication use and triptan use, after 90 days of treatment. After 180 days of treatment, the POP group reported significant improvements in headache-related quality of life (measured by SF-36v2, p < 0.001 for both subscales), an effect that was not seen in the COC group. However, when directly compared, no differences in SF-36v2 scores between the two groups were found. The participants using the POP also reported slightly less pain medication use at 180 days (mean difference = 1.0, p = 0.044) than participants on the COC pill.
Morotti et al. (33) examined the effects of the desogestrel POP (n = 55), which is used continuously (without a hormone-free interval), compared to the same desogestrel-containing COC, with the prescribed hormone-free interval (n = 62) in women with MO and rectovaginal endometriosis. The POP group had significantly fewer migraine attacks than the COC group after both 90 days (mean difference = −1.1 attacks/month, p < 0.001) and 180 days of treatment (mean difference = −1.04 attacks/month, p < 0.001). Migraine attacks were also significantly shorter (mean difference = −2.94 hours, p < 0.001 at 90 days, with a similar effect at 180 days) and less intense (mean difference = −0.29 on a four-point rating scale, p < 0.001 at 90 days, with a similar effect at 180 days) in the POP group compared to the COC group.
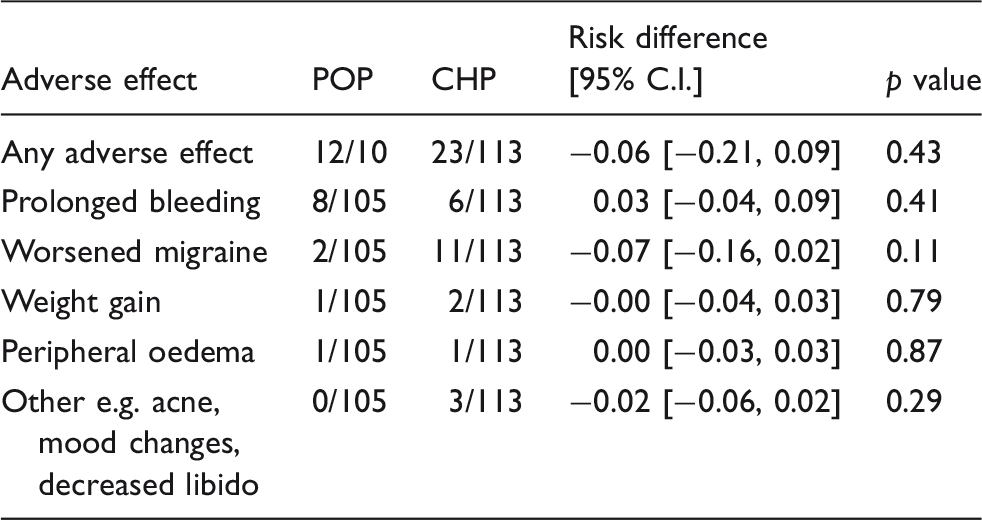
Adverse effects and days with bleeding: POP compared to COC at 180 days
Risk differences for adverse effects leading to treatment cessation, associated with POP compared to COC in Morotti, 2014a and Morotti, 2014b.
Discussion
Summary of main results
This systematic review examines the current evidence for the use of a POP for migraine management in women. A comprehensive literature search found only four observational studies that met the inclusion criteria, all of which examined the effects of a single POP containing desogestrel 75 micrograms per day over a 180-day treatment period. None of the included studies were randomised. Meta-analysis demonstrated that the POP reduces the number of migraine attacks and number of days with migraine per month at 90 days and 180 days post-treatment, compared with the pre-treatment baseline. However, the effect size was small and likely reflects variability in treatment response between women. In fact, two included studies (28,33) found that days with migraine or headache increased post-POP treatment in 12.9–16.7% of women. However, Merki-Feld et al. observed a 25% post-treatment reduction in the number of headache and migraine days in 55% of participants, and a 30% reduction in pain was observed in 60% of participants (28).
The desogestrel POP was also associated with a significant reduction in the duration of migraine and a reduction in the use of triptans 180 days after commencement of treatment, but not at 90 days. The POP also reduced the number of pain medications required throughout the post-treatment period. Merki-Feld et al. (28) reported a substantial improvement in MIDAS scores associated with the POP. Overall, the quality of evidence for the POP in treating migraine is considered low to very low for all outcome measures (see Table 2 and Appendix C, Supplementary material), indicating that future research is likely to alter the effects for each outcome measure.
Two studies directly compared women using the desogestrel POP to women using a COC containing desogestrel-ethinylestradiol. Given that our review searched widely on progestin-only contraceptives for migraine treatment, it is likely that these are the only two current studies in English comparing the COC with the POP for migraine treatment. One study (33) showed minimal differences in migraine symptoms between women on the POP compared to a COC used continuously, without a hormone-free break. However, the second study (32), found that the POP was associated with significant reductions in frequency, duration and intensity of migraine attacks, compared with the COC used with a regular withdrawal period, for women with MO and comorbid rectovaginal endometriosis. Although POPs are typically associated with unpredictable bleeding patterns (35), pooled analysis of adverse effects in our study showed similar risks of adverse effects, including prolonged bleeding, in women with MO on both the POP and the COC.
Overall completeness and applicability of evidence
No studies had placebo-controlled or randomised groups, as this may be ethically difficult with drugs that affect fertility, but two studies compared the POP to the COC as a likely alternative approach. In general, however, the lack of control groups is a significant limitation of the current evidence on progestin-only treatments for migraine, as improvements noted may be due to the natural history of migraine, regression to the mean or amelioration due to the passage of time (22). The GRADE analysis indicated a low to very low quality of evidence for each outcome measure. In particular, the duration of migraine outcome was downgraded, as one group in Nappi et al. (31), who had never taken COCs, experienced a slight increase in migraine duration following treatment with the POP. The average headache intensity outcome was also downgraded for indirectness, as the averaging method used means it is more likely a measure of migraine morbidity (both intensity and frequency) rather than intensity alone (see Appendix C, Supplementary material).
Meta-analysis of all reported quality of life data was impeded by unavailability of post-treatment means and standard deviations in two studies (32,33), although improvements in headache-related quality of life were reportedly significant in these studies. Similarly, although all studies followed the International Headache Society guidelines in principle (22), there was inconsistency between studies in the computation of averaged outcomes (e.g. average headache intensity and pain medications used). In our review, two studies (one with a COC control group) used “number of migraine attacks per month” and two studies (the other with COC control group) used “number of migraine days per month”, reducing the total participant data for each outcome. Although “number of migraine attacks” is considered the superior primary efficacy measure in International Headache Society guidelines (22), it is possible that “days with migraine” data is more reliably collected by participants, potentially explaining the inconsistency between studies.
Despite the extensive literature search, data for this meta-analysis was limited to a single POP, the desogestrel 75 mcg/day pill, whose positive effects on migraine may be related to the inhibition of ovulation (8). It is likely that similar effects may be seen with the etonogestrel implant, which also inhibits ovulation (36). However, other progestin-only treatments such as the LNG-IUS, which exerts its hormonal action at a local level within the uterus, rather than through inhibition of ovulation, or the lower-dose POPs, which act primarily through their effect on cervical mucus, may have not have the same effect on migraine. It is possible that amenorrhoea may also impact on migraine symptoms (37), which may provide an additional mechanism for contraceptives such as the etonogestrel implant and LNG-IUS. The practical application of these findings is also geographically-specific, as the desogestrel 75 mcg/day pill is not approved for clinical use in some countries including Australia.
In discussing the generalisability of findings, it is also important to consider the types of participants included in each study as well as their diagnosis and clinical presentation. All included studies utilised the widely-accepted diagnostic criteria of the International Headache Society (ICHD-II) and between the included studies, data for women with both MO and MA is available (see Table 1). Only Merki-Feld et al. (28) included women on preventative medication (with no regime changes permitted, see Table 1) and a small number of women (n = 6) with chronic daily headache, so the results of this meta-analysis are more likely to apply to women with less frequent or severe migraines. Morotti et al. (32) compared the effects of the POP and the COC on different migraine patterns including pure menstrual migraine (PMM), menstrually-related migraine (MRM) and non-menstrual migraine (NMM). They found that women with NMM on the POP had fewer migraine attacks than women with NMM on the COC (p < 0.001). Additionally, women with PMM and MRM on the POP had less intense migraine attacks than those with PMM and MRM on the COC (p < 0.001).
Implications for future research
Migraine in women is not a trivial issue. In addition to the morbidity for the individual, the high prevalence and chronicity of migraine translates to a major burden on health resources and economic burden due to loss of productivity (2). Despite this, migraine is often overlooked in health care agendas and there is surprisingly little data regarding the effectives of POP for migraine, in particular, there being no randomized trials. Although this meta-analysis shows promising treatment effects of the desogestrel POP for migraine, there is a critical need for further prospective, cohort or randomised trials examining the effects of hormonal contraceptives for migraine treatment in general. Intuitively, the modest benefit identified in this paper would translate to significantly larger outcomes over a lifetime when followed for longer timeframes. More consistency in the use of the International Headache Society guidelines on migraine research (22), particularly in use of migraine frequency measures and calculation of headache intensity, will facilitate more reliable comparison of study results. In light of the variability in treatment response documented by two studies (28,33), further studies should also focus on the identification of patient and migraine features that might predict a favourable response to hormonal contraceptives.
In addition, the effects of other frequently used progestin-only contraceptives, such as the etonogestrel implant and the LNG-IUS, on migraine have not been studied. Further research on other doses of the desogestrel POP, as well as other progestin formulations, may be warranted. POPs appear to be acceptable to and safe for a significant proportion of women, but our understanding of their effects on migraine is currently incomplete.
Implications for clinical practice
This meta-analysis supports the emerging role of the POP, specifically the desogestrel POP, for migraine in women with both MO and MA. The POP was associated with significant improvements in migraine symptoms and reduction in acute medication polypharmacy over a short follow-up period of 180 days. Although these improvements are modest in terms of clinical effect, the benefits and improvements associated with these small changes in migraine symptoms, especially in larger populations of women, could result in a significantly-reduced global burden of disease. Furthermore, it appears that the clinical effects of the POP on migraine are much greater in some women than others, and seem to result in significant clinical improvement for up to 60% women (28).
Desogestrel is a highly-selective third generation progestin with low androgenic activity. The 75 mcg/day formulation is not widely used in the United States and is unavailable in Australia, but is used frequently in European countries such as Sweden (18,38). As a relatively high dose of daily progestin (compared to other progestin-only ‘mini-pills’), it inhibits ovulation in 99% of cycles (39,40) and may lead to amenorrhoea (41). These effects are both likely contributors to its positive effects on migraine symptoms. Progesterone is also postulated to have direct effects on the nociceptive pathways in the trigeminovascular system (42) and administration of synthetic progestins can modulate oestrogen variation by inhibiting ovulation. An advantage of the desogestrel POP is its safety for use in women with a range of comorbid conditions, including migraine with aura and hypertension (14,43). However, like other progestin-only contraceptives, the desogestrel POP can cause unfavourable bleeding patterns (e.g. frequent or irregular bleeding and prolonged bleeding), which occur as result of the continuous progestin effects on the endometrium and can be a reason for treatment cessation (44,45). Further, the impacts of long-term anovulation, such as osteoporosis risk, need to be considered in this cohort. At the time of writing, no published data on bone mineral density and fracture risk in desogestrel users was available.
Pre-menopausal women with migraine frequently present to neurologists, reproductive health physicians and primary care physicians with the clinical dilemma of optimal hormonal contraceptive manipulation. This dilemma requires a careful multi-disciplinary approach that considers the individual woman’s migraine diagnosis (with or without aura), comorbid risk factors, gynaecological conditions such as endometriosis or heavy menstrual bleeding, and preferences around bleeding patterns. Specialist members of the multi-disciplinary team need to be aware that medications may often interact in these women. For example, the COC may worsen migraine, and certain migraine preventative treatments (e.g. topiramate) may act as hepatic enzyme inducers and reduce circulating hormone levels, potentially compromising contraceptive efficacy. Women also require significant education and counselling around their hormonal contraceptive options and their associated adverse effects, so they can be informed participants in this decision-making. This meta-analysis provides data that may help a woman and her treating physicians decide whether desogestrel 75 mcg/day, if available, will suit her clinical needs. It appears that for the majority of women, desogestrel 75 mcg/day will provide effective contraception, which may additionally and modestly improve migraine symptoms.
Clinical implications
The desogestrel 75 mcg/day POP is associated with modest reductions in migraine frequency and duration as well as reduced use of analgesics and triptans after 180 days’ use in most women. Evidence is observational and future prospective, randomised trials will assist in determining the true clinical effects of the desogestrel POP and other progestin-only contraceptives in migraine treatment. The desogestrel POP should be considered in women with migraine, particularly those with common contraindications to COC pill use such as migrainous aura and hypertension.
Footnotes
Acknowledgements
The authors would like to acknowledge the invaluable advice and guidance of Associate Professor Sally Lord, University of Notre Dame, with regard to study design and analysis.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: One of the authors, Gabriele Merki-Feld, was an author of one study included in the meta-analysis, but analysis of all included papers was performed independently. As part of her role as Medical Director of Family Planning NSW, Deborah Bateson has provided expert advice to Bayer healthcare and MSD, which produce contraceptive pills and the LNG-IUS and etonogestrel implant respectively. She has been supported to attend and speak at conferences by Bayer Healthcare and MSD, but has never received personal remuneration for these services.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: St Vincent’s Clinic Foundation and the Brain Foundation (Australia).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.