
Abstract
Neurophysiological investigations have demonstrated that there are unique fluctuations in the migraine brain functional activity between the ictal and interictal periods. Here we investigated the possibility that there are fluctuations over time also in whole brain morphometry of patients affected by episodic migraine without aura (MO).
Twenty-four patients with untreated MO underwent 3T MRI scans during (n = 10) or between attacks (n = 14) and were compared to a group of 15 healthy volunteers (HVs). We then performed voxel-based-morphometry (VBM) analysis of structural T1-weighted MRI scans to determine if changes in brain structure were observed over the course of the migraine cycle.
Interictally, MO patients had a significantly lower gray matter (GM) density within the right inferior parietal lobule, right temporal inferior gyrus, right superior temporal gyrus, and left temporal pole than did HVs. Ictally, GM density increased within the left temporal pole, bilateral insula, and right lenticular nuclei, but no areas exhibited decreased GM density.
These morphometric GM changes between ictal and interictal phases suggest that abnormal structural plasticity may be an important mechanism of migraine pathology. Given the functional neuroanatomy of these areas, our findings suggest that migraine is a condition associated with global dysfunction of multisensory integration and memory processing.
Introduction
Migraine is defined as a recurrent, painful condition of the head with ictal dysfunction that includes headaches accompanied by multisensory symptoms and interictal pain-free periods of variable length between attacks. The diagnosis of migraine is generally based on medical interviews and an objective neurological examination. Paraclinical tests are recommended only if secondary forms of headache are suspected (1). Nonetheless, during the last two decades many research groups have used neurophysiological and neuroimaging techniques to discover functional and structural biomarkers of subtle factors that may predispose individuals to recurrent migraine attacks. Using a variety of neurophysiological methods, researchers have demonstrated that there are significant changes in the bioelectrical activity of the migraineur brain that strongly correlate with the migraine cycle. Notably, deficient short- and long-term habituation/adaptation to many forms of repetitive sensory stimulation was frequently observed between attacks, while central sensitization and normal sensory adaptation was observed during migraine attacks (2,3). Using diffusion tensor (DT) magnetic resonance imaging (MRI), we recently reported that there are dynamic variations in the anatomical microstructure of the thalamus of patients with migraine without aura (MO) during the migraine cycle (4). However, it is unknown if abnormal structural brain plasticity is a characteristic of migraine, and further studies are needed to definitively address this issue.
Voxel-based morphometry (VBM) is a powerful analytical tool that enables semi-quantitative, unbiased evaluation of morphological data from MR images. VBM permits the investigation of region-specific changes in density of gray matter (GM) by averaging results across individuals (5–7). The use of this imaging technique has grown considerably in recent years, because it is highly sensitive to neural changes at the cellular level and thus provides information pertaining to brain microstructure. In vivo temporal changes in brain morphology revealed by VBM are strongly correlated with functional neuroplasticity associated with highly dynamic cortical processes relevant to adaptation and learning. Spine and synapse turnover are more likely responsible for rapid morphometric changes associated with fast-adapting neuronal processes (8,9). VBM is thus well suited to the study of functional disorders of the brain such as migraine (10,11).
There are several reports of GM morphometric changes in migraine patients. The majority show a significant decrease of GM in several areas involved in the transmission of pain (12–20). However, these studies used heterogeneous patient selection criteria, and none of these studies explored the relationship of brain morphological properties to the cyclical recurrence of migraine attacks. Therefore, we decided to determine if there are fluctuations in the morphometry of the whole brain over time in patients affected by episodic MO. We present a high-resolution structural 3T MRI-VBM study comparing GM morphometry of healthy volunteers (HVs) with that of migraineurs without aura during and between attacks.
Material and methods
Participants
Twenty-four consecutive right-handed migraine patients (19 women, mean age 32.3 years) treated at our headache clinic were enrolled and subsequently participated in a comprehensive battery of neuroimaging tests, including morphometric MR imaging. DT imaging (DTI) studies of these patients have already been published (4). Of the 24 participants, 14 (MO) underwent MRI scans during the interictal period, defined as an absence of migraine attacks for at least three days before and after MRI. Ten patients were scanned within a time range of 12 hours before or after the beginning of an attack. In accordance with previous neurophysiological (21–23) and neuroimaging (24) studies, this group of migraine patients were considered to be in the ictal period. For MO patients, inclusion criteria were as follows: no previous history of other neurologic diseases, systemic hypertension, diabetes or other metabolic disorders, connective or autoimmune diseases, and any other type of primary or secondary headache. Our MO patients showed mono/bilateral migraine headaches not always localized on one specific side. In order to avoid confounding effects on neuroplasticity due to pharmacologic treatment, no preventive antimigraine drugs were taken by the study participants during the preceding three months. For those patients experiencing a migraine attack during the scan, no acute antimigraine drugs were allowed until the end of the imaging session. The control group comprised 15 right-handed healthy volunteers (HVs) made up of medical school students and health care professionals of comparable age and gender distribution to the experimental group. Controls did not have any overt medical conditions, personal or family history of migraine or epilepsy, or take regular medication. Female participants were always scanned at mid-cycle. All scanning sessions were performed in the afternoon (4:00–7:00 p.m.).
None of the enrolled individuals had sleep deprivation or ingested alcohol the day preceding the scans. Caffeinated beverages were not allowed on the day of scanning. Further exclusion criteria both for HVs and MO were evidence of brain lesions on structural MRI. All participants received a complete description of the study and granted written informed consent. The ethics review board of the Faculty of Medicine, University of Rome, Italy, approved the project.
MRI
All images were acquired using a Siemens 3T Verio MRI scanner and we used a sagittal T1-weighted image to determine patient and control position. High-resolution T1-weighted three-dimensional (3D) images (176 slices) were acquired with repetition time (TR) = 1900 ms, echo time (TE) = 2.93 ms, slice thickness 1 mm, flip angle = 9 degrees, matrix size = 256 × 256, and field of view (FoV) 260 × 260 giving an in-plane resolution of 0.98 × 0.98 mm for every participant.
Image post-processing
Image data processing was performed on a personal computer using the Statistical Parametric Mapping (SPM8) software package (Wellcome Trust Centre for Neuroimaging, London, UK; http://www.fil.ion.ucl.ac.uk/spm). The image series for each participant was reoriented in order to have the same point of origin (anterior commissure) and spatial orientation. For each group, we generated a template (mean T1) and smoothed the original images (GM and white matter (WM), cerebrospinal fluid (CSF)) to a full width half maximum (FWHM) of 8 × 8 × 8 mm. The final segmented images were obtained using the template and original images as previously calculated; modulated routines were used and hidden Markov random field (HMRF) was fixed at 0.3. Lastly, the GM and WM volume were smoothed with a 12 mm FWHM Gaussian filter for every participant.
Statistical analysis
SPM8 (Wellcome Department of Cognitive Neurology, London, UK) running under Matlab (Mathworks, Sherborn, MA, USA) was used for all statistical analysis. Differences between the patients’ groups’ clinical features were assessed using the one-way analysis of variance (ANOVA) test.
For neuroimagings, we first performed a two-sample t-test to compare the GM volume of each patient group to that of the control group and to assess relative GM atrophy across patient groups. A threshold of p < 0.001 uncorrected for multiple comparisons was applied. As a further step and in order to search for a correlation between regional GM density changes and clinical patients’ features, we performed a multivariate regression model including duration of migraine history and attack frequency as independent variables using a stepwise selection procedure.
Results
Clinical and demographic characteristics of healthy volunteers (HVs) and migraine patients without aura scanned between (MO) and during (MI) the attacks. Data are expressed as means ± SD.
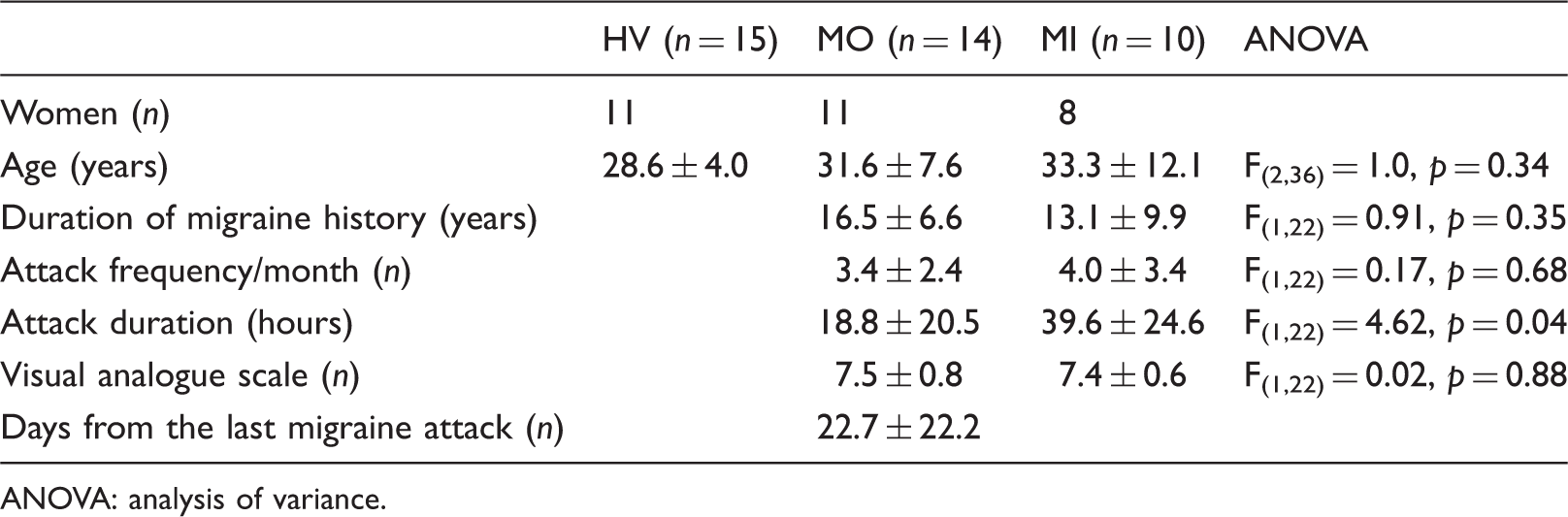
ANOVA: analysis of variance.
Local GM comparison between MO patients scanned between attacks and HVs
Regions of significant gray matter reduction in migraine patients scanned between attacks vs. healthy volunteers using unmodulated images (p < 0.001 uncorrected).

R: right; L: left.
Significant GM density reductions were found in the right inferior parietal lobule, right inferior temporal gyrus, right superior temporal gyrus and left temporal pole. Figure 1 shows these differences as identified by a statistical parametric map.
SPM regions superimposed on a high-resolution T1-weighted scan showing decreased GM density in MO patients scanned between attacks compared with healthy volunteers (p < 0.001 uncorrected). Areas of significant reduced GM density are observed in the right inferior parietal lobule, right temporal inferior gyrus, right superior temporal gyrus, and left temporal pole. SPM: statistical parametric mapping; STG: superior temporal gyrus; GM: gray matter; MO: migraine without aura; IPL: inferior parietal lobule; ITG: inferior temporal gyrus; TP: temporal pole.
Local GM comparison between MO patients scanned ictally and HVs
Regions of significant gray matter increase in migraine patients scanned ictally vs. healthy volunteers using unmodulated images (p < 0.001 uncorrected).

R: right; L: left; NA: not applicable.
Significant GM density increases were found in the right lenticular nuclei, bilateral insula, and left temporal pole. Figure 2 shows these differences as identified by a statistical parametric map.
SPM regions superimposed on a high-resolution T1-weighted scan showing increased GM density in MO patients scanned during the ictal period compared with HVs (p < 0.001 uncorrected). Areas of increased GM density are visible in the left temporal pole, bilateral insula, and right lenticular nuclei. SPM: statistical parametric mapping; GM: gray matter; MO: migraine without aura; LN: lenticular nuclei; INS: insula; TP: temporal pole.
No correlation was disclosed between the duration of migraine history and attack frequency and regions of increased or decreased GM density.
Discussion
The main finding of our study is the observation of a significantly lower GM density within the right inferior parietal lobule, right temporal inferior gyrus, right superior temporal gyrus and left temporal pole in patients scanned between attacks when compared with healthy volunteers. In contrast, no areas showing decreased GM density were detected during the ictal phase, while GM increased within the left temporal pole, bilateral insula, and right lenticular nuclei. Bilateral insula and lenticular nuclei (composed of the putamen and globus pallidus) are brain areas belonging to the pain network and are thought to subserve the sensory-discriminative dimension of pain processing and analgesia (25,26). Their involvement observed only during an attack may reflect a general transient response to pain, as has been shown through other neuroimaging techniques in migraine and in other pain disorders (26–28). The differences in density within temporo-parietal areas are, however, unlikely to be directly related to pain perception. Although several papers have investigated VBM GM morphometric structures of the migraineur brain (15,29–37), our study is the first specifically designed to investigate GM density changes distinctly in ictal and interictal migraine. Although little is known about the neurobiological basis of the physiological and structural changes that occur in GM, we will discuss the possible neurobiological underpinnings of our present data and their potential relevance for migraine pathophysiology.
VBM allows quantitative evaluation of brain morphology, investigating region-specific changes in density of GM by averaging results across patients (6). One of the immense advantages of this MRI technique is the ability to make in vivo observations of temporal changes in brain morphology as a function of adaptation and learning processes (5,10,11). However, the neurobiology of these GM morphometric changes on a microscopic level are still a matter of much debate. Besides providing information about the morphological properties of distinct cerebral areas, VBM also may be sensitive to variations in the cellular composition of the cerebrum. Changes in the cellular structure as a function of learning include variations in the volume of neural and glial cell bodies and their processes, changes in the levels of myelination and the dynamic vascularization of the brain (38). Nevertheless, fast-adapting neuronal processes, such as spine and synapse turnover (8), rather than the relatively slow-evolving mechanisms such as neuronal or glial cell genesis (39), are more likely responsible for rapid morphometric changes (9) observed over the course of the migraine cycle in our patients. In MO patients scanned between attacks, several areas of the right side of the brain, including the inferior parietal lobule, the inferior and superior temporal gyrus, as well as the left temporal pole, showed significant GM density reductions compared with HVs. This interictal morphometric pattern may result from a restructuring of neural circuits, pruning of axonal and dendritic processes, and/or changes in cortical synaptic connectivity (8).
Brain morphometric differences in the migraineur brain are enriched in areas important for sensory information and attention. Morphological and functional studies in animals and humans show that the inferior parietal lobule and inferior and superior temporal gyrus are associative regions belonging to the so-called ventral stream of the visual pathway (40), which acts as a link between auditory and visual processing, perception and memory. The right inferior temporal gyrus is responsible for visual object recognition and receives and processes visual information related to color and form, from the V1–V5 regions of the geniculate and tectopulvinar pathways (41). The right superior temporal gyrus is an essential structure involved in auditory processing and social cognition (42,43). The right inferior parietal lobule has been involved in maintaining attention when working toward current task goals and responds to salient new information or alerting stimuli in the environment (44) through interaction with the ventral visual stream in the superior temporal gyrus (45). When taken together with the functional properties of these brain regions, our findings in migraineurs during the pain-free period are suggestive of a condition of global dysfunction of sensory integration and memory processes.
Another striking finding of our study is that the GM density within the left temporal pole decreased between attacks and increased during an attack when compared to HVs. It is worth noting that temporal pole metabolism observed with H215O positron-emission tomography has previously been shown to increase in migraine patients during spontaneous acute attacks when compared with the interictal state (28). More recently, Moulton and colleagues (2011) used functional neuroimaging to study the effect of placing a heat stressor over the forehead of migraineurs and reported an interictal increase in temporal pole blood flow in migraineurs compared to HVs that further increased during attacks (46). Our present data extend these functional MRI (fMRI) findings by demonstrating that there are dynamic variations in the structure of the left temporal pole during attack, which are not caused by the administration of a painful stimulus such as a heat stressor.
Many studies indicate there is a prominent role of the anterior temporal pole in processing all modalities of conceptual information through multiple sensory forms (e.g. words, pictures, sounds and emotions) (47,48). It is considered an amodal hub that integrates information associated with a complex concept (49,50). Thus, the peculiar neuroplasticity of the anterior temporal lobe in migraine points again to general dysfunction in multisensory integration as a component of migraine pathology that is most affected during attack when central sensitization mechanisms are also abnormal (2).
Relevance for migraine pathophysiology
Previous studies of VBM in MO have provided evidence for reduced GM within or in close proximity of the same temporal and parietal areas described in the present study (temporal lobes bilaterally, the right superior temporal gyrus, the left middle temporal gyrus, the right and left inferior parietal lobes) (15,19,31,32,34,35). In these studies, individuals were not scanned during an attack. Although overall our main finding of an interictal decrease of GM density in temporo-parietal areas is very similar to the above-mentioned studies, our interpretation of these results is different. These studies have attributed GM differences to permanent changes of or damage to the brain as a result of the continuous activation of pain-related pathways during repeated migraine attacks. This suggests that migraine is a progressive disorder of the brain (15,31). Because a progressive disorder would result in permanent morphometric abnormalities, the abnormal decrease in GM density interictally would be expected to persist during attacks. Our data do not support this hypothesis, as GM volumetric abnormalities were not detected in patients scanned during the ictal state. The aforementioned studies generally did not account for the occurrence of an attack hours or days after the scan and thus the point in the migraine cycle when patients were scanned is unknown. This is an essential detail, as neurophysiological studies of migraineurs clearly demonstrate that brain functional responses vary during the migraine cycle (21,51–56). We have also described plastic fluctuations of brain microstructural integrity relative to the time of an attack by diffusion-weighted MRI (4). Therefore, our present observations that all the areas showing interictal reductions in GM density either increased to the normal range or grew from a decrease to an increase is not unexpected. This study provides further evidence of time-dependent plastic changes in brain microstructure correlated with dynamic patterns of the ictal and interictal phases that represent the so-called “migraine cycle.” We cannot exclude that the interictal, probably inherited, subtle factors that determine the observed reduction in GM density within parieto-temporal areas may not only plastically alter brain microstructure, but also predispose patients to the next attack. That genetic predisposition may play an important role in migraine abnormal brain morphology is further underlined by the recent observation that GM volumetric abnormalities found in adults were also observed in pediatric migraine and in the absence of correlation with patient clinical characteristics (19).
It remains to be determined if the cyclical remodeling of neural circuits that may underline ictal/interictal morphometric variability is a primary pathology or a secondary maladaptive consequence of abnormal thalamic variation in microstructure, previously observed by DTI in the same group of patients (4). Whether these effects are primary or secondary, we speculate that dysfunction of these circuits may contribute to the ictal/interictal migraineur susceptibility to abnormal sensory perception, such as visual and auditory discomfort (57,58), or to general impairment in short- and long-term synaptic plasticity leading to deficient habituation/adaptation to sensory stimuli (2). This interpretation is supported by experimental data in healthy humans demonstrating that temporo-parietal areas play an important role in the levels of discomfort associated with loud auditory stimuli (59) and habituation to repetitive visual and auditory stimulation (60–62), all of which are known to be dysfunctional in migraine. Thus, it is significant that one of the most frequently observed functional abnormalities of the migraineurs’ brain, the deficient habituation phenomenon, was also recently detected using a visual stimulus known to elicit response preferentially from brain areas (V3A and V5) that occupy an intermediate position between V1 and the temporal pole along the ventral stream (63). Moreover, it is intriguing that the temporo-parietal areas receive extensive connections from the visual regions of the thalamus, including the pulvinar, non-image-forming visual pathway that was recently identified as a possible anatomical source of light-induced pain (photophobia) in migraine (64).
Finally, we acknowledge certain limitations of the present study. First, the number of participants per group is relatively small, although our cohort was sufficient to produce strong statistical significance. Not all the patients in the two groups (ictal/interictal) served as their own baseline reference; however, this procedure has been successfully validated in previous neurophysiological (21–23) and neuroimaging (24) studies. Following the same patients longitudinally would have provided more robust statistical power.
Conclusions
To conclude, the morphometric GM changes seen in the present study between ictal and interictal phases suggest that there are abnormal migraine-related mechanisms of neural plasticity. Future work will repeat this analysis in a larger clinical sample to follow patients longitudinally, i.e. during their attacks as well as at different time points during their pain-free periods, and to enable the study of different clinical migraine subgroups. We would particularly like to assess migraine with visual aura, for which abnormalities within the temporal cortex associated with visual disturbances were previously noted by magneto-electroencephalography (65). Finally, it would be of interest to verify whether targeted therapies that alter sensory and cognitive functions could potentially improve migraine and, at the same time, normalize abnormal plasticity in brain microstructure.
Clinical implications
We have performed a 3T magnetic resonance imaging (MRI)-voxel-based morphometry (VBM) study comparing gray matter (GM) morphometry of healthy volunteers with that of migraineurs without aura during and between attacks. We observed GM morphometric changes in temporo-parietal areas over the course of the migraine cycle. We suggest that there are abnormal migraine-related mechanisms of neural plasticity, which may contribute to the ictal/interictal migraineur susceptibility to abnormal multisensory perception.
Footnotes
Acknowledgment
The contribution of the Fondazione Bietti in this paper was supported by Ministry of Health and Fondazione Roma.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.