
Abstract
Background
Hypnic headache (HH), first reported in 1988, is a rare sleep-related headache disorder. In 2013 a new diagnostic criteria was proposed for HH in the International Classification of Headache Disorders, the third version beta (ICHD-3β).
Purpose
This review aimed to update the clinical characteristics, therapeutic options and clinical outcomes in patients with HH and also validate the new diagnostic criteria.
Methods
Based on a literature search in the major medical databases, we analyzed all case reports or case series on HH that have been published since the first description by Raskin. Except for symptomatic patients, all reported patients were included regardless of which diagnostic criteria were adopted. Four studies that reported the field-testing results of the ICHD-2 criteria were selected to validate the new ICHD-3β criteria.
Results
In total, 250 adult and five childhood patients are described in this review. The majority of patients were elderly and their ages of onset were typically more than 50 years old (92%). Approximately 7.7% of patients had some trigeminal autonomic features, which are not permitted in the ICHD-3β criteria. Compared with the ICHD-2 criteria, the diagnostic rate under the new criteria increased from 65% to 85% in recently reported cases. Randomized control trials both for acute and prophylactic treatment are lacking. Based on observational studies, the most effective acute treatment is caffeine and prophylactic medications in use are lithium, caffeine and indomethacin. Without treatment, the disease course is usually protracted but spontaneous remission did occur in 12 patients (4.8%). In those treated with prophylactic agents, no recurrence was noted in 43% of patients, even following withdrawal of medication.
Conclusions
The new ICHD-3β criteria are more sensitive and exhaustive for HH than the ICHD-2 criteria. Prophylactic treatment provides better outcomes; however, randomized controlled studies for treatment are needed to further verify the efficacy of the different drugs.
Introduction
The ICHD-2 and ICHD-3 criteria (beta version) of hypnic headache.

4.9.1 Probable HH: fulfills criterion A, B, F and two of criterion C–E. ICHD-2: International Classification of Headache Disorders, second edition; ICHD-3: International Classification of Headache Disorders, third version.
The new criteria were more evidence based for clinical use and research. However, there are still differing opinions for the diagnostic criteria. For example, some case series have reported mild trigeminal autonomic symptoms in as many as 15% of patients (3,8,9).
Many studies have reported the therapeutic experience of HH. Lithium, caffeine and indomethacin are the most mentioned effective treatments; whereas other drugs have also been reported to be effective, albeit only in case reports (5). Some case reports have also described the successful alternative treatment of patients who did not respond to conventional medication or those contraindicated for first-line treatment (12–18). However, the natural course and long-term outcomes of HH after treatment have been described in only a few studies (3,10,19–21). Thus, this review article intends to summarize the currently available information on the clinical characteristics, therapeutic options and outcomes in HH patients.
Method
Based on a literature search in the major medical databases (PubMed, Embase and Current Contents), we analyzed all case reports or case series on HH that have been published since the first description by Raskin (1). Because there is no formal diagnostic criteria of HH before the publication of the ICHD-2, and because some different broadening criteria were adopted in the discussed studies, we enrolled all cases with sufficient demographic and clinical data where the patients were defined as having HH by the authors. The symptomatic cases whose HHs were related to neoplasm (n = 6) (22–25), stroke (n = 1) (26), intracranial hypotension (n = 1) (27), and drugs (n = 3) (28–30) were excluded from further analysis. In this study, HH patients with nocturnal hypertension or obstructive sleep apnea syndrome (OSAS) were counted as idiopathic HH regardless of the treatment response for OSAS or nocturnal hypertension because the association between HH and nocturnal hypertension or OSAS is not clear. Cases with double publications were considered only once; the respective articles or abstracts of double publications were omitted totally or in part. Data were analyzed based on demographic and clinical features, therapeutic experience and clinical outcomes. The data are presented as the arithmetic mean with the standard deviation (SD) or as percentages. The percentage is always related to the total number of patients on whom information was available for the specific issue.
Epidemiology
At the time of writing, 250 adult patients and five child patients with idiopathic HH have been described in the literature (31–33). More than 50% of cases (n = 140) were described in seven major case series (each with more than 10 patients) from the United States (US) (34), Taiwan (10), France (9), Germany (8), Spain (7,35) and Brazil (6). The precise prevalence of HH is unknown and data from the literature give only an estimation of its frequency among headache patients consulting tertiary headache centers or clinics. HH was reported to account for 0.07% of all headache patients in an earlier case series (34). In two later studies reported in 2003 and 2004, HH was diagnosed in approximately 0.09% to 0.1% of all headache patients and, notably, in 1.4% of geriatric patients (>65 years of age) (21,36). HH prevalence appears slightly higher when the three recent case series reported in 2008, 2009 and 2013 are considered (6,9,10) as they indicated that HH was diagnosed in 0.3%, 0.35% and 0.22% of all headache patients, respectively. Furthermore, another recent study reported that HH accounted for 1.7% of geriatric headache patients (37). The frequency of HH diagnosis has gradually increased in recent years and is probably due to the increasing recognition of HH. The true prevalence needs further investigation.
Clinical characteristics
Clinical characteristics in adult hypnic headache.
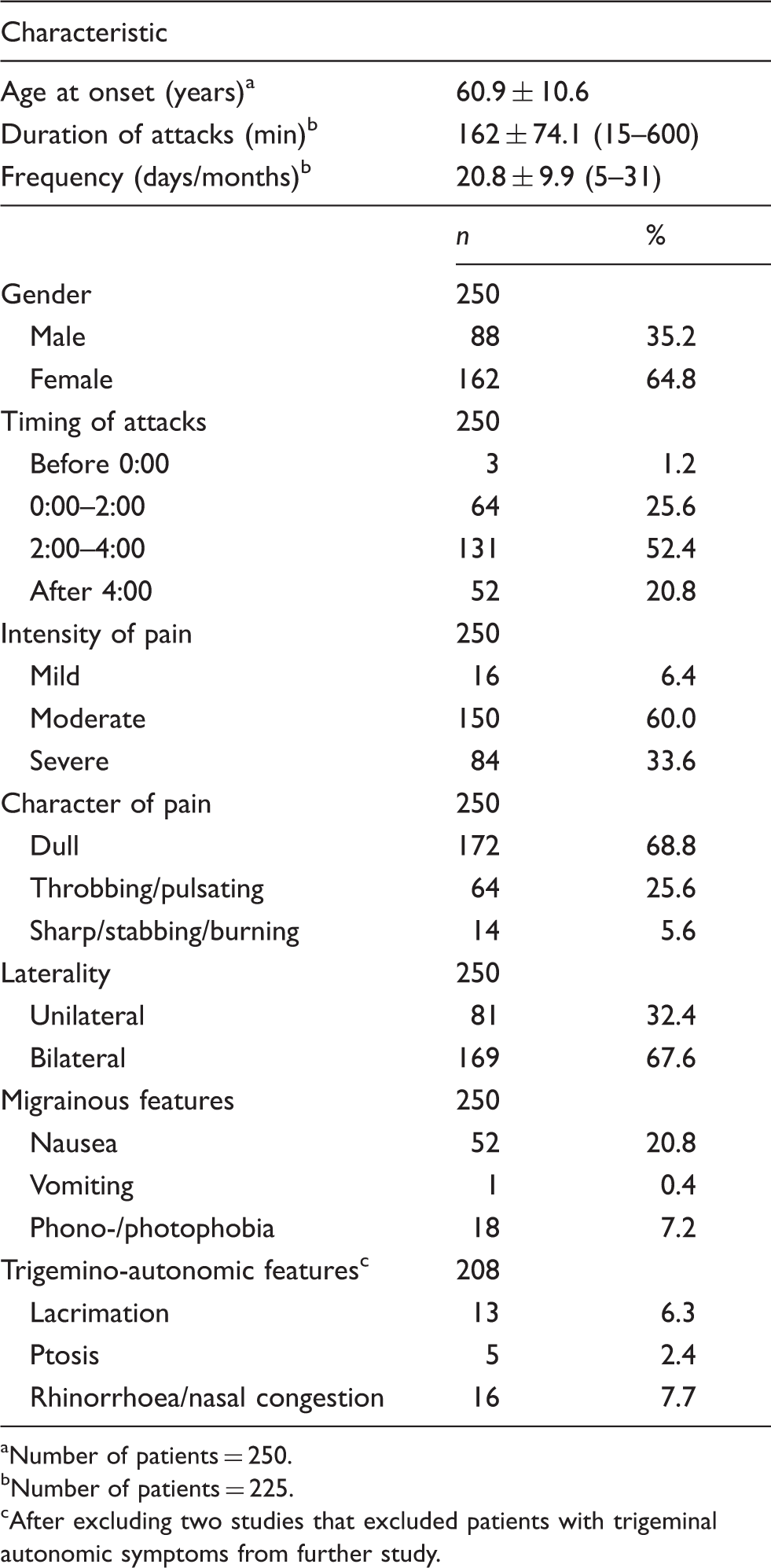
Number of patients = 250.
Number of patients = 225.
After excluding two studies that excluded patients with trigeminal autonomic symptoms from further study.
Although the first case series by Raskin reported five of six patients to be male, 65% of HH patients were female out of all the reported 250 patients. Regarding the pain intensity and type, 64.4% of patients reported that the headaches were mild to moderate. Dull headaches were reported by 68.8% of patients, followed by throbbing or pulsating headaches (25.6%). Thus, a dull headache is not necessary for HH diagnosis in the new criteria. Most HHs are bilateral and the most mentioned location of the headaches were the frontotemporal area (46%) or holocranial/diffuse (46%).
The average frequency of attacks per month was 20.8 days and up to 67% of patients suffered from daily headaches, as reported in one study (10). The mean duration of headache episodes was near three hours. This finding was further confirmed by a recent case series that reported that 64% of HH patients (n = 25) had headaches lasting more than two hours (6). As suggested by the previous name for HH, “alarm clock” headache syndrome, nearly all patients reported headaches at consistent times (1,6,8,9,36). However, it should be noted that a few exceptions exist (10). The most frequent time of occurrence was between 2 a.m. and 4 a.m. According to the result of polysomnography (PSG) from 58 HH attacks in 37 patients, 53% occurred during non-rapid eye movement (NREM) sleep, mainly in stage 2 (38%) (5). Most patients had only one attack per night, but a few patients reported up to five or six headache episodes within one night (3,6,8,10,38). In the two latest PSG study series, five out of 13 (38.5%) patients had attacks both in the REM and NREM stages (10,38). The PSG findings did not support that HH is a REM sleep-related disorder.
Recent studies have paid more attention to the motor activities after patient awakening due to the headache, and two systemic investigations regarding such motor activities have been conducted (8,9). The different activities are considered signs that may help to differentiate headaches that occur during sleep. For example, almost all of the HH patients were found to leave the bed for some purposeful activity (drinking, watching TV, reading, urinating, etc.), whereas migraine patients are prone to stay in bed and avoid moving their head. One hypothesis suggests that motor activities may help relieve HH by decreasing intracranial pressure through the adoption of an upright body posture (9,39). Nevertheless, whether the motor activities are specific for HH needs to be further confirmed because these observed motor activities in HH patients are not unusual for insomnia patients who wake up in the middle of the night. Current consensus is that the degree of motor activities during awakening does not reach the degree of restlessness, which is typically seen in cluster headaches (8,9,39).
Nausea was reported in three of the first six patients of Raskin and the presence of mild migrainous features were included in the ICHD-2 criteria. On the whole, nausea was reported in 52 patients (20.8%), followed by phonophobia or photophobia. Only one patient experienced vomiting (7). However, in three of the studies included in this review, 5% to 24% of patients reported more than one of nausea, vomiting or phonophobia (7,9,10). Taking the above into consideration, migrainous features have been removed from the criteria of ICHD-3β.
The issue most debated with regards to HH diagnosis is the presence of trigeminal autonomic symptoms. The first six cases described by Raskin exhibited no trigeminal autonomic symptoms. Akin to ICHD-2, absence of trigeminal autonomic symptoms is needed for definite HH diagnosis in the new ICHD-3β criteria. Nevertheless, a headache could be categorized as probable HH if the headache characteristics fulfill all criteria other than criterion E (no cranial autonomic symptoms or restlessness). The proportion of trigeminal autonomic symptoms in HH patients varied in the different series that were assessed in this review (3,7–9) and was up to 15% of patients in two of these studies (7,8). However, some studies excluded patients with trigeminal autonomic symptoms for further evaluation. (6,10). There has been no study focusing on the difference between patients with and without trigeminal autonomic symptoms. Whether the presence of trigeminal autonomic symptoms contradicts the diagnosis of HH needs further investigation.
Comorbidities
Other primary headache disorders are often reported in HH patients (3,7–10,35). In a Spanish series, 12 of 13 patients reported other primary headaches (eight migraine-type headaches, two tension-type headaches, one nummular headache and one hemicrania continua) (7). In general, migraines were the most reported comorbid primary headache in more than one-third of HH patients, followed by tension-type headaches. Of note, the diagnosis of HH should be made only after excluding other primary or secondary headache-related nocturnal attacks.
Other than headache, two other comorbidities, OSAS and hypertension, are frequently reported in HH patients. OSAS was detected in 83% and 73% of HH patients in two studies (10,38) and the presence of OSAS usually confounds HH diagnosis. However, there were no temporal correlations between the headache attacks and oxygen desaturation in these studies. Thus, the high prevalence of OSAS in HH patients is probably due to the high prevalence of OSAS in the elderly (40) rather than a causal association. Arterial hypertension was reported in 55% of HH patients (5), but only a few studies reported the result of 24-hour blood pressure monitoring of HH patients (41,42). Nocturnal hypertension-headache syndrome, first proposed in 1992 (43) was considered as an important differential diagnosis of HH based on four successfully treated cases (41,44,45). There is also no study reporting the proportion or clinical features of the nocturnal headache among patients with nocturnal hypertension. Therefore, the association between nocturnal hypertension and HH is still unclear.
Therapeutic options
There is currently no information about whether diet or lifestyle modification influences the clinical course of HH. Successful acute and prophylactic treatment of HH have been reported in some case series and case reports. However, none of them are controlled studies. Thus, treatment recommendations are based on observational studies and need further validation. Beyond effectiveness, adverse effects are another major concern for HH treatment because most HH patients are elderly and present with comorbidities.
Acute treatment options
Acute treatment used for hypnic headache attacks.

Only the treatments tested in at least three patients are presented.
The efficacy is classified according to the statements of the respective authors. NSAIDs: nonsteroidal anti-inflammatory drugs.
Prophylactic treatment options
Medications used in the prophylactic treatment of hypnic headache.

Only the drugs tried in at least five patients are presented.
The efficacy is classified according to the statements of the respective authors. NSAIDs: nonsteroidal anti-inflammatory drugs.
Lithium (150 to 600 mg/day; plasma level 0.5 to 1.0 mmol/l)
Lithium was the first reported drug for HH prevention (1) and the only drug that has been used in more than 100 patients so far (1,3–8,10,20,21,34,35,44,46,47,49,54–59). It has been shown to provide HH relief in 76.6% of patients that used the medication at dosages between 150 and 600 mg/day, resulting in a plasma level of between 0.5 and 1.0 mmol/l, and the most frequently used effective dosage has been shown to be 300 mg (6,10). Because of the regularity of nocturnal attacks, HH is considered to be a chronobiological disturbance-related disorder. Thus, lithium has been used because it is thought that it is beneficial in such chronobiological disturbance disorders for its action to increase serotonin production and serotonergic transmission in the central nervous system (60), as well as its indirect increase of nocturnal melatonin levels (61,62). However, the use of lithium is known to be limited because of its side effects, including sleepiness, tremor, diarrhea, increased thirst, polyuria and worsening headache attacks, especially in the elderly. Lithium is also contraindicated in patients with heart or kidney failure, psoriasis, cardiovascular disease, electrolyte disturbance and hypothyroidism. Indeed, one study reported the incidence rate of adverse effects following lithium treatment of HH to be as high as 100% (34). Furthermore, the discontinuation rate due to such side effects has been reportedly high according to some studies (8,34). Despite safety and tolerability concerns, some case series have shown that lithium is generally tolerable at dosage of 300 mg or below (6,10).
Caffeine (a cup of strong coffee at bedtime)
Caffeine appears to be a promising and safe prophylactic treatment option in HH, as found in some studies (8,17,18,21,34,36,46,48,63,64). However, one Spanish study reported only one patient obtained effective relief out of a total of 23 patients (35); thus, the average response rate among the studies discussed here was 54.7%. The best prophylactic effect was observed when patients drank a cup of coffee before going to sleep. Some patients also combined the caffeine with lithium for HH prevention (21). Pharmacologically, caffeine reduces cortical hyperexcitability by regulating the adenosine receptor and is a significant cerebral vasodilator (65,66). Many patients worried about the potential sleep disturbance that might occur by drinking coffee at bedtime and hesitated to do so. However, caffeine-induced sleep problems have been described in only a few patients (34,36). Clinically, higher proportions of Asians, especially the elderly, do not drink coffee. In such patients, caffeine-containing analgesics can be considered for prevention, but should be used with caution because the total dose resulting from a combination of drugs may easily exceed the critical amount and increase the risk of medication-overuse headache.
Indomethacin (25 to 150 mg/day at bedtime)
The average response rate of HH to indomethacin among the studies was 53.8% at dosages of 25 to 150 mg/day (7,8,19,20,34,35,44,46–48,53,54,57,63,64,67–70). Of note, indomethacin showed distinct efficacy in patients with unilateral HH, especially if there were subtle trigeminal autonomic symptoms (nasal stuffiness, lacrimation, etc.) (48,70). The mechanism of indomethacin in the treatment of HH is still unclear. Some studies hypothesized that HH is related to cerebrospinal fluid (CSF) pressure changes and indomethacin exerts its therapeutic effect by lowering CSF pressure (38,71). The main concern of indomethacin treatment is its side effects. An increased risk of gastrointestinal hemorrhage and renal side effects may cause discontinuation in some patients (8) or prohibit use of indomethacin. In addition, daytime headaches may occur after indomethacin use (48).
Other prophylactic options
Topiramate was taken by 24 patients in the studies assessed in this review (25–100 mg/day) and was at least partially effective in 45.8% of patients (7,8,12,35,50,58). Tricyclic antidepressants and flunarizine were also frequently used for HH prevention in the assessed studies, but the results were disappointing (4,5,35). Melatonin (3–5 mg/day), which is considered beneficial in chronobiologic disturbance disorders, was suggested as a therapeutic option for HH and showed highly variable response rates among the studies (8,17,31,48). However, melatonin is the only reported preventive medication that has been used to treat childhood HH (31). Oxetorone, a serotoninergic antagonist and a potent histamine H1 receptor antagonist with hypnotic properties, has also been reported to have excellent efficacy but it was used in only eight patients in a single French study (9). Gabapentin (900–2700 mg/day) was found to be effective in three out of five patients in some studies (7,46,72) and sodium ferulate, lamotrigine, pregabalin and azolamide also showed good treatment responses, albeit only in one or two patients from single case reports (12,13,17,69). In contrast, other drugs, including β blockers, verapamil, NSAIDs other than indomethacin, prednisone, valproate, benzodiazepines, pizotifen and methysergide, were largely unbeneficial for HH prevention (5).
Onset of recovery and duration of treatment
The onset of efficacy with regards to preventive medication has been described in a few case reports (13,21,48,50). With general agreement, an effective preventive medication decreases HH frequency within two weeks, but sometimes one month is needed for dosage titration. The duration of prophylactic treatment has been less widely reported and varied according to the clinical course. One study reported that the duration of lithium treatment ranged from two weeks to 64 months with a median of four months (10). Some patients needed continuous treatment to prevent recurrence (10,21). Based on current evidence, we recommend the administration of a prophylactic medication for at least three to six months, followed by gradual reduction of the dose.
Other prophylactic considerations
Botulinum toxin type A (75 U, injected in the corrugator, splenius capitis, semispinalis or trapezius muscles) was noted to be effective in one patient who was contraindicated to indomethacin, unresponsive to caffeine and did not want to use lithium due to possible side effects (18). Occipital nerve stimulation provided a sustained effect for the treatment of HH in a medically unresponsive patient up to 36 months (14). Pain recurred after lead disconnection, but ceased again after revision.
It is noteworthy that some patients with nocturnal hypertension reported that the preventive medication was effective, but the headache recurred when the medication was steadily withdrawn (44). Treatment of their nocturnal hypertension totally eliminated the headaches in four patients, regardless of the type of antihypertensive agents that were used (41–45). Thus, it is important to rule out nocturnal hypertension-headache syndrome before the diagnosis of HH. Furthermore, antihypertensive agents (such as β blockers or verapamil) are generally ineffective in HH prevention, and those that do respond to antihypertensive treatment may be those with nocturnal hypertension. On the contrary, differences in prophylactic treatment response were not observed in HH patients with or without OSAS (5). Only one case with severe OSAS improved significantly with regards to HH after treatment with nasal continuous positive airway pressure and supplemental oxygen (73).
Clinical outcomes
Proposed subdivision criteria for hypnic headache according to the clinical course.

Clinical outcomes of hypnic headache in follow-up studies. a

NA: not available.
Only the case series that included more than three patients and had a follow-up duration of more than six months are presented.
HH in children
Five childhood HH cases were described in three reports considered in this review (31–33). The age ranged from 8 to 11 years old. Four of them (80%) were female. The headache frequency varied largely, from one to 25 nights when HH occurred per month whereas the duration was short compared with the adult patients and was not more than 60 minutes in all five patients. None of them had trigeminal autonomic symptoms, while two patients reported nausea during attacks. Two patients responded well to melatonin treatment (31) and one patient had a spontaneous remission two months after diagnosis (33). HH persisted for more than one year in the other two patients, but they did not take any prophylactic medication because of low headache frequency (<2/month) (31,32). Childhood HH patients showed some atypical features, such as a lower frequency and not fulfilling the ICHD-2 or ICHD-3β criteria. However, like migraines, HH may have a different clinical picture in childhood patients and should have broadened diagnostic criteria to encompass childhood cases. Finally, only a few cases between the ages of 18 and 50 years have been reported, and we should carefully search for the overlooked HH cases in this age group and reconsider the authenticity and mechanism of childhood HH.
Field-testing the ICHD-3β criteria
Four studies that field-tested the ICHD-2 criteria were selected to validate the ICHD-3β criteria (7–10). There were 72 patients in total and the proportions of patients who fulfilled every criterion of the ICHD-2 criteria in the four studies were 61%, 85%, 50% and 65%, respectively, with an overall percentage of 65% (47 out of 72). The leading missing criterion in these studies was criterion A (dull in quality; Table 1), followed by criterion D (absence of trigeminal autonomic and migrainous features).
The overall proportions of patients who fulfilled every criterion of the ICHD-3β criteria were estimated to be 83% to 86% in the four studies (60–62 out of 72) because two patients were reported to have a frequency of less than 15 days but no exact number was reported (9). Criterion E of ICHD-3β (absence of trigeminal autonomic symptoms) was missing in eight (11.1%) patients, and criterion C (occurs >10 times/month for three months) was missing in three to five (4.2%–6.9%) patients. All patients fulfilled criterion A, B, D and F. Only one patient did not fulfill the criteria of probable HH. Therefore, compared to ICHD-2, the new ICHD-3β criteria are more sensitive and exhaustive.
Conclusions
In this review we have updated the clinical characteristics of HH according to current available information and correlated these finding with the ICHD-3β criteria. In summary, the new criteria are more sensitive and exhaustive, resulting in an increased diagnostic rate from 65% to 85% in the recently reported cases. However, a small proportion of patients may present trigeminal autonomic features during headache attack, which is not permitted for the definite diagnosis of HH under ICHD-2 or the new criteria. Lithium, caffeine and indomethacin showed better efficacy for prophylactic treatment but double-blind placebo-controlled studies regarding treatment are needed to further verify the efficacy.
The natural course of HH remains unclear since prophylactic treatment may have modified the clinical course. Other than the presence of trigeminal autonomic features and the natural course of disease, there are still some unresolved issues, such as the association between HH and nocturnal hypertension, the variable treatment response among studies and the clinical features of young adults and childhood HH.
Clinical implications
The new International Classification of Headache Disorders (ICHD-3) beta version (2013) criteria are more sensitive and the diagnostic rate is consequently approximately 85% of the recently reported cases. The presence of trigeminal autonomic features contradicts definite hypnic headache (HH) diagnosis, but a small proportion (7.7%) of reported cases exhibited this feature. Although spontaneous remission is rare in HH, about half of HH patients had favorable outcomes after prophylactic treatment. Caffeine is the most effective acute treatment, while lithium, caffeine and indomethacin are the three most effective prophylactic medications, although none of them have been tested in randomized, controlled trials. Nocturnal hypertension-headache syndrome should be ruled out before the diagnosis of HH.
Footnotes
Funding
This work was supported in part by grants from Taipei Veterans General Hospital (VGHUST102-G7-6-1, V102C-118, V102E9-001, V102B-039), National Science Council (NSC) support for the Center for Dynamical Biomarkers and Translational Medicine, National Central University (NSC 101-2911-I-008-001), the Brain Research Center, National Yang-Ming University, and a grant from the Ministry of Education (Aim for the Top University Plan).
Conflict of interest
None declared.