
Abstract
Objective
Episodic cluster headache is characterized by abnormalities in tyrosine metabolism (i.e. elevated levels of dopamine, tyramine, octopamine and synephrine and low levels of noradrenalin in plasma and platelets.) It is unknown, however, if such biochemical anomalies are present and/or constitute a predisposing factor in chronic cluster headache. To test this hypothesis, we measured the levels of dopamine and noradrenaline together with those of elusive amines, such as tyramine, octopamine and synephrine, in plasma of chronic cluster patients and control individuals.
Methods
Plasma levels of dopamine, noradrenaline and trace amines, including tyramine, octopamine and synephrine, were measured in a group of 23 chronic cluster headache patients (10 chronic cluster ab initio and 13 transformed from episodic cluster), and 16 control participants.
Results
The plasma levels of dopamine, noradrenaline and tyramine were several times higher in chronic cluster headache patients compared with controls. The levels of octopamine and synephrine were significantly lower in plasma of these patients with respect to control individuals.
Conclusions
These results suggest that anomalies in tyrosine metabolism play a role in the pathogenesis of chronic cluster headache and constitute a predisposing factor for the transformation of the episodic into a chronic form of this primary headache.
Introduction
Cluster headache (CH) is a trigeminal autonomic cephalalgia (TAC) characterized by unilateral, excruciating, severe headache attacks. Most of the patients present with episodic CH in which the painful attacks occur with a variable frequency, daily or weekly during the active periods and then subside in remission periods. The active periods last from weeks to months and occur in a periodic manner. A minority of patients present with chronic cluster headache (CCH) in which the bouts occur continuously from at least one year from the onset. However, CCH may also develop from episodic CH (ECCH). In this case, patients present with a progressive prolongation of the active periods associated with the absence of the remission periods (1).
The pathogenesis of CH is unknown; however, increasing evidence, generated mainly from our laboratory, shows that profound alterations of tyrosine (Tyr) metabolism may have an intriguing role in the occurrence of this primary headache (2,3). Tyr is the amino acid precursor for the synthesis of catecholamines and elusive amines. The Tyr hydroxylase enzyme synthesizes dopamine (DA) and noradrenaline (NE) whereas Tyr decarboxylase results in the production of elusive amines such as tyramine (TA), octopamine (Oct) and synephrine (Syn) (4). Both enzymes are regulated by mitochondrial activity. In conditions of low mitochondrial function, the activity of the decarboxylase increases, whereas that of the hydroxylase enzyme decreases (5–7). Elusive amines, previously almost ignored in human pathology for many reasons (difficulty of their measurement in biological fluids, unknown receptors for elusive amines), are now considered to play a significant role in synaptic transmission within the central nervous system (CNS) acting as neuromodulators. Neuromodulators are chemicals released from the neuron that act to modify the action (increasing or decreasing their activity) of coexisting neurotransmitters that, however, do not change the excitability of postsynaptic cells in the absence of the neurotransmitters DA, NE and 5-HT. Furthermore, elusive amines are agonists of the recently discovered trace amine associated receptors (TAARs) (8–10). TAAR1 is an inhibitory presynaptic receptor in catecholaminergic neurons and as such modulates the synaptic release of catecholamines in many subcortical structures. TAAR1 is widely distributed in the hypothalamus and in all the connected structures, such as the amygdala, thalamus, limbic system and centers of the pain matrix (11). The hypothalamus plays an important role in the pathogenesis of CH as its inhibition, through implantation of a stimulator in the posterior region, may reduce the number of bouts in CH patients (12).
The nature of the hypothalamic dysfunction and its role in the pathogenesis of CH is unknown. Studies have demonstrated that the levels of DA and TA, Oct and Syn are very high in plasma and platelets of CH patients in remission and active periods, whereas those of NE are significantly lower than those of control individuals (2,3,13). We suggested that if the same biochemical abnormalities are present in the hypothalamus and other centers of the pain matrix, these biochemical anomalies may be involved in the pathogenesis of episodic CH (2).
The pathogenesis of chronic CH and the process that leads the episodic form to the chronic one are completely unknown. It is unknown whether the anomalies in the synthesis of catecholamines and elusive amines, found in ECH patients, play a role in the pathogenesis of CCH. In order to explore this hypothesis, we assessed the plasma levels of NE, DA, TA, Oct and Syn in a group of CCH patients and control groups.
Patients and methods
Demographic and clinical characteristics of control and CH patient groups.

CH: cluster headache.
A group of 16 healthy individuals was used as the control group (Table 1). All control participants were free from headaches, diabetes, hypertension or other relevant pathological disorders. After an informed consent was obtained, the levels of DA, NE, TA, Oct and Syn were measured in the plasma of all participants.
Peripheral venous blood (20 ml) was drawn from the antecubital vein at 9 a.m. from participants after 10 minutes of resting in the supine position, within four hours after the last bout. The blood was drawn by an expert operator and collected into tubes with citrate as an anticoagulant. The blood was centrifuged at 3500 rpm for 15 minutes to obtain poor platelet plasma (PPP). One ml of PPP was used to measure the amines. The analysis was performed using high-performance liquid chromatography (HPLC) as previously described (15).
Elusive amine and catecholamine plasma levels were first tested for normality using the Shapiro-Wilk test and for equality of variance by Levene’s test. All groups displayed a parametric distribution with equal variance; therefore, the differences between groups were tested using the independent samples t-test. Evaluation of differences between the CCH and ECCH patients was performed for plasmatic levels of DA, NE, TA, Oct and Syn. Pearson’s correlations were performed between concentration levels and also with clinical variables assessed during a clinical interview. Differences in the plasma levels of DA, NE, TA, Oct and Syn between males and females were also evaluated. The results were expressed as the mean + SD and the level of significance was assumed for a p value <0.05.
Results
Plasma levels of catecholamines and elusive amines of controls and cluster headache patients.

Results are reported as mean values ± SD. P value was obtained by unpaired t-test.
Plasma levels of catecholamines and elusive amines (mean ± SD) of chronic CH patients evolved from the episodic form and those with the chronic form ab initio.
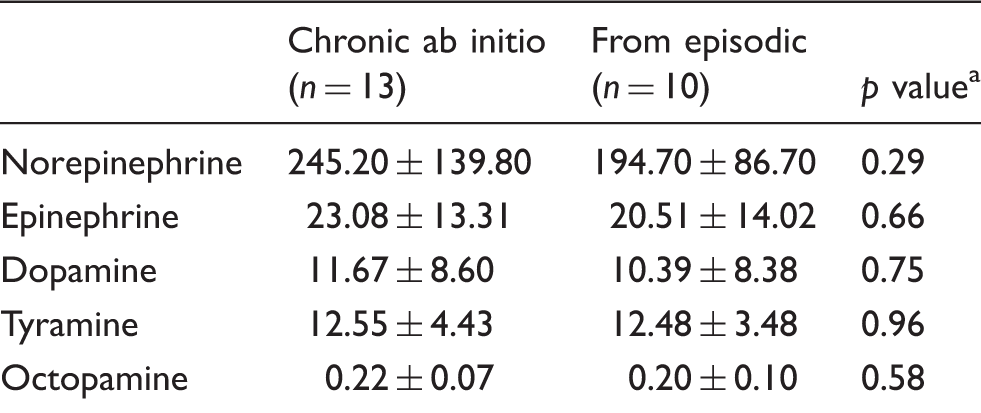
CH: cluster headache. aUnpaired t-test. P value was obtained by unpaired t-test.
Discussion
This study clearly shows that abnormalities of Tyr metabolism occur in CCH patients. In comparison to control individuals, these patients have very high plasmatic levels of DA and NE along with TA, whereas those of Oct and Syn are significantly lower. The high DA and TA levels are suggestive of increased decarboxylase activity since this enzyme converts Tyr in TA and levodopa (L-DOPA) in DA. This confirms the results found in ECH patients in remission and active periods and suggests that there occurs, as in a migraine, a metabolic shift toward an increased decarboxylase enzyme activity (16). The origin of the anomalous high plasma levels of DA and TA, as reported in the episodic cluster, is likely a consequence of the activation of the sympathetic autonomic system since TA and DA are released from the nerve endings surrounding the trigeminovascular bed of the CNS (17,18). In addition, increased functionality of the dopaminergic system is more than probable. In fact, it has been reported that the abnormal 24-hour prolactin secretion and the blunted response to thyrotropin-release hormone found in CH patients occur as a consequence of the increased synthesis and release of DA from the dopaminergic tuberoinfundibular system, which is the main inhibiting factor of prolactin release from the pituitary gland (19,20). The neurons of this system are located in the arcuate and periventricular nuclei of the hypothalamus. It is well known that an anomaly of hypothalamic function plays a pivotal role in the pathophysiology of CH, a result in line with numerous neuroendocrinological, neuroimaging and pharmacological studies (21–23). Although the nature of this abnormal function of the hypothalamus in CH is uncertain, the abnormally high levels of TA may, at least in part, offer an explanation. TA, like Oct and Syn, is a neuromodulator regulating the physiological function of dopaminergic synaptic clefts (24). If the high levels of TA, here found in plasma, are also present in the CNS, TAAR receptors, particularly TAAR1, are stimulated. These receptors are located abundantly in the hypothalamus and in other interconnected dopaminergic and noradrenergic brainstem nuclei. The high levels of TA together with the elevated levels of DA may affect the functionality of TAAR1 receptors, resulting in changes of their inhibitory function on the presynaptic catecholaminergic neurons (25). These alterations may affect the release of DA in the competent synaptic clefts of all dopaminergic fibers connected to the hypothalamus and of the synaptic clefts within the hypothalamus itself. This biochemical dopaminergic dysregulation may contribute to the abnormal hypothalamic function in CH patients.
The elevated level of NE in chronic CH patients is an unexpected result and not in line with those previously reported in ECH patients in which such levels are reported to be lower than those found in control individuals. This may be because the synthesis of NE is dependent on mitochondrial energy shown to be reduced in CH (26). One possible explanation for the abnormally high levels of NE in our patients is that, as in chronic migraine, there occurs an interaction between TA and its TAAR1 receptors. As described above, TA, like β-phenylethylamine (β-PEA) and DA, is a potent agonist of TAAR1 receptors. It is possible that, as hypothesized in chronic migraine, the abnormal high TA availability in DA and NE circuitries results in anomalies of TAAR1 functionality (24). Changes in TAAR1 inhibitory function may determine alterations in NE in the synaptic clefts of the neurons of the noradrenergic and sympathetic system and its release into the circulation from the sympathetic endings.
The significant low levels of Oct and Syn here found in CH are in contrast to those showed in platelets and plasma of ECH patients published in our previous study (2). The reasons for this biochemical discrepancy are unclear; one possibility is that the DA hydroxylase enzyme activity that converts TA into Oct is reduced because of impairment of mitochondrial functions demonstrated in the muscles and brain of ECH patients (27). It is possible that the mitochondrial function is further reduced in CCH resulting in an accumulation of TA along with reduced synthesis of Oct and Syn.
In conclusion, our data suggest the occurrence of a biochemical abnormality of Tyr metabolism in CCH patients: Tyr decarboxylase enzyme activity is increased, resulting in an accumulation of TA and DA whereas the plasma levels of Oct and Syn are significantly low, suggesting that the hydroxylase enzyme activity is reduced. The high levels of noradrenaline are probably a consequence of abnormal functionality of TAAR1s, which are the presynaptic inhibitory receptors affecting catecholamine release in the synaptic clefts of the hypothalamus and pain matrix. Our hypothesis is that the high levels of DA and TA may constitute the biochemical abnormal milieu that causes the hypothalamic and pain matrix dysfunctions in CCH patients. The high levels of NE and low levels of Oct and Syn may be the cause of the vegetative symptoms that accompany the CH attacks as these amines are neurotransmitters and neuromodulators of the sympathetic system (28,29). It is possible that treatment(s) that normalize(s) this abnormal biochemical background of CCH may prevent the transformation of ECH to the chronic form and may treat the CCH itself.
This study has some limitations. The first is that all patients considered were undergoing pharmacological treatments, the impact on our results of which is unknown. However, in previous studies, similar Tyr anomalies were found in patients in remission (without treatments) and active (in treatment) periods suggesting that the treatments may have had a limited influence. A prospective study enrolling CCH patients out of therapy is required to confirm our results. The second limitation is that we have not contemporarily enrolled ECH patients in this study, allowing for comparison with previous studies in this patient group. The third limitation is that we did not evaluate the levels of the biomarkers considered during the bout. We do not know if the metabolism of Tyr further changes during the painful attack.
Clinical implications
Plasma levels of products of tyrosine (Tyr) metabolism are altered in chronic cluster headache (CCH) patients with respect to those of control individuals. The very high level of dopamine (DA) and tyramine (TA) found in our patients provides a possible explanation of the hypothalamic dysfunctions and related neuroendocrine abnormalities previously described in CH sufferers. Higher plasma levels of noradrenaline (NE) together with lower levels of octopamine (Oct) and synephrine (Syn) found in CCH patients, unlike those reported in episodic CH patients, may be associated with chronicity of a CH. The possible dysfunction of the trace amine associated receptor TAAR1, due to the high levels of TA, may explain the high levels of the neurotransmitters. The synthesis of pharmacological agents modulating the function of TAAR receptors may constitute a future avenue for a better comprehension of CH pathophysiology, the process involved in its chronicity and eventually its treatment.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was partially funded by the F.I.C.E.F. (Italian Foundation for Headache Research, Naples, Italy).