
Abstract
Introduction
Migraine is a syndrome rather common in children. Recent results have accounted evidence of altered activity corresponding to the supplemental motor area in this pediatric population. Given the role of this region in the motor timing of supra-second temporal intervals, we hypothesized that time representation is abnormal in childhood migraine.
Subjects and methods
We compared time-processing abilities between 11 children with migraine and 11 age-matched healthy children, employing a time reproduction task in which subjects actively reproduced different supra-second temporal intervals.
Results
We show that children with migraine are less accurate (overestimate) and more variable in reproducing time intervals.
Conclusion
Results are discussed on the basis of the recent evidence about abnormal cortical and neurochemical activity in childhood migraine, but also in relation to a possible alteration of spatial attention mechanisms in this clinical population. The low number of patients examined represents a limit of this study and indicates that further investigation is needed.
Keywords
Introduction
Migraine is a recurrent headache disorder manifesting in attacks lasting four to 72 hours, typically characterized by unilateral location, pulsating quality, moderate-severe intensity, aggravation by routine physical activity, and association with nausea and/or photophobia and phonophobia (International Classification of Headache Disorders, second edition (ICHD-II)). The prevalence rate of migraine before puberty is between 3% and 24.5% (1), and younger children may commonly report pain on both sides of the head. Children with migraine were found to exhibit mild abnormalities in several cognitive domains. Abnormalities in the responding latency and source activation patterns were reported, with the intriguing finding of significantly higher odds of activation in the supplementary motor area (SMA) in children with migraine compared to age-matched control subjects (2). This abnormal activation pattern of the SMA during the execution of motor tasks raises the possibility that the spectrum of cognitive abnormalities observed in pediatric migraine might include also a complex domain such as time processing, particularly if related to motor tasks (motor timing). A recent meta-analysis (3) on the functional anatomy of time processing highlighted the SMA as a crucial area involved in the detection of supra-second temporal intervals. The processing of supra-second temporal intervals is considered a cognitively controlled timing task, since it requires the explicit orientation of attentional sources toward the duration of stimuli lasting more than one second (4,5).
Anagnostou and Mitsikostas (6) performed the first study in adults with migraine (during the interictal period) by using a task that involved time processing of auditory stimuli. Results show temporal abnormalities, although performance has been explained in relation to co-existing depressive symptoms. More recently, time processing has been explored in adult migraineurs (interictal period) using a motor timing task (7). The authors documented timing abnormalities selectively for the sub-second interval range.
Here, we expand this issue by testing temporal processing in children with pediatric migraine and healthy volunteers. Given the reported abnormal SMA activation pattern (2), patients were submitted to a motor timing task. We predict a worse performance for our clinical sample compared to controls.
Subjects and methods
Participants
Attack frequency was divided into high (HF; 10–14 attacks a month), intermediate (IF; from five to nine attacks per month) and low frequency (LF; from less than once a month to four attacks per month), and chronic migraine (CM) for the patient who presented 15 or more migraine attacks per month.
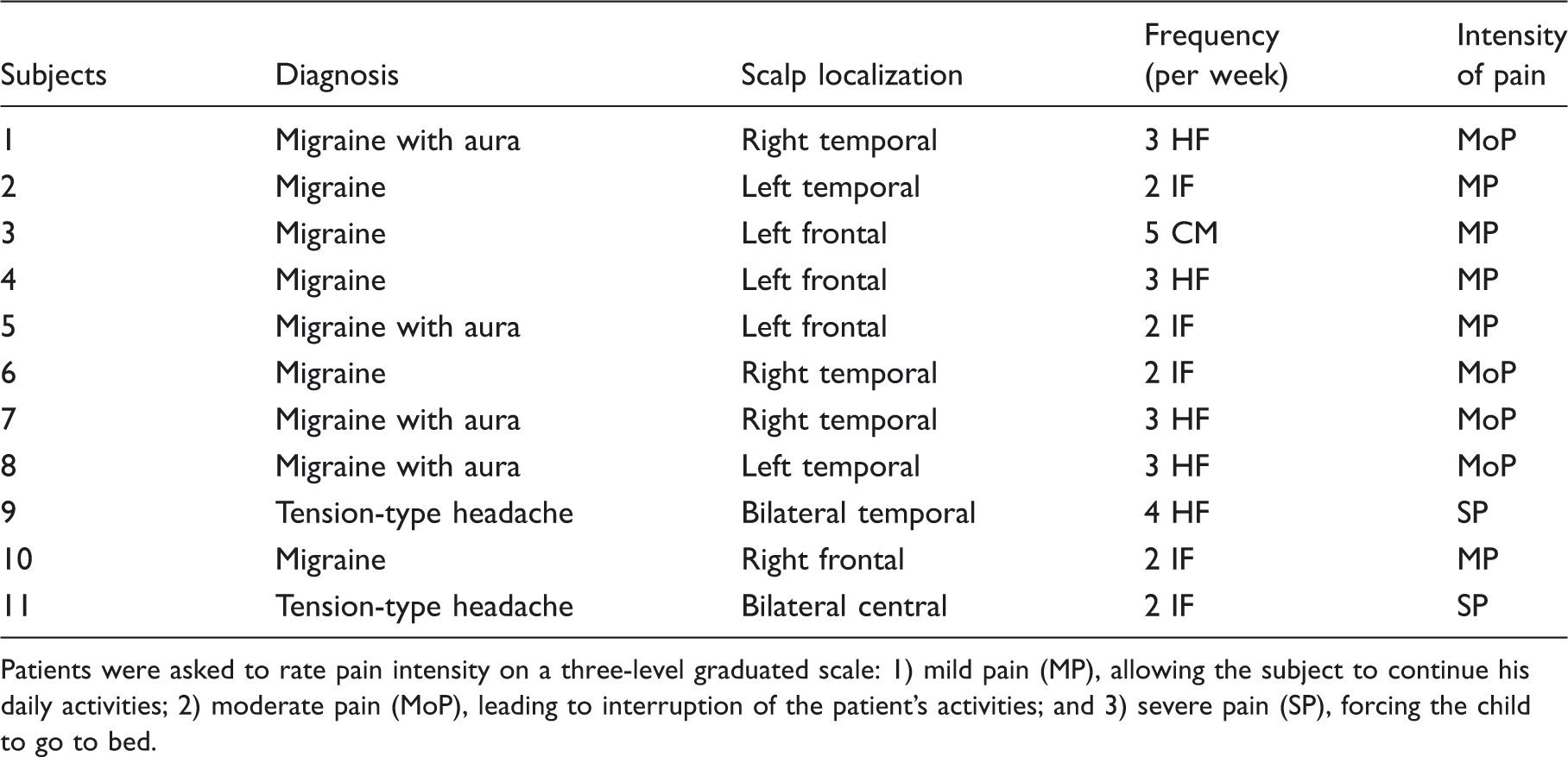
Patients were asked to rate pain intensity on a three-level graduated scale: 1) mild pain (MP), allowing the subject to continue his daily activities; 2) moderate pain (MoP), leading to interruption of the patient’s activities; and 3) severe pain (SP), forcing the child to go to bed.
We compared their performance with that of a control group of 11 right-handed, age-matched healthy volunteers (six males and five females, age 8.1 ± 0.28). Children with migraine were recruited at the Department of Pediatrics, Ospedale Policlinico, University of Catania, Italy. Children without migraine were recruited from a primary school in Palermo, Italy. Children with Diagnostic and Statistical Manual of Mental Disorders, fourth edition, text revision (DSM-IV-R) diagnoses of co-morbid neurological and psychiatric disorders, such as attention deficit hyperactivity disorder (ADHD), obsessive-compulsive disorder, anxiety, depressive and conduct disorders, were excluded (10) (see Supporting document). The study was approved by the ethics committee of the Department of Pediatrics, Ospedale Policlinico, University of Catania, Italy, and written consent was obtained from all participants and their adult caregivers.
Procedure
We used a version of the time reproduction task previously used by our group (11,12). Subjects sat at a distance of 50 cm opposite the monitor configured to a refresh rate of 60 Hz, and fixated on a black cross of 0.2 degrees in diameter, centrally located on the screen. After 500 ms, the black circle (test stimulus; size: 0.8 degrees × 0.1 degrees) appeared in the same location of the fixating cross; after a specified period, it disappeared. Immediately after the black circle disappeared, subjects were instructed to reproduce the interval they had just perceived by pressing the space bar on the computer keyboard with the index finger of their dominant (right) hand. During such time they fixated on a white screen. When they had judged that the same amount of time had elapsed, they had to release the space bar. At this point a new fixation cross immediately appeared on the computer screen to alert the arrival of a new trial (Figure 1).
Experimental procedure. Example of typical event trials for time reproduction.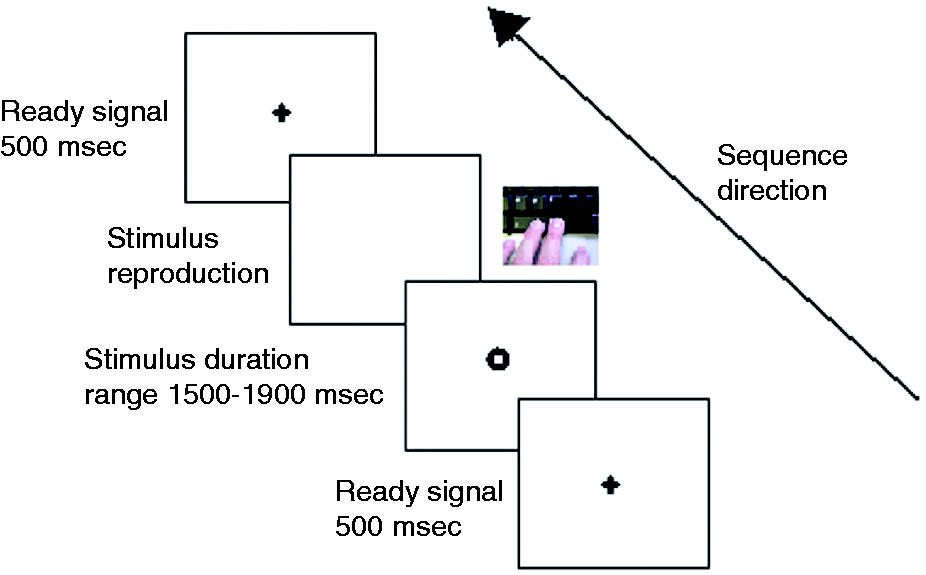
We chose to challenge subjects in the reproduction of five different time intervals (1500, 1600, 1700, 1800, 1900 ms) in order to minimize the chance of a learning process throughout the performance of the task. The total number of trials was 50 (10 trials × five intervals). Stimulus durations were presented in a randomized order.
Results
Trials that fell three standard deviations (SD) above or below each individual mean for each experimental condition were excluded as outliers. Analysis of variance (ANOVA) for repeated measures on accuracy detected a significant main effect of group (migraine vs control) factor on the time reproduction task (F(1,20) = 4.77, p = 0.040, η2 = 0.192): Migraine participants overestimated durations with respect to control participants. Likewise we also detected a main effect of duration (1500–1900 ms) factor (F(4,80) = 7.94, p < 0.001, η2 = 0.284). No significant result was reported for the interaction term group × duration (F(4,80) = 0.71, p = 0.584, η2 = 0.034; see Figure 2).
Response duration: Duration means of the pressure on the space bar while reproducing supra-second intervals for migraine and no-migraine participants. The vertical bars indicate standard error of the mean.
The coefficient of variation (CV, SD/mean response time) was also analyzed as a measure of performance variability. No significant main effect of group was detected (F(1,20) = 1.53, p < 0.229, η2 = 0.071). However, we detected a main effect of duration (F(4,80) = 4.77, p = 0.001, η2 = 0.192) and of group × duration interaction (F(4,80) = 17.01, p < 0.001, η2 = 0.459). Post-hoc analysis (t test Bonferroni corrected) showed that patients were significantly more variable than controls on 1900 ms interval reproduction (p = 0.019). No significant difference was detected for the other intervals (p = 1.00; Figure 3).
Coefficient of variation (CV): This parameter indicates the group variability while reproducing supra-second intervals for migraine and no-migraine participants. The * indicates significant post-hoc comparison differences. The vertical bars indicate standard error of the mean.
No within-group difference was detected comparing patients with predominantly left-sided pain compared to patients with predominantly right-sided pain (t = −0.23; p = 0.817).
Finally, we performed a correlation analysis between the average accuracy and variability scores and participants’ age. We observed a trend for a negative correlation between temporal overestimation and age (r = −0.579, p = 0.061), and for a positive correlation between CV and age (r = 0.56, p = 0.067). No such trend was observed in the control group (accuracy: r = 0.439, p = 0.204; CV: r = –0.45, p = 0.191).
Discussion
Research on time perception in the pediatric population is scanty if compared with that available for the adult population. The study of time processing in children affected by neurological and cognitive disorders has involved participants affected by ADHD (13), Tourette syndrome (14), dyscalculia (15) and inherited conditions (16). Our study expands this field by providing the first case-control study in pediatric migraine. In particular, we chose a classical motor timing task, based on the evidence (2) of a deranged activity within cortical regions modulating motor control, such as the SMA. According to the results of Zhang et al. (7), we found that children with migraine overestimate temporal intervals. However, contrary to what was claimed by these authors, we detected an alteration of the supra-second temporal domain. A possible explanation for the difference between the current result and that reported by Zhang et al. (7) could refer to the fact that these authors tested timing performance for durations longer (three to five seconds) than those considered in our study (1500–1900 ms). Moreover, we studied pediatric populations, which are known to differ from adult in timing performance (17).
The result of CV analysis has also shown that children with migraine showed more variable results in reproducing durations, although this difference was significant only for the longer temporal interval (1900 ms). The exclusion of severe cognitive deficits potentially able to influence the timing performance of our clinical sample, e.g. working memory and sustained attention, makes a role of cognitive profile in our participants’ performance unlikely. Moreover, our participants were not affected by depressive symptoms, another potential confounder for timing performance (6). Nevertheless, our migraine sample was heterogeneous for type of migraine, pain location, severity and frequency of attacks, hindering the identification of which, among these features, is primarily responsible for timing performance.
From a neurophysiological perspective, different factors can be called into play, beyond the role of SMA (10), to explain the observed abnormality in time processing. Dysfunctional neurotransmission might be involved. In a recent review (18) it is postulated that migraine attacks could be characterized by an ictal dopamine release in subjects with dopamine receptor hypersensitivity secondary to a chronic dopaminergic deficit synergistic to serotoninergic impairment. Given the role of both these neurotransmitters in temporal processing (19), we cannot exclude their influence on timing performance. Alternatively, the alteration of brain arousal documented in this clinical population by previous works (20) may also be involved, given that increase was proposed to explain the relative overestimation of time intervals longer than a second (20).
Our study bears limitations, including the relatively low number of patients, a limited exploration of time-processing abilities exclusively to the supra-second range, and clinical heterogeneity. This notwithstanding, we believe it creates the rationale for more extensive investigation of this complex cognitive domain in pediatric migraine.
Clinical implications
Accurate temporal estimations play a critical role in planning action and formulating decisions in everyday life. The evidence of altered timing functions in childhood migraine is relevant to understand the impact played by this disorder on cognitive development. Particularly, abnormalities of executive functioning (EF) development may negatively affect overall academic and social functioning. A recent work has discussed the strict relationship between EF development (attention, working memory and inhibitory control) and the progression of the level of sophistication of time-keeping skills. Accordingly, the study of time processing in childhood migraineurs is timely, since it might be a reflection of a broader abnormality of EF development.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.