
Abstract
Background
In this paper, we describe a cohort of patients with short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT), a rare trigeminal autonomic headache, managed in the outpatient clinic of a tertiary hospital.
Methods
Patients were identified through review of individual records between January 1, 2008 and June 30, 2014.
Results
Fifteen patients were identified (eight males:seven females), with mean age at onset of 49.7 years, mean number of attacks per day of 7.5 and mean attack duration of 54.6 seconds. Pain was mostly orbital, periorbital or temporal. Cranial autonomic signs/symptoms were universally present; one patient reported ipsilateral epistaxis. Two symptomatic cases were identified and treated surgically. Most patients responded to lamotrigine, one to topiramate and another to eslicarbazepine.
Conclusion
Our case series is among the largest reported, with findings similar to others already published, but the first to report epistaxis during SUNCT attack and response to eslicarbazepine.
Background
Diagnostic criteria for SUNCT.

Data from: ICHD-3beta. SUNCT: short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing; ICHD-3beta: International Classification of Headache Disorders, 3rd edition beta (2).
The pathophysiology of SUNCT, similarly to other trigeminal autonomic headaches, is incompletely understood. However, ipsilateral autonomic features suggest both cranial parasympathetic activation and sympathetic hypofunction. These appear to be related to the activation of the trigeminal-autonomic reflex (3). In SUNCT, hypothalamic dysfunction is thought to give rise to activation of hypothalamic-trigeminal connections, resulting in a massive parasympathetic outflow due to central disinhibition of the trigeminal autonomic reflex (4). This hypothesis is supported by functional imaging and deep brain stimulation studies (5–7).
Given SUNCT’s rarity, several cases were reported, but only a few case series have been published. The purpose of this study is to describe clinical characteristics and therapeutic results of SUNCT patients managed in the outpatient clinic of a tertiary referral hospital, and to compare our case series with those previously published. In doing so, we attempt to provide additional epidemiological data that will lead to a more thorough understanding of these patients and better management.
The headache outpatient clinic of Centro Hospitalar do Porto was the first dedicated headache clinic in Portugal, and was started 30 years ago. This is a tertiary referral clinic serving a population of almost 1 million inhabitants. During the screening period, approximately 1000 patients were consulted. Of these, 50 patients were diagnosed with TAC. The high prevalence of TACs is explained by a high level of referral from other neurologists (either from outpatient clinics or from emergency care).
Methods
Individual records of all patients followed in our outpatient headache clinic between January 1, 2008 and June 30, 2014 were reviewed. Only patients fulfilling the ICHDH-3beta SUNCT criteria (2) were included. Demographic and clinical data were retrieved, including diagnostic work-up and treatment response, using a standardized protocol. Data were combined and analyzed using Microsoft Excel 2013®.
Results
SUNCT patient demographic and clinical characteristics.

F: female; M: male; R: right; L: left; O: orbital; T: temporal; SO: supraorbital; CREST: calcinosis, Raynaud phenomenon, esophageal dysmotility, sclerodactyly, and telangiectasia; HTN: hypertension; DM: diabetes mellitus; Dyslip: dyslipidemia; TBI: traumatic brain injury; AVM: arteriovenous malformation; LTG: lamotrigine; ESL: eslicarbazepine; TPM: topiramate; MRI: magnetic resonance imaging; CT: computed tomography.
Pain site (Figure 1) was orbital in three patients (20.4%), supra-orbital in two (13.3%) and temporal in two (13.3%). The remaining patients had the following combinations: orbital and supra-orbital in five (33.3%); orbital and temporal in three (20.4%). The attacks were left sided in eight patients and right sided in seven; none had bilateral or side-shifting attacks.
Pain location.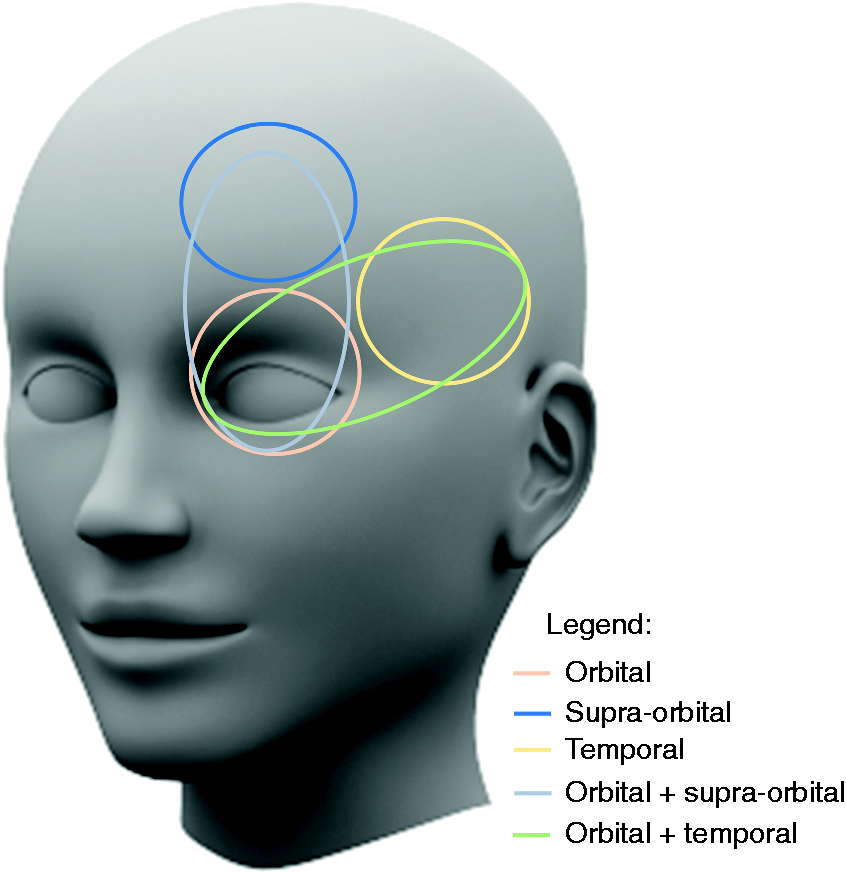
Mean attack duration was 54.6 seconds (SD = 45.4), being <30 seconds in seven patients (46.7%), about 60 seconds in four (26.7%) and about 120 seconds in four (26.7%). The mean number of attacks per day was 7.5 (min = 2; max = 20), and all patients were pain free between attacks.
Besides ipsilateral conjunctival injection and lacrimation, other reported autonomic signs were ipsilateral ptosis (three) and facial sweating (one). One patient reported ipsilateral epistaxis only during some of the attacks, but never between attacks.
Although the majority of attacks were spontaneous, all patients reported triggered attacks: touching the face or scalp (eight), chewing (six) and eating (six). During the attack, all patients reported agitation.
Neurological examination between episodes was normal in all patients except for an ipsilateral ptosis in two patients. All patients were investigated with brain imaging—computed tomography (CT) in two and magnetic resonance imaging (MRI) in the remaining. CT scans did not reveal significant changes and MRI was normal in six patients. In the remaining patients, the MRI revealed ipsilateral trigeminal neurovascular contact in four, unspecific white matter changes in one, cavernous sinus thrombosis associated with an arteriovenous malformation (AVM) in one and a carotid-cavernous sinus fistula in another patient.
Of note, six patients had been previously misdiagnosed with other conditions: three with a temporomandibular joint disorder, two with trigeminal neuralgia and one with chronic sinusitis. All patients had a negative family history for headache.
Regarding management, the two symptomatic cases were surgically treated and have remained headache free since then. In the remaining 13 patients, lamotrigine was the first drug to be introduced, with doses ranging from 75 to 150 mg/day. Of these patients 61.5% (eight of 13) were responders: Four patients were rendered pain free and the other four maintain acceptable control of pain attacks, with <5 attacks per week. In the five patients refractory to lamotrigine, different medical treatments were tried: topiramate, carbamazepine, oxcarbazepine, gabapentin, verapamil, eslicarbazepine, indomethacin and corticosteroids. Two of these five patients entered into spontaneous remission and are now under no medical treatment. Another patient is also under no medical treatment because of the failure of all previous treatments and to a current reduction in pain frequency (<5 attacks per week). One patient attained reasonable control of attack frequency with topiramate 100 mg/day. The other patient was rendered pain free under eslicarbazepine 800 mg/day, but died of an unrelated cause one year later.
Discussion
In this paper, we present a large case series of SUNCT patients. Contrary to the findings of Cohen et al. (6), only a discrete male preponderance was identified. However, age of onset was similar to the aforementioned report. Despite previous reports of familial SUNCT (8), all the patients in our cohort had negative family history.
There was no significant side predominance, and no bilateral or side-shifting attacks were reported. Similarly to previous reports (6), orbital and supraorbital were the most frequently reported pain sites, followed by the temporal region. The duration of attacks was similar to that reported by Cohen et al. (6), but the mean number of attacks per day was considerably lower in our cohort. The majority of attacks were spontaneous, although all patients reported triggered attacks, with no refractory period, similarly to previous reports (1,6). Agitation was a common feature during attacks. All patients had associated cranial autonomic features similar to those already described in other reports. There was, however, a patient who presented with epistaxis during the attacks, with no other known local or systemic disorder that could explain the epistaxis. After initiation of medical treatment, both SUNCT attacks and epistaxis became rare. Although there are several reported cases of epistaxis associated with migraine (9–11), an association with SUNCT has never been reported. The proposed mechanism is vasodilation of internal and external carotid branches induced by trigeminovascular system activation, leading to an increase in blood flow on the vascular plexus of the nasal mucous membrane, predisposing to hemorrhage.
Similarly to other case reports (4,6,12), we found two symptomatic SUNCTs. One was secondary to a cavernous sinus thrombosis associated with an AVM and another to a carotid-cavernous sinus fistula. Both patients had an abrupt onset with frequent attacks per day and poor response to medical treatment, and both experienced complete resolution after directed surgical treatment. Trigeminal neurovascular contact was identified in four patients, similarly to what has been reported by other authors (1,6). None of our patients was submitted to surgery thanks to satisfactory control under medical therapy. Therefore, the significance of this association could not be ascertained.
Sodium channel blockers appear to be the most effective for SUNCT, which raises the possibility of an underlying sodium channelopathy (5). Based on case reports, lamotrigine appears to be the most effective treatment (4). In one review (5) a treatment algorithm was proposed, with lamotrigine as first-line treatment; oxcarbazepine, topiramate and duloxetine as second-line; and carbamazepine, gabapentin, pregabalin, mexiletine and lidocaine patches as third line. Intravenous lidocaine and corticosteroids (oral or intravenous) were considered as transitional therapies. In our cohort, lamotrigine was by far the most effective preventive treatment. Satisfactory pain control was also attained with topiramate in one patient and pain freedom was achieved with eslicarbazepine in another. The latter does not appear to be due to a spontaneous remission given that several other drugs had failed to control the pain attacks and that the patient was rendered pain free in 72 hours. To our knowledge, this is the first description of response to eslicarbazepine in SUNCT.
Conclusions
Our case series is among the largest SUNCT series reported. While most of the clinical characteristics are similar to those already reported, we found no significant male preponderance in our series and the mean number of attacks per day was lower. To our knowledge, this is the first series to report a case of epistaxis associated with SUNCT. Lamotrigine appears to be the most effective treatment, but other medications can also be effective, as eslicarbazepine here reported in SUNCT for the first time.
Clinical implications
Male predominance in short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT) is not clearly established. Epistaxis may be another disautonomic signal accompanying trigeminal autonomic cephalalgia (TAC). Secondary causes of SUNCT syndrome must always be excluded. Lamotrigine is the most effective drug in SUNCT treatment. Eslicarbazepine may be an option in the treatment of SUNCT.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.