
Abstract
Objective
We aimed to investigate the morphological changes and potential correlation between chronic headaches and the rectus capitis posterior minor muscle (RCPmi).
Methods
Comparison of RCPmi between patients with chronic headaches and healthy adult volunteers were collected using magnetic resonance imaging (MRI) and Mimics software.
Results
Among the 235 MRI images analyzed, the data between the two groups were considered statistically significant. The number of males was larger than that of females (p < 0.001) and the headache group showed greater hypertrophy than the control group in both males (p < 0.001) and females (p = 0.001).
Conclusions
Chronic headaches were correlated with the RCPmi. Patients with chronic headaches suffered from more obvious hypertrophy than that of the control group. Additionally, it was supposed that RCPmi hypertrophy may be one pathogenesis of the chronic headaches.
Introduction
In clinical practice, a chronic headache is defined as a headache that lasts for at least 15 days a month for a minimum of 3 months, irrespective of any underlying headache disorder (1). The two most common primary headaches are migraine and tension headaches (2–4). In recent studies, a new hypothesis of chronic headaches was proposed. In 1995, a new anatomical structure, named the myodural bridge (MDB) was first described by Hack et al. (5). It is a dense connective tissue bridge located between the rectus capitis posterior minor muscle (RCPmi) and the spinal dura (5). This structure connects to the posterior atlanto-occipital membrane perpendicularly, and merges with the cervical dura mater. It is believed that the continuity of the fibers may protect against the movement of the spinal dura (6). The MDB plays an important role in chronic headaches (7–13). Whenever pathological changes occurred in the RCPmi, improper forces may be transmitted through the MDB to the pain-sensitive spinal dura, resulting in chronic pain. In 2004, a case reported by Hack (14) identified one patient who suffered from chronic headaches that were initially precipitated by trauma. When examined by magnetic resonance imaging (MRI), physicians found that the suboccipital muscles of the patient appeared hypertrophied. By severing the connection between the hypertrophic suboccipital musculature and the dura mater, the patient experienced relief.
Despite the importance of RCPmi and MDB, there is still a lack of studies to illustrate the importance of this muscle in individuals with chronic headaches.
Our study investigated the differences of the RCPmi between normal adults and patients who suffered from chronic headaches, and assessed the potential effects of the MDB, the aim of which was to find a new explanation of the chronic headache using MRI.
Materials and methods
Patients
This is an observational cross-sectional study comparing two groups. This research was approved by the Ethics Committee of Dalian Medical University. The clinical MRI images were collected from the 403 Affiliated Hospital of Chinese PLA General Hospital in Dalian from June 2014 to April 2016. All volunteers provided written informed consent for primary data acquisition and the publication of their individual clinical details. The control group was composed of 120 participants who did not meet the diagnostic criteria of any headache and other physical illnesses. The group of 115 patients had suffered from chronic headaches for more than 15 days per month for longer than 3 months, excluding a history of cardiovascular, neurological or other certain cervical disorders.
Data collection
The scanning apparatus and parameter used in this study was a 0.35 T MRI scanner (BTI-035) with a neck-phased array coil (Shenzhen Basda Medical Apparatus Co., Ltd., China). The scanning sequence T2WI/FSE (TR/TE 3200 ms/115 ms) was employed with a thickness of 5 mm, interval of 1 mm, matrix: 256 × 279, field of view: 272 × 272 mm and NEX: 2. All identifying information was removed when the sample images were obtained.
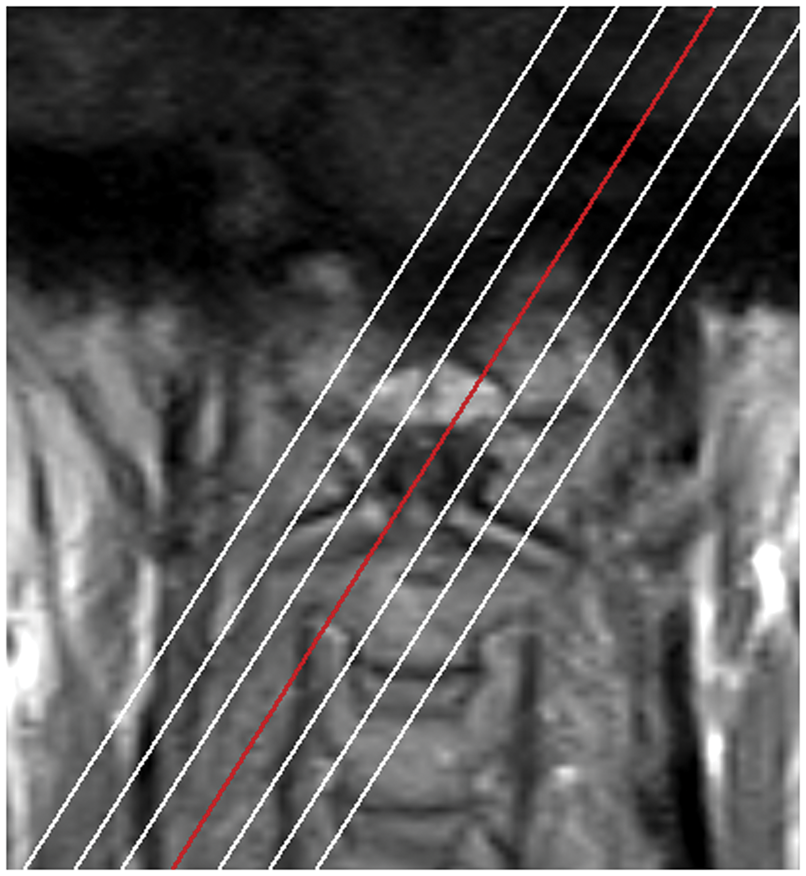
To justify the standard of the image measurement, a pre-experiment dissection was done in 10 head-and-neck specimens with the RCPmi before the collection. The angle (α, Figure 1) between the medial and lateral borders of the RCPmi was measured and the value was (60.7 ± 4.4)°. For the standard of measurement, a 30° deviation was considered the greatest plane image of the RCPmi. The left RCPmi of all volunteers were scanned with a 30° deviation from the sagittal plane by T2-weighted MRI scanning. The image, passing through the mid-posterior arch of atlas, was selected for measurement (Figure 2, red line). The data was collected and mixed by one physician and analyzed by another.
Dissection photograph of the rectus capitis posterior minor muscle (RCPmi). The mean value of the angle of measurement between the medial and lateral border of the RCPmi was 60.7 ± 4.4°. As a result, the angle α = 30° was designed for magnetic resonance imaging (MRI) scanning for better view. The measuring method and image selection. All volunteers were scanned with a 30° deviation from the sagittal plane and the image passing through the mid-posterior arch of atlas was selected for measurement.
Measurement
After the collection, RCPmi measurement was performed without any information from volunteers (the double-blinded method). These selected images were measured using Mimics Software (Version 17.0, Materialise China Office, Shanghai, China) (Figure 3). Mimics is a software interface and image segmentation system for the transfer of imaging information from a variety of imaging sources to an output file. It is also used as software for simulating, measuring and modeling. In our research, we measured the surface area within a closed polygon after information is displayed. The gray values may be chosen within a certain range and the surface decided semi-automatically. After the measurement, the value of the surface may be computed immediately. In our research, to avoid an inaccurate impact of adipose tissue and connective tissue, only the muscle belly of the RCPmi was measured. The signal range of the RCPmi was determined by Mimics, compared with the same muscular low signal of the semispinalis capitis.
30° deviation MR images of the RCPmi. The outline of the RCPmi was determined by the Mimics Software in each MR image. The cross-sectional area of the RCPmi was determined and the data was exported immediately. RCPmi: rectus capitis posterior minor muscle. C1: the first cervical vertebra. SSC: semispinalis capitis.
Statistics
After measurement, the data was divided into two groups based on the information from volunteers. Data was analyzed using the Statistical Package for the Social Sciences (IBM SPSS Statistics 19.0). The 95% confidence interval and mean ± standard deviation (SD) of the RCPmi were recorded, and the mean values between two groups were examined for statistical significance using an independent-sample t-test. A two-sided p-value of less than 0.05 indicated statistically significant differences. The p-values reported in this paper are not adjusted for multiplicity. No individuals were excluded in the analysis.
Results
Sectional area analysis of the rectus capitis posterior minor muscle (RCPmi) compared with two groups.

The unit of measurement was mm2. There were no statistical differences in age between the two groups in males (p = 0.334) and females (p = 0.202). *Comparison of the male between control group and headache group, p < 0.001; •comparison of the two groups in females, p = 0.001. Based on the statistical analysis, the headache group showed obviously greater hypertrophy than the control group.
Of the 235 MRI images analyzed, the data of the two groups—the control group and the headache group—were considered statistically significant. This indicated that the headache patients had significant hypertrophy of the RCPmi compared with the control group.
Discussion
The suboccipital region is one of the most complicated areas in the human body and consists of cranii, atlas, axis and deep muscles, including the RCPmi, rectus capitis posterior major muscle (RCPma), obliquus capitis superior muscle and obliquus capitis inferior muscle (OCI) (15). Many reports revealed that there were soft tissue connections from the suboccipital muscles to the cervical spinal dura mater through the posterior atlanto-occipital and atlanto-axial interspaces, known as the MDB. Since the existence of the RCPmi-MDB was first described, many hypotheses have been proposed (5,10,16–20). Subsequently, another similar connection, which originated from the RCPma and the OCI, respectively, was also described as the MDB. In this situation, the RCPma- and OCI-MDB entered the epidural space directly through the atlanto-axial interspace and terminated at the posterior cervical spinal dura mater (21–24). A dense fascial structure in the nuchal ligament (NL) was reported in the midline between the NL and the posterior cervical dura mater at the atlanto-occipital and atlanto-axial intervals (25,26). Zheng et al. found the presence of two novel ligaments, namely the ‘to be named ligament’ and the vertebro-dural ligament, linking the atlas, the axis and the NL with the cervical dura mater (27).
The functional significance and pathology mechanism of MDB have been extensively discussed. Many studies have presumed that the MDB was related to chronic cervicogenic headaches (7,11,20,26,28–30) and have suggested it may provide an anatomic and physiological basis for cervicogenic headaches (2,8,14,31). Whenever pathological changes occurred in these deep muscles, improper forces may be transmitted from the MDB to the pain-sensitive spinal dura, resulting in cervicogenic pain. Alix and Bates suggested that the spinal dura’s potential role in cervical chronic headache might be the result of its being innervated by the C1–C3 spinal nerves and projecting to the trigeminal nucleus, where it may gather painful inputs from the head, and the MDB might also apply direct traction to the pain-sensitive spinal dura through the foramen magnum (7). Elliott noted that the RCPmi with chronic cervicogenic pain contained significant amounts of fatty infiltration, which suggested a relationship between suboccipital musculature and symptoms of chronic headaches (9,16,32).
In this study, the measurement and morphological analysis of the RCPmi between the headache and control group were processed. The results showed that the RCPmi had significantly undergone more hypertrophy in the headache group than in the control group. Additionally, the male’s RCPmi was larger than the female’s in the headache group. These findings illustrated that the chronic headache patients of males suffered from more hypertrophy of the RCPmi. It was also suggested that RCPmi hypertrophy might be one pathogenesis of the chronic headache, even though the interrelationship of cause-and-effect was unclear.
The ICHD-3 has been released and the main etiologies of headache include nerve, haemorrhage, infection, trauma, and medication (33) etc. Furthermore, one of the headache classifications is that the headache attributes to cerebrospinal fluid (CSF) pressure. Zheng et al. (27) suggested that the MDB may influence the circulation of CSF. A pulse may be generated whenever pathological changes occur in the RCPmi, and is transmitted to the spinal dura mater through the MDB, resulting in a change to negative pressure within the subarachnoid space. The chronic headache may be caused by changes in the circulation of CSF whenever improper changes occurred in the RCPmi. This muscle in the suboccipital region was one of the forces contributing to the circulation of CSF, resulting in chronic headaches (27,34). Our hypothesis may be an explanation as to why morphological changes in RCPmi occur in chronic headache patients.
It is important to recognize that there were a number of limitations to this study, one of which was that we only chose to measure and analyze the RCPmi and that the MDB may be formed by the RCPmi and/or RCPma and/or OCI. Future studies should focus on the correlations between RCPma and OCI and how they relate to chronic headaches. Additionally, this was not a longitudinal study to establish a more accurate morphological correlation between RCPmi and the chronic headache.
Conclusions
Based upon our study, a pathogenesis for chronic headaches may be proposed. It is believed that hypertrophy of the RCPmi may lead to chronic headaches. If this is true, knowledge of the changes in the RCPmi may be an important guide to future physical therapy treatments for patients with chronic headaches.
Clinical implications
The RCPmi of the suboccipital region showed that chronic headache patients suffered from significant hypertrophy of this muscle. RCPmi hypertrophy might be one of the forces affecting the normal circulation of CSF, resulting in chronic headaches. Physical therapy may be an appropriate treatment for patients with chronic headaches.
Footnotes
Acknowledgments
The authors thank all participants. We would also like to thank the 403 Affiliated Hospital of Chinese PLA General Hospital for helping with image collection and Dr. Yan Li of Mclean Hospital, Belmont, MA, USA, for helping with language editing.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Natural Science Foundation of China (grant number 31571234) and the Liaoning Province Natural Science Funds, China (grant number 2014023017).