
Abstract
Aim
The aim of this article is to investigate the vascular safety profile of triptans through an analysis of the United States Food and Drug Administration Adverse Event Reporting System (FDA_AERS) database with a special focus on serious and unexpected adverse events.
Methods
A case/non-case analysis was performed on the reports entered in the FDA_AERS from 2004 to 2010: Cases were reports with at least one event included in the MedDRA system organ classes ‘Cardiac disorder’ or ‘Vascular disorders’, whereas non-cases were all the remaining reports. Co-reported cardiovascular drugs were used as a proxy of cardiovascular risk and the adjusted reporting odds ratio (adj.ROR) with 95% confidence intervals (95% CI) was calculated. Disproportionality signals were defined as adj.ROR value >1. Adverse events were considered unexpected if not mentioned on the relevant label.
Results
Among 2,131,688 reports, 7808 concerned triptans. Cases were 2593 among triptans and 665,940 for all other drugs. Unexpected disproportionality signals were found in the following high-level terms of the MedDRA hierarchy: ‘Cerebrovascular and spinal necrosis and vascular insufficiency’ (103 triptan cases), ‘Aneurysms and dissections non-site specific’ (15), ‘Pregnancy-associated hypertension’ (10), ‘Reproductive system necrosis and vascular insufficiency’ (3).
Discussion
Our analysis revealed three main groups of unexpected associations between triptans and serious vascular events: ischaemic cerebrovascular events, aneurysms and artery dissections, and pregnancy-related vascular events. A case-by-case assessment is needed to confirm or disprove their plausibility and large-scale analytical studies should be planned for risk rate estimation. In the meantime, clinicians should pay special attention to migraine diagnosis and vascular risk assessment before prescribing a triptan, also promptly reporting any unexpected event to pharmacovigilance systems.
Keywords
Background
Triptans are specific antimigraine drugs generally recommended to patients in whom traditional analgaesics or acetaminophen are ineffective (1). The therapeutic effect of triptans appears to stem from their ability to activate the serotoninergic 5HT1b/d receptors in the trigemino-vascular system, causing vasoconstriction of the cerebral vessels and neuronal inhibition. Despite their relative selectivity, the vasoconstrictive activity of triptans also affects coronary and peripheral arteries, although to a lesser extent (2,3). Most of the clinical evidence on triptans comes from patients without known vascular diseases (4). For these reasons triptans should be avoided or prescribed with caution in subjects with a history of cardio- or cerebro-vascular diseases and in those with pre-existing vascular risk factors (5).
Although no epidemiological study to date has highlighted an increased risk of serious vascular accidents (2), a number of published case reports have documented serious ischaemic adverse events after triptan use (6–9), and summaries of product characteristics of triptan-containing medicines list ischaemic coronary accident (e.g. arteriospasm coronary, Prinzmetal angina, acute coronary syndrome, myocardial infarction) and serious peripheral vascular events (e.g. ischaemic colitis) among possible adverse reactions to triptan consumption (5,10).
Overall, findings from clinical practice surveys have shown that patients and clinicians seem to follow the recommendations for the safe use of triptans (11), but some users concomitantly receive prescriptions that suggest a contraindication or a potentially increased risk of vascular accidents related to triptan intake (12).
Since triptan use in the general population is relatively low (a one-year prevalence around 1% with about 50% of the incident users receiving only one prescription (12,13)) and serious ischaemic events appear to be very rare in patients eligible for triptan treatment (1:100,000 treated attacks with sumatriptan) (2), spontaneous reporting data can add further information on the vascular safety of triptans in clinical practice, particularly on serious and infrequent adverse events. To our knowledge, no independent studies have been published on this topic. Therefore, the aim of the present analysis was to investigate the vascular safety profile of triptans by analysing the largest international spontaneous reporting database (the United States (US) Food and Drug Administration Adverse Event Reporting System (FDA_AERS)) with a special focus on serious and unexpected adverse events.
Materials and methods
The FDA_AERS database collects spontaneous reports of adverse events associated with the administration of drugs and therapeutic biologics, using specific submission forms according to the MedWATCH programme (for details on required items, see http://www.fda.gov/downloads/Safety/MedWatch/HowToReport/DownloadForms/UCM082728.pdf). Reports are mainly submitted to the database by healthcare professionals, consumers and manufacturers, from the US and other countries (14). Each report can include more than one concomitantly occurring adverse event, and many administered drugs.
Since the first quarter of 2004, downloading of raw data extracted from the AERS database has been made available to the public from the FDA website (http://www.fda.gov/cder/aers/extract.htm).
Information included in each submitted report is recorded in seven different datasets: DEMO_file (patient demographic and administrative information); DRUG_file (name of drugs/biologics and the relevant role in the occurrence of adverse event; e.g. suspected); REAC_file (adverse events); OUTC_file (patient outcomes); RPSR_file (reporting sources); THER_file (date of therapy start/end) and INDI_file (indications for use). Two codes, the ‘case number’ and the individual safety report (ISR), link all the datasets. Moreover, in agreement with FDA_AERS recommendations (as described in the README file included in each downloadable dataset), possible duplicates of each single report were identified and merged by considering the ‘case number’.
Adverse events are coded into the FDA_AERS using the preferred term (PT) level of the standardized terminology of the Medical Dictionary for Regulatory Activities (MedDRA) version 13.0. According to the hierarchical structure of MedDRA, based on term specificity, higher levels of the dictionary (HLT: high level terms; HLGT: high-level group terms; SOC: system organ classes) are automatically assigned to each PT, providing a more general diagnostic classification of the coded event (15).
For the purpose of the present analysis, all the reports submitted to the database FDA_AERS from 2004 through 2010 were considered. Before performing statistical analyses, the dataset was prepared mapping each drug reported as suspected or interacting to its generic name and to the relevant anatomical therapeutic chemical (ATC) code (16–18).
In order to highlight those adverse events disproportionally reported following the use of a triptan, a case/non-case analysis was performed and the reporting odds ratio (ROR) values, with the relevant 95% confidence intervals (95% CI), were calculated by Mantel-Haenszel univariate analysis. The ROR is a disproportional measure based on the ratio of the odds of cases in triptan reports in comparison with reports without triptans (Figure 1) (19). In the present analysis, adverse events coded through PTs belonging to the MedDRA SOCs ‘Cardiac disorder’ or ‘Vascular disorders’ were considered outcomes of interest. Each report containing one or more outcomes of interest was considered one case, whereas non-cases were all the remaining reports other than cases. Disproportionality signals were defined when cases were ≥3 and ROR was statistically >1 (i.e. lower limit of 95% CI >1).
Calculation of ROR (reporting odds ratio): Contingency table and formula.
Since the more general diagnostic classification provided by higher levels of MedDRA can increase the sensitivity of signal detection (20), we performed the primary analysis testing on all the HLGTs and HLTs belonging to the SOCs considered. In contrast, the secondary analysis concerned only PTs subordinated to those HLTs previously resulting in a disproportionality signal: The higher specificity of the PT level may better describe the event associated with drug exposure (15,20).
As an additional analysis, six standardised MedDRA queries (SMQs) considered suitable for the purposes of the present study were also applied. SMQs are provided by the MedDRA dictionary to allow grouping of terms describing the same medical condition (15).
Moreover, the presence in the report of drugs labelled to treat cardiovascular conditions (ATC code C) was considered a rough proxy of possible pre-existing risk (see also Table 1S in the supplementary material). This parameter was used to adjust raw ROR values (adj.ROR) and to estimate the association between drug and events independently from the pre-existing vascular risk.
The disproportionality signals obtained were considered expected or unexpected on the basis of the information reported in the FDA Prescribing Information of triptans (5) and the Summary of Product Characteristics of triptans issued by the Medicine and Healthcare products Regulatory Agency (MHRA) (10).
Data management and analysis were performed using the Microsoft Access Office 2003 and Epi Info, version 3.4.3 software packages.
Results
Total reports and number of cases with at least one adverse event in the MedDRA “Cardiac disorders” or “Vascular disorders” SOCs per specific triptan (active substance).

aIn 101 cases more than one triptan was reported.
SOC: system organ classes.
In the primary analysis (see Figure 2 and supplementary material) application of the ROR to all the HLGTs included in the cardiac or vascular disorders SOCs (N = 21) yielded four signals of disproportionate reporting: ‘Coronary artery disorders’ (adj.ROR = 2.00; 95% CI = 1.85–2.16), ‘Cardiac disorders sign and symptoms’ (1.11; 1.03–1.20) ‘Vascular disorders NEC (not elsewhere codified)’ (2.01; 1.34–2.99) and ‘Aneurysms and artery dissections’ (2.01; 1.34–2.99).
‘Primary analysis’ of triptan-associated vascular events classified at different MedDRA levels: SOC: system organ class; HLGT: high-level group term; HLT: high-level term. White boxes include terms resulting in disproportionality signals, while grey boxes include terms without disproportionality; †NEC: not elsewhere codified; (crude and adjusted reporting odds ratios (RORs) for each MedDRA term are reported in the supplementary material). MedDRA: Medical Dictionary for Regulatory Activities.
Among 102 HLTs tested, ten resulted in a disproportionality signal both before and after statistical adjustment for concomitant cardiovascular drugs (see Figure 2 and supplementary material). The highest reporting disproportions suggested by the adj.ROR values were ‘Ischaemic coronary artery disorders’ (adj.ROR = 2.08; 95% CI = 1.93–2.25), ‘Cerebrovascular and spinal vascular disorders NEC’ (3.55; 3.27–3.87), ‘Gastrointestinal necrosis and vascular insufficiency’ (2.82; 1.78–4.40), ‘Aneurysms and dissections non-site specific’ (3.45; 1.99–5.86) and ‘Vascular malformations and acquired anomalies’ (2.36; 1.19–4.51). Two additional HLTs resulted in a signal only before the statistical adjustment: ‘Ocular haemorrhagic disorders’ (ROR = 2.51; 95% CI = 1.48–4.25) and ‘Cerebrovascular aneurysm and dissections’ (1.64; 1.00–2.68).
Preferred terms resulting in a statistically significant reporting odds ratio (ROR) either before or after statistical adjustment (secondary analysis).
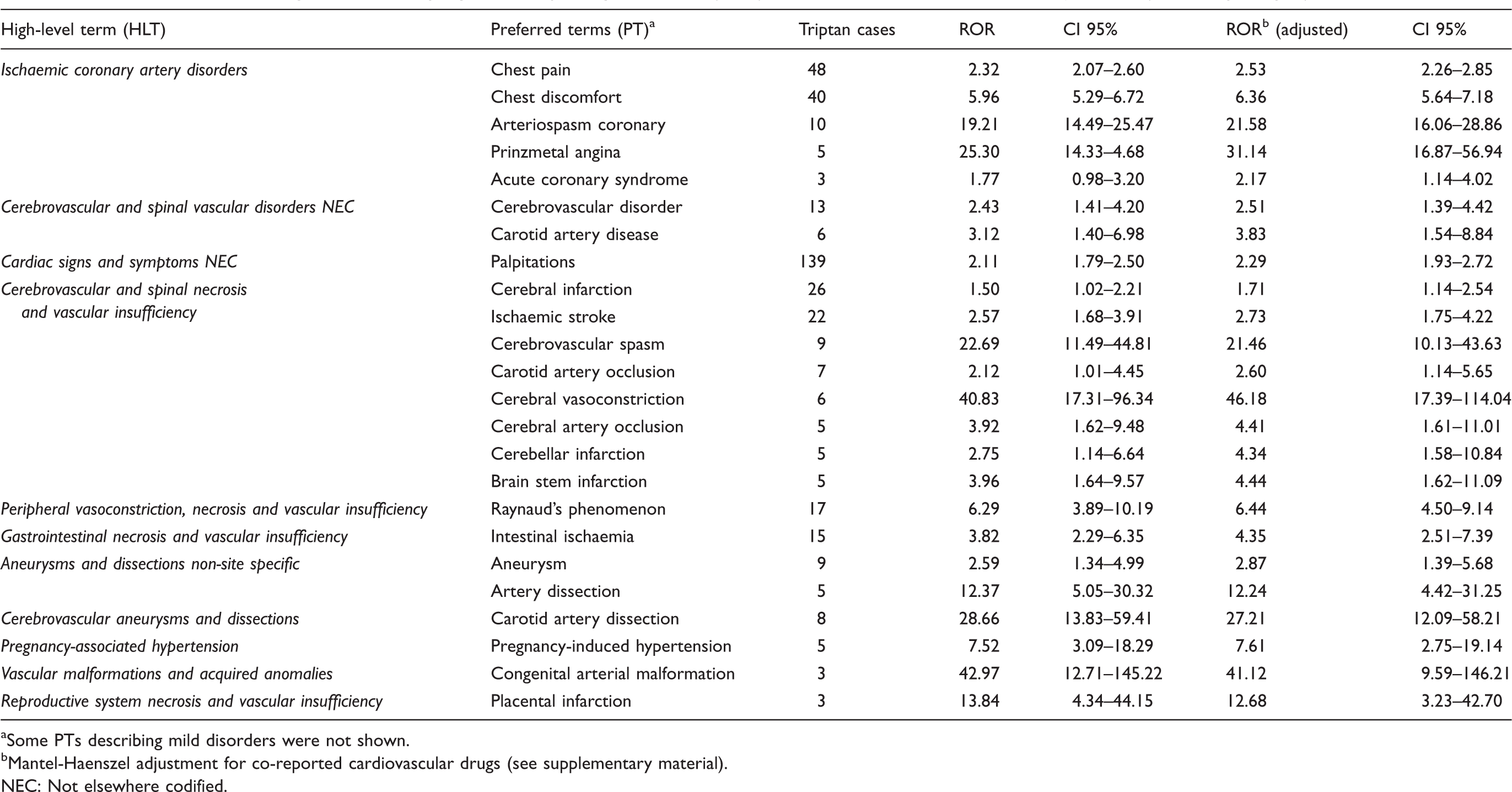
aSome PTs describing mild disorders were not shown. bMantel-Haenszel adjustment for co-reported cardiovascular drugs (see supplementary material). NEC: Not elsewhere codified.
Reporting odds ratio (ROR) for the Standardised MedDRA Queries (SMQs) considered suitable for the purposes of the present analysis.
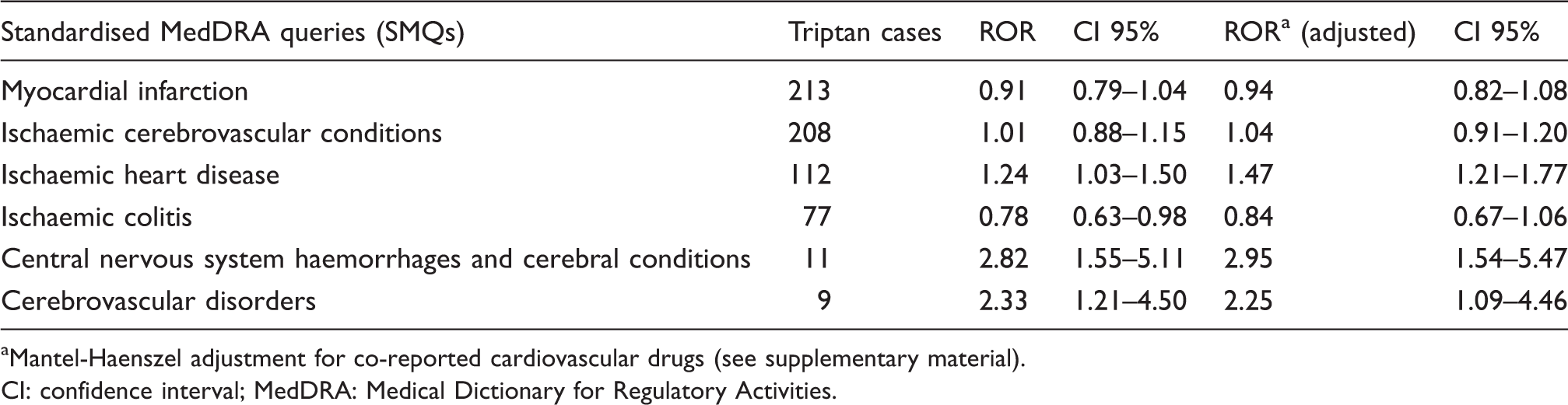
aMantel-Haenszel adjustment for co-reported cardiovascular drugs (see supplementary material). CI: confidence interval; MedDRA: Medical Dictionary for Regulatory Activities.
Discussion
This is the first independent study to investigate the vascular safety profile of triptans in a large spontaneous reporting database since the consensus statement on cardiovascular safety profile of triptans, which analysed the FDA_AERS database up to 2002 (4). Our analysis disclosed three main groups of unexpected associations: ischemic cerebrovascular events, aneurysms and artery dissections, and pregnancy-related vascular events. All the remaining associations highlighted in the study were consistent with the already known features of the triptan safety profile (5,10) (i.e. expected), thus confirming the validity both of the data-mining method applied and the data source used.
Our method identified specific events that were more frequently reported in association with the studied drugs than with all the other drugs in the dataset. In particular, analyses of passive post-marketing surveillance data cannot estimate the incidence rate of an adverse event because of the lack of both the total number of patients exposed to the drug of interest and the total number of patients experiencing a particular adverse event (underreporting) (21). For this reason, our results should be interpreted with caution as a starting point for more specific studies (e.g. case-by-case analysis, case-control and cohort studies).
In terms of the demographic characteristics of triptan reports, the mean age and female/male ratio were in agreement with the epidemiological features of migraine (12).
Almost all disproportionality signals obtained appeared independent from possible underlying cardiovascular disorders (identified by co-reported cardiovascular drugs and used for the statistical adjustment), suggesting that triptans may represent an additional risk factor for serious vascular events and confirming the need to pay special attention to underlying risk before prescribing a triptan. This result is in accordance with the finding of Visser et al., who found no difference in cardiovascular risk between subjects with and without sumatriptan-induced chest symptoms among 735 migraine patients who had used sumatriptan for two years (22). Therefore, the apparent independence of our results from the concomitant use of other cardiovascular drugs could substantiate the hypothesis of a rare subjective susceptibility (e.g. genetic variations) to a triptan vasoconstrictive effect, as also suggested by some cases of serious ischemic events in patients without pre-existing risk factors (6–9).
The main unexpected signals of disproportionate reporting are discussed below.
Cerebrovascular events
We found a significant association between triptan use and a range of serious cerebrovascular events such as ‘cerebral infarction’ (patients’ mean age 42.6 years; female/male ratio 3.3:1) and ‘ischaemic stroke’ (patients’ mean age 40.1 years; female/male ratio 1.8:1). The FDA prescribing information of Imitrex® (sumatriptan) currently states that ‘cerebrovascular events have been reported (…). The relationship of sumatriptan to these events is uncertain’ (5). Instead, this information is not mentioned in the relevant summary of product characteristics available in the United Kingdom (UK) (10), where the oral formulation of sumatriptan 50 mg can also be purchased without a prescription. Moreover, on the basis of post-marketing epidemiological studies, triptans are not considered to increase the risk of ischaemic stroke when adequately prescribed (2,23). For these reasons, we considered such associations unexpected. However, our findings may have been influenced by an indication and/or a protopathic bias. The association between migraine and stroke has yet to be clarified since (a) migraineurs are considered to have about a twofold risk of ischaemic stroke (24), (b) migraine per se is identified as one of the numerous aetiologies of ‘ischaemic stroke of unusual causes’ (25) and (c) the symptoms of cerebral ischaemia may resemble a migraine attack (26). Therefore, in the light of current knowledge, an accurate diagnosis of migraine, excluding all other possible mimicking conditions, remains crucial for the safe use of triptans as their vasoconstrictive effect on cerebral vessels (3,27) may act as a triggering factor for brain infarction (28). Appropriateness of use is one of the crucial aspects of the safety profile of triptans. The European Medicine Agency (EMA) recently refused the centralised authorisation for a low-dosage sumatriptan formulation as a non-prescription product (29) because of the ‘theoretical’ increased risk of cerebro- and cardiovascular events related to a misuse of these antimigraine agents.
Aneurysms and artery dissections
The second group of unexpected signals concerns aneurysms and artery dissections, which were highlighted at any level of specificity of the MedDRA classification tested. In particular, the specific combination triptan-carotid artery dissection (patients’ mean age 47.6 years; female/male ratio 3:1) was striking. To date there are no published case reports on this association. A case report of carotid artery dissection after ergotamine abuse hypothesised a causal relationship between the two (30). A possible role of triptan in triggering or precipitating such an event cannot be excluded in the light of the vasoconstrictive effect of triptans on the carotid arteries (10,27) and of the multifactorial aetiology of carotid artery dissection. Nevertheless, an indication and/or protopathic bias could also have influenced our results in this case (31,32).
Pregnancy-related vascular events
Our findings raised potential safety issues concerning maternal and foetal outcomes related to triptan use during pregnancy.
Concerning maternal vascular risk, an association between triptan use and ‘pregnancy-associated hypertension’, ‘pregnancy-induced hypertension’ and ‘placental infarction’ was found respectively. A possible pathophysiological role of 5HT1b/d receptors in pre-eclampsia had been already hypothesised by Gupta et al. (33), who also provided evidence of a progressive increase in contractile response to sumatriptan during the third trimester in isolated umbilical arteries from normotensive pregnant women. Therefore, on the basis of the triptan mechanism of action, such events could reasonably be included among the conditions to be monitored when a triptan is used during pregnancy. In any case, disorders such as pre-eclampsia and gestational hypertension, which are also related to placental infarction (34), seem to be more frequent in women with migraine (35,36).
The second interesting disproportional association in pregnancy concerns foetal outcomes: Three reports listing the event ‘congenital arterial malformations’ were found. Although this term refers to very non-specific outcomes in few reports, the issue probably merits further evaluation. To date, available studies on the safety of triptan use in pregnancy appear to be reassuring, but lack robust evidence (37,38). A preclinical study reported an increased incidence of cervicothoracic vascular malformation in rabbits exposed to triptans during organogenesis (10), making this association potentially plausible.
Strengths and limitations
The first strength of this study is the data source. The FDA_AERS database has already been widely used for post-marketing surveillance of drugs and biologics, showing its usefulness for the identification of serious and rare reactions that resulted in labelling changes and in some cases market withdrawals (14). Second, we applied the disproportionality approach to different MedDRA levels and to the appropriate SMQs, to increase the sensitivity of the analysis for possible detection of unexpected events (20). Third, the statistical adjustment of the ROR attempted to control the potential confounding factor represented by pre-existing risk, suggested by co-reported cardiovascular drugs. Although the proxy used could generate misclassification when some beta-blockers or calcium channel blockers are used for migraine attack prophylaxis, all triptan reports listing such drugs reported at least one additional cardiovascular drug as confirmation of underlying disease.
Different factors should also be considered potential sources of bias for the results obtained. Underreporting, selective reporting and residual duplicates represent intrinsic limits of the data analysed (18). Contraindications and precautions concerning cerebro- and cardiovascular events included in triptan package inserts and labels (5,10) may lead prescribers to over-report such events (notoriety bias). Moreover, since people with migraine are considered to be more at risk for different ischaemic events and other cardiovascular conditions (24,35,36), our analysis could have been affected by an indication bias. In addition, a protopathic bias could have also affected our results for those events easily mistaken for a migraine attack, (e.g. ischaemic cerebrovascular conditions and carotid artery dissection (26,32)).
Conclusions
Although triptans remain a safe antimigraine approach when appropriately used, this study highlights a number of reports of unexpected serious vascular events that may represent rare adverse reactions to triptan intake in ‘real’ clinical practice. Our results show a range of ischaemic cerebrovascular events, aneurysms and artery dissections, and pregnancy-related vascular events disproportionally reported after triptan use. Nevertheless, the associations discussed here should not be considered definite evidence of causality. A case-by-case analysis of the individual reports containing the unexpected events discussed above is necessary to confirm or disprove the plausibility of a causal relationship between drug and event, and to add useful evidence for further regulatory decisions on the most appropriate dispensing regimen of this drug class. Lastly, validated signals from spontaneous reports should represent hypotheses to be tested through large-scale analytical studies based on clinical databases, in order to obtain information on the estimated risk rate of the suspected adverse drug reaction in exposed and unexposed subjects.
Although our findings need to be confirmed, they raise concerns about triptan use in patients with risk factors for vascular disorders and during pregnancy. Furthermore, patients with atypical migraine possibly related to underlying vascular disorders or malformations should be investigated in depth before receiving a triptan.
Clinical implications
Appropriateness of use is one of the crucial aspects of the safety profile of triptans, as in rare instances their vasoconstrictive effect can cause severe vascular events. By analysing the United States Food and Drug Administration FDA Adverse Events Reporting System database, this study highlights a number of reports of serious and unexpected vascular events associated with triptan use (i.e. ischaemic cerebrovascular events, aneurysms and artery dissections, and pregnancy-related vascular events). Although our findings await confirmation, they raise concerns about triptan use in patients with risk factors for vascular disorders and during pregnancy. Furthermore, patients with atypical migraine disorders possibly related to underlying vascular conditions or malformation should be investigated in depth before receiving a triptan.
Footnotes
Funding
The study was supported by funds from the University of Bologna.
Conflict of interest
None declared.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.