
Abstract
Aims
There are no previous epidemiologic studies on concurrent headache and sleep problems (HSP). This cross-sectional study aimed to determine the prevalence of HSP in Denmark, broadly characterize those with HSP, and examine associations between HSP and socioeconomic/lifestyle factors.
Methods
A total of 129,150 randomly selected individuals were invited to participate in the Danish National Health Survey 2010. Respondents were asked about headache, sleep problems, depression and anxiety in the last two weeks, health-related lifestyle and quality of life (SF-12). Socioeconomic data were retrieved from national registers. Prevalence proportions were adjusted for stratified sampling and non-response. Regression analyses examined associations between HSP and socioeconomic/lifestyle factors.
Results
Of 68,518 respondents, 16.3% reported only headache, 21.1% only sleep problems, and 18.1% HSP with 2.6% being severely affected. Prevalence was higher among women and the middle-aged. Severe HSP was associated with low socioeconomic position, non-Western ethnicity, unhealthy lifestyle, high stress and anxiety/depression. Those with HSP had substantially reduced quality of life; more so than those having only headache or only sleep problems.
Conclusions
HSP is a highly prevalent condition. Lifestyle modification, stress reduction, and screening for concurrent depression and anxiety may play important roles in management. The high prevalence of HSP suggests a common pathophysiological mechanism.
Introduction
Very little is known about the precise relationship between headache and sleep problems when these occur concurrently. Sleep can alleviate headache, but lack of or too much sleep can also trigger headache (1). Concurrent headache and sleep problems (HSP) may be explained by the existence of multiple anatomical and physiological links (2,3), but an exact mechanism for a causal relationship or an underlying pathology is yet to be determined. Nonetheless, concurrent headache and sleep disorders are clinical entities classified in two systems: the International Classification of Sleep Disorders (ICSD-2) (4) and the International Classification of Headache Disorders (ICHD-3 beta) (5).
Population-based studies have found an increased prevalence of sleep problems/disorders among people with headache (6–8). Rasmussen (7) found that sleep problems were positively associated with tension-type headache (TTH) but not with migraine, although migraineurs who had sleep problems reported a significant lack of refreshment after sleep. Furthermore, TTH was associated with a lower average number of sleeping hours.
In addition, comorbid sleep disorders seem to affect headache frequency (9,10). Follow-up studies have shown that sleep problems are a predictive factor for chronification of TTH (11) and severe insomnia may increase the risk of medication-overuse headache and chronic headache (12).
Previous population-based studies reporting an association between headache and sleep problems did not describe those with concurrent problems as a distinct sub-group. In this first epidemiologic study, we examined the prevalence of any headache occurring with sleep problems within a 14-day recall period. Improving our knowledge of those affected by HSP would lead to a greater understanding of the pathophysiology of these two common complaints, and improve treatment and/or prevention strategies.
Therefore, the objectives of this population-based cross-sectional study were 1) to determine the prevalence of: severe and moderate concurrent headache and sleep problems (severe and moderate HSP), only sleep problems, only headache, and those with neither problem; 2) to characterize the five groups above in terms of demographic, socioeconomic and lifestyle factors, self-reported symptoms of depression and anxiety, and quality of life (QoL), and 3) to examine associations between severe HSP and socioeconomic and lifestyle factors.
Methods
Sampling and data collection
The Danish National Health Survey 2010 (DNHS) is a large cross-sectional, population-based survey conducted in the five regions in Denmark. It consisted of a standard questionnaire with 52 questions on chronic illness, health behaviors, and QoL, with each region including questions of specific local interest (e.g. headache) (13). In this paper we analyzed data from the Capital Region and Region Zealand with a total population of 2,024,979 inhabitants. The sample was randomly drawn from the adult population (age ≥16 years) using data from the Danish Civil Registration System where each individual permanently residing in Denmark has a unique personal identification number. The sample included 129,150 individuals: 95,150 in the Capital Region and 34,000 in Region Zealand (corresponding to 7.0% and 5.2%, respectively, of the regional populations aged ≥16 years).
A letter containing an introduction letter and a paper questionnaire was sent to all selected individuals. Participants could also complete the questionnaire on the Internet. Participation was voluntary. Non-respondents were sent a minimum of two postal reminders. Data were collected from January to April 2010.
The respondents were asked: “In the past 14 days, have you been affected by headache problems?” and a subsequent question about sleep problems was asked in the same time frame. For both questions, respondents could choose from three answers: “yes, very much affected,” “yes, moderately affected” and “no.” Respondents who answered yes to both questions were considered as having concurrent headache and sleep problems (HSP) and were further classified as having severe or moderate HSP (Figure 1). There were no further questions that would allow for a more precise diagnosis of a specific headache or sleep disorder.
Participation in the Danish National Health Survey of 2010, and number of respondents per category of headache and sleep problems.
Demographic (age, sex and ethnicity) and socioeconomic data (employment status, highest educational attainment and income) were retrieved from national central registers. Employment status was classified into seven categories: student, full-time employed, unemployed, receiving illness allowance, receiving social security, early retired and retired. Educational attainment was categorized as primary/secondary school, vocational education, academy/bachelor degree, or master’s/PhD degree. Income was computed as household income divided by the number of adults in the household, categorized as six income groups and converted from Danish kroners (DKK) to US dollars (one US dollar = 5.5 DKK). Ethnicity was based on country of origin and was determined from the respondent’s place of birth, citizenship and parents’ place of birth. Ethnicity was categorized into three groups: Danish, Western and non-Western.
Family status was classified as one of four categories based on information obtained from the questionnaire: living alone with/without children, living with partner with/without children.
Six unhealthy lifestyle indicators were investigated. Respondents were asked “Do you smoke?” and could choose from five possible responses according to frequency. For simplicity, respondents were categorized as daily smokers (yes/no). Body mass index (BMI) was calculated from self-reported height and weight then categorized as underweight (<18.5 kg/m2), normal (18.5–<25 kg/m2), overweight (25–29.9 kg/m2), or obese (≥30 kg/m2). Level of physical activity was based on a previously validated self-report instrument (14). Respondents were asked to fill in the average number of hours and minutes spent on different activities each day or each week. Low physical activity was defined as doing moderate to hard physical activity less than 30 minutes a day. Respondents were asked to list the number of units of beer, wine or spirits they drank, on average, each day of the week in the past year. Respondents were then classified as drinking above or below the recommendations of the Danish Health and Medicines Authority (women: ≤7 units/week, and men: ≤14 units/week). Very high alcohol intake was defined as drinking >35 units/week. Stress was quantified using Cohen’s Perceived Stress Score (15). Responses were scored from 0 to 4 on a Likert scale (total score ranged from 0 to 40). Respondents were grouped into quintiles based on their total scores. If there were more than three missing answers the total score for the respondent was not computed, and if there were ≤3 missing answers, items were scored as 2 (neutral on the Likert scale).
Psychological symptoms of anxiety and depression were self-reported and not assessed using a validated questionnaire. Respondents were asked if they had felt sad/depressed/unhappy, or anxious/nervous/uneasy in the last 14-days, to which they could reply: “yes, very much affected,” “yes, moderately affected” or “no.”
QoL was assessed using the eight domains of the SF-12 (16): physical functioning (PF), role limitations due to physical health problems (RP), bodily pain (BP), general health (GH), vitality, energy, fatigue (VT), social functioning (SF), role limitations due to emotional problems (RE) and mental health (MH).
Data analysis
Respondents were classified into five groups (Figure 1): severe and moderate concurrent headache and sleep problems (severe HSP, moderate HSP), only sleep problems, only headache, and no headache or sleep problems. Percentage distributions of these five groups were calculated by sociodemographic factors. The prevalence of unhealthy lifestyle factors, and self-reported symptoms of anxiety and depression were calculated for each group. Percentage distributions across categories were compared using chi-square tests. P values <0.05 were considered significant. Univariate logistic regression analyses were performed using severe HSP as the outcome variable and socioeconomic and lifestyle factors as explanatory variables, adjusted for potential confounders (sex and age). Multivariate regression analysis was also performed with mutual adjustment for education, employment status, income, family status, ethnicity, daily smoking, BMI, low physical activity, alcohol intake above recommended, very high alcohol intake, stress quintile, and self-reported symptoms of depression and anxiety.
SF-12 scores in eight domains were calculated for the five groups (16). Scores were compared with the reference group (those with neither headache/sleep problem) using t-tests.
All calculations were adjusted for stratified sampling and non-response. Because of the unique personal identification number of residents in Denmark, both respondents and non-respondents can be linked, on an individual level, to different central registers. Weights were computed by Statistics Denmark to adjust for potential differential non-response based on register information on sex, age, municipality of residence, highest completed educational level, income, marital status, ethnic background, number of visits to a general practitioner, a hospitalization (yes, no), occupational status, house-owner/tenant status and protection from inquiries during statistical and scientific surveys (13,17).
All respondents gave informed consent. Data collection and analysis followed the standards of the Danish Data Protection Agency and the Danish Act on the Processing of Personal Data. All raw data were accessed from Statistics Denmark servers. Authors MW and CG had access to the data in order to perform analyses, but could not edit individual entries. Identities of respondents were not known to investigators.
Results
Questionnaires were returned by 68,518 people (response rate 53.1%). Non-respondents were more likely to be young men, elderly women, unmarried and/or of an ethnic background other than Danish (13).
The majority (>80%) responded using the paper questionnaire. Response via Internet was 17.5% in the Capital Region and 11.8% in Region Zealand, with most Internet respondents (88.8% in the Capital Region) being under 55 years old.
Prevalence a of concurrent headache and sleep problems (HSP), only headache, only sleep problems and no problems, by sex and age.

All proportions were adjusted for stratified sampling and non-response. Row totals equal 100. Age-specific distributions are presented by sex and as totals for males and females. bp values refer to results of chi-square tests comparing distributions across age groups in each of the five categories. Sex-specific tests were also highly significant (p = 0.0001 to p < 0.0001). HSP: concurrent headache and sleep problems; F: female; M: male; CI: confidence interval; All: total percentage for females and males.
A female preponderance was seen among those with severe and moderate HSP (p < 0.0001), and those affected by only headache (p < 0.0001). There was no significant sex difference among those with only sleep problems (p = 0.1299).
HSP was most prevalent among those aged 45–54 years, and least among people 65 years or older. The prevalence of only headache was highest among those aged 16–44 years, then decreasing with age. This trend was opposite among those affected by only sleep problems, where the prevalence increased from age 45 and up.
Demographic and socioeconomic factors
Prevalence a of concurrent headache and sleep problems (HSP), only headache, only sleep problems, and neither problem, by sociodemographic categories.

All proportions were adjusted for stratified sampling and non-response. Row totals equal 100. bIncome was converted from DKK to US dollars (5.5DKK = 1 US dollar). HSP: concurrent headache and sleep problems; CI: confidence internal. P values refer to chi-square tests comparing proportions in each category.
Lifestyle factors
Distribution a of lifestyle factors, self-reported depression and anxiety among the five categories of respondents: with severe or moderate concurrent headache and sleep problems (HSP), only headache, only sleep problems and no problems.
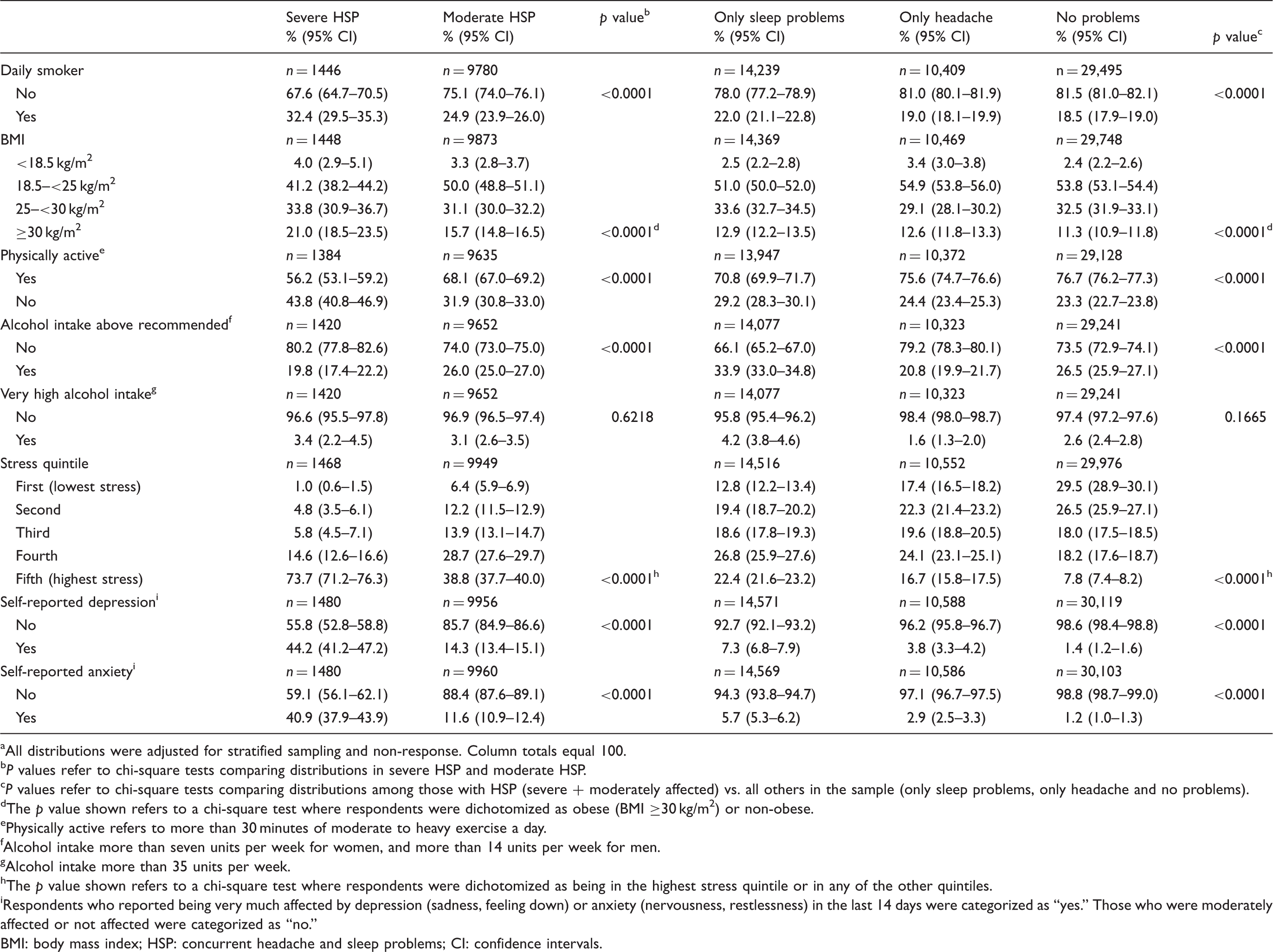
All distributions were adjusted for stratified sampling and non-response. Column totals equal 100.
P values refer to chi-square tests comparing distributions in severe HSP and moderate HSP.
P values refer to chi-square tests comparing distributions among those with HSP (severe + moderately affected) vs. all others in the sample (only sleep problems, only headache and no problems).
The p value shown refers to a chi-square test where respondents were dichotomized as obese (BMI ≥30 kg/m2) or non-obese.
Physically active refers to more than 30 minutes of moderate to heavy exercise a day.
Alcohol intake more than seven units per week for women, and more than 14 units per week for men.
Alcohol intake more than 35 units per week.
The p value shown refers to a chi-square test where respondents were dichotomized as being in the highest stress quintile or in any of the other quintiles.
Respondents who reported being very much affected by depression (sadness, feeling down) or anxiety (nervousness, restlessness) in the last 14 days were categorized as “yes.” Those who were moderately affected or not affected were categorized as “no.”
BMI: body mass index; HSP: concurrent headache and sleep problems; CI: confidence intervals.
Those with HSP were clearly in the higher quintiles of Perceived Stress Scores. As many as 73.7% of those severely affected and 38.8% of those moderately affected were in the highest quintile, compared to 22.4% with only sleep problems, 16.7% with only headache, and 7.8% with no problems.
Among those with severe HSP, 44.2% had self-reported symptoms of depression and 40.9% of anxiety. In comparison, the other groups had significantly fewer reports of depression and anxiety.
Severe HSP and associated factors
Associations between severe concurrent headache and sleep problems, socioeconomic variables and lifestyle factors.
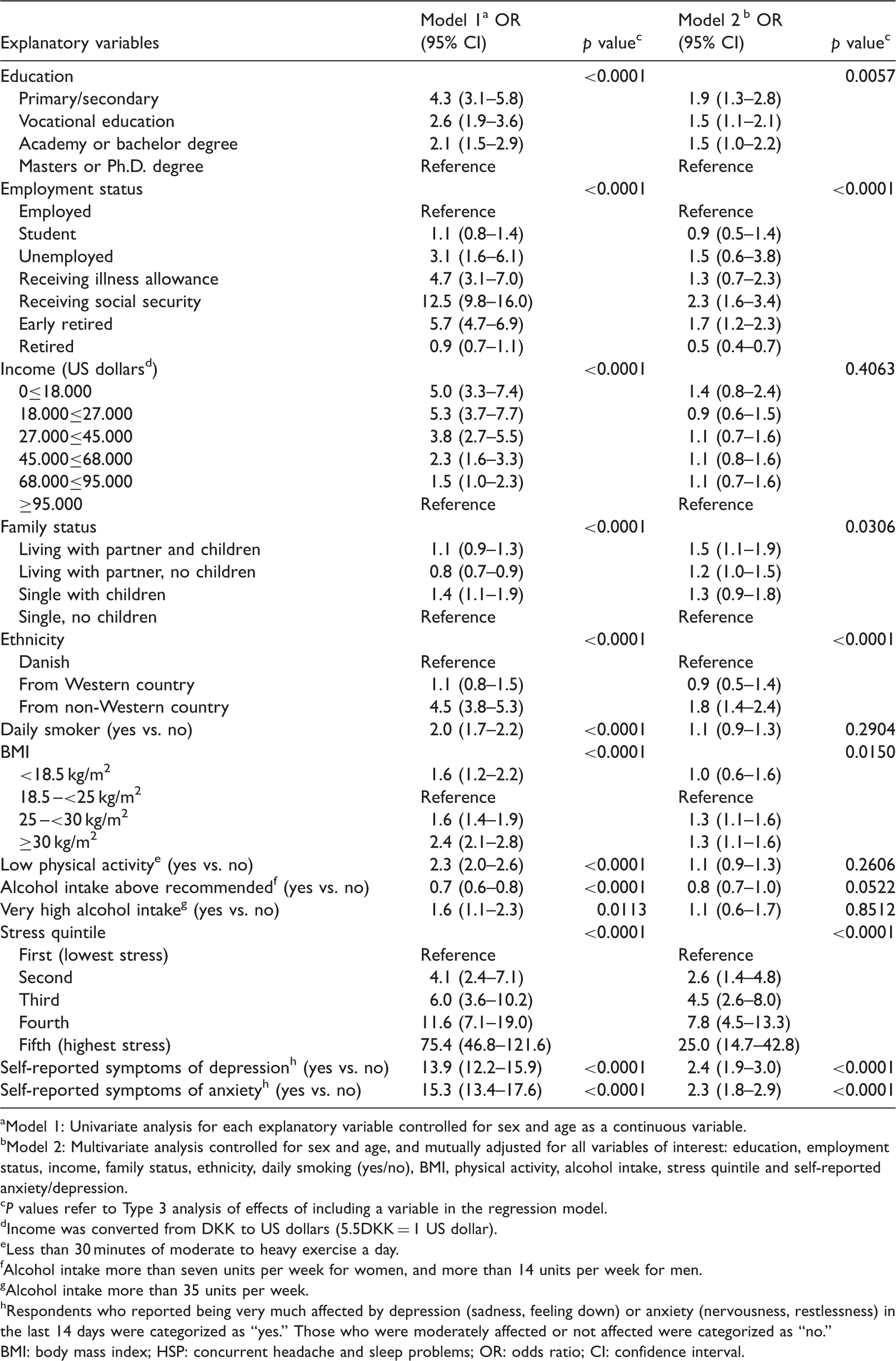
Model 1: Univariate analysis for each explanatory variable controlled for sex and age as a continuous variable.
Model 2: Multivariate analysis controlled for sex and age, and mutually adjusted for all variables of interest: education, employment status, income, family status, ethnicity, daily smoking (yes/no), BMI, physical activity, alcohol intake, stress quintile and self-reported anxiety/depression.
P values refer to Type 3 analysis of effects of including a variable in the regression model.
Income was converted from DKK to US dollars (5.5DKK = 1 US dollar).
Less than 30 minutes of moderate to heavy exercise a day.
Alcohol intake more than seven units per week for women, and more than 14 units per week for men.
Alcohol intake more than 35 units per week.
Respondents who reported being very much affected by depression (sadness, feeling down) or anxiety (nervousness, restlessness) in the last 14 days were categorized as “yes.” Those who were moderately affected or not affected were categorized as “no.”
BMI: body mass index; HSP: concurrent headache and sleep problems; OR: odds ratio; CI: confidence interval.
QoL
People suffering from severe HSP scored the lowest in all eight SF-12 domains, followed by people with moderate HSP, only sleep problems, only headache, and people with neither problem (Figure 2). All comparisons against the group without headache/sleep problems showed highly significant differences (p < 0.0001), except for the physical functioning (PF) scores for those with only headache versus those with no HSP (p = 0.03).
SF-12 scores for respondents with no headache or sleep problems, only headache, only sleep problems, and severe and moderate concurrent headache and sleep problems.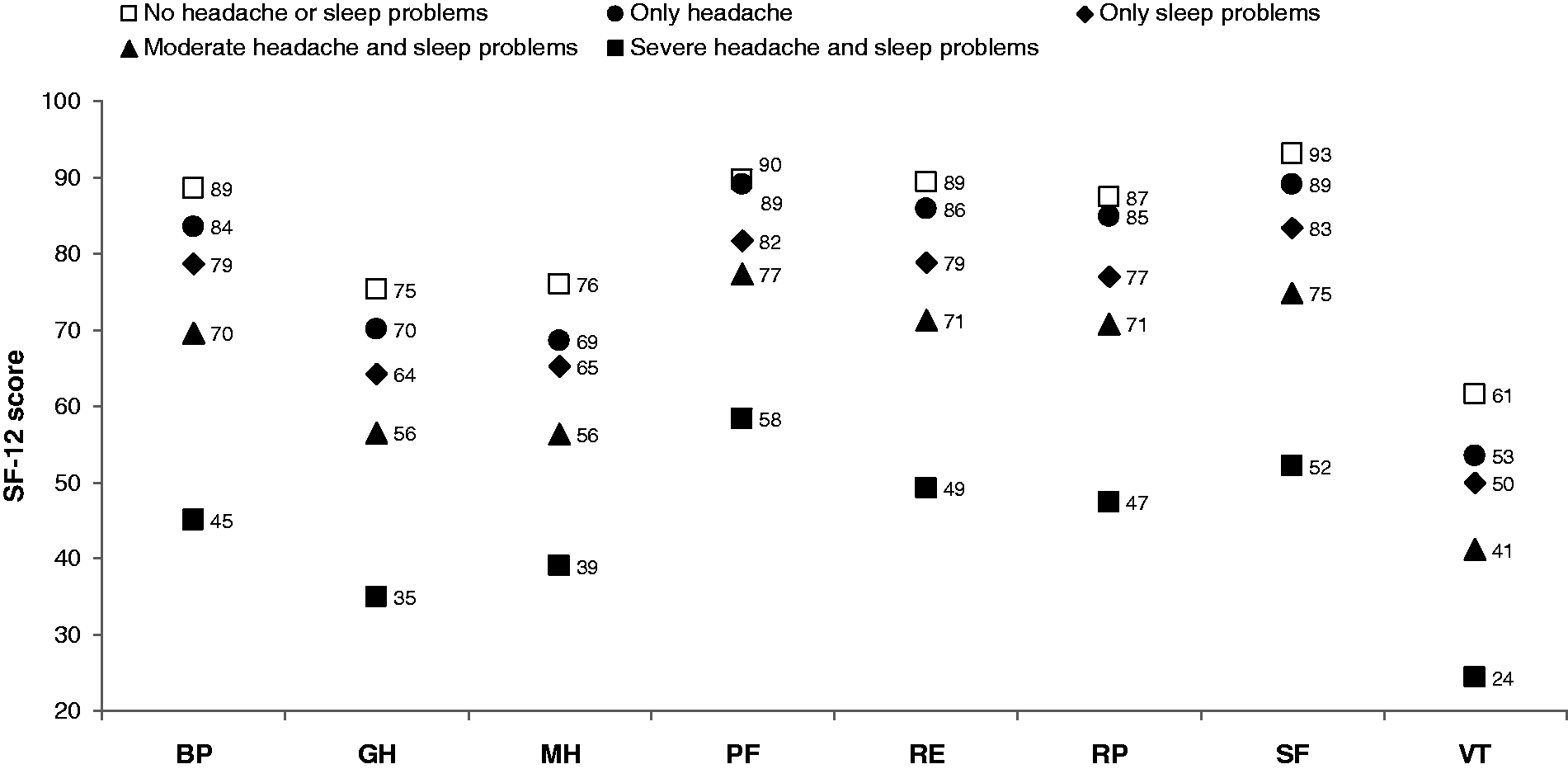
Discussion
Prevalence of concurrent headache and sleep problems
This is the first large epidemiologic study focused on headache and sleep as concurrent problems. We document that HSP is common in the general population, affecting about one in five people. HSP prevalence was highest among females, the middle-aged, and those of non-Western ethnicity. Severe HSP was associated with low SEP, unhealthy lifestyle, high stress, and self-reported symptoms of anxiety and depression. Furthermore, QoL was significantly reduced among those with HSP.
Data from a questionnaire-based study by Boardman et al. of 2662 United Kingdom (UK) citizens (6) can be used to calculate the prevalence of HSP, only headache, and only sleep problems. In their sample, as many as 67% had HSP, 24% had only sleep problems, 4% had only headache, and as few as 5% had neither problem. The focus of their study was headache, and the purpose was to look at sleep as an associated factor (among other factors). As a headache prevalence study, there might have been strong interest bias (those with headache were more likely to respond because they found the study was relevant.) This might explain the relatively high prevalence of headache reported (70% in a three-month period), compared to the mean European one-year prevalence of 51% (18). This might also explain the higher proportion of those with concurrent problems. In contrast, the DNHS was a general health survey and inquired about many chronic illnesses. Headache-related or sleep-related interest bias would be expected to be minimal. Differences in methodology could possibly also explain part of the divergence (sleep problems were recorded in a 14-day period similar to ours, but headache symptoms were recorded for a three-month period compared to our 14-day period). Another factor to consider was how sleep problems were ascertained. Respondents in the Boardman et al. study were asked about specific symptoms: trouble falling asleep, waking up several times per night, trouble staying asleep, etc. and the severity of these problems (based on frequency and number of symptoms). In our study, participants were asked only about the presence of a sleep problem, without prompts on specific symptoms.
Headache prevalence in the current study was high among adults aged 16–44 years, then fell with increasing age. This parallels the findings of international studies summarized in a large European review (18). A previous Danish population-based study (19) found similar results in relation to TTH, but not for migraine. As to sleep disorders, the higher prevalence we observed among those aged 45 years and up matches the age distribution for the most common sleep disorders: insomnia, sleep apnea and restless legs syndrome (20). As could be anticipated, the prevalence of HSP was thus highest in middle age.
The high female preponderance for HSP and for headache also parallels the findings of several population-based studies (7,8,18,21). There was only a slight female preponderance for sleep problems, possibly because among the common sleep disorders insomnia is more prevalent in females whereas sleep apnea is more so in men (20,22).
The prevalence of HSP was higher among immigrants from non-Western countries compared to Western immigrants and ethnic Danes. The association between severe HSP and non-Western ethnicity remained strong after adjusting for potential confounders including SEP. Several Danish and European studies have shown a higher prevalence of chronic headache, musculoskeletal pain and chronic pain among immigrants compared to the local population (9,23–26). We have no baseline data prior to immigration and the cause-effect relation cannot be clarified in this cross-sectional study. Previous studies on chronic headache suggest that SEP might play a role in the higher prevalence observed in relation to headache (9,24). In Denmark, diagnosis and hospital treatment is free of charge; therefore health care is accessible to all. However, cultural barriers might influence access to primary care and compliance to treatment for symptoms of headache and sleep problems.
Socioeconomic and lifestyle factors
An inverse relationship was seen between severe HSP and SEP as measured by education and employment. Income did not seem to be a significant factor once adjusted for the two other SEP indicators. Low SEP could be a risk factor for HSP, but another plausible explanation is that disability due to HSP lowers productivity and limits upward mobility. Our findings show that HSP represents a social burden, both for the individual and society.
We also found that unhealthy lifestyle habits (smoking, overweight/obesity, physical inactivity, and very high alcohol intake) were associated with severe HSP. However, these behaviors are also differentially more common among groups with low SEP. After adjustments, only high BMI was clearly associated with severe HSP.
Studies have shown that obesity is associated with several sleep disorders, including obstructive sleep apnea (20). It is also associated both with headache and migraine (27–30) and has been suggested as a risk factor for migraine chronification (30).
The variable that showed the strongest association with severe HSP was perceived stress. The source of this stress was not directly assessed in the questionnaire, but based on available data it could be explained in part by low SEP, or being part of an ethnic minority. We did not look into the specific effects of comorbid chronic illness, coping mechanisms, personality, or social support structures. Headache and sleep disorders both are associated with psychiatric disorders (20,31,32) and as expected, HSP was found to be strongly associated with symptoms of depression and anxiety.
The relationship between HSP and alcohol is very interesting. Those with headache (HSP or only headache) drank the least alcohol, very likely because alcohol can trigger headache (7). Alcohol intake was highest among those with only sleep problems, possibly because alcohol is used as an easily available hypnotic, although chronic alcohol abuse actually causes poor sleep (22). We found that HSP was not significantly associated with alcohol intake after adjusting for SEP and other possible confounders.
QoL
Our data showed that having HSP greatly reduced QoL. Those with severe HSP had the lowest scores in all domains of the SF-12. Having one problem (headache or sleep problem) resulted in a lower QoL compared to having no problems. This suggests that decreasing the severity of HSP, or removing even just one of the two problems, would greatly improve QoL. Surprisingly, those affected by only sleep problems had lower QoL in all eight areas compared to those with only headache, suggesting that, at least in the short term, physical and mental health may be more affected by sleep problems than by headache.
Possible anatomical and physiological links
The high rate of co-occurrence of headache and sleep problems in the same person suggests that there might be an anatomical or physiological basis for these symptoms. People who suffer from migraine, TTH and cluster headache commonly report sleep problems (1,33). There may be links to arousal-promoting systems, where several nuclei are highly involved both in sleep-wake regulation (34) and in descending pain-modulation mechanisms (3). Research on possible overlaps between regions involved both in headache and sleep problems is ongoing. With current knowledge, the following hypotheses can be put forward: 1) Headache may cause awakenings and thereby hampers normal sleep initiation and maintenance; and 2) poor sleep and fatigue affect pain sensitivity and possibly also the ability to cope with problems or stressors. In this way poor sleep is an initiating and/or contributing factor to headache and vice versa. However, as much is still unknown, other modes of interaction cannot be ruled out.
Limitations and strengths
The very large number of participants increased the power of the study, and allowed for analysis of subgroups of the population according to severity of HSP. This graded division of HSP is very important in relation to future studies of treatment strategies and prognosis.
The survey included questions on a broad diversity of illnesses and health conditions, therefore respondents were unlikely to be disproportionally selected for headache or sleep problems. The survey had an acceptable response rate, and calibrated weights were used to minimize the effect of non-response bias. Data on demographic and socioeconomic factors were taken from national databases and were thus not subject to recall bias or social desirability bias.
The advantages of using DNHS data include large sample size and representativeness. The disadvantage is that the questions used were limited and did not allow for making specific headache nor sleep diagnoses. There were likely differences in respondents’ interpretations of what constitutes a sleep problem, and whether their headache or sleep problems were severe or moderate. It was beyond the scope of the present study to link survey data with patient registries where gold-standard diagnoses could be made. Self-reported symptoms of depression and anxiety were not further explored, and were not correlated with clinical records of psychiatric diagnoses. The 14-day time frame reduced recall bias but increased the likelihood of missing those suffering from low-frequency headache or sleep problems. Also, we could not measure duration of symptoms beyond this period. If there had been misclassification (i.e. those who had both headache and sleep problems were not detected in this short time frame), then the prevalences presented here might be underestimates.
Causality cannot be concluded from our data, but it is clear that there are associations between demographic, socioeconomic, lifestyle and psychological factors in HSP. Most likely, a vicious circle exists where physical, social and psychological stressors influence a biological predisposition to headache and/or sleep problems. Management should therefore address this complexity.
Conclusions
HSP is discussed in this paper as a confluence of two problems in the same person. The two problems are often evaluated and treated separately even though they coexist very often. Concurrent symptoms might be easily overlooked in specialty clinics focusing on only one or the other problem. HSP was found to be a very common problem in the Danish general population and significantly lowers QoL. Lifestyle modification and screening for psychological disorders may play a role in the treatment and prevention both of headache and sleep disorders. Our findings underline the importance of reducing the degree of concurrent problems and a more aggressive approach toward identifying sleep problems among headache patients and vice versa. The high prevalence of concurrent disorders suggests a common pathophysiological mechanism. Future studies should focus on verifying these clinically important findings in specific headache and sleep disorders.
Clinical implications
Concurrent headache and sleep problems (HSP) are very common in the general population, occurring in 18.1% with 2.6% being severely affected. Prevalence is highest among females, the middle-aged, and those of non-Western ethnicity. Low socioeconomic position, unhealthy lifestyle (particularly overweight/obesity), high stress, and self-reported symptoms of depression and anxiety, are associated with severe HSP. Those with HSP have reduced quality of life; more so than those having only headache or only sleep problems. Headache and sleep disorders are comorbid problems that should be identified in the clinical setting.
Footnotes
Funding
The Danish National Health Survey 2010 was a joint project of The Capital Region of Denmark, and Region Zealand in cooperation with the Research Center for Prevention and Health. MW received a research grant from IMK Almene Fond, and the Danish patient organization Migræne og Hovedpineforeningen in relation to this study.
Conflict of interest
RJ has given lectures for Pfizer, Berlin-Chemie, Allergan, Merck, and Autonomic Technologies and is a member of the advisory boards of Autonomic Technologies, Medotech and Neurocore. MW has received travel grants from Pfizer and Lundbeck Fund. The other authors have nothing to declare.
Acknowledgments
The authors would like to thank the team responsible for the Danish National Health Survey from the Research Centre for Prevention and Health, particularly Carsten Agger, who facilitated access to data from the survey and relevant national central registers. Furthermore, we thank Inger Helt Poulsen, who facilitated the use of data from Region Zealand; Statistics Denmark; and everyone who responded to the surveys.