
Abstract
Background
Dihydroergotamine (DHE) and sumatriptan are contraindicated in patients with cardiovascular disease because of their vasoconstricting properties, which have originally been explored in proximal coronary arteries. Our aim was to investigate DHE and sumatriptan in the proximal and distal coronary artery, middle meningeal artery and saphenous vein.
Methods
Blood vessel segments were mounted in organ baths and concentration response curves for DHE and sumatriptan were constructed.
Results
In the proximal coronary artery, meningeal artery and saphenous vein, maximal contractions to DHE (proximal: 8 ± 4%; meningeal: 32 ± 7%; saphenous: 52 ± 11%) and sumatriptan (proximal: 17 ± 7%; meningeal: 61 ± 18%, saphenous: 37 ± 8%) were not significantly different. In the distal coronary artery, contractions to DHE (5 ± 2%) were significantly smaller than those to sumatriptan (17 ± 9%). At clinically relevant concentrations, mean contractions to DHE and sumatriptan were below 3% in proximal coronary arteries and below 6% in distal coronary arteries. Contractions in the meningeal artery and saphenous vein were higher (7%–38%).
Conclusions
Contractions to DHE in distal coronary arteries are smaller than those to sumatriptan, while at clinical concentrations they both induce only slight contractions. In meningeal arteries contractions to DHE and sumatriptan are significantly larger, showing their cranioselectivity. Contractions to DHE in the saphenous vein are higher than those in the arteries, confirming its venous contractile properties.
Introduction
Dihydroergotamine (DHE) and sumatriptan are both 5-HT receptor agonists, and two of the most widely used drugs for the acute treatment of migraine (1–3). DHE is part of the ‘ergot alkaloid family’, together with ergotamine and methysergide. Ergot alkaloids have been used for many decades for the treatment of migraine attacks. Ergotamine is derived from the fungus Claviceps purpurea that grows on grain, which was infamous in former centuries for causing ergotism and miscarriages when ingested through infected bread (2). DHE is derived from ergotamine by reducing an unsaturated bond. DHE and ergotamine are both constrictors of cranial arteries. DHE is less potent in constricting peripheral arteries than ergotamine, but is more potent in constricting peripheral veins (4). DHE is preferred over ergotamine because it has fewer side effects (4). Ergotamine, and from 1945 also DHE, were for decades the classical drugs for the acute treatment of a migraine attack, until the discovery of the triptans in the 1990s. Sumatriptan, which is used in this study, was the first available triptan and is a specific agonist at 5-HT1B/1D/1F receptors, whereas DHE is a non-specific 5-HT receptor agonist and also has affinity for dopamine and noradrenegic receptors (4–6). Next to its less-specific receptor binding, the diffusion of DHE from its receptor is very slow. This may lead to longer-lasting effects and side effects than with the triptans (7). Because triptans are not effective in all patients, ergot alkaloids are still often prescribed. Recently, a phase 3 clinical trial with a new orally inhaled formulation of DHE, MAP0004, was performed in 903 adult migraineurs and was demonstrated to be well tolerated and effective in treating migraine compared to placebo (8). Oral inhalation of DHE causes lower peak plasma concentrations, thus reducing side effects (3,9). Because of their vasoconstrictive properties, both DHE and sumatriptan are contraindicated in patients with cardiovascular disease. This contraindication is based on studies in which small contractions to these drugs were observed in human proximal coronary arteries (7,10). Recently, we showed that the effect of sumatriptan is larger in distal coronary arteries than in proximal coronary arteries (11). This is of clinical relevance because smaller coronary arteries might also account for angina-like symptoms and myocardial ischemia (12,13). The effect of DHE in distal coronary arteries, however, has never been reported and thus it is relevant to compare the contractile properties of those two drugs in distal coronary arteries. Furthermore, the effect of DHE has never been studied in human middle meningeal arteries, where its main therapeutic action in migraine may be located. Knowledge about the amount of contraction that is induced in the meningeal artery, combined with data on its clinical efficacy, provides information on the relevance of this contraction in the treatment of migraine. Because DHE has been reported to be more potent in peripheral veins than in arteries, we included the saphenous vein to obtain a measure of peripheral venoconstriction in response to DHE.
Therefore, the aims of this study were to investigate the contractile effects of DHE and sumatriptan 1) in distal human coronary arteries next to proximal coronary arteries, in view of its safety, 2) in the human middle meningeal arteries, to assess the role of the meningeal artery in its therapeutic efficacy, 3) in human saphenous vein to obtain a measure for the peripheral venous constrictor potential of DHE and 4) to relate our findings to the plasma concentrations observed in clinical practice.
Materials and methods
Tissues
Human proximal (inner diameter 2–3 mm) and distal (inner diameter 0.5–1.0 mm) coronary arteries were removed from healthy human hearts (donors died from non-cardiac disorders, five female, five male, 16–65 years) that were brought to the laboratory within 24 hours after circulation stop. The hearts were provided by the Heart Valve Bank Rotterdam from Dutch postmortem donors, following removal of the aortic and pulmonary valves for homograft valve transplantation. All donors gave permission for research. The hearts were stored in a sterile medium at 4℃ until arrival at the laboratory. The coronary arteries were isolated from the heart, placed in cold (4℃) Krebs buffer solution (composition: NaCl 118 mM, KCl 4.7 mM, CaCl2 2.5 mM, MgSO4 1.2 mM, KH2PO4 1.2 mM, NaHCO3 25 mM and glucose 8.3 mM; pH 7.4), aerated with carbogen (5% CO2 and 95% O2) and stored overnight for organ bath experiments. Human middle meningeal arteries (inner diameter 0.5–1.0 mm) were obtained from pieces of the dura mater of patients who underwent a neurosurgical operation (two male, four female, 44–75 years) and stored in a cold sterile medium M199 (Gibco, Invitrogen, Carlsbad, CA, USA) at 4℃ until arrival at the laboratory. The arteries were cleaned and placed in cold (4℃) Krebs buffer solution for meningeal arteries (composition in mM: NaCl 119; KCl 4.7; CaCl2 1.25; MgSO4 1.2; KH2PO4 1.2; NaHCO3 25 and glucose 11.1; pH 7.4), aerated with carbogen and stored overnight for organ bath experiments in the same way as the coronary arteries. Saphenous veins (inner Ø 0.5–3 mm), obtained from patients who underwent surgery for limb ischemia or varicose vein (four male, two female, 28–67 years) were collected and placed in physiological saline solution, transported to the laboratory and stored overnight in cold (4℃) Krebs buffer solution (composition in mM: NaCl 118, KCl 4.7, CaCl2 2.5, MgSO4 1.2, KH2PO4 1.2, NaHCO3 25 and glucose 11.1; pH 7.4), aerated with carbogen for organ bath experiments.
Organ baths and construction of concentration response curves
Three-mm rings of the proximal coronary arteries and some saphenous vein segments too large to mount in wire myographs were mounted in 15-ml organ baths and vessel tension was set to 15 mN as described previously (14). Two-mm rings of the distal coronary arteries, middle meningeal arteries and the remaining part of saphenous vein segments were mounted in wire myographs (Danish Myo Technology, Aarhus, Denmark) between two small aluminium wires (Ø 40 µm). The tension was normalised to 90% of the estimated diameter at 100 mm Hg pressure (15). All the baths were filled with warm Krebs buffer (37℃), composed as mentioned above for the respective tissues, and aerated with carbogen.
The rings were washed and stabilised for 15 minutes and 30 mM KCl was added. After washout, 100 mM (coronary and meningeal artery) or 65 mM (saphenous vein) KCl was added to compare reactivity between the tissues. After 30 minutes, the KCl was washed out. Concentration response curves were constructed to increasing concentrations of DHE (1 nM–10 µM) or sumatriptan (1 nM–10 µM) and expressed as a percentage of the 100 mM KCl-induced contractions for coronary and meningeal arteries. Endothelial function was evaluated through the addition of U46619 (10–100 nM), a thromboxane A2 analogue, and subsequent addition of substance P (1–10 nM) for coronary and middle meningeal arteries. Saphenous veins were pre-contracted using sumatriptan (1 µM) and upon plateau, endothelium-dependent relaxation was assessed using bradykinin (BK) (10 µM), because substance P is nearly inactive in saphenous veins (16). Contractions were expressed as a percentage of 65 mM KCl-induced contractions.
Compounds
The compounds used in this study were: DHE (dissolved in dimethyl sulfoxide (DMSO) as 10 mM stock solution and further diluted in H2O, Tocris Bioscience, Bristol, UK), sumatriptan (dissolved in DMSO as 10 mM stock solution and further diluted in H2O, Sigma Chemical Co., St. Louis, MO, USA), BK (dissolved in 0.1 M acetic acid, Sigma Chemical Co., St Louis, MO, USA), U46619, substance P and KCl (dissolved in H2O, Sigma Chemical Co., St Louis, MO, USA).
Statistics
The contractile responses to DHE and sumatriptan were expressed as a percentage of the previous response to 65 or 100 mM KCl in the same segment. All data are presented as mean ± SEM, and n refers to the number of tissue donors. In each case, one tissue from each donor was included to study DHE and one tissue from the same donor was included to study sumatriptan. Curves that cover the full sigmoidal range were analysed by means of a computerised curve-fitting technique to obtain Emax and pEC50 values. Statistical analysis of the concentration response curves was accomplished with Graphpad Prism 5 software, using Wilcoxon signed rank test for comparisons of Emax and pEC50 values within tissues and Kruskal-Wallis test for comparisons of these values between tissues. Statistical significance was accepted at p < 0.05 in all cases.
Results
Vascular responses to DHE and sumatriptan in human proximal and distal coronary arteries
In proximal coronary artery segments, the endothelium-dependent relaxant response to 10 nM substance P was 69 ± 7% of the precontraction induced by 10 nM U46619 (n = 8). Maximal contractions and pEC50 values to DHE (Emax: 8 ± 4%; pEC50: 6.7 ± 0.3) (n = 9) and sumatriptan (Emax: 17 ± 7%; pEC50: 6.0 ± 0.2) (n = 9) were not significantly different, thus confirming the data in a previous study in proximal coronary arteries (7) (Figure 1). In distal coronary arteries the endothelium-dependent relaxant response to 10 nM substance P was 91 ± 4% of the precontraction induced by 10 nM U46619 (n = 8). The maximal contractile responses to DHE (5 ± 2%) (n = 10) were significantly smaller than those to sumatriptan (17 ± 9%) (n = 10) (p value = 0.004) (Figure 2). Furthermore, the pEC50 values were larger for DHE (7.7 ± 0.4) than for sumatriptan (6.4 ± 0.1; p value = 0.04).
Contractions to dihydroergotamine (DHE) and sumatriptan in human proximal coronary arteries. Mean ± SEM, n = 9. Contractions to dihydroergotamine (DHE) and sumatriptan in human distal coronary arteries. Mean ± SEM, n = 10.

Vascular responses to DHE and sumatriptan in human middle meningeal arteries and human saphenous vein
In the middle meningeal artery, the endothelium-dependent relaxant response to 10 nM substance P was 82 ± 6% of the precontraction induced by 10 nM U46619 (n = 5). Maximal contractions of middle meningeal arteries to DHE (Emax: 32 ± 7%, n = 6) tended to be smaller than maximal contractions to sumatriptan (Emax: 61 ± 18%, n = 5), although this difference was not statistically significant (p value = 0.188, Figure 3). Similarly, the pEC50 of DHE (7.9 ± 0.4) was not significantly different from that of sumatriptan (6.7 ± 0.2) (p value = 0.125). In the saphenous vein, the endothelium-dependent relaxation to 10 µM bradykinin was 64 ± 15% of the precontraction induced by 1 µM sumatriptan (n = 6). No differences in either Emax or pEC50 values were observed between contractions to DHE (Emax: 52 ± 11%; pEC50: 7.4 ± 0.4, n = 6) and sumatriptan (Emax: 37 ± 8%; pEC50: 6.7 ± 0.2, n = 6).
Contractions to dihydroergotamine (DHE) and sumatriptan in human middle meningeal arteries. Mean ± SEM, n = 5–6.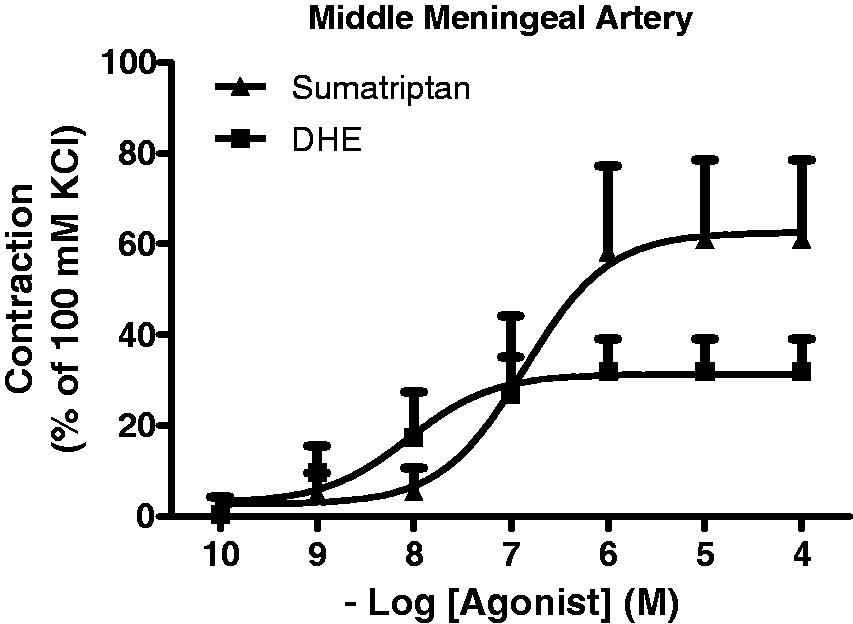
Comparison of response to sumatriptan and DHE between the studied vessels
For both sumatriptan (p value = 0.0131) and DHE (p value = 0.0003), significant differences between the Emax values in the different tissues were observed, with the largest differences present between the coronary artery vs. meningeal artery and saphenous vein. Neither the pEC50 values of sumatriptan (p value = 0.0529) nor DHE (p value = 0.2575) were significantly different between tissues.
Contractions at clinically relevant plasma concentrations
Both DHE and sumatriptan have different formulations. Because the amount and route of administration of the drugs differ for different formulations, this leads to different plasma concentrations (for references, see Table 1). The expected contractions of the investigated blood vessels for these different plasma concentrations can be predicted by interpolating the data of the concentration response curves for DHE and sumatriptan that were constructed. At clinically relevant plasma concentrations, mean contractions both to DHE and sumatriptan in proximal as well as distal coronary arteries are below 7% of maximal contraction obtained with 100 mM KCl (Table 1). In human middle meningeal arteries, mean contractions were between 7% and 38% of maximal contraction obtained with 100 mM KCl. The contractions of the saphenous vein at clinically relevant concentrations of both DHE and sumatriptan were between 10% and 38% of the maximal contraction obtained with 65 mM KCl (Table 1). There is a large variation in contractions to sumatriptan between the patients (95% confidence interval (CI) for Emax values: proximal coronary artery 1%–33%, distal coronary artery 0%–37%, middle meningeal artery 14%–50%, and saphenous vein 18%–57%), illustrated by the large error bars in the graphs (Figures 1, 2, 3 and 4). In most of the patients, the maximal contractions of the coronary arteries at clinically relevant plasma concentrations remain relatively small (Table 1).
Contractions to dihydroergotamine (DHE) and sumatriptan in human saphenous veins. Mean ± SEM, n = 6. Therapeutic doses and Cmax in patients. Therapeutic doses and the subsequent acquired Cmax (corrected for plasma protein binding) in patients are compared to the graphs in Figures 1 and 2 to predict contraction both in proximal and distal coronary arteries as well as middle meningeal arteries. Plasma concentrations obtained from the references mentioned in the table are averaged and corrected for plasma protein binding as described earlier (7). PO: oral; SC: subcutaneous; IV: intravenous; OI: oral inhalation; min: minimum; max: maximum.

Discussion
In the current study, we investigated contractions to DHE and sumatriptan in human proximal as well as the distal coronary artery, which is relevant in view of its cardiovascular safety. In addition, we studied contractions to DHE and sumatriptan in the human meningeal artery, which may be indicative of its therapeutic efficacy. Finally, we included the human saphenous vein in our study to obtain a measure for peripheral venous vasoconstrictor potential of the two compounds. To keep the experimental conditions as physiological as reasonably possible with an in vitro approach, we made no attempt to remove the endothelium from the vessel segments. The endothelial relaxations measured in the vessel segments indicate that the endothelium is functionally intact in our setup. Previously, we demonstrated in the proximal coronary artery that contractions to sumatriptan were slightly more pronounced in vessel segments with intact endothelium (17), underlining the relevance of assessing the endothelial quality.
As expected, contractions both to DHE and sumatriptan in the middle meningeal artery were larger than those in the coronary artery, indicating the cranioselectivity both of DHE and sumatriptan. Across the various blood vessels studied, the potency of DHE seemed somewhat higher than that of sumatriptan (see Figures 1–4), which is in accordance with the higher affinity of DHE than sumatriptan for 5-HT1B receptors (11) (pKi DHE: 9.2–9.5; sumatriptan: 7.4–7.8) (18–20). As known from previous studies, both DHE and sumatriptan induced a small contraction of the human proximal coronary artery (7) and no significant differences in Emax were found between the two compounds. In contrast, contractions to sumatriptan in the smaller distal coronary artery were significantly higher than contractions to DHE. The smaller contractions to DHE in the distal coronary artery deserve further investigation because, as already mentioned in the introduction, smaller vessels can also be involved in coronary artery disease (12,13). Smaller contractions to DHE in the distal coronary artery compared to that of sumatriptan may seem an advantage in view of cardiovascular safety; however, it should be kept in mind that DHE has a much longer-lasting effect than sumatriptan (7), which adds to its side effect potential.
Although there was no statistically significant difference, contractions to DHE in the middle meningeal artery seemed smaller than those to sumatriptan. Furthermore, the different formulations of DHE led to a lower Cmax than the formulations of sumatriptan (Table 1), further increasing the difference in contraction between DHE and sumatriptan in middle meningeal arteries at clinically relevant concentrations. Similar results were observed in a study of cerebral arteries by Nilsson et al. (21). Based on previous assumptions that contractions of the middle meningeal artery are responsible for the clinical efficacy, this might suggest that the antimigraine efficacy is lower for DHE than for sumatriptan. However, in a comparison study, headache relief after subcutaneous sumatriptan was comparable to headache relief after DHE, both around 80% (22). This finding supports the more recent hypothesis that these antimigraine drugs may also work through multiple other mechanisms (blocking nociception, blocking release of calcitonin gene-related peptide (CGRP), etc.), besides vasoconstriction. Indeed, DHE may also exert its antimigraine efficacy via activation of central trigeminal neurons (23). Similarly, we also recently suggested that the migrainogenic role of meningeal artery dilation cannot definitely be confirmed (24). On the other hand, the prolonged action of DHE, caused by slow diffusion from its receptors, may via a vascular mechanism also contribute to its therapeutic action. In two previous studies we also measured contractions to sumatriptan in meningeal arteries, and the Emax values (107 ± 13% and 103 ± 13%) were larger than the Emax values in this study (61 ± 18%) (11,16). As we described earlier for the human coronary artery (25), responses to sumatriptan in human arteries are highly variable, underlining the importance of a paired parallel setup when comparing responses of a blood vessel to sumatriptan to responses to another compound, as applied in the current study.
As expected, contractions to DHE were largest in the saphenous vein, although it should be taken into account that these are expressed as a fraction of contraction to a lower contraction of KCl (65 mM) than in the coronary and meningeal arteries, where 100 mM KCl was used as an internal standard. However, if this were an important factor, this would also have repercussions on the contractile response to sumatriptan. Moreover, the observations in the current study are in the same range as we observed before (26). Whereas the clinical relevance of the larger contractions of DHE in the saphenous vein remains to be demonstrated, these larger contractions are in accordance with the fact that DHE binds to both adrenoceptors and 5-HT1 receptors, which are present in veins. Sumatriptan has no affinity for adrenoceptors, explaining its smaller effects in the saphenous vein.
There are different formulations on the market both for DHE and sumatriptan (9,27,28). Patients prefer oral formulation over injections, but the bioavailability of DHE after oral administration is only 1%, compared to 100% bioavailability of intramuscular injections. A new orally inhaled aerosol formulation, providing a high bioavailability, recently was demonstrated to induce fewer side effects and to have a higher patient preference than the existing DHE formulations (28). We calculated the expected contractions in both proximal and distal coronary arteries obtained in the clinical situation after using different formulations of sumatriptan and DHE that are currently available, as well as the investigational orally inhaled formulation of DHE (Table 1). For all different formulations, mean calculated contractions in proximal coronary arteries were below 3% and in distal coronary arteries below 6%. Outliers were maximal 5% in proximal coronary arteries and maximal 35% in distal coronary arteries. All contractions are percentages of their maximal contraction obtained with 65–100 mM KCl. As coronary blood flow remains intact until 80% constriction of original lumen diameter in healthy individuals, both sumatriptan and DHE should be safe to use in patients who do not suffer from cardiovascular diseases (29). As exemplified by the presence of endothelium-dependent relaxant responses and the absence of macroscopically visible atherosclerotic lesions in our tissues, these tissues may be considered as cardiovascularly normal. In contrast, in patients who already have cardiovascular problems, even a small contraction of a vessel can lead to a reduced blood supply or even a complete occlusion, and these drugs should thus not be used in these patients.
Overall, from this study we can thus conclude that 1) coronary artery contractions to DHE in distal coronary arteries are smaller than those to sumatriptan, 2) in the clinical situation both drugs are likely to induce only a small contraction in both proximal and distal coronary arteries and 3) contractions both to DHE and sumatriptan are larger in middle meningeal arteries than in coronary arteries, demonstrating the cranioselectivity of these drugs. Although contractions both of sumatriptan and DHE in coronary arteries are mostly small, higher outliers can occur and thus the use of these drugs in patients with coronary artery disease should remain contraindicated.
Clinical implications
Contractions to dihydroergotamine (DHE) and sumatriptan are larger in middle meningeal arteries than in coronary arteries, confirming cranioselectivity. Contractions to DHE are smaller than contractions to sumatriptan in distal coronary arteries. At clinically relevant concentrations, both DHE and sumatriptan induce only a slight contraction of coronary arteries, making them safe to use in patients without cardiovascular disease, although their contraindication should remain for patients with cardiovascular disease.
Footnotes
Funding
This study was supported by the Netherlands Organization for Scientific Research (Vidi grant 917.11.349) and by MAP Pharmaceuticals/Allergan.
Conflict of interest
None declared.
Acknowledgements
The authors would like to express their gratitude to the Heart Valve Bank of the Erasmus Medical Center Rotterdam, The Netherlands, for providing the tissues for this study.