
Abstract
Background
Headache is a common symptom during space travel, both isolated and as part of space motion syndrome. Head-down-tilted bed rest (HDTBR) studies are used to simulate outer space microgravity on Earth, and allow countermeasure interventions such as artificial gravity and training protocols, aimed at restoring microgravity-induced physiological changes.
Objectives
The objectives of this article are to assess headache incidence and characteristics during HDTBR, and to evaluate the effects of countermeasures.
Methods
In a randomized cross-over design by the European Space Agency (ESA), 22 healthy male subjects, without primary headache history, underwent three periods of –6-degree HDTBR. In two of these episodes countermeasure protocols were added, with either centrifugation or aerobic exercise training protocols. Headache occurrence and characteristics were daily assessed using a specially designed questionnaire.
Results
In total 14/22 (63.6%) subjects reported a headache during ≥1 of the three HDTBR periods, in 12/14 (85.7%) non-specific, and two of 14 (14.4%) migraine. The occurrence of headache did not differ between HDTBR with and without countermeasures: 12/22 (54.5%) subjects vs. eight of 22 (36.4%) subjects; p = 0.20; 13/109 (11.9%) headache days vs. 36/213 (16.9%) headache days; p = 0.24). During countermeasures headaches were, however, more often mild (p = 0.03) and had fewer associated symptoms (p = 0.008).
Conclusions
Simulated microgravity during HDTBR induces headache episodes, mostly on the first day. Countermeasures are useful in reducing headache severity and associated symptoms. Reversible, microgravity-induced cephalic fluid shift may cause headache, also on Earth. HDTBR can be used to study space headache on Earth.
Introduction
Space travel may trigger headaches (1–3). Up to 70% of astronauts report symptoms during space flights, most often confined to the first days in microgravity (4–6). We recently showed that space headache is a frequent condition in outer space. The majority (71%) of astronauts who otherwise did not experience headaches on Earth reported having headaches during launch, stay at the space station or landing (7). These headaches can be both isolated and as part of space motion syndrome (7–11).
The head-down-tilted bed rest model (HDTBR) is regarded as a gold standard for simulating the physiological effects of weightlessness on the human body (12–15): The whole bed is tilted head downwards at a 6-degree angle. By using the Earth-based HDTBR model of the European Space Agency (ESA) that simulates microgravity similar to the gravitational forces in space, headache prevalence and pathophysiology can be studied adequately in a controlled situation (16). Gravitational countermeasures such as transient enhanced artificial gravity (AG) and training protocols (TPs) aim to prevent an impact on microgravity-induced physiological changes (17). Countermeasures can also be implemented in the HDTBR model.
In this study, we aimed to assess occurrence and characteristics of headache in artificial microgravity conditions and to evaluate effects of countermeasures on headache.
Subjects and methods
Subjects
Between March 2010 and May 2011, 22 male healthy volunteers with a mean ± SD age of 31.5 ± 6.7 years participated in two HDTBR studies of the ESA, in Cologne, Germany (Deutsches Zentrum für Luft- und Raumfahrt e.V. (DLR; Study center 1)), and Toulouse, France (Institut de Médecine et de Physiologie Spatiales (MEDES; Study center 2)). All subjects were non-smokers, were used to regular moderate physical activity, and had no history of primary headaches. Participants provided written informed consent. The study was approved by local ethics committees.
Design
Experimental set-up of the HDTBR cross-over studies.

At Study center 1, two different training protocols (TP) were implemented in separate sessions. At Study center 2, artificial gravity protocols (AG) were added in separate sessions. HDTBR: head-down-tilted bed rest; TP1: aerobic physical exercise; TP2: standing upright 30 minutes; AG1: 30 minutes’ centrifugation at 1 G per day; AG2: six sessions of five minutes’ 1 G centrifugation per day.
TPs
Periods with TPs included either a daily period of 30 minutes of aerobic physical exercise in the upright position (a combination of squats and jumping movements with intervening rest breaks to specifically train muscle groups involved in normal walking), or a 30-minute period of standing upright) (Table 1).
AG
Periods with AG conditions included either a daily 30-minute short-arm centrifugation protocol (Short-Arm Human Centrifuge (SAHC), Verhaert Space, Belgium), exposing the horizontal supine subject to 1 G; or a period when subjects underwent six 1 G centrifugation sessions of five minutes each in the same centrifuge (Table 1).
Headache assessment
During the head down period, subjects completed a specifically designed headache questionnaire. If headache was reported, its characteristics and symptoms were questioned in a yes/no manner. Questionnaires were completed daily at the same time (10 p.m.). Based on the questionnaire, headache diagnosis was made by three headache experts (WPJvO, AAV and GMT) in consensus. Most headache disorders require recurrent headache periods for clinical diagnosis, and this could not be assessed accurately during the five-day HDTBR sessions. We therefore used, for example, the term “migraine” for headache episodes that fulfilled ICHD-IIR (18) migraine criteria, without taking into account the necessity of recurrence of attacks. Headache episodes were defined as periods of headache, preceded and followed by a headache-free period of minimum of four hours. Headache severity was classified by participants as “mild,” “moderate” or “severe.”
Statistics
Data analysis was performed using a descriptive clinical approach, additionally using chi square tests and Fisher’s exact tests where appropriate when comparing unpaired proportions, and using McNemar’s test and a linear mixed model with random patient factor for paired comparisons. Analyses were performed in SPSS 20.0.0 (SPSS Inc, IBM, USA) and R version 2.15.1.
Results
All participants had passed pre-study screening and were considered healthy male subjects, with a mean ± SD age of 31.5 ± 6.7 years and body mass index (BMI) of 24.0 ± 1.7 kg/m2. None of them were diagnosed with a primary headache disorder prior to entrance to the study. All volunteers tolerated the HDTBR period well. There was a single incident during the centrifugation procedure, when the centrifugation had to be stopped because of the development of bradycardia and almost the loss of consciousness. Acute appendicitis caused one participant to be excluded from the respective study arm. After recovery, he was included several weeks later in the last tier of the study (19,20). These incidents did not influence data analysis.
Occurrence and characteristics of headache during HDTBR studies.
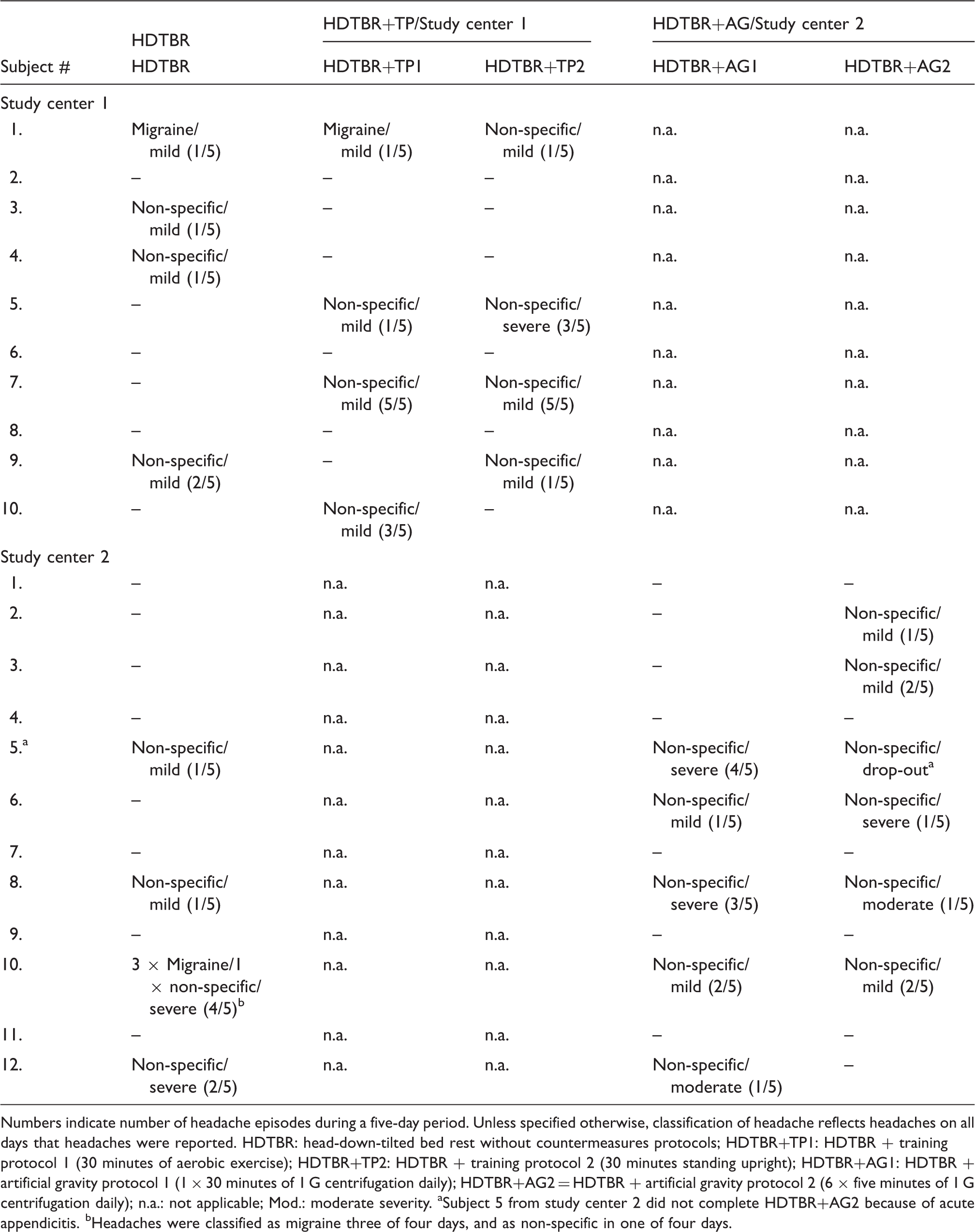
Numbers indicate number of headache episodes during a five-day period. Unless specified otherwise, classification of headache reflects headaches on all days that headaches were reported. HDTBR: head-down-tilted bed rest without countermeasures protocols; HDTBR+TP1: HDTBR + training protocol 1 (30 minutes of aerobic exercise); HDTBR+TP2: HDTBR + training protocol 2 (30 minutes standing upright); HDTBR+AG1: HDTBR + artificial gravity protocol 1 (1 × 30 minutes of 1 G centrifugation daily); HDTBR+AG2 = HDTBR + artificial gravity protocol 2 (6 × five minutes of 1 G centrifugation daily); n.a.: not applicable; Mod.: moderate severity. aSubject 5 from study center 2 did not complete HDTBR+AG2 because of acute appendicitis. bHeadaches were classified as migraine three of four days, and as non-specific in one of four days.
Effects of countermeasures on headache prevalence
The proportion of participants reporting headache did not differ between HDTBR without (eight of 22; 36.4%) vs. HDTBR with countermeasures: 12/22 (54.5%); p = 0.20. This proportion was also not different between the three different conditions separately: HDTRB eight of 22 (36.4%) vs. HDTBR+AG: seven of 12 (58.3%; p = 0.07); or vs. HDTBR+TP: five of 10 (50.0%; p = 0.84).
The incidence of days with headache was also not different: HDTBR without 13/109 vs. HDTBR with 36/213 (p = 0.24), nor between the three different conditions: HDTBR 13/109 (11.9%), HDTBR+AG 16/115 (13.9%); HDTBR+TP 20/98 (20.4%); p = 0.21 (Table 3; Table s1). Overall, headache episodes were most often reported on day 1 (15/35; 42.9%), most clearly during the period without countermeasures: six of 13 (46.2%) (Figure 1).
Occurrence of headache and associated symptoms during HDTBR. (a) Occurrence of headache episodes during five consecutive days in the HDTBR session without countermeasures (HDTBR; n = 22 subjects); with artificial gravity protocols (HDTBR+AG; n = 12 subjects); with training protocols (HDTBR+TP; n = 10 subjects); and in total. Most headache episodes occurred on the first day. (b) Proportion of headache episodes accompanied by additional symptoms (nausea, vomiting, phonophobia, photophobia) per day. HDTBR: Head-down-tilted bed rest. Incidence and characteristics of headache periods. Headache episodes during five consecutive days of HDTBR and HDTBR + countermeasure protocol (HDTBR+TP/HDTBR+AG). All participants (n = 22) underwent HDTBR session (period A), n = 12 participants underwent artificial gravity protocols (HDTBR+AG), and n = 10 participants underwent training protocols (HDTBR+TP). HDTBR: head-down-tilted bed rest without countermeasures protocols; TP: training protocols; AG: artificial gravity protocols; P.a.: physical activity; HA: headache.

Effects of countermeasures on headache characteristics
Headache episodes were mostly described as pulsating (21/50; 42%) or pressing (22/50; 44%) and located bilaterally (27/50; 54.0%). Countermeasures did not affect headache type (p = 0.32) or headache localization (p = 0.99) (Table 3, Table s1).
Effects of countermeasures on headache severity
Headache episodes (n = 50) were classified by participants as mild (31/50; 62.0%), moderate (two of 50; 4.0%), or severe (17/50; 34.0%). Appliance of countermeasures affected the classification of headache severity, resulting in more mild headaches during HDTBR+TP (17/20; 85.0%; p = 0.03), Figure 2.
Headache severity during HDTBR. Diagram depicts proportion of headache episodes of mild, moderate and severe intensity during different HDTBR conditions. Headache episodes are more often mild in HDTBR with training protocols (HDTBR+TP) vs. HDTBR without countermeasures (HDTBR) or HDTBR with artificial gravity protocols (HDTBR+AG). HDTBR: Head-down-tilted bed rest.
Effects of countermeasures on associated symptoms
Use of countermeasures decreased the prevalence of associated symptoms. The proportion of headache episodes accompanied by those symptoms was lower: HDTBR six of 13 (46.2%) vs. HDTBR+TP seven of 20 (35.0%) vs. 0/17 (0%); p = 0.008. The proportion of subjects tended to be lower: five of eight (62.5%) vs. four of 12 (33.3%); p = 0.054. Nausea (10/50; 20.0%), vertigo/lightheadedness (12/50; 24.0%) and photophobia (six of 50; 12.0%) were the most common associated symptoms (Table 3, Table s1). Associated symptoms were most prevalent on the first day of HDTBR (Figure 1).
Classification of headaches
Overall, 45/50 (90.0%) headache episodes were classified as non-specific headache, and five of 50 (10.0%) as migraine. Non-specific headaches were more prevalent during countermeasures, compared to sessions without countermeasures: 36/37 (97.3%) vs. nine of 13 (69.2%); p = 0.004. The five migraine episodes were reported by two subjects: two and three episodes each.
Difference between countermeasure protocols
TPs
There was no difference in proportion of subjects with headache between 30-minute aerobic exercise (TP1) and 30 minutes of standing upright (TP2): TP1 four of 10 (40.0%) vs. TP2 four of 10 (40.0%); Fisher’s exact test p = 1.00. Incidence of headache episodes also did not differ: TP1 10/50 (20.0%) vs. TP2 10/48 (20.8%); p = 0.92.
AG conditions
The proportion of subjects reporting headache did not differ between 1 × 30 minutes of 1 G centrifugation (AG1) and 6 × 5 minutes 1 G centrifugation (AG2): AG1 five of 12 (41.7%) vs. AG2 six of 12 (50.0%); Fisher’s exact test p = 0.68. Incidence of headache episodes was also not different between AG1 and AG2: seven of 55 (12.7%) vs. nine of 60 (15.0%); p = 0.73.
Discussion
Our study shows that episodes of headache frequently occur during simulated microgravity in HDTBR studies in subjects who otherwise do not suffer from headache. TPs or AG by centrifugation do not decrease the incidence of headache episodes but could decrease headache severity, and associated symptoms are less common.
In total, 14/22 (63.6%) subjects reported a headache during this cross-over HBTDR study in different protocols. In the HDTBR period without countermeasures, six of 13 headache episodes were associated with accompanying symptoms such as nausea, vomiting or vertigo. The majority of headache episodes were classified as non-specific (nine of 13). The proportion of subjects with headache (63.6%), and the occurrence of nausea (38.5%) and vertigo (38.5%), are comparable to earlier findings in astronauts (71%, 44% and 33%, respectively) (7,8,21).
In the current study, two types of countermeasures were implemented next to continuous bed rest, assuming these would restore gravitational body homeostasis. Although we found that the incidence of headache episodes did not differ between HDTBR periods with and without countermeasures, the severity of the headaches was less during countermeasures, and accompanying symptoms were fewer. Gravitational countermeasures such as TPs and centrifugation aim to prevent and impact on microgravity-induced physiological changes (22,23), and show beneficial effects on muscles and bone in on-Earth microgravity models (24,25) and in space (26,27). Simulation of gravity stimulates all the physiological systems simultaneously by reproducing Earth’s normal gravitational environment. They lead to normalize vascular shear stress and endothelial function, thereby preventing microcirculatory impairment and orthostatic intolerance (17). Our data show that, with regard to microgravity-induced headache, they clearly prevent severe headaches, as well as ameliorate accompanying nausea, vertigo and vomiting. Limitations of the study include enrollment of male subjects only, thereby excluding possible hormonal effects but also slightly compromising overall generalizability. Although the study design was not primarily aimed at assessing the effects of countermeasures on headache frequency and severity, it enabled us to study the reduction of the physical deconditioning and headaches associated with prolonged weightlessness.
Interestingly, in this HDTBR study, headaches were mainly reported on the first day, just as was reported in real space headache. This may be due to adaptational physiological changes such as neurovestibular changes and fluid shifts (9) similar to real microgravity (7,28).
Pathophysiologically, there are two major hypotheses explaining space headache and accompanying symptomatology (9). Firstly, the sensory conflict theory accounts for two different sorts of sensory rearrangements occurring in the first days of microgravity: Sensory conflict between the visual and vestibular systems (including the semicircular canals and the otolith organ) could result in headache or additional symptoms, due to resetting of the vestibular organs (29). Secondly, the fluid shift hypothesis (21) looks more plausible in explaining particularly the phenomenon of headache along with accompanying symptoms. The absence of hydrostatic pressure in the circulatory system in zero G leads to a rostral distribution of blood and lymph. Alterations of blood flow and volume have been shown during exposure to microgravity (2). The cephalic blood shift then might result in a relative imbalance of endolymphatic and perilymphatic pressures in the labyrinth, creating a situation akin to labyrinthine hydrops (Menière’s disease) (30). Furthermore, the fluid shift to the brain and probable brain edema could lead to an increase in intracranial pressure (2,21,31), possibly triggering headaches (32). The fluid shift hypothesis is appealing because shifts of hundreds of cc’s occur in space, which allegedly cannot be without functional consequences (11). On Earth, hydrostatic pressure approaches zero when the body is supine, as is simulated in the HDTBR model. Previously, transient central venous hypertension has been reported to play a role in headaches of high altitude or microgravity (33), thereby also suggesting physiological adaptation mechanisms are related to onset of symptoms.
We conclude that simulated microgravity during HDTBR induces headaches, which resembles space headache with respect to timing, incidence, characteristics and accompanying symptoms. While countermeasures did not decrease the occurrence of headache episodes, headache severity was lower and accompanying symptoms were fewer compared to HDTBR periods without countermeasures. We would therefore consider HDTBR to be an adequate model to study space headache on Earth. These findings suggest intracranial pressure increases play an important role in headache pathophysiology.
Clinical implications
Headaches are not restricted only to Earth, but humans also suffer from headaches in space. The head-down tilted bed rest (HDTBR) model is a valid model to study microgravity-induced extra-terrestrial headaches on Earth, leading to headache episodes that are similar in characteristics to headaches reported by astronauts. The HDTBR model also enables studying the effects of countermeasures on headache prevalence. The underlying mechanism of microgravity induced headache might be intracranial pressure changes due to cephalic fluid shifts.
Footnotes
Funding
This work was supported by grants from the Netherlands Organisation for Scientific Research (NWO) (903-52-291, M.D.F.; Vici 918.56.602, M.D.F; GO-MG/14 from the User Support Program Space Research A.V; 907-00-217 GMT; Vidi 917-11-319 GMT), and by a grant from the Center for Medical Systems Biology (CMSB) established by the Netherlands Genomic Initiative/Netherlands Organisation for Scientific Research (NGI/NWO). They had no role in the design or conduct of the study.
ESA sponsored the design and development of a Short-Arm Human Centrifuge (SAHC) by an industrial company (Verhaert Space, Belgium). The design of this centrifuge complied with integration in a module of a space station, and makes this countermeasure feasible during real space flights. MEDES has hosted the centrifuge since April 2007 in its facility called “Space Clinic,” located in the Rangueil Toulouse Hospital.
Conflict of interest
WPJ van Oosterhout, MD, has nothing to declare. GM Terwindt, MD, PhD, has received grants and consultancy/industry support from Merck, Janssen-Cilag, Almirall. AA Vein, MD, PhD, has received a grant from GO-MG/14 from the User Support Program Space Research (NWO). MD Ferrari, MD, PhD, has, in the past three years, received grants and consultancy/industry support from Medtronic, Menarini, Merck, and independent support from the NWO.
Acknowledgements
The authors would like to thank Patrik Sundblad, MD, PhD, and Thu Jennifer Ngo-Anh, MD, PhD, Directorate of Human Spaceflight and Operations, ESA; Marie-Pierre Bareille, project scientist, Institut de Médecine et de Physiologie Spatiales (MEDES) Toulouse, France; and Edwin Mulder, PhD, project scientist, Deutsches Zentrum für Luft- und Raumfahrt e.V. (DLR), Cologne, Germany for their kind collaboration.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.