
Abstract
Hypnic headache is rarely reported in Asians, and the proposed International Classification of Headache Disorders (ICHD)-2 criteria have never been field-tested. We studied 17 consecutive Taiwanese patients (M/F: 9/8, mean age at onset 69.6 years) with hypnic headache from a headache clinic. Fifteen patients (88%) reported >15 headache attack days per month. Polysomnography studies done on 11 patients recorded 12 attacks in seven patients: two during rapid eye movement (REM) sleep, three during non-REM sleep and two having both. Five of the seven patients reported their headache profile during polysomnography studies. The clinical course was mostly episodic without recurrence (n = 9, 53%), followed by relapsing/remitting (n = 5) and chronic (n = 3). The ICHD-2 criteria were not fulfilled in 35% (6/17) patients based on patient recall or 60% (3/5) patients based on direct questioning during polysomnography studies. The major reason was the presence of pulsatile rather than dull headache in our patients. Unlike previous studies, our study showed hypnic headache occurred equally in both REM and non-REM sleep, and most patients ran an episodic course.
Introduction
The term hypnic headache was first coined by Raskin in 1988 (1), describing headache attacks only during sleep with a tendency to occur in the elderly. The International Classification of Headache Disorders, 2nd edn (ICHD-2) first adopted it as a primary headache disorder (code 4.5) and proposed its diagnostic criteria (Table 1) (2). In addition to the core feature of exclusively sleep-related headache, the ICHD-2 criteria also characterize the headache profile including headache duration, characteristics and associated symptoms. However, the headache features were not completely the same among different criteria of hypnic headache (1, 3, 4), and, moreover, the ICHD-2 criteria have never been field-tested.
The ICHD-2 criteria of hypnic headache and the results of field-testing according to patient recall and direct questioning during PSG studies
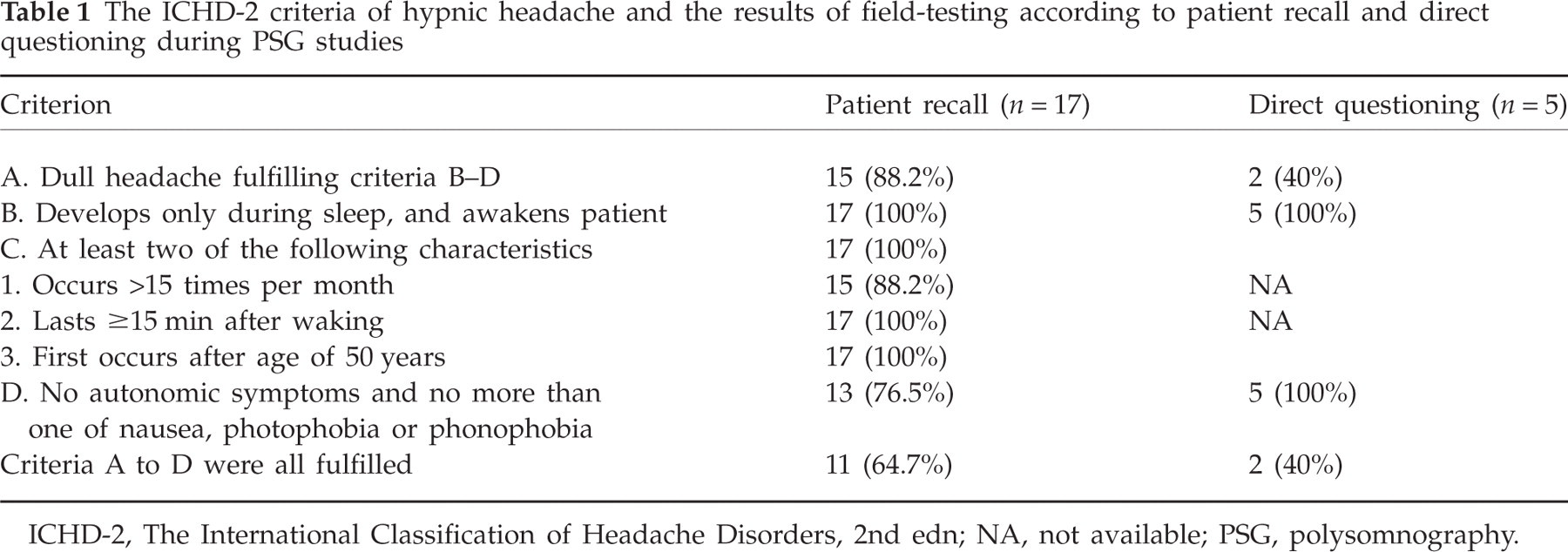
ICHD-2, The International Classification of Headache Disorders, 2nd edn; NA, not available; PSG, polysomnography.
Hypnic headache is rare and has been reported to account for 0.07% of all headache patients in a case series (5). Based on literature review, about 90 patients with this headache disorder have been reported, and, of them, 24 patients having a total of 30 polysomnography (PSG) studies were reported (6–15). These case series (4, 16) help elaborate the panorama of this disorder, but controversy exists when examining the PSG results, pathophysiology, response to lithium and disease course. Moreover, no large series of patients have been reported from Asia.
To explore the clinical picture, treatment responses to lithium and outcomes of hypnic headache as well as field-test the ICHD-2 criteria, a retrospective study was conducted on patients with hypnic headache seen in a headache clinic, including their PSG findings.
Methods
Consecutive patients with frequent sleep-related headaches, who visited the headache clinic of Taipei-Veterans General Hospital (VGH) from July 1998 to June 2006, were reviewed. The patients diagnosed with cluster headache or other trigeminal autonomic cephalalgias were excluded from review. The diagnostic criteria of hypnic headache in this study were: (i) headaches exclusively occur during sleep and awaken the patient from sleep; (ii) frequent attacks, at least 10 times per month for at least 1 month; (iii) no autonomic symptoms during headache attacks; and (iv) not attributed to other secondary causes. These core features were compatible with those proposed by the ICHD-2 (2) and two other criteria published before (3, 4). Headache features or accompanying symptoms in the diagnostic criteria were not characterized but, instead, the headache frequency was broadened from at least 15 times per month to 10 times per month, so that we could compare our patients with the criteria proposed by the ICHD-2. In addition, mild or moderate sleep apnoea based on the PSG results was not considered as a secondary cause of hypnic headache (see below). This study protocol was approved by the Institutional Review Board of the hospital.
Hospital settings
Taipei-VGH is a 2198-bed national medical centre that serves both veterans and non-veteran citizens. In 1995, Taiwan launched the National Health Insurance programme, which is a compulsory social insurance programme embracing the entire population. All of the insured are provided with the right to equal access to healthcare services. Because of a weak gatekeeper referral system, patients have the complete freedom to choose hospitals and physicians regardless of the nature or severity of their illness (17); therefore, almost all patients in our headache clinic were self-referred. The headache clinic in Taipei-VGH has been operating since 1996. All patients arriving at the headache clinic must complete a detailed headache intake form during their first visit and must keep a headache diary for use at follow-up visits.
Polysomnography study
Patients with hypnic headache underwent PSG to evaluate their headache attacks in relation to sleep stages and any occurrence of sleep apnoea. The PSG study included four-channel-EEG, two-channel electrooculography, a chin electromyogram (EMG), measurements of thoracic and abdominal respiratory effort, nasal airflow and pulse oximeter with finger probe (SaO2), surface EMG of tibialis anterior muscle, ECG, digital voice and video imaging. Patients also used an event marker to signal any nocturnal headache attacks. Sleep stages were analysed according to conventional criteria (18). According to the report of the American Academy of Sleep Medicine (19), an episode of apnoea is defined as cessation of airflow for ≥10 s. An episode of hypopnoea is defined as meeting one of the following two criteria: (i) reduction of airflow to <50% of baseline; and (ii) reduction of airflow to >50% of the baseline associated with either desaturation (>3%) or electroencephalographic arousals. Apnoea-hypopnoea index (AHI) is calculated as the total number of apnoeas and hypopnoeas per hour of sleep. The severity of sleep apnoea is further classified as mild (5 < AHI ≤ 15), moderate (15 < AHI ≤ 30) and severe (AHI > 30) (18). In addition, if patients were awakened by headaches during PSG recording, technicians, using a structured hypnic headache questionnaire, would question the patient to identify the headache features.
Treatment
All patients with hypnic headache received lithium treatment in our headache clinic if not contraindicated. Patients usually took 300 mg/day at bedtime or a higher dosage (600 mg/day) if the effect at 300 mg was not satisfactory. In our clinic, we usually tried to taper lithium if freedom of headaches was achieved for 3 months. Lithium would be resumed if headache recurred after tapering or discontinuing.
Data collection
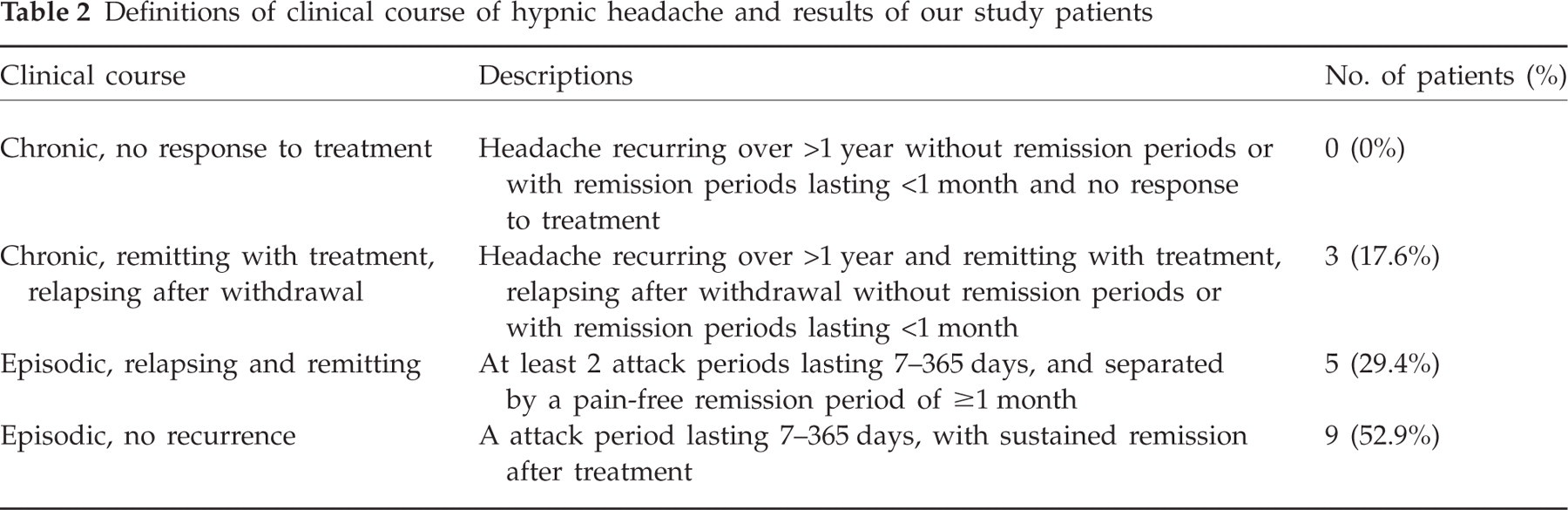
One author (J-F.L.) reviewed the charts, headache intake forms and headache diaries and recorded headache frequency, characteristics, severity, localization, duration, timing, accompanying symptoms, the results of neurological examination, neuroimaging [magnetic resonance imaging (MRI) or computed tomography (CT) scan] and PSG studies. We determined drug response based on headache diaries and/or chart review. A good response was rendered if no more hypnic headaches occurred after treatment; whereas a partial response was assigned if headache frequency decreased >50%. In December 2006, one physician (J-F.L.) called all patients to follow-up on their current headache conditions. The disease outcomes were divided into four different patterns based on the proposal of Lisotto and colleagues, i.e. chronic course with no response to treatment, chronic-remitting course with treatment, relapsing after withdrawal, episodic course with relapse and remission, and episodic course without recurrence (Table 2) (20).
Definitions of clinical course of hypnic headache and results of our study patients
Results
Patients
During the study period, 6106 patients with headache visited our headache clinic, of whom 36 (0.6%) complained of frequent sleep-related headaches. After exhaustive reviews of the secondary causes of their sleep-related headache, 19 patients were excluded (chronic migraine, n = 13; medication overuse headache, n = 6) because they also had frequent non-sleep-related headaches during daytime. A total of 17 patients (0.3%) [M/F 9/8, mean age 71.6 ± 8.6 years (range 61–83)] with hypnic headache were diagnosed. The mean age at onset was 69.6 ± 9.7 years (range 54–81) and mean latency of headache onset to diagnosis was 26.4 ± 34.5 months (2 months to 11 years). Eleven patients (64.7%) had a history of hypertension and two (11.8%) had diabetes mellitus. The neurological examinations and brain CT or MRI studies were unremarkable in these 17 patients. The average body mass index was 25.0 ± 3.9 (range 18.2–31.2). Two female patients had a history of migraine without aura, whereas none of the others had a significant headache history before hypnic headache.
Headache profile
Of the 17 patients with hypnic headache, 12 (70.6%) reported that they were awakened by headache in a fixed time period, i.e. headache developed between midnight and 03.00 h regularly in six patients, whereas one patient reported headaches before midnight and five other patients reported headaches after 03.00 h. The other five patients did not have a fixed time period. Three patients (17.6%) also experienced headache during daytime naps. Headache duration was 15–30 min in 11 patients (64.7%) and 30 min to 2 h in the other six (35.3%) patients. Eleven (64.7%) patients reported headache attacks every night; four (23.5%) patients 20–25 days in a month and two patients 10–15 days in a month. One patient (5.9%) reported headache intensity as mild, nine (52.9%) as moderate and seven (41.2%) as severe.
Headache sides were bilateral in 14 patients (82.3%) and unilateral in three. Headaches were located over the frontal region in five patients (29.4%), temporal in four (23.5%), parietal in three (17.6%) and occipital in two. The other three patients had holocephalic headache. The headache character was dull in 15 (88.2%), throbbing in one and explosive in the other. The patients reported accompanying symptoms of nausea in five (29.4%), photophobia in four (23.5%) and phonophobia in four (23.5%). None had vomiting. No patient reported cranial autonomic symptoms.
Sleep recordings
PSG studies were performed in 11 patients (64.7%). There was no difference in age, sex or headache profile between patients with and without PSG studies (data not shown). All PSG studies were done before lithium treatment. Twelve headache attacks were recorded between 21.44 h and 05.38 h during the PSG studies in seven patients (Table 3). Three patients (42.9%) had their headache attacks exclusively during non-REM (NREM) sleep, two patients (28.6%) in REM sleep and the other two patients (28.6%) having both. Of the attacks during NREM, all happened during light sleep (one in stage 1 and five in stage 2). None of them had periodic leg movement during sleep.
The results of polysomnography in seven patients whose hypnic headache attacks were recorded during the sleep studies

AHI, Apnoea/hypopnoea index; REM, rapid eye movement.
Direct questioning of the features of hypnic headache was done in five patients during their PSG study. Three of the five patients were awakened by headaches in the REM sleep, but only two reported dreaming. The other two patients were awakened by headaches in the NREM sleep. Headache character was pulsatile in three patients and dull in two. Two patients rated their headache as severe and two mild; of the rest, one had three attacks and reported mild, moderate and severe for each. Only one patient experienced vomiting, but none reported photophobia, phonophobia or autonomic signs. All five patients fell asleep again without any treatment.
Of the 11 patients with PSG studies, eight had an AHI of >5 (72.7%) with a mean AHI of 15.4 (range 5.2–27.9). Of these eight patients, four had an AHI < 15 and the other four had AHIs of 16.8, 17.9, 23.2 and 27.9. All respiratory events were predominantly obstructive.
Treatment
In the end, dosages of lithium were 300 mg in 12 (70.6%) patients and 600 mg in the other five (29.4%). The duration of treatment ranged from 2 weeks to 64 months with a median of 4 months. Three patients with a chronic course had been on lithium for 24, 26 and 64 months, respectively. In patients with an episodic course, the mean duration was 4.9 ± 4.2 months (range 2 weeks to 10 months) for each headache period. Fourteen patients (82.3%) reported good response to lithium treatment and the other three (17.7%) reported partial improvement. Of all patients, one reported hand tremor with a dosage of 600 mg/day (serum lithium level 1.13 mmol/l), which subsided after dosage reduction to 300 mg. Two patients who showed good response to lithium had received flunarizine 10 mg/day for 1 month before lithium. However, both of them considered flunarizine ineffective. None of our patients received melatonin, indomethacin or caffeine for treatment.
Of the eight patients with an AHI of >5, six (75%) had good response and two had partial response to lithium treatment. Of note, none of these eight patients received treatment for their sleep-disordered breathing because their severity of sleep apnoeas was mild to moderate (AHI < 30) and none had excessive daytime sleepiness (19, 21).
Outcome
Follow-up information was obtained from all patients with a mean duration of 50 ± 28 months (range 6–99) (Table 2). The most common clinical course was ‘episodic without recurrence’ (n = 9, 52.9%) followed by ‘episodic with recurrence’ (n = 5, 29.4%). Three patients (17.6%) with a chronic course reported good response to lithium, but headache relapsed after lithium withdrawal.
Field-testing of the ICHD-2 criteria
Based on patient reports (n = 17), 11 (64.7%) patients fulfilled all the ICHD-2 diagnostic criteria for hypnic headache (Table 1). Four patients failed to meet criterion D (less than one of nausea, photophobia or phonophobia) and two patients failed to meet criterion A (dull headache). In contrast, based on direct questioning of five patients during the PSG studies, three did not fulfil criterion A (60%) because their headaches were pulsatile.
Discussion
Patients with hypnic headache were uncommon, accounting for only 0.3% of all patients in our headache clinic based on the core features of hypnic headache, i.e. frequent exclusively sleep-related headache without accompanying autonomic symptoms. In contrast to the tension-type headache pattern suggested by the ICHD-2 criteria, our study as well as previous studies has shown that some patients with hypnic headache did have migrainous features (4). A comprehensive review of 71 cases in the literature has shown that pain was throbbing in more than one-third of cases and about 20% subjects had nausea (4). About one-third of our patients reported migraine characteristics and, furthermore, direct questioning during PSG studies showed that three of five patients (60%) had throbbing headache and one patient (20%) had vomiting. Therefore, the field-testing results suggest that the headache features of the ICHD-2 hypnic headache criteria may be too strict and require revision.
Our PSG studies have shown that hypnic headaches occurred in both REM and NREM sleep with similar frequencies. In contrast, the literature review (6–15) of 21 attacks with 19 PSG studies showed the proportion of REM sleep to be much higher (71%) than that of NREM sleep. Our results downplay the hypothesis that pain-processing structures of hypnic headache are activated during REM sleep stage (4, 16, 22). It was originally hypothesized that during REM sleep stage, the activities of the dorsal raphe and locus coeruleus nuclei are absent, and these two structures, with periaqueductal grey, are essential for antinociceptive system (23). Our results suggest that hypnic headache can occur in any sleep stage; however, awakening by headache is more likely during light sleep (stage I and II of NREM) or REM sleep, which have lower arousal pain thresholds than deep sleep (22).
Most of our patients reported that the lithium was effective; however, we cannot be sure whether the efficacy was totally related to lithium treatment or spontaneous remission in those with episodic hypnic headache. The dosage we used was low, which accounted for the high tolerability in this study. The underlying mechanism of lithium for hypnic headache is unknown. It has been postulated that lithium may increase serotonin production, serotonergic transmission in the central nervous system (24) and indirectly increase the nocturnal melatonin level (25, 26). Based on a literature review and our study results, we suggest a short course of 300–600 mg lithium should be tried first, followed by tapering. If headache recurs during tapering, a longer duration of treatment may be needed. Shifting to other anecdotal medications such as caffeine, melatonin (15, 27), indomethacin or flunarizine (28, 29) is suggested when lithium is contraindicated or not effective. Most patients in our study had a good outcome, i.e. an episodic course after treatment (53%). Only 18% patients had a chronic course. This is contrary to previous studies, where most patients with hypnic headache ran a chronic or continuous course (4, 20). The reason for this discrepancy is unknown. The mean duration of disease before diagnoses was shorter than that reported in a recent review (2.2 vs. 5 years) (4). It is possible that some mild or less persistent patients with hypnic headache were early recognized in our study. In addition, ethnic factors should also be considered.
It is still a matter of controversy whether sleep-disordered breathing is a cause for morning headaches (2, 30, 31). However, the presence of a sleep-breathing disorder does complicate the diagnosis of hypnic headache. Up to eight patients (73%) among our 11 patients with PSG studies showed an AHI > 5. Nevertheless, we do not consider ‘hypnic’ headache to be related to sleep-disordered breathing in these patients, for the following reasons. First, no temporal correlation of apnoea episodes and headache attacks was recorded during the PSG studies. Second, there were no typical complaints of sleep-disordered breathing in our patients (19). Third, treatment efficacy of lithium did not differ between those with and those without sleep-disordered breathing. Fourth, none of our patients received treatment for sleep apnoea in this study, which strengthened the efficacy of lithium and their headache disorder. In contrast, the high frequency of sleep-disordered breathing in our patients was probably due to the advanced age of our patients (32, 33). In fact, the prevalence of sleep apnoea in our study (73%, AHI > 5) corresponds to that reported in a US community dwelling of elderly based on portable sleep recordings (81%, AHI > 5, age range 65–99 years) (33) and a Spanish elderly cohort based on the PSG results (81% in men and 80% in women, AHI > 5, age range 70–100 years) (32).
In conclusion, our study has shown that hypnic headache occurred in both REM and NREM sleep with similar frequency. The existence of sleep-disordered breathing should not exclude the diagnosis of hypnic headache. The ICHD-2 diagnostic criteria for hypnic headache are too strict in headache characteristics and may need revision. The majority of our patients with hypnic headache responded to a short course of lithium treatment and their condition ran an episodic course.
Footnotes
Acknowledgements
This study was supported in part by a grant from Taipei-Veterans General Hospital (VGH V96C1-041).