
Abstract
Objective
The objective of this review is to describe auditory hallucinations (paracusias) associated with migraine attacks to yield insights into their clinical significance and pathogenesis.
Background
Isolated observations have documented rare associations of migraine with auditory hallucinations. Unlike visual, somatosensory, language, motor, and brainstem symptoms, paracusias with acute headache attacks are not a recognized aura symptom by the International Headache Society, and no systematic review has addressed this association.
Methods
We retrospectively studied patients experiencing paracusias associated with migraine at our center and in the literature.
Results
We encountered 12 patients (our center = 5, literature = 7), 58% were female, and 75% had typical migraine aura. Hallucinations most commonly featured voices (58%), 75% experienced them during headache, and the duration was most often <1 hour (67%). No patients described visual aura evolving to paracusias. Most patients (50%) had either a current or previous psychiatric disorder, most commonly depression (67%). The course of headache and paracusias were universally congruent, including improvement with headache prophylaxis (58%).
Conclusion
Paracusias uncommonly co-occur with migraine and usually feature human voices. Their timing and high prevalence in patients with depression may suggest that paracusias are not necessarily a form of migraine aura, though could be a migraine trait symptom. Alternative mechanisms include perfusion changes in primary auditory cortex, serotonin-related ictal perceptual changes, or a release phenomenon in the setting of phonophobia with avoidance of a noisy environment.
Introduction
Approximately 12% of the United States population suffers from migraine (1), and up to 38% may experience aura (2). Visual phenomena are the most common aura and are a form of organic hallucinations (2). Auditory hallucinations, or paracusias, are the most common hallucination in psychosis, affecting about 70% of schizophrenia patients during the illness course (3). Auditory hallucinations have also been associated with hearing impairment (4) and a variety of neurological disorders, including Parkinson’s disease (5), dementia with Lewy bodies (6), stroke (7), epilepsy (8), narcolepsy (9), and focal brain lesions (10). Although tinnitus has been reported with migraine (11), isolated case studies have also reported paracusias, including auditory verbal hallucinations in the context of headache. Most of these reports, however, lacked clinical detail and information on psychiatric comorbidities, and no comprehensive review has yet addressed the potential association between paracusias and migraine.
In our practice we have encountered patients with headache disorders that have experienced auditory hallucinations in the setting of acute attacks or exacerbations of daily headache. Unlike visual, somatosensory, language, motor, and brainstem symptoms, auditory hallucinations are currently not recognized as an aura symptom by the third edition of the International Classification of Headache Disorders (ICHD-3 beta) (12). By presenting a case series from our center and aggregating literature reports, we aim to characterize this unusual phenomenon associated with migraine, stimulate consideration of paracusias within the clinical spectrum, and speculate about the underlying pathophysiology.
Methods
This study was conducted in two stages. The first retrospectively reviewed charts of patients seen at the Montefiore Headache Center (MHC) in the Bronx, NY, from January 1, 2006 through December 31, 2013. MHC treats a diverse urban patient population, as well as many regional and national referrals. All new patients completed a standardized questionnaire that captured demographic, headache, past medical, social, and family history characteristics (13). Aura, premonitory and associated symptoms, and triggers were recorded. In 2008, the Allodynia Symptom Checklist (ASC) was added (14), as were the Patient Health Questionnaire (PHQ-9) (15) and the Generalized Anxiety Disorder (GAD-7) (16). The majority of patients were evaluated by both a headache fellow and faculty member, and additional testing was undertaken as clinically indicated. Primary headache disorders were diagnosed according to the ICHD-2 (5) in real time, and retrospectively we applied the updated ICHD-3 beta criteria for confirmation.
We applied David’s definition that an auditory hallucination occurs in the absence of external stimulation, is considered real by the individual, and is not under conscious control (17). Since there is disagreement on whether auditory events other than voices (such as hearing tones) should be classified as auditory hallucinations (18), we opted for a broader definition for inclusivity in this review.
By reviewing charts of all MHC patients reporting auditory hallucinations or other auditory phenomena in association with migraine, we compiled available information on participant demographics (age, gender, and ethnicity); detailed descriptions of the paracusias (specific sounds, duration of hallucination, and timing with respect to headache and aura symptoms); headache features (location, laterality, nausea, vomiting, photophobia, phonophobia, osmophobia, aggravation by physical activity, autonomic symptoms, attack triggers); ICHD-3 beta diagnosis; medical and psychiatric history; review of systems with particular attention to any hearing or vestibular complaints; previous preventive, abortive, intravenous, and interventional medication trials; PHQ-9 and GAD-7 scores; investigations (neuroimaging, electroencephalography, and cerebrospinal fluid analysis); and response of both headache and paracusias to therapies.
The second part of the study entailed a literature search completed in December 2013 of the online databases PubMed and Google Scholar to identify additional case reports of auditory phenomena associated with headache. Search terms included the following used singly and in combination: auditory, hallucination, paracusia; each with migraine, headache, and aura. Cases were selected for inclusion only where the presence of auditory hallucination was experienced in close temporal proximity to migraine. Reference lists for all publications identified on the initial search were hand-checked as well. Authors EEM and MSR independently conducted the searches and reviewed all collected references. In order to extract descriptive results from as large a sample as possible, we combined the data from our clinic sample with literature case reports. Our study protocol was deemed exempt by our institutional review board, obviating the need for informed consent.
Results
Of 4238 patients seen at our center during the eight-year time period, seven reported auditory phenomena related to headache, a prevalence of 0.17%. Literature review yielded an additional nine patients experiencing auditory hallucinations in conjunction with headache disorders (19–24). Unlike our clinic cases, most of the case reports lacked detail of headache presentation or patients’ medical and psychiatric comorbidities. To present a more homogeneous patient population, we focused on the 12 patients (MHC = 5, literature = 7) diagnosed with migraine (supplemental file), excluding one patient with post-traumatic headache, one patient with new daily persistent headache, and two patients in the literature without clear diagnoses.
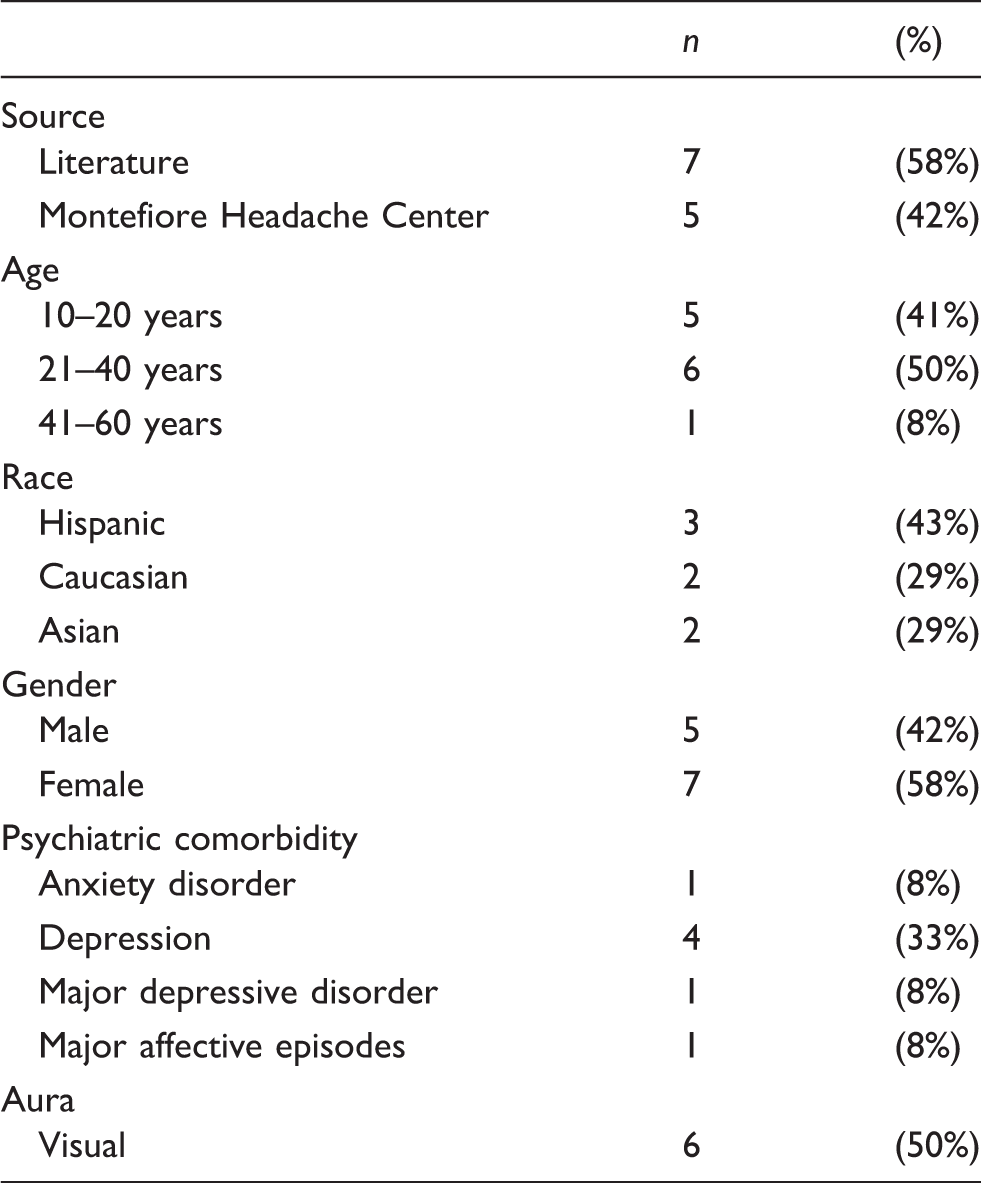
Demographics
Characteristics of patients with primary headache attacks and auditory hallucinations.
Phonophobia and visual aura
Overall, four patients described symptoms of phonophobia during their headache. Half of all patients reported typical visual migraine aura, including spots, lines, and flashes of light. Two patients experienced visual aura prior to headache onset while five experienced visual aura during headache, all of whom also experienced their auditory hallucinations during their headache. Of the two patients experiencing visual aura prior to headache, one patient also had the auditory hallucination before the migraine whereas the other one had her auditory hallucination during the headache.
Character of hallucinations
Half of the patients experienced hearing human voices, with three hearing a single voice and three multiple voices. One patient heard a recognizable voice while the others heard unfamiliar voices. Other paracusias included general background noise such as a refrigerator hum (n = 2), crickets (n = 1), ringing bells (n = 1), repetitive beeping (n = 1), and a hissing noise (n = 1). Only one patient described an evolution of her paracusia during the headache (“hearing hissing noises inside her head, which were initially muffled, but after several repetitions, these noises clearly sounded like the word ‘death’”).
Timing and duration of paracusias
Features of auditory hallucinations in patients with primary headache disorders.

The duration of auditory hallucinations was reported in seven patients, two of whom experienced phenomena lasting less than 10 minutes, and two had a hallucination lasting 10 to 60 minutes. One patient each had hallucinations lasting greater than one hour, “the duration of the headache,” and “nearly constant” but more apparent during the headache phase.
Medical and psychiatric comorbidities
Of the 11 cases with reported medical history, seven patients had no documented medical comorbidities. The remaining five had various comorbidities including hypertension, asthma, and arthritis (supplemental file).
Psychiatric comorbidities were described in six patients. Using all reported history and screening results, four had depression and one had anxiety. One patient was diagnosed with major depressive disorder, and another experienced major affective episodes. One patient had symptoms suggesting schizophrenia or another thought or personality disorder, featuring multiple psychiatric admissions for medication overdose attributed to command hallucinations occurring exclusively during severe headaches (23). None of the remaining cases had evidence of a psychotic disorder.
Diagnostic studies
All 12 patients had at least one reported modality of brain imaging. Three patients had a head computed tomography (CT), all of which were normal. Nine patients received a magnetic resonance imaging (MRI) of the brain, of which six were normal. The abnormal MRIs included one patient with a stable, patchy fluid-attenuated inversion recovery (FLAIR) hyperintensity over the posterolateral aspect of the left cerebral peduncle just below the level of the red nucleus. Another showed an axial FLAIR image with a small, focal, irregular, linear hyperintensity located at the posterior tip of the left putamen along with prominent post-contrast vascular markings extending from the anterior margin of the left trigone toward the left putamen and external capsule (believed to be a deep venous angioma). The third abnormal MRI showed a few scattered hyperintensities within white matter on FLAIR sequences. Four patients underwent routine electroencephalography (EEG) and one patient had 48-hour EEG monitoring, and no events were captured in any case.
Response to treatment
Ten patients were prescribed prophylactic medications. Seven of these patients achieved at least partial relief of headache symptoms with their medication, with efficacy unconfirmed for one other who did not return for follow-up. In cases with treatment success, the course of the paracusias paralleled the headache course: Resolution of headache was associated with resolution of the hallucination and persistence of the headache yielded persistence of the paracusias. The most common successful treatments were propranolol (n = 3), amitriptyline (n = 2), and greater occipital nerve block (n = 2).
Discussion
In an eight-year period, the prevalence of auditory hallucinations among all patients seen at our headache center was 0.17%. This phenomenon is extremely rare in comparison to visual and sensory aura, as well as compared to olfactory hallucinations, which we previously reported in the same population to have a prevalence of 0.66%, almost quadruple that of auditory hallucinations (25).
In our series, auditory hallucinations occurred roughly equally in men and women with migraine, although they were rarely reported in patients with other primary headache diagnoses. The typical hallucination lasted less than 10 minutes, occurred shortly before or simultaneous with the onset of head pain, and included a range of auditory phenomena from human voices to ringing bells to general background noise. In most patients, the course of auditory hallucinations paralleled that of headache following initiation of prophylactic therapy for headache. Based on semiology, timing, and response to headache prophylaxis, we propose that auditory hallucinations in migraine are probably an uncommon but distinctive migraine trait symptom. Though limited, our data indicate that auditory hallucinations may not necessarily be associated with aura, corresponding to the findings regarding visual hallucinations reported by Jürgens et al. (26).
Verbal auditory hallucinations are not uncommon in the general adult population, with a population prevalence between 5% and 28% (27–30), most commonly featuring hearing sentences or words not identified as being self (31), lasting for two to three minutes, occurring approximately every three days, and causing little or no distress (32). In fact, one study found that only 25% of those people with verbal auditory hallucinations carried a diagnosis of psychosis (33), consistent with the predominantly nonpsychotic sample we describe here.
With a prevalence of migraine in the United States at 12% (1), up to 3.4% of people in the United States may coincidentally suffer from migraine as well as auditory hallucinations, absent psychosis. Therefore, it is surprising that in our tertiary center migraine associated with auditory hallucinations was so rare, though this may relate to the retrospective nature of the study and the underreporting of symptoms if infrequent or unintrusive.
Auditory hallucinations are often associated with psychosis but may also manifest in the presence of both affective disorder and anxiety (34). Since more than half of our sample reported a history of depression and anxiety disorders, its presence could be related to psychiatric comorbidity, which ideally would be clarified by longitudinal study (19,35).
The pathophysiology of paracusias in patients with migraine is unknown, though we speculate it may be related to various brain structures and processes that have been implicated in the manifestation of auditory hallucinations in nonpsychotic populations (36). Temporal lobe dysfunction, possibly due to a redistribution of blood flow or ischemia (37), has been implicated in epilepsy, where 3.3% of patients experience auditory hallucinations, increasing to 14% in temporal lobe epilepsy (38), possibly related to hyperfusion of the primary auditory cortex (39).
The brainstem has been implicated in auditory hallucinations, including migraine with brainstem aura that features tinnitus. In patients experiencing migraine with typical aura, brainstem aura is reported at a rate of approximately 10% (40). Though not necessarily associated with migraine, auditory hallucinations have been documented with peduncular lesions, including thalamopeduncular, upper midbrain, and brainstem hemorrhagic infarcts, as well as pontine bleeding with extension rostrally to the midbrain. These authors reported that the hallucinosis were stereotyped, complex, and scenic, with both visual and auditory components. The auditory features varied and included whispering, talking, or screaming human voices (including the patients’ own voices), band music, animal sounds (cows, sheep, dogs, rodents), bells, gunfire, and train sounds. Each of the subjects reported hearing or conversing with other humans in addition to experiencing other environmental sounds (41).
Brainstem abnormalities associated with auditory hallucinations in the presence of headache were reported by Cascino and Adams (42). Three cases, involving a serpiginous enhancing lesion in the lateral wall of the fourth ventricle, an arteriovenous malformation (AVM) in the pontine tegmentum, and a tumor mass in the lower midbrain, were believed to cause auditory symptoms ranging from hearing bells, buzzing, chattering, musical notes, seashell resonance, metallic grinding/banging, and humming. None of these cases, however, reported hearing words, unlike in our series where verbal hallucinations were most common.
We found only one case report of diagnosed brainstem lesion associated with both migraine and auditory hallucination involving human voices to include in our series. Lo et al. (20), described a 22-year-old who had a midbrain lesion believed to contribute to his migraine-related auditory hallucinations. The authors hypothesized that since the patient’s symptoms corresponded to descriptions of peduncular hallucinosis, the lesion reflected a migrainous infarct. They proposed that since the hallucinatory symptoms routinely appeared immediately prior to the patient’s migraine and resolved concomitantly with the migraine symptoms, the loss of brainstem control of the descending cortical processes from the prior infarct was likely responsible for the migraine-related auditory hallucinations (41,43).
Tinnitus has been described as being on one end of a “continuum of complexity” with auditory hallucinations (44). The brainstem is not the only central structure related to the production of tinnitus, and any insult to the auditory pathway from the ear up to the auditory cortex could be responsible (11). Furthermore, Volcy and colleagues suggest that tinnitus in migraine relates to either central sensitization during migraine (making tinnitus an allodynic symptom), or perhaps cortical hyperexcitability (45).
The mechanism for auditory hallucinations during migraine may not relate to the source of tinnitus. Further exploration will be needed to determine whether the mechanism for verbal auditory hallucinations is similar to the mechanism that produces tinnitus. In fact, recent functional magnetic resonance imaging (fMRI) neuroimaging studies of patients with auditory hallucinations have identified multiple areas of activation in both psychiatric and non-clinical samples, including the superior temporal gyri, insula, bilateral inferior frontal gyri, inferior parietal lobule, left precentral gyrus, right cerebellum, and superior temporal pole (46).
In addition to structural abnormalities, auditory hallucinations are common in substance-induced states due to altered neurotransmission in the brain (20). Owing to a central imbalance within the serotonergic system, patients with migraine have been shown to have reduced serotonin available interictally, with the migraine attack correlating with a significant increase in available serotonin in the brain. Consequently, the increasing levels of serotonin are believed to “upregulate” levels of arousal and attention, affecting perception. Tests of auditory perceptual rivalry have supported this hypothesis by demonstrating delayed perceptual switching during interictal periods for individuals with frequent migraine, equivalent to the results of normal participants whose availability of serotonin has been reduced pharmacologically (47).
We additionally propose that the paracusias experienced by our patients may be part of a release hallucination phenomenon, as the high rate of phonophobia (48) leads many patients likely to seek out a quiet environment during their attacks. In an environment of reduced auditory input, such hallucinations may be more likely to manifest. Therefore, future studies should include baseline hearing tests to rule out hearing impairment (intrinsic quiet environments) as a potential nidus for the paracusias experienced by these patients.
Our study has major limitations, most of which are inherent in the retrospective design. We are limited by lack of data on the specific progression of when auditory hallucination occurs to migraine headache onset. We have captured only a small number of patients, though paracusias with headache attacks seem rare and it is the largest study characterizing this phenomenon to date. None of our patients had formal audiometry.
A recent retrospective descriptive study found evidence that specific transitory sensory and neuropsychological symptoms (SNS) are migraine trait symptoms. While their study focused on visual hallucinations, we have identified a smaller subgroup of patients experiencing auditory phenomena with an analogous presentation. To follow up, they suggested a prospective, face-to-face study in order to validate their retrospective study longitudinally to refine the relationships of such symptoms to migraine and aura attacks (26).
Similarly, we propose a case-control study of patients with migraine to prospectively capture other transient symptoms including auditory and olfactory hallucinations to more accurately define their epidemiology, clinical spectrum, and relationships with headache diagnoses, aura, other transient SNS and psychiatric comorbidity. We additionally suggest that headache referral centers using intake questionnaires incorporate queries for nontraditional migraine symptoms such as auditory and olfactory hallucinations to encourage more reports of these phenomena.
Clinical implications
Auditory hallucinations (paracusias) are rarely but distinctively associated with migraine attacks. Paracusias in migraine most commonly feature voices, occur during rather than before headache attacks, are of <1 hour in duration, and remit contemporaneously with headache improvement. Auditory hallucinations may be a migraine trait symptom or relate to perfusion changes in primary auditory cortex, serotonin-related ictal perceptual changes, or a release phenomenon in the setting of phonophobia.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest
EEM has nothing to declare. BMG has served on a scientific advisory board for Kowa Pharmaceuticals America Inc, and Tribute Pharmaceuticals; has received speaker honoraria from Zogenix; receives research support from Allergan Inc, Boston Scientific, and ElectroCore; and receives book royalties from Wiley. SCC has nothing to declare. MSR has received honoraria from the American Headache Society, Prova Education, American College of Physicians, MedLink, North Shore-LIJ Hofstra School of Medicine, and SUNY Downstate College of Medicine, and receives book royalties from Wiley.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.