
Abstract
Aims
This study aims to investigate the resting-state functional connectivity (rs-fc) of the right frontoparietal network (rFPN) between migraineurs and healthy controls (HCs) in order to determine how the rFPN rs-fc can be modulated by effective treatment.
Methods
One hundred patients and 46 matched HCs were recruited. Migraineurs were randomized to verum acupuncture, sham acupuncture, and waiting list groups. Resting-state functional magnetic resonance imaging data were collected before and after longitudinal treatments. Independent component analysis was applied in the data analysis.
Results
We found that migraineurs showed decreased rs-fc between the rFPN and bilateral precuneus compared with HCs. After treatments (real and sham), rFPN rs-fc with the precuneus was significantly reduced. This reduction was associated with headache intensity relief. In order to explore the role of the precuneus in acupuncture modulation, we performed a seed-based rs-fc analysis using the precuneus as a seed and found that the precuneus rs-fc with the bilateral rostral anterior cingulate cortex/medial prefrontal cortex, ventral striatum, and dorsolateral prefrontal cortex was significantly enhanced after treatment.
Conclusion
Our results suggest that migraineurs are associated with abnormal rFPN rs-fc. An effective treatment, such as acupuncture, may relieve symptoms by strengthening the cognitive adaptation/coping process. Elucidation of the adaptation/coping mechanisms may open up a new window for migraine management.
Keywords
Introduction
Migraine, a disabling chronic brain disorder, has become an important public healthcare and social issue due to its high prevalence, large medical burden (1), disabling effects (2), and serious reduction in quality of life (3). Nevertheless, many questions regarding its pathophysiology remain unclear. An improved understanding of the mechanisms underlying migraine and the modulating effects of treatment will open up new and promising avenues for the discovery of its causes, as well as the development of new therapeutic methods.
Despite its high prevalence and social burden, treatments for migraine are far from satisfactory (4). Previous studies showed that acupuncture may achieve its therapeutic effect by enhancing the human body’s self-regulation/healing process, and both verum or sham acupuncture can significantly relieve migraine headache intensity and frequency (5,6). Although the mechanism underlying acupuncture is complex, studies have demonstrated that non-specific effects (including attention, cognition, and expectation) play important roles (7). As a result, acupuncture treatment can be used as a useful treatment tool in order to investigate the underlying neural physiopathology of migraine.
Recently, investigators have begun to explore the functions of individual brain regions of interest as well as the neural networks involved in migraine (8–12) and have found that the brain structure and function of migraineurs differ significantly from those of healthy individuals. These differences may result from their reaction to pain, light, and smell, or as an adaptive response to repeated pain (stressor) attacks (13,14).
More recently, accumulating evidence has suggested that resting-state functional connectivity (rs-fc) may be a valuable tool for understanding brain networks (15). One such brain network is the right frontoparietal network (rFPN), which plays an important role in cognitive control and top-down modulation (16), and has been reliably identified by independent component analysis (ICA) (17). For instance, previous studies suggested that pain and cognition interact reciprocally (i.e., pain can negatively influence cognitive performance, while cognition can significantly modulate our pain experience) (18,19). In addition, studies also show that attention can significantly influence pain experience through a top-down mechanism, and many studies demonstrated that distraction can reduce pain experience (20).
Recently, studies have shown that migraineurs are associated with impaired rFPN rs-fc (21,22). Therefore, this study aims to investigate: 1) the rFPN rs-fc between migraine patients (during the interictal period when they were free from headache symptoms) and matched healthy controls (HCs); and 2) how longitudinal acupuncture, which is an effective treatment, can modulate rFPN rs-fc in migraineurs. We hypothesize that migraineurs will be associated with altered rFPN rs-fc in order to adapt/cope with repeated headache attacks, while an effective non-pharmacological treatment can further modulate the adaptation/coping process.
Materials and methods
We briefly describe the experimental procedures below. Please also see previously published studies (23) for more details on the experimental procedure. The data have been used in previous studies investigating the functional connectivity of periaqueductal gray (PAG) changes between migraineurs and HCs, as well as the modulating effect of acupuncture. In this study, we used ICA in order to investigate the rFPN rs-fc difference between migraineurs and HCs and how an effective treatment can modulate the rFPN rs-fc. These results have not been reported before.
Participants
The Ethics Committee of the 1st Teaching Hospital of Chengdu University of Traditional Chinese Medicine approved all of the study procedures. The experiment was performed in accordance with approved guidelines. This study was then registered on ClinicalTrials.gov (NCT01152632, 27 June 2010). Patients (n = 100) and HCs (n = 46) were enrolled from the outpatient department of the 3rd Teaching Hospital, local advertisements, or the Chengdu University of Traditional Chinese Medicine campus. All participants signed a written consent form. Recruitment started in June 2011 and ended in November 2013.
Migraine without aura patients
Migraineur inclusion criteria were as follows: 1) 17–45 years of age (to improve demographic homogeneity) and right-handed; 2) matched the diagnosis of migraine without aura (MwoA) based on the International Classification of Headache Disorders, 2nd Edition (ICHD-II) MwoA criteria (24); 3) had not received any prophylactic headache medicine or acupuncture treatment in the past 3 months; 4) had experienced migraine for at least 6 months; and 5) had at least one headache attack per month in the past 3 months. Exclusion criteria included: 1) alcohol or drug abusers; 2) pregnant or lactating women; 3) suffered from psychiatric, neurologic, cardiovascular, respiratory, or renal illnesses; 4) had any other type of headache or a history of head trauma with loss of consciousness; 5) magnetic resonance imaging (MRI) contraindications such as claustrophobia; and 6) acupuncture contraindications such as excessive bleeding.
Healthy controls
Right-handed individuals aged between 17 and 45 years who were free from headache and other chronic pain conditions were recruited for this study as HCs. Each subject underwent a review of their medical history evaluation, physical examination, hepatic function, renal function, and routine analysis of blood, urine, and stool in order to exclude organic disease carriers. Individuals with abnormal test results or a history of head trauma with loss of consciousness, pregnancy, or lactation were excluded.
Study design
The total observation period for MwoA patients in this study was 8 weeks. After screening, all MwoA patients were randomized into five groups: verum acupuncture (VA) groups 1, 2, and 3 (VA1, VA2, and VA3), a sham acupuncture (SA) group, and the waiting list (WT) group. All patients were blinded to the group allocation. In this study, we included three VA prescriptions in order to better represent different acupoint selection strategies (25). Weeks 1–4 constituted the baseline phase, during which patients recorded baseline headache diaries. Weeks 5–8 constituted the intervention phase, during which patients in treatment groups received verum or sham acupuncture. All patients continued recording headache diaries during this treatment period. In addition, MRI scans were applied at the end of the fourth and eighth weeks for the migraine patients. All MwoA patients were migraine-free for at least 72 hours at the time of the MRI scan. HCs received only the baseline MRI scan (Figure 1).
Study flow chart.
Interventions
Two licensed acupuncturists administered all acupuncture treatments. Acupoint and non-acupoint selection were similar to those in our previous randomized controlled trials (6). Acupoints selected in VA1 included Yanglingquan (GB34), Qiuxu (GB40), and Waiguan (SJ5). VA2 acupoints included Xiyangguan (GB33), Diwuhui (GB42), and Sanyangluo (SJ8). VA3 acupoints included Zusanli (ST36), Chongyang (ST42), and Pianli (L16). SA acupoints included non-acupoints 1, 2, and 3 (NAP1, NAP2, and NAP3) (Figure 2).
Acupoint locations.
All acupoints and non-acupoints were punctured bilaterally using disposable needles. The needles were inserted perpendicularly at a penetration of 5–15 mm and were gently twisted, lifted, and thrust at an even amplitude, force, and speed to acquire deqi sensation (deqi sensation is a complex feeling including soreness, numbness, heaviness, distention, or dull pain at the site of needle placement) (26) in all treatment groups. The MwoA patients in acupuncture groups (AGs) received 20 treatments (30 minutes each) over a 4-week period: once per day for 5 weekdays followed by a 2-day break. Acupuncture or SA treatment was not performed on HCs and migraineurs in the WT group.
MwoA patients were instructed and agreed not to take any regular medications for migraine treatment. In cases of severe pain, ibuprofen (300 mg per capsule with sustained release) was allowed as a rescue medication.
Outcome measures
The clinical outcomes included headache intensity (visual analog scale (VAS) of 0–10) and frequency (number of migraines separated by pain-free intervals of at least 48 hours) in the past month obtained from the headache diary. The metrics obtained were consistent with the guidelines of the International Headache Society (IHS) for Clinical Trials in Migraine (27). In addition, the self-rating anxiety scale (SAS) and self-rating depression scale (SDS) were applied in order to assess the MwoA patients’ emotional status (28,29).
MRI data acquisition
MRI data were acquired with a 3.0 T magnetic resonance scanner (Siemens 3.0 T Trio Tim, Munich, Germany) with an eight-channel head coil at the West China Hospital MRI center. Prior to the functional run, a high-resolution structural image for each subject was acquired using a three-dimensional MRI sequence with a voxel size of 1 mm3 employing an axial fast spoiled gradient recalled sequence (repetition time (TR) = 1900 ms; echo time (TE) = 2.26 ms; data matrix: 256 × 256; field of view: 256 × 256 mm2). The blood oxygen level dependent (BOLD) resting-state functional images were obtained with echo-planar imaging (30 continuous slices with a slice thickness of 5 mm; TR = 2000 ms; TE = 30 ms; flip angle: 90°; total volumes: 180; in-plane resolution: 3.75 × 3.75 mm2; matrix size: 64 × 64; field of view: 256 × 256 mm2). Subjects were instructed to stay awake and remain motionless during the scan with their eyes closed.
Data analysis
Clinical data analysis
The clinical variables were analyzed using SPSS16.0 software (SPSS Inc., Chicago, IL). A threshold of p < 0.05 (two-tailed) was applied. Continuous variables were presented as the mean (standard deviation) with 95% confidence intervals. Categorical variables were described as n (percentage). χ2 was applied for categorical variable comparisons. For continuous variables, paired t-tests were applied for within-group comparisons, two-sample t-tests were applied for two-group comparisons, and one-way analysis of variance was applied when there were more than three groups.
ICA for resting-state functional MRI data
Resting state data were processed using FMRIB Software Library (FSL) and Analysis of Functional NeuroImages, software (AFNI) following the same processing steps (pipeline) described previously (17). Previous studies suggested ICA to be a reliable method for analyzing rs-fc, particularly for the attention and control networks (30,31).
Preprocessing of functional images included removal of non-brain structures, motion correction, temporal bandpass filtering at 0.01–0.1 Hz, spatial smoothing (6 mm full-width at half-maximum Gaussian kernel), and eight-parameter nuisance signal (global signal not included (32)) extraction. Similarly to a previous study (17), in order to co-register functional MRI (fMRI) images to a standard space, functional images were first registered to each individual’s high-resolution T1 anatomical scan and further registered to the Montreal Neurological Institute 152 (MNI152) template using affine transformations with 12 degrees of freedom (33,34).
Probabilistic ICA at low dimensionality (20 components) was performed (MELODIC and FSL (35)) in order to derive the group’s (n = 190) resting-state networks. Spatial correlations between our group-level networks and the template networks derived from 1414 healthy subjects (17) were calculated. The group-derived network that showed the highest spatial overlap with the rFPN in the template network was assigned to the rFPN.
Then, a dual-regression (36) analysis was applied. Using the rFPN as spatial regressors in a general linear model (GLM), we were able to extract the temporal dynamics associated with each spatial map. The resulting time courses served as temporal regressors in a GLM in order to generate subject-specific maps of the whole brain for each subject. Finally, group analyses were performed using whole-brain subject-specific network maps from the second GLM. The results represent the strength of the rs-fc for each voxel with the rFPN. A two-sample t-test and paired t-test were conducted in order to compare the between-group and within-group differences.
In addition, we also applied multiple regression analyses on migraine patients in order to explore the association between baseline functional connectivity and the corresponding migraine intensity as measured by VAS, as well as the association between pre- and post-treatment functional connectivity changes and corresponding VAS changes in all treatment groups, including age, gender, disease duration, SAS, and SDS as non-interest covariates. A threshold of z > 2.3 and p < 0.05 corrected was applied.
Seed-based functional connectivity
Using ICA analysis, we found that the precuneus plays an important role in the modulation of acupuncture. In order to further explore the modulation process, we performed a seed-based rs-fc analysis using the precuneus as a seed. The fMRI data were preprocessed using Data Processing Assistant for Resting-State fMRI (DPARSF) software (available at: http://rfmri.org/DPARSF). The fMRI images were slice timing and head motion corrected, co-registered to the respective structural images for each subject, segmented, regressed out eight-parameter nuisance signal (including six rigid body motion, white matter and cerebrospinal fluid signal), normalized using structural image-unified segmentation, and then re-sampled to 3-mm cubic voxels. After linear detrending, data were filtered using a typical temporal bandpass (0.01–0.08 Hz) in order to remove low-frequency noise (including slow scanner drifts) and the influences of higher frequencies reflecting cardiac and respiratory signals. We removed frames with framewise displacement (FD) > 0.5 mm (‘scrubbing’), and one time point before ‘bad’ time points and two time points after ‘bad’ time points were deleted. Finally, the data were smoothed using a full-width half maximum of 6 mm.
Functional connectivity analysis for individual subjects was carried out in DPARSF by applying a seed-region approach using the right precuneus (2, −62, 50, 3 mm) so that the coordinate represents the peak of the overlap cluster observed in the ICA results. Next, the averaged time course was obtained from the seed and correlation analysis was performed in a voxel-wise manner in order to generate the functional connectivity (FC) map. The correlation coefficient map was converted into a Fisher z-map using Fisher’s r-to-z transform by calling functions in REST (Resting-State fMRI Data Analysis Toolkit, software) to improve normality. Group analysis was calculated with a random effect model using SPM8 (Statistical Parametric Mapping 8, software). We first compared the rs-fc difference between MwoA patients and HCs using two-sample t-tests. Then, we compared the changes in rs-fc differences (post-treatment minus pre-treatment) between AGs (verum + sham) and the WT group in the factorial design module in SPM8. Similarly to previous study (23), a threshold of voxel-wise p < 0.005 (uncorrected) and p < 0.05 family-wise error corrected at cluster level was applied for all of the analyses.
Results
One hundred and fifty patients were screened, of which 100 patients were recruited for this study. Forty-six age- and gender-matched HCs were also recruited. Eighty-eight patients participated in the first fMRI scan and 81 patients participated in the second. Seven patients did not participate in the second fMRI scan due to scheduling conflicts (two in VA1, two in VA2, one in VA3, and two in the SA group). Of the 81 patients who participated in the two MRI scans, nine patients were excluded from the data analysis due to incomplete scans (lack of resting-state MRI or T1 anatomy; three in V1, one in V2, two in V3, two in the SA group, and one in the WT group) (Figure 1).
Baseline characteristics
Baseline characteristics of migraine without aura patients (subjects finished the two scans with completed data) in different groups and healthy controls.

χ2 test was applied for gender comparison, one-way analysis of variance was applied for the rest of the comparisons among VA1, VA2, VA3, SA, and WT groups; **χ2 test was applied for gender comparison, two-sample t-tests were applied for the rest of the comparisons between MwoA patients and HCs.
HC: healthy control; MwoA: migraine without aura; VA: verum acupuncture; SA: sham acupuncture; SAS: self-rating anxiety scale; SDS: self-rating depression scale; WT: waiting list; CI: confidence interval.
Clinical outcomes
Clinical outcomes before and after treatment in different groups.
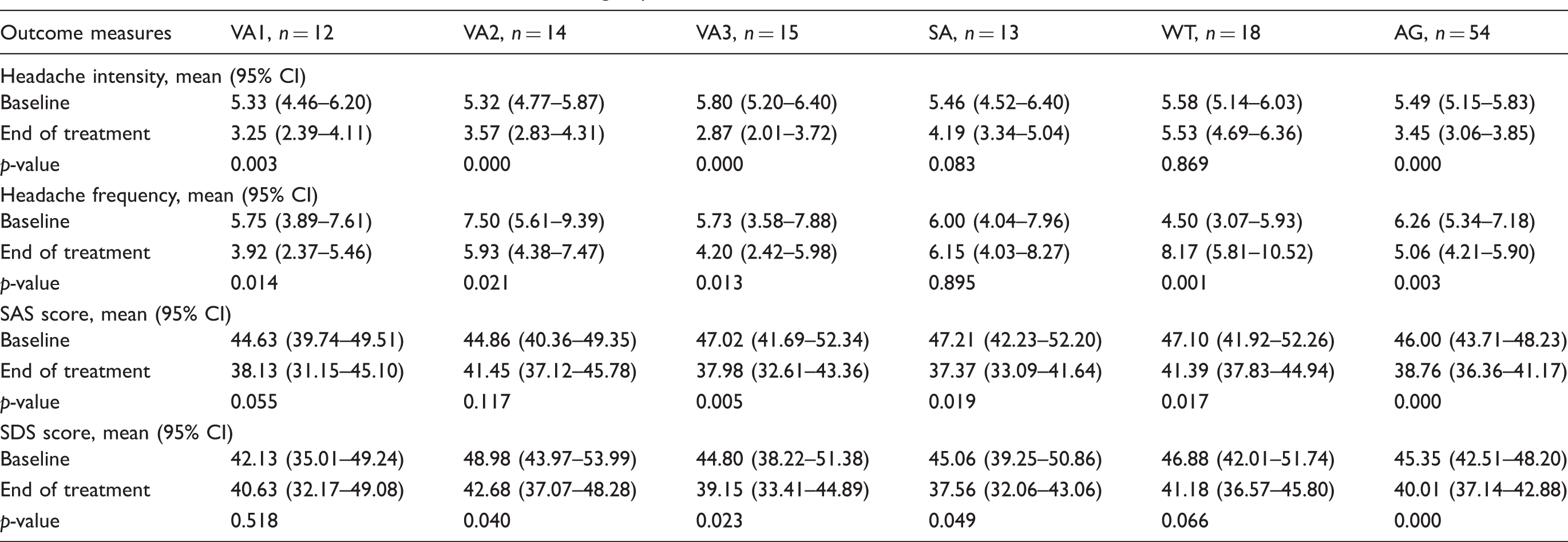
Paired t-tests were applied for comparisons in each group.
AG: acupuncture group, including both verum acupuncture and sham acupuncture; VA: verum acupuncture; SA: sham acupuncture group; SAS: self-rating anxiety scale; SDS: self-rating depression scale; WT: waiting list; CI: confidence interval.
ICA results
As expected, ICA analysis including all subjects/scans has produced a rFPN, which mainly covers the right dorsolateral prefrontal cortex (DLPFC), ventrolateral prefrontal cortex (VLPFC), bilateral inferior/superior parietal lobules, medial prefrontal cortex (MPFC), insula, and left cerebellum (Figure 3 and Table 3). This component is consistent with findings from previous studies (39).
Right frontoparietal network revealed by independent component analysis in this study. Comparisons of the therapeutic effects between different groups. One-way analysis of variance was applied for the comparisons between the VA1, VA2, VA3, SA and WT groups; **two-sample t-tests were applied for the comparisons between MwoA patients and HCs. AG: acupuncture group; HC: healthy control; VA: verum acupuncture; SA: sham acupuncture; SAS: self-rating anxiety scale; SDS: self-rating depression scale; WT: waiting list; CI; confidence interval.

Compared with HCs, MwoA patients showed significantly decreased rFPN rs-fc with the bilateral precuneus, lingual gyrus, middle temporal gyrus, and superior temporal gyrus; left fusiform and secondary somatosensory cortex (S2); and right cerebellum, inferior occipital gyrus, inferior temporal gyrus and cuneus (Figure 4 and Table 4). Regression analysis showed that the rFPN rs-fc with the bilateral precuneus, rostral anterior cingulate cortex (rACC)/MPFC, and left superior frontal gyrus was positively associated with migraine headache intensity (VAS) at the baseline. The rFPN rs-fc of the right inferior temporal gyrus was negatively associated with headache intensity (Figure 4 and Table 4).
rFPN resting-state functional connectivity (rs-fc) results. (a) MwoA showed reduced rFPN rs-fc with the precuneus at baseline compared with HCs. (b) rFPN rs-fc between the precuneus and medial prefrontal cortex/rostral anterior cingulate cortex was associated with headache VAS at baseline. (c) Reduced rFPN rs-fc with the precuneus due to acupuncture treatment (verum + sham). (d) The greater reduction of rFPN rs-fc with the right precuneus was associated with greater headache intensity relief. A threshold of z > 2.3 and p < 0.05 was applied. The right frontoparietal network resting-state functional connectivity (independent component analysis). AG: acupuncture group; G: gyrus; HC: healthy control; Inf: inferior; L: left side; MwoA: migraine without aura; Mid: middle; PCC: posterior cingulate cortex; R: right side; rFPN: right frontoparietal network; MIN: Montreal Neurological Institute coordinate space; MPFC: medial prefrontal cortex; pgACC: perigenual cingulate cortex; Sup: superior; S2: secondary somatosensory cortex; VAS: visual analog scale.

Paired t-tests showed that after longitudinal treatment (real and sham), the rFPN rs-fc with the right precuneus and left middle frontal gyrus was significantly reduced; the rFPN rs-fc with the bilateral posterior cingulate cortex was significantly increased (Figure 4 and Table 4). Regression analysis showed that after treatment, the decrease of rFPN rs-fc with the bilateral precuneus, right paracentral gyrus, and postcentral gyrus was positively associated with a decrease in headache intensity (Figure 4 and Table 4).
In the WT group, we found that the rFPN rs-fc with the left inferior frontal gyrus (peak MNI coordinates: −52, 30, 8; cluster size: 351) and bilateral MPFC (peak MNI coordinates: 0, 44, 28; cluster size: 273) was significantly reduced; the rFPN rs-fc with the middle temporal gyrus/angular gyrus (peak MNI coordinates: −52, −68, 38; cluster size: 208) was significantly increased in MwoA patients (second time minus first time). The comparison between the acupuncture treatment (real and sham; post- minus pre-treatment) and the WT group showed a significant difference in the left cerebellum (peak MNI coordinates: −6, −46, −30; cluster size: 163) and right middle frontal gyrus (peak MNI coordinates: 38, 6, 46; cluster size: 123). In addition, we also compared the rFPN rs-fc change (post- minus pre-treatment) between SA and WT groups. The results showed a significant difference at the right precuneus (peak MNI coordinates: 24, −66, 26; cluster size: 205), right posterior cingulate cortex (peak MNI coordinates: 6, −60, 18; cluster size: 87), right cuneus (peak MNI coordinates: 8, −80, 40; cluster size: 35), and left cuneus (peak MNI coordinates: −4, −76, 26; cluster size: 20).
Seed-based rs-fc analysis results
We found that the right precuneus plays an important role in the pathophysiology of migraine, specifically finding: 1) reduced rs-fc between the rFPN and the right precuneus in MwoA patients as compared with HCs; 2) the rs-fc between the rFPN and right precuneus was associated with headache intensity in baseline MwoA patients; and 3) the decrease of rFPN rs-fc with the right precuneus was positively associated with a decrease in headache intensity due to acupuncture treatment. In order to further explore the role of the right precuneus in the pathology of migraine and its role in treatment, we applied a functional connectivity analysis using the peak of the overlapped cluster at the right precuneus (2, −62, 50, 3 mm) as the seed. We found that, compared with HCs, MwoA patients showed reduced right precuneus rs-fc with the left precuneus, supramarginal gyrus, and inferior temporal gyrus. After longitudinal acupuncture treatment (verum + sham), MwoA patients showed increased right precuneus rs-fc with the bilateral rACC/MPFC, ventral striatum, middle/inferior occipital gyrus, cuneus, DLPFC and cerebellum, and left VLPFC and right superior temporal gyrus (Figure 5 and Table 4).
Precuneus resting-state functional connectivity (rs-fc) results. (a) MwoA showed reduced precuneus rs-fc with the supramarginal gyrus and inferior temporal gyrus compared with HCs. (b) MwoA patients showed increased right precuneus rs-fc with the bilateral rACC/MPFC, ventral striatum, DLPFC, and VLPFC due to acupuncture treatment (verum + sham). A threshold of voxel-wise p < 0.005 and p < 0.05 family-wise error corrected was applied.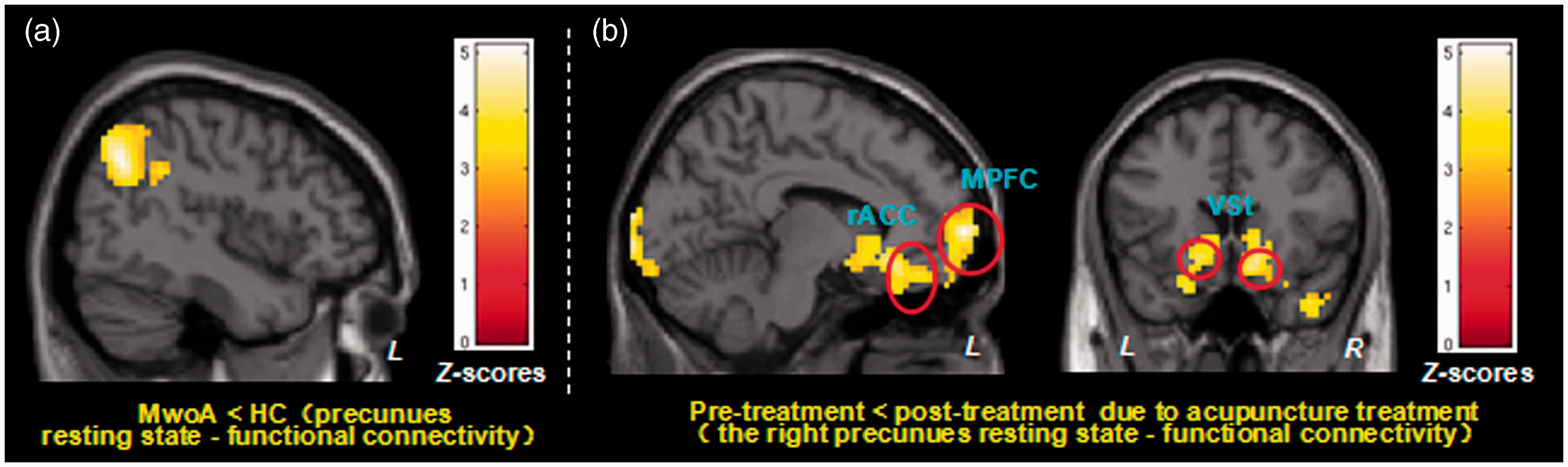
Discussion
In this study, we found that MwoA patients showed reduced rFPN rs-fc with the bilateral precuneus during the interictal period compared with HCs. The rFPN rs-fc between the MPFC/rACC and precuneus was positively associated with headache intensity in MwoA patients at baseline. Interestingly, acupuncture (both real and sham), could significantly reduce rFPN rs-fc with the precuneus. Greater headache intensity relief was associated with greater reduced rFPN rs-fc with the right precuneus. Seed-based functional connectivity analysis (using the right precuneus as the seed) showed that longitudinal acupuncture treatment significantly enhanced the precuneus rs-fc with the MPFC/rACC, ventral striatum (40), and DLPFC/VLPFC (41,42).
A previous study suggested that the left frontoparietal network corresponds strongly to cognition–language paradigms, while the rFPN corresponds strongly to perception–somesthesis–pain (39). Thus, in this study, we only focused on the rFPN. Our results are partly consistent with previous studies in which investigators found impaired rFPN rs-fc in MwoA patients (21,22). In a previous study, Xue and colleagues (21) found that migraineurs (n = 23) showed increased rFPN rs-fc in the middle frontal gyrus and anterior insula. In another study, Russo and colleagues (22) found that MwoA patients (n = 14) had reduced rFPN rs-fc with the middle frontal gyrus and dorsal anterior cingulate cortex compared to HCs. The differences in rFPN rs-fc changes in migraineurs between our study and previous studies may not necessarily be contradictory, as we believe that these differences reflect the complexity of the neural physiopathology of migraine (43).
Studies have suggested that key regions of the rFPN, including the VLPFC, DLPFC, and the parietal gyrus (39), are involved in the cognitive control of pain, and that all of these regions have direct connections with the brain regions involved in affective (i.e., anterior cingulate cortex, MPFC, and amygdala) and sensory (i.e., primary somatosensory cortex (SI) and S2/insula) pain process components (41,42). We found that MwoA patients showed reduced rFPN rs-fc with the precuneus, which is associated with reduced headache intensity. In a previous study, investigators divided the precuneus into three sub-regions based on the rs-fc patterns: the anterior, central, and posterior precuneus. The precuneus region in our study is predominantly located in the central precuneus, which is connected to the dorsolateral/dorsomedial prefrontal and multimodal lateral inferior parietal cortices, suggesting a cognitive/associative brain function (44). Our results are consistent with previous studies showing that the precuneus is closely connected with the rFPN both anatomically and functionally (44,45).
The precuneus is a key node in the default mode network (DMN) (39), a brain network that is associated with self-referential processing (46,47) and mind-wandering (48), whereas the rFPN plays an important role in attention, memory processes, and cognitive control (16). We thus speculate that the reduced rs-fc between the rFPN and the precuneus in migraine patients before treatment may represent the brain’s self-compensatory adaptation/coping responses to continued attacks of migraine (20,49,50). Specifically, paying attention to pain (51) results in more suffering, while distraction (52) from pain results in a less painful experience. The body may automatically apply a distraction strategy as a natural response in order to avoid suffering.
Interestingly, we found that longitudinal acupuncture treatment could further reduce rFPN rs-fc with the right precuneus, and that reduced right precuneus–rFPN rs-fc was associated with migraine headache intensity reduction. Previous studies suggested that expectation, attention, and reappraisal are crucial components of the non-specific effects of treatments (41,42,53). In addition, studies have also shown that the non-specific effects play important roles in acupuncture’s treatment of chronic pain (54–56). Taken together, our results suggest that acupuncture may relieve headache intensity by enhancing the self-compensatory adaptation/coping process. This finding is consistent with a previous brain imaging study of cognitive–behavioral therapy in fibromyalgia showing that, rather than reducing pain responses in patients with fibromyalgia, cognitive–behavioral therapy increases access to executive regions for the reappraisal of pain (57).
Results from the seed-based functional connectivity analysis, showing the altered right precuneus resting-state functional connectivity in MwoA as compared with healthy controls and the pre- and post-treatment resting-state functional connectivity differences across patients.

HC: healthy control; G: gyrus; DLPFC: dorsolateral prefrontal cortex; Inf: inferior; L: left side; MIN: Montreal Neurological Institute coordinate space; MPFC: medial prefrontal cortex; MwoA: migraine without aura; Mid: middle; R: right side; rACC: rostral anterior cingulate cortex; rFPN: right frontoparietal network; Sup: superior; VLPFC: ventrolateral prefrontal cortex.
We also found increased precuneus rs-fc with the VLPFC, DLPFC, and ventral striatum/nucleus accumbens. A previous study (62) showed that pain relief could produce negative reinforcement through activation of the mesocorticolimbic reward-valuation circuitry. Lee and colleagues found that acupuncture needles associated with a treatment context could produce greater fMRI signal increases at the ventral striatum as compared to pure needle stimulation that is associated with a treatment context (63). A more recent human fMRI–positron emission tomography study (64) found increased endogenous opioid release at the nucleus accumbens during pressure pain. Taken together, our results suggest that the cognitive control network, reward system, and descending pain modulatory network may all be involved in the modulating process of acupuncture treatment.
In summary, we believe that our findings suggest the existence of top-down coping/adaptation modulation in MwoA patients during migraine-free phases. Specifically, the brains of migraineurs have formed a reduced rFPN–precuneus connectivity mechanism in order to prepare for/cope with the potential pain attack, which may reflect the application of a top-down distraction strategy. Interestingly, we also found that the non-pharmacological treatment of acupuncture can: 1) further enhance this coping mechanism by further reducing the rFPN–precuneus rs-fc; and 2) increase precuneus rs-fc with the MPFC/rACC and ventral striatum, which may indicate the involvement of the descending pain modulation system and reward system. These results together may suggest a central pathway (including the DLPFC, VLPFC, parietal lobules, precuneus, ACC/MPFC, and PAG) underlying the acupuncture treatment of chronic pain. The elucidation of this pathway/mechanism may shed new light on our understanding of the self-regulation/coping process and facilitate the development of new treatments for migraine.
There are several limitations to this study: 1) the sample size in each acupuncture treatment group is small, which prevents us from testing clinical outcome differences between different acupuncture treatment groups. In addition, the dropout rate is relatively high; however, we would like to emphasize that the reasons for dropout do not seem to be associated with treatment response. In addition, the aim of this study is to explore the neural physiopathology of migraine, so using the treatment as a mediator was intended to enable the investigation of how an effective treatment can modulate the rFPN rs-fc, rather than to test the efficacy of acupuncture itself. Nevertheless, future studies with large sample sizes are needed in order to elucidate the specific treatment effects of acupuncture treatment. 2) Although the patients were migraine-free for at least 72 hours at the time of the MRI scan, they could have been in different stages with regards to the upcoming migraine attack (65). Studies that investigate the rs-fc changes at different phases of migraine and the modulating effects of acupuncture and other treatments will further enhance our understanding of the physiopathology of migraine. 3) We do not have a second fMRI scan for the matched HCs. Thus, we cannot completely rule out the notion that the results were observed due to drift effects over time or habituation to the scanning environment. Further studies with better controls are needed in order to replicate the results of this study.
Conclusion
Migraine is associated with abnormal rFPN rs-fc during the interictal period. The reduced rFPN rs-fc with the DMN is associated with lower headache intensity, suggesting an adapting/coping cognitive mechanism in migraine patients. An effective treatment, such as acupuncture, may achieve symptom relief by strengthening this cognitive adapting/coping mechanism.
Clinical implications
Migraineurs might be associated with abnormal right frontoparietal network resting-state functional connectivity. An effective treatment, such as acupuncture, may relieve symptoms by strengthening the cognitive adaptation/coping process. Elucidation of the adaptation/coping mechanism may open up a new window for migraine management.
Footnotes
Acknowledgements
The authors would like to thank Wei Qin, Jinbo Sun, Jixin Liu, Minghao Dong, Qizhu Wu, and Xiaoqi Huang from Xidian University and the West China Hospital of Sichuan University for their assistance in this study. ZL, FZ and LL contributed equally to this article. Study protocol and design: FL, FZ, YL, and QG; acquisition of data: ML, LL, TG, FW, YG, MD, and JY; analysis and interpretation of data: ZL, NM, JH, FZ, and JK; and drafting of the manuscript: ZL, LL, SS, NM, and JK. All authors reviewed the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: grants from the State Key Program for Basic Research of China (2012CB518501), the National Natural Science Foundation of China (No.81590950, No.81273154, and No.81473602), the Program for New Century Talents in the University of Ministry of Education of China (2013) and the Youth Foundation of Sichuan Province (No.2012JQ0052); JK is supported by R01AT006364 (NCCIH/NIH), R01AT008563 (NCCIH/NIH), R21AT008707 (NCCIH/NIH), and P01 AT006663 (NCCIH/NIH).