
Abstract
Background
Clinical findings suggest cerebellar dysfunction in patients with migraine. Eyeblink classical conditioning (EBCC) is a simple form of associative learning which depends on the integrity of the cerebellum. The aim of this study was to assess whether EBCC is disturbed in patients with migraine.
Methods
A delay conditioning paradigm was used in the headache-free interval in 32 female patients with migraine, in 24 of them without (MwoA) and eight with aura (MwA), and in 32 age-matched female controls. As primary outcome measure acquisition and as secondary outcome measures timing and extinction of conditioned eyeblink responses (CR) were assessed.
Results
CR acquisition was significantly reduced in all migraine patients (mean total CR incidence 35.2 ± 22.1%) compared to controls (54.7 ± 21.3%; p < 0.001; Bonferroni-corrected p level < 0.025) and in MwA patients (19.9 ± 20.2%) compared to matched controls (58.2 ± 27.0%; p = 0.006) but not in MwoA patients (40.3 ± 20.6%) compared to matched controls (53.6 ± 19.7%; p = 0.028; Bonferroni-corrected p level < 0.0166). Decrease of CR incidences in MwA patients was not significantly different compared to MwoA patients (p = 0.021; Bonferroni-corrected p level < 0.0166). CR timing and extinction was not affected in migraine patients.
Conclusions
Reduced acquisition of CRs in the cohort of female patients studied here supports findings of a cerebellar dysfunction in migraine.
Introduction
There is some evidence for a cerebellar dysfunction, commonly of mild degree, in patients with migraine (see references (1–4) for review). Early clinical studies recognised that patients with special subtypes of migraine exhibited brain stem or cerebellar signs within attacks (5). In more recent years balance abnormalities and paroxysmal vertigo have been shown to occur frequently in the most common subtype of familial hemiplegic migraine (FHM) (6). Cerebellar symptoms have been found in FHM-1, which is caused by mutations in the CACNA1A gene (7). To date, only a few studies have investigated cerebellar function in common forms of migraine (1,2). Overall, clinical signs of cerebellar dysfunction appear to be mild and commonly in the subclinical range. For example, a subclinical hypermetria of reaching movements has been reported which was most pronounced in patients with migraine with aura (3). These findings suggest that cerebellar structures may be affected in migraine, possibly most pronounced in patients with migraine with aura.
Besides its well-established importance for motor coordination, the cerebellum plays a major role in certain forms of non-declarative, e.g. associative learning. The form of cerebellum-dependent learning which has been examined in greatest detail is classical conditioning of eyeblink responses (8,9).
A behaviourally neutral conditioned stimulus (CS), such as a tone, is presented and followed by the unconditioned stimulus (US), such as a corneal air-puff. This is delivered to the eye, eliciting a reflexive blink, the unconditioned response (UR), which consists of closure of the eyelid in humans. When CS and US are repeatedly paired, subjects learn to blink the eyelid to the tone. This conditioned response (CR) develops in a carefully timed manner such that the eyelid is lowered when the air-puff arrives. The neural circuits involved in eyeblink conditioning are one of the best studied biological systems (10). In short, both cortical areas of the intermediate cerebellum and the interposed nucleus contribute to this form of associative learning. Some animal studies provide evidence that simultaneous input of climbing and mossy fibres induces synaptic changes that is long-term depression (LTD) at the parallel fibre-Purkinje cell synapses which leads to reduced inhibition of the cerebellar nuclei. This allows the CS alone to generate an eyeblink CR, so that the eye is closed just before the air-puff arrives. Studies in patients with cerebellar degeneration and focal cerebellar lesions have shown that both acquisition and timing of CRs is dependent on the cerebellum in humans (11–13).
Eyeblink conditioning has proved helpful to search for cerebellar dysfunction in various neurological diseases. In essential tremor (14) and neuropsychiatric disorders including attention-deficit hyperactivity disorder (15), impaired CR acquisition suggests that these conditions are associated with cerebellar disorders. The aim of the present study was to determine whether eyeblink conditioning is impaired in patients with common forms of migraine. Impaired eyeblink conditioning would provide evidence for a cerebellar involvement in migraine. In addition, we were interested whether possible findings in eyeblink conditioning were more pronounced in migraine with aura than without aura.
Methods
Subjects
Clinical characteristics of migraine patients and controls.

Group mean values are expressed ± standard deviation (SD). MwoA: migraine without aura; MwA: migraine with aura. ICARS: International Cooperative Ataxia Rating Scale; SARA: Scale for the Assessment and Rating of Ataxia. Ataxia scores are expressed as the number of subjects who showed mild disorders of stance (SARA: tandem stand, one-leg stand is not tested in SARA; ICARS: tandem and/or one-leg stand) and kinetic function of limbs.
Duration of illness was at least one year. Disease duration was not significantly different between migraine subgroups (p = 0.283, unpaired t test). MwoA patients showed a higher attack frequency as assessed by a headache diary (p = 0.033); mean migraine days per month were not different between groups (p = 0.809). Female migraine patients with a regular menstrual cycle or taking oral contraceptive were included. The patients were free from any migraine-preventive medication during the last six months. They were allowed to use acute headache medication. Patients fulfilling criteria for medication-overuse headache with accompanying tension-type headache, and patients with chronic migraine or more than 10 attacks per month, were excluded from the study. None of the control subjects had a history of neurological diseases.
Because CR acquisition has been shown to be influenced by oestrogen levels with the higher learning rates due to high oestrogen (17), subjects were investigated within the phase of the menstrual cycle with high oestrogen, i.e. 14 ± 1 day after the last menses. Eyeblink conditioning was at least seven days before or after a migraine attack or acute migraine treatment. This was confirmed by phone contact one week after participation. The study was approved by the local ethics committee and written informed consent was obtained from all subjects.
To determine cerebellar signs or ataxia symptoms the neurological examination included the International Cooperative Ataxia Rating Scale (ICARS) (18) and the Scale for the Assessment and Rating of Ataxia (SARA) (19). The clinical examination was conducted either by D.T. or M.G.
At the beginning of the experiment hearing thresholds were determined in each subject using 1 KHz, the frequency of the CS. Thresholds of both ears (dB SPL) were within normal age limits in all participants; there was no significant difference between patients and controls. None of the participants suffered from eye diseases.
Eyeblink conditioning
Details of the delay conditioning procedure were reported previously and are repeated briefly (12,13). All patients were investigated by the same investigator (L.R.) in the same, quiet room, at the same part of the day, that is, noon or in the early afternoon. First, 10 CS- and 10 US-alone trials were presented in an unpaired and random order, followed by 100 paired CS-US trials and 30 CS-alone trials as extinction trials. An air-puff (duration 100 ms, intensity 400 KPa at source, 110 KPa at nozzle) was used as US, directed near the outer canthus of the right eye at a distance of about 10 mm. A tone (1 KHz; 70 dB sound pressure level, SPL; duration 540 ms) as CS was presented ipsilaterally and coterminated with the air-puff. Surface electromyography (EMG) recordings were taken from orbicularis oculi muscles ipsilaterally to the US.
Eyeblink CRs were semiautomatically identified within the CS-US interval in paired and extinction trials using custom-made software (20). The investigator (L.R.) was not blinded for the experimental group. Response onset was defined where EMG activity reached 7.5% of the EMG maximum in each recording with a minimum duration of 20 ms and a minimum integral of 1 mV*ms. Trials were visually inspected and implausible identification of CRs was manually corrected. Responses occurring within the 150 ms interval after CS onset were considered as reflexive responses to the tone (i.e. alpha-responses) and not CRs (11). Trials with spontaneous blinks occurring prior to CS onset were excluded from the analysis.
Primary outcome measure was CR acquisition, a measure of learning. The total number of paired trials was subdivided into blocks of 10 trials each. The number of CRs was expressed as the percentage of trials containing responses with respect to each block of 10 trials (percentage CR incidence) and the total number of trials (total percentage CR incidence).
As secondary outcome measures, timing and extinction of CRs was assessed. Two timing parameters (onset and peaktime) were used, both in CRs and URs. Onset and peaktime of CRs in paired trials and URs in unpaired were automatically quantified as outlined above. US onset was set as 0 ms. CR onset and peaktime were expressed as negative values (prior to US onset) (13). EMG amplitudes were not analysed because of methodological considerations in surface EMG recordings.
To evaluate extinction effects of CR incidence within the last block of paired trials, block 10 was compared with the last block of extinction trials (extinction block 3). Moreover, the decline of CR incidence across the three extinction blocks was analysed. Analysis of extinction was performed only in those subjects who exhibited at least one CR in the first extinction block to ensure a remaining ability of learning in the paired trials (14).
In each session the frequency of spontaneous blinks was measured within one minute both at the beginning and the end of the experiment. The rate of alpha-blinks was analysed within the 150 ms interval after CS onset of 100 paired trials.
Data analysis
In paired trials analyses of variance for repeated measures (ANOVAs) were calculated with percentage CR incidence as dependent variable, block (1–10: 10 blocks of 20 paired trials) as within-subject factor and group (all controls vs. all migraine patients; controls vs. MwoA patients vs. MwA patients) as between-subject factor. Changes across the 10 blocks of 10 trials were used to quantify learning. Level of significance was set at p < 0.025 (Bonferroni corrected). Post hoc testing was performed comparing MwoA patients vs. age-matched controls, MwA patients vs. age-matched controls and MwoA patients vs. MwA patients. Comparisons to matched controls were performed because direct comparisons between migraine subgroups were limited by age and group size. Note that CR acquisition declines after the age of 40 years (21). Level of significance was set as p < 0.0166 (Bonferroni corrected). For all effects, the degrees of freedom were adjusted, if appropriate, according to Greenhouse-Geisser (22). Accordingly, ANOVA was calculated in extinction trials. Results of timing parameters of conditioned eyeblink CRs, spontaneous blink rate, alpha blinks and eyeblink URs were compared between groups (all controls vs. all migraine patients) using unpaired t tests.
Results
Clinical examination
Mild balance disorders, e.g. slight difficulties in tandem stance (items one through seven of ICARS, items one through three of SARA) were present in 28% (nine of 32) of the migraine patients and 15% (5/32) of the controls. There were no accompanying cerebellar signs, except mild limb dysfunction in two patients and one control (Table 1).
CR acquisition
Mean percentage of CR incidences ± standard error (SE) in paired trials in control subjects (n = 32), in all migraine patients (n = 32) and in MwoA (n = 24) and MwA patients (n = 8) are shown in Figure 1(a) and (b). Control subjects had significantly increased percentage CR incidences across the 10 blocks (mean total CR incidence 54.7 ± 21.3%). In the group of all migraine patients there was also an increase across blocks. As the primary endpoint, mean total CR incidence was lower than in controls (35.2 ± 22.1%), that is CR acquisition was reduced in migraine patients. Compared to matched controls mean percentage CR incidence was reduced in MwoA patients (53.6 ± 19.7% vs. 40.3 ± 20.6%) and in MwA patients (58.2 ± 27.0% vs. 19.9 ± 20.2%). ANOVA with percentage of CR incidence as dependent variable, block (1–10) as the within-subject factor and group (all controls vs. all migraine patients) as the between-subject factor revealed a significant main effect of group (F(1,62) = 13.1; p = 0.001). The block effect was significant (F(1,62) = 9.3; p = 0.003), the block by group interaction effect was not significant (F(1,62) = 2.6; p = 0.11).
Mean percentage conditioned response (CR) incidence and standard errors (SE) in paired trials shown per block of 10 trials (total = mean total percentage CR incidence) in all migraine patients (green dots and column) and in control subjects (blue dots and column) (a) and in patients with migraine without aura (MwoA; green dots and column) and migraine with aura (MwA; grey dots and column) (b).
Comparison of controls vs. migraine subgroups revealed a significant main effect of group (F(2,61) = 9.8; p < 0.001). The block effect was significant (F(2,61) = 9.9; p < 0.001), the block by group interaction effect was not significant (F(2,61) = 1.1; p = 0.33).
The group effect was not significant comparing MwoA patients and matched controls (F(1,46) = 5.2; p = 0.028), but significant comparing MwA patients and matched controls (F(1,14) = 10.3; p = 0.006). The block effect was significant comparing MwA patients and matched controls (F(1,14) = 10.2; p = 0.006), not comparing MwoA patients and matched controls (F(1,46) = 5.4; p = 0.024). Group by block interaction effects were not significant (p values > 0.3). The group effect comparing CR incidences between MwoA patients and MwA patients did not reach significance (F(1,30) = 5.9; p = 0.021; Bonferroni-corrected p level < 0.0166).
To exclude possible age-related effects, analysis was re-conducted considering only patients and control subjects under the age of 40 years. Again, mean percentage CR incidence was reduced in patients (all migraine patients: 40.8 ± 20.6%; MwoA patients: 43.9 ± 19.3%; MwA patients: 27.6 ± 22.4%) compared to controls (57.4 ± 19.2%). ANOVA with group (all controls vs. all migraine patients) as the between-subject factor revealed the same results (group effect: F(1,50) = 9.4; p = 0.003; block effect: F(1,50) = 17.3; p < 0.001; block by group interaction: F(1,50) = 1.6; p = 0.43). Comparison of controls vs. migraine subgroups revealed a significant main effect of group (F(2,49) = 6.2; p = 0.004). The block effect was significant [F(2,49) = 16.8; p < 0.001]; the block by group interaction effect was not significant (F(2,49) = 0.8; p = 0.64).
Group findings are further illustrated by examples of EMG recordings in individual subjects (Figure 2). EMG data are shown of the 100 paired CS-US trials from the first (top) to the last trial (bottom). CRs are specified by EMG bursts occurring within the relevant CS-US window, i.e. beyond the 150 ms interval after CS onset, indicated by the two vertical lines. An example of a 23-year-old control subject is shown; the total percentage CR incidence was 70%. CRs started after the first block of paired trials. Examples of a 27-year-old MwoA patient (migraine since 12 years, in mean one to two headache days per month) and 21-year-old MwA patient (migraine since four years, in mean one to two headache days per month) are shown. The total CR incidences were 51% and 30%, respectively. Note that CRs were reduced both in the MwoA and MwA patient.
Eyeblink conditioning in an individual control subject, a patient with migraine without aura and migraine with aura. Rectified and filtered EMG-data of the orbicularis oculi muscle of 100 paired CS-US trials are shown from the beginning (top) to the end (bottom) of the experiment. The first vertical line indicates the 150 ms after CS onset from where responses were counted as CR and the second vertical line the beginning of the air-puff (US), set as 0 ms. See Methods for further details. EMG: electromyography; CS: conditioned stimulus; US: unconditioned stimulus.
CR timing
Means and standard deviations (SD) of onset and peaktime latencies of conditioned (CR) and unconditioned (UR) eyeblink responses in control subjects, all migraine patients, in patients with migraine without aura (MwoA) and migraine with aura (MwA).
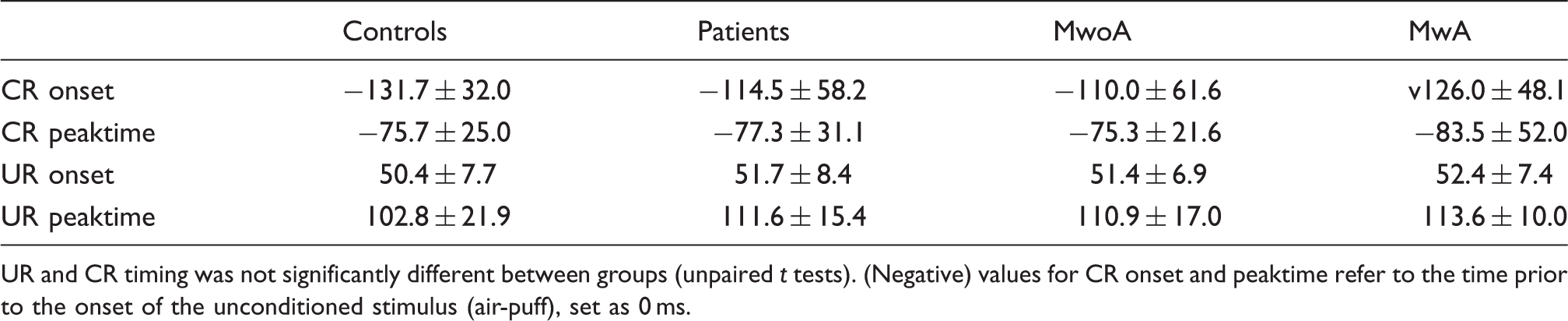
UR and CR timing was not significantly different between groups (unpaired t tests). (Negative) values for CR onset and peaktime refer to the time prior to the onset of the unconditioned stimulus (air-puff), set as 0 ms.
Extinction
As further secondary outcome measure extinction was assessed. Thirty controls, 23 MwoA and five MwA patients, exhibited at least one CR in the first extinction block and were included in analysis (14). In patients and controls the number of CRs showed a decline comparing the last block of paired trials (block 10) and the last block of extinction trials (extinction block 3) (Figure 3). This was also true in the MwoA subgroup and matched controls. The number of remaining MwA patients was too small to draw clear conclusions. ANOVA with percentage CR incidence as dependent variable, block 10 and extinction block 3 as the within-subject factor and group as the between-subject factor revealed significant effects of block (that is, extinction effect) (F(1,55) = 91.7, p < 0.001). The group (F(2,55) = 4.6, p = 0.014) and extinction by group effects were significant (F(2,55) = 4.0, p = 0.023) because of the lower CR incidence of migraine patients in block 10 of paired trials.
Effects of conditioned response (CR) extinction: mean percentage CR incidence and standard errors (SE) in the last acquisition block (Block 10) of paired trials compared to extinction block one, two and three in control subjects (n = 30), in patients with migraine without aura (n = 23) and migraine with aura (n = 5). Data are shown of subjects who exhibited at least one CR in the first extinction block.
Post hoc analysis comparing MwoA patients and matched controls revealed similar results with significant extinction effects (p values < 0.001). The group effect, however, was not significant (F(1,44) = 3.8, p = 0.058).
The ANOVA comparing extinction blocks 1–3 between all patients and controls as well as MwoA patients and matched controls revealed significant block effects in all groups (p values < 0.001). The block by group and group effects were not significant (all p values > 0.2).
Unconditioned eyeblink responses, spontaneous blink-rate and alpha-blinks
Mean values of onset and peaktime of URs in controls, all migraine patients and patient subgroups are given in Table 2. There were no significant group differences comparing UR onset and peaktime latencies between all migraine patients and controls (p = 0.51, p = 0.068; unpaired t test). Also the comparison of patient subgroups and matched controls did not reveal significant differences (p = 0.72, p = 0.10 in MwoA patients; p = 0.52, p = 0.40 in MwA patients).
The mean number of spontaneous blinks did not differ comparing all migraine patients (at the beginning 10.8 ± 5.7 blinks/min, at the end 10.3 ± 4.4) and controls (at the beginning 11.0 ± 5.6 blinks/min, at the end 10.6 ± 4.6) and was not different between the subgroups of patients and matched controls (all p values > 0.2). Also the rate of alpha-blinks did not differ between groups (all p values > 0.2).
Discussion
In the present study the acquisition of eyeblink CRs was significantly reduced in patients with migraine. Findings in MwoA patients were less marked than in MwA patients. Appropriate timing and extinction of responses was not disturbed. Impaired acquisition of eyeblink CRs suggests that cerebellar function is affected in patients with migraine.
Findings of several human lesion and brain imaging studies provide good evidence that the human cerebellum is essentially involved in simple delay eyeblink conditioning (11–13). Thus, the present findings suggest a cerebellar dysfunction in patients with migraine. Impaired eyeblink conditioning has also been shown in essential tremor and has been interpreted in favour of disturbed cerebello-cortical pathways in this condition (14). Interestingly, patients with migraine might be prone to develop essential tremor (23).
The decrease of CR incidences in particular in MwA patients was within the range reported in patients with cerebellar disorders, notably with cerebellar degeneration. Although structural changes of the cerebellum in patients with FHM and MwA have been reported (24), one may also discuss functional disturbances of cerebellar circuits in migraine.
A possible cerebellar dysfunction in migraine likely affects most parts of the cerebellum. In common forms of migraine, only a few studies assessed cerebellar function in more detail. During or between attacks balance disturbances (1) and a decreased accuracy of saccadic eye movement (25) have been reported. Eye movement and balance are controlled by the medial cerebellum. Mild balance disorders in tandem stance in a few patients in the present study are in line with mild dysfunction of the medial cerebellum in migraine.
Disordered cerebellar function has been suggested following findings of mild hypermetria of reaching movements in MwoA, and, more pronounced, in MwA (3). In that study hypermetria has been discussed as related to a disturbed function of the lateral cerebellum. However, both animal and human lesions studies show that hypermetria follows dysfunction of the intermediate cerebellum, including the interposed nucleus and corresponding cortical structures of the paravermal cerebellar hemisphere (26). Because eyeblink conditioning is mediated by the intermediate cerebellum, the present study provides further evidence of dysfunction of the intermediate cerebellum in migraine.
How may migraine be linked to the cerebellum? There is a strong association between genetically defined forms of migraine and cerebellar ataxias, in particular spinocerebellar ataxia type 6 (SCA6) and episodic ataxia type 2 (EA2) in which up to half of the patients experience migraine attacks. In addition, a subset of patients with FHM shows mild cerebellar symptoms. In these genetically defined disorders several mutations have been found leading to changes in neurotransmitter release and neuronal excitability. Because of CACNA1A mutations, in FHM-1 as well as in SCA6 and EA2, deficient P/Q-type calcium channels have been identified which are distributed over the central nervous system and are widely expressed on Purkinje cells of the cerebellar cortex. Ataxia symptoms may develop because of disordered membrane and Purkinje cell function (27). Furthermore, proton magnetic resonance (MR) spectroscopy (1H MRS) studies in FHM patients suggest cerebellar neuronal loss or dysfunction (28,29).
In patients with hemiplegic migraine and ataxia cortical cerebellar atrophy has been reported; however, this has not been found in patients with typical MwA (30) even using voxel-based morphometry (31).
The neurophysiological background of cerebellar findings in common forms of migraine is not yet conclusively explained. Although it has been proposed that the cerebellum might be more resistant to spreading depression (SD), animal studies described SD in the cerebellum and structures of the posterior fossa (32). Clinical cerebellar signs have been reported in special types of MwA entitled ‘cerebellar migraine’ or ‘basilar-type migraine’ (5,33). Patients may exhibit cerebellar or brain stem symptoms like vertigo, diplopia, dysarthria, ataxia and visual disturbances as part of aura.
Finally, there is some evidence for circulatory changes in patients with migraine. A population-based study showed a significantly increased risk of clinically silent infarct like lesions in the deep white matter as well as located infratentorially within the cerebellum. An increased prevalence of lesions in the posterior circulation has been shown in MwA patients (24). Subclinical cerebellar signs have been related to these small infarct-like lesions. The underlying pathophysiology is not fully understood. A combination of several factors is debated such as a decreased perfusion in cerebellar vascular border zone regions or genetically defined small vessel disease related to migraine (34). On follow-up nine years later, women with migraine had a higher incidence of white-matter lesions, but did not show a higher progression of infratentorial lesions as compared to controls (35). Another recent population-based study showed lesions in MwA patients predominantly located outside the cerebellum and brain stem (36). However, it has to be noted that female patients of the present study were of younger age, when structural brain lesions are commonly rare.
Beyond acquisition, adaptive timing of eyeblink CRs is known to be cerebellar dependent, the cortex of the anterior cerebellar lobe seems to be of particular importance. Typically, a shortened onset of responses has been reported (13). However, reduced CR acquisition is not always accompanied by disordered CR timing. Similar to patients with essential tremor (14), CR timing was not affected in the present migraine patients, neither in MwoA nor in MwA patients. Furthermore, migraine patients showed CR extinction to a similar extent as control subjects. Extinction has been shown to be a process of learning distinct from acquisition. The present patients also showed a disturbed acquisition but unaffected timing and extinction of CRs.
Major limitations of the present study are the relatively small groups and different number of patients. Because direct comparison of MwoA and MwA patients is further limited by age differences, migraine subgroups were compared with matched controls. CR acquisition is known to decline with age. Age-related decline begins at the age of 40 years (21). In the eight MwA patients, three patients were older than 40 years of age, compared with only three patients in the group of 24 MwoA patients. However, re-analysis considering only migraine patients and controls under the age of 40 years revealed similar results. Furthermore, only women were investigated to avoid possible confounding effects on eyeblink conditioning by gender (37). Since high oestrogen levels have been shown to enhance procedural memory function (17), all female patients were investigated in the menstrual cycle phase of high oestrogen. For that reason findings cannot be generalised. Finally, it has to be noted, that although CRs were semiautomatically identified, the investigator was not blinded for the diagnoses.
Conclusions
Findings of the present eyeblink conditioning study strengthen previous clinical data and suggest that the cerebellum is affected in common forms of migraine, possibly because of ion channel or neurotransmitter abnormalities, SD or circulatory changes. Whether this is predominant in MwA needs to be confirmed in further studies with larger groups of patients.
Clinical implications
Eyeblink conditioning reduced acquisition. Cerebellar dysfunction. Female migraine patients.
Footnotes
Funding
This work was supported by a non-restricted grant from MSD Sharp & Dohme GmbH.
Conflicts of interest
Dr Gerwig has received speaker honoraria and/or travel reimbursement from Novartis, Pfizer and Ipsen Pharma and research support from MSD.
Lisa Rauschen reports no disclosures.
Dr Gaul is a member of the advisory board of Desitin (Germany) and Allergan (Germany) and has received speaker honoraria from Berlin Chemie AG (Germany), MSD (Germany), St. Jude Medical (Germany) and Boehringer Ingelheim (Germany). Prof Katsarava serves on the editorial boards of Journal of Headache and Pain, has received research support from the German Federal Ministry for Research and Education and Bayer Schering, and speaker honoraria and/or travel reimbursement from the International Headache Society, European Headache Federation, Allergan, Merck Serono, Bayer Shering, and has served as consultant to Allergan. Prof Timmann has received research support from the German Research Foundation (DFG), grants DFG Ti 239/9-1 and DFG TI 239/10-1, the European Union (partner in one of the Marie Curie Initial Training Networks), the Bernd Fink Foundation and the German Heredoataxia Foundation.
Acknowledgement
The authors would like to thank Beate Brol for her help in conducting the experiments, in data analysis and preparing the figures.