
Abstract
Objective:
The pathogenesis of chronic migraine (CM) remains largely unknown. We hypothesized that anomalies of tyrosine metabolism, found in migraine without aura (MwwA) patients, play an important role in the transformation of MwwA into CM, since the increase in the number of MwwA attacks is the most predisposing factor for the occurrence of CM.
Methods:
To test our hypothesis we measured the plasma levels of dopamine (DA), noradrenaline (NE) and trace amines, including tyramine (TYR) and octopamine (OCT), in a group of 73 patients with CM, 13 patients with chronic tension-type headache (CTTH) and 37 controls followed in the Headache Centers of the Neurology Departments of Asti, Milan and Vicenza hospitals in Italy.
Results:
The plasma levels of DA and NE were several-fold higher in CM patients compared with control subjects (p > 0.001). The plasma levels of TYR were also extremely elevated (p > 0.001); furthermore, these levels progressively increased with the duration of the CM.
Conclusions:
Our data support the hypothesis that altered tyrosine metabolism plays an important role in the pathogenesis of CM. The high plasma levels of TYR, a potent agonist of the trace amine associated receptors type 1 (TAAR1), may ultimately down-regulate this receptor because of loss of inhibitory presynaptic regulation, therein resulting in uncontrolled neurotransmitter release. This may produce functional metabolic consequences in the synaptic clefts of the pain matrix implicated in CM.
Introduction
Chronic migraine (CM) is a form of headache in which the frequency of attacks progressively increases to daily or nearly-daily headache attacks. Until recently, there was no universal consensus for the optimal definition and the diagnostic criteria for CM, particularly when patients use large amounts of acute drugs that lead to medication overuse (MO) (1–4). The major requirements for diagnosis of CM include the presence of a headache for at least 15 or more days per month and a history of previous typical migraine attacks, with a portion of the current attacks being classified as migraine without aura (MwwA). The different classification systems are not coincident, although the most recent criteria proposed by the International Headache Society (IHS) (3) better concur with Silberstein and Lipton criteria (1) than the original ICHD-2 criteria for CM (2), as shown by Bigal et al. (4). The prevalence of CM is quite high, being estimated in the range of 1.4% to 2.2%. Furthermore, 3% of episodic migraine sufferers occur in the general population, and 14% in clinical cohorts may develop CM every year (5,6). CM imposes a relevant burden on individuals and on society, including a reduced health-related quality of life, increasing medical costs and limitations in daily functioning during occupational, social and family activities (7–10).
The pathogenesis of CM is largely unknown. The natural history raises the possibility that CM constitutes a complication and/or transformation of episodic migraine when the frequency of the attacks increases over time. This complication is more frequent when other risk factors, such as female gender, psychological and social aspect, comorbid conditions and particularly MO of analgesics or other acute drugs to abort headache attacks are present in the same patients (7,8). It is reasonable to hypothesize that aspects of the pathogenesis of MwwA play an important role in the transformation of MwwA into CM.
Biochemical studies performed during this last decade have shown that abnormalities in tyrosine metabolism occur in patients affected by MwwA (11). Tyrosine is the amino acid precursor for the synthesis of catecholamines, including dopamine (DA), nordrenaline (NE) and elusive amines, such as tyramine (TYR), octopamine (OCT) and synephrine (SYN). The enzymes that govern the production of catecholamines and elusive amines are tyrosine hydroxylase and tyrosine decarboxylase, respectively (12).
The trace or “elusive” amines have a similar molecular structure to that of catecholamines and are present in minute amounts in areas of the central nervous system (CNS), including the hypothalamus, limbic areas, extrapyramidal system and nuclei of the brain stem (13). The physiological role of these amines was unknown for decades until a new class of G protein-coupled receptors, known as trace amine-associated receptors (TAARs), was discovered in multiple mammalian tissues including humans. In the CNS, TAARs are located in subcortical structures that also have higher concentrations of elusive amines (14). Among the TAARs, TAAR1 is the most abundant receptor in the CNS. Recent studies have shown that TYR and OCT are agonists of TAAR1 and act as neuromodulators of DA and NE receptors (15). A neuromodulator is a chemical released from a neuron that acts to modify the action (increase or decrease) of a coexisting neurotransmitter that, however, does not change the excitability of post-synaptic cells in the absence of the neurotransmitter. Catecholamines and elusive amines play an important role in the physiology and pathology of the CNS because they modulate many subcortical structures with specific functions, including the regulation of pain threshold (16).
Previous studies, including ones from our laboratory, have demonstrated that the levels of OCT and SYN were notably high in plasma and platelets of MwwA patients compared with those of control subjects (17,18). In the same patients platelet levels of DA were increased (19), while NE levels were decreased (20,21). These data strongly suggest that a metabolic abnormality of tyrosine metabolism could explain the increased levels of neuromodulators and unphysiological levels of neurotransmitters that are found in patients with MwwA. This breakthrough in the understanding of MwwA may also play an important role in the pathogenesis of CM.
There is a paucity of information about the possible biochemical abnormalities of neurotransmitters and neuromodulators in CM. In particular, it is unknown if the same anomalies of tyrosine metabolism in MwwA are present in CM patients, and if these alterations affect the evolution of episodic MwwA to CM or the occurrence of CM per se. To explore this hypothesis, we assessed the plasma levels of DA, NE, TYR and OCT in control subjects and patients with CM or chronic tension-type headache (CTTH).
Patients and methods
A sample of consecutive patients presenting at the Headache Centers of Neurology Departments in three Italian hospitals (Vicenza, Milan and Asti) from January 15, 2011, to March 15, 2011, were enrolled in our study. The inclusion criteria consisted of a history of chronic headaches lasting one year or more and a diagnosis of CM or CTTH. A diagnosis of CTTH was made according to ICHD-2 criteria (2). The diagnosis of CM included patients classified according to appendix criteria of the International Headache Society (IHS). Also the presence of MO was assessed based on recently revised criteria proposed in the same paper (3). Although the diagnosis of CM using the aforementioned criteria requires the absence of MO, we first made the diagnosis of CM and later identified if a given patient also met the criteria for MO (i.e. CM + MO). This criteria recommendation was suggested in Manack et al. (6). After the blood sampling, analgesic and acute antimigraine drugs were suspended in all patients, thereafter submitted, in day-hospital regimen, to hydration and prophylactic antiepileptic therapy (valproate or topiramate) for CM patients and mainly amitriptyline for CTTH patients.
Study population. No differences were found comparing mean age of CM, CTTH and control subjects.

CM: chronic migraine; CTTH: chronic tension-type headache; SD: standard deviation.
The blood was centrifuged at 3500 rpm for 15 minutes to obtain poor platelet plasma (PPP). One ml of PPP was used to measure the amines. The analysis was performed using high-performance liquid chromatography (HPLC) as previously described (22). The results are presented as the mean + SE. Elusive amine plasma levels were first tested for normality using the Kolmogorov-Smirnov test. All groups displayed a nonparametric distribution; therefore the differences between groups were tested using the Mann-Whitney U-test. The level of significance was set at a p value < 0.05.
Considering the sub-sample of patients with CM only, non-parametric Spearman’s correlations were performed between the levels of DA, NE, TYR and OCT. These values were also correlated to clinical variables that were assessed during a clinical interview (i.e. duration of headache, duration of CM, and number of days/month in which acute drugs were consumed, total number of acute drugs consumed/month, migraine disability assessment (MIDAS) score, number of days with a headache and average headache severity in the last three months). This statistic method was not applied to CTTH and controls because of the limited number of subjects. A two-sample Kolmogorov-Smirnov test was used to assess differences in the plasma levels of DA, NE, TYR and OCT between males and females. Significance was set at p < 0.05 for both correlation analysis and the Kolmogorov-Smirnov test. Linear regression models were used to evaluate the predictability of levels of DA, NE, TYR and OCT based on the aforementioned clinical variables. These variables were entered and removed using the probability of F as criterion (removal if F.10). Collinearity diagnostics were employed. Regression models were required to have condition indices lower than 30 and, for each predictor, tolerance levels higher than 0.20 and a variance inflation factor (VIF) lower than 5.
Results
Main clinical characteristics of CM and CTTH patients.
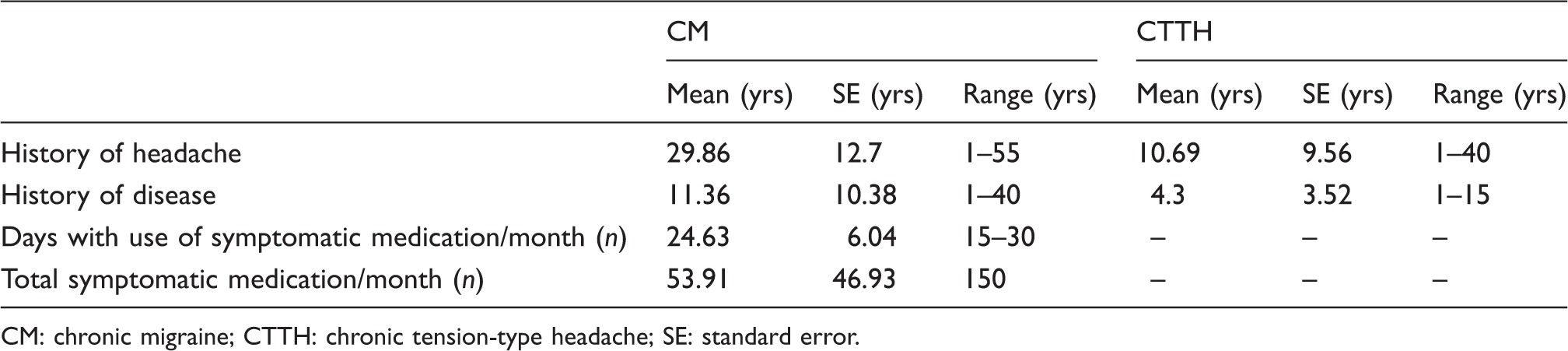
CM: chronic migraine; CTTH: chronic tension-type headache; SE: standard error.
Mean values (ng/ml) ± standard errors (SE) of plasma levels of elusive amines in controls, CTTH and CM subjects.

CTTH: chronic tension-type headache; CM: chronic migraine. p values refer to the statistical analysis performed for CM and CTTH patients vs. control subjects (nonparametric Mann-Whitney U test).
Linear regression model.

SE: standard error; CM: chronic migraine; MIDAS: migraine disability assessment; VIF: variance inflation factor. Dependent variable: TYR: tyramine. ap < 0.05.
Discussion
Based on previous findings in patients with MwwA, the aim of this study was to ascertain possible anomalies in tyrosine metabolism in CM sufferers and to verify if this underlies transformation of MwwA into CM. In addition, we included a group of CTTH patients because the pathogenesis of this form of chronic headaches is completely unknown. In particular it is not known if CTTH and CM share similar pathogenic aspects.
Our results show that complex abnormalities in tyrosine metabolism are present in CM patients. DA and NE plasma levels are notably high in CM patients compared with control subjects. These results are only partially in line with those reported in MwwA patients in that only DA levels were reported to be elevated while NE was reported to be reduced.
Two current hypotheses can explain the anomalies in MwwA patients. One hypothesis is that the abnormal levels of DA and NE are due to polymorphism(s) of the gene that regulates the function of dopamine β-hydroxylase activity. Indeed, polymorphisms have been shown to occur in MwwA, and this genetic anomaly causes a reduction in the transformation of DA in NE leading to an accumulation of DA and reduced synthesis of NE (23). A second hypothesis is that stress, which constitutes a precipitating factor for migraine attacks, causes a release of NE from the autonomic endings of the sympathetic nervous system innervating the vessels followed by an increasingly spillover of DA (24) due to rapid decline of NE availability. However, our findings of high levels of NE suggest that the catecholamine abnormalities found in CM require alternative explanations.
Additionally, the plasma elusive amine profile of CM differs from that reported in MwwA patients. Previous studies from our laboratory have shown that MwwA patients have TYR levels in the normal range, whereas levels of OCT and SYN (not measured in this study) are elevated. In the present study we show the TYR plasma levels are markedly elevated in CM patients and those of OCT only slightly elevated when compared with controls.
We have previously hypothesized that a metabolic shift of tyrosine metabolism occurs in migraine resulting in increased synthesis of elusive amines due to an increase in decarboxylase enzyme activity (25,26). This shift may be consequent to reduced mitochondrial activity. It should be noted that the hydroxylase and decarboxylase enzyme activities require different amounts of energy. The hydroxylase activity requires a large and efficient energy supply, whereas the decarboxylase is activated at a lower level of mitochondrial activity (27). In support of this hypothesis, many studies have shown that platelets, muscles and the CNS of migraine patients have reduced mitochondrial functions probably originating from genetic abnormalities (26). This energetic defect worsens as the number of migraine attacks increases over time. It has been demonstrated that by-products of free radical reactions, such as iron anions, are generated in the CNS during migraine attacks, and that they increasingly accumulate in the neurons of many nuclei when the number of headache attacks are frequent as in CM (28). Based on this evidence, we suggest that an important shift of tyrosine metabolism underlies the abnormal high plasma levels of TYR in CM patients because tyrosine decarboxylase converts tyrosine into TYR. Our finding that CM duration predicts high levels of TYR is in line with this hypothesis. In fact, it is possible that the progression over time of this headache further decreases the efficiency of mitochondrial function, producing a greater shift toward the decarboxylation of tyrosine and the reduction in the activity of the hydroxylase that coverts TYR into OCT. This hypothesis also explains why the levels of OCT are not increased to the extent of TYR in our CM patients. Although no clear correlation was found between the plasma levels of elusive amines and the number of days in which acute drugs were consumed by CM patients, it cannot be excluded that MO influences the plasma levels of TYR in CM patients.
We hypothesize that the high levels of TYR and its interaction with the TAAR1 receptor may be the key to understanding our results in CM patients. The TAARs are a new class of G-protein coupled-receptors that are present in many biological tissues in mammals. In the human CNS, TAARs have been found in the amygdala, raphè magnus, locus coeruleus, limbic, extrapyramidal, cerebellar, and other structures of the brain stem. TAAR1 is widely distributed in the dopaminergic system, including the ventral tegmental area (VTA), and in the limbic and noradrenergic circuitries of the brain stem (29). TAAR1 is a presynaptic inhibitory receptor that regulates the release of catecholamines in the synaptic clefts of the CNS. Tyramine and β-phenyletylamine (β-PEA) are potent agonists of TAAR1 (30). One hypothesis is that an abnormal increase in TYR availability in DA and NE circuitries results in TAAR1 dysfunction, therein causing release of DA and NE from activated presynaptic terminals. Another possibility is that the continuous stress due to the daily pending headache attacks may contribute to higher NE levels in CM with respect to MwwA.
A dysregulation of DA and NE systems may occur in CM patients, given that TYR, DA and NE are released in the circulation from sympathetic nerves and high levels of TYR, DA and NE are also present in the CNS (31,32). In support of this hypothesis, a recent study utilizing functional magnetic resonance imaging (MRI) demonstrated that CM patients show a significant reduction in the function of TGA. This abnormality persisted even when the patients were free from MO (33). As mentioned above, TAAR1and D2 receptors are densely distributed in the TGA and limbic structures, suggesting that variable levels of TYR and DA may affect their functions (29).
In conclusion, our results clearly demonstrate that tyrosine metabolism is altered in CM patients and suggest that the high levels of TYR may play a significant role in the transformation of episodic MwwA into CM. Although these results require confirmation in population based-samples studies, they raise the possibility that treatments normalizing the dopaminergic and noradrenergic systems may constitute a useful strategy in the treatment of CM patients.
In contrast to our results in CM patients, we observed that tyrosine metabolism is normal in CTTH patients. Therefore the pathophysiology and adequate treatment of this primary headache remains a mystery.
Clinical implications
Plasma levels of tyramine (TYR), dopamine (DA) and noradrenaline (NE) were several-fold higher in chronic migraine (CM) patients compared with control subjects (p > 0.001). TYR plasma levels progressively increase with the duration of the CM. The high plasma levels of TYR, potent agonist of the trace amine-associated receptor 1 (TAAR1), may ultimately down-regulate this receptor because of a loss of inhibitory release on presynaptic function. As a consequence, a massive release of the neurotransmitters in the synaptic clefts of the central nervous system (CNS) may occur. These data support the hypothesis that altered tyrosine metabolism plays an important role in the pathogenesis of CM.
Footnotes
Funding
This research was partially funded by the F.I.C.E.F. Milano foundation.
Conflict of interest
None declared.