
Abstract
Background
Hypnic headache (HH) is a rare primary headache disorder that is characterised by strictly sleep-related headache attacks.
Purpose
Because of the low prevalence of this headache disorder, disease information is mainly based on case reports and small case series. This review summarises current knowledge on HH in regard to clinical presentation, pathophysiology, symptomatic causes and therapeutic options.
Method
We review all reported HH cases since its first description in 1988 by Raskin. Broadened diagnostic criteria were applied for patient selection that slightly deviate from the current ICHD-II criteria. Patients were allowed to describe the headache character to be other than dull. Additionally, accompanying mild trigemino-autonomic symptoms were permitted.
Conclusions
Mainly elderly patients are affected, but younger patients and even children might also suffer from HH. Headache attacks usually last between 15 and 180 minutes, but some patients report headache attacks up to 10 hours. Almost all patients report motor activity during headache attacks. Cerebral MRI and 24-hour blood pressure monitoring should be performed in the diagnostic work-up of HH. Other primary headache disorders such as migraine and cluster headache may also present with sleep-related headache attacks and should be considered first. Caffeine taken as a cup of strong coffee seems to be the best acute and prophylactic treatment option.
Introduction
IHS classification (ICHD-II) of hypnic headache.

IHS: International Headache Society; ICHD: International Classification of Headache Disorders, second edition.
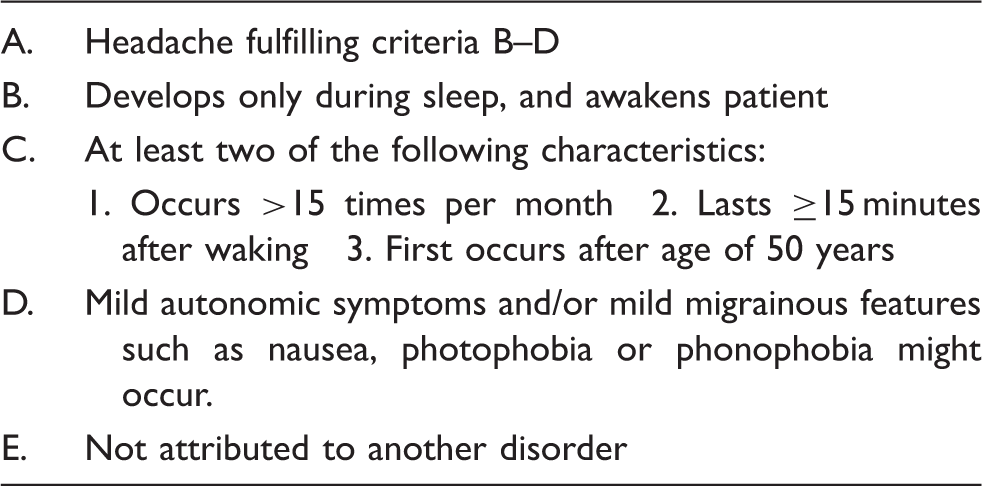
Broadened diagnostic criteria used in this review.
Epidemiology
Currently, only 225 adult patients with idiopathic HH have been described in the literature. In the headache clinic at Mayo Hospital, one out of 1400 patients suffered from HH (19). In a specialized Spanish headache clinic, one of 100 patients with strictly unilateral headache suffered from an HH (20). However, especially mild symptoms might be overlooked and increasing knowledge of this disease might also increase prevalence data. On average it takes about five years before the correct diagnosis of HH is made in affected patients. Single cases of patients with disease duration of more than 20 years before diagnosis have been reported (17).
In Raskin’s initial description of patients, a clear male predominance was reported (1). In contrast, following case reports and case series rather suggested that more women than men are affected by this disease (3,4). HH usually starts beyond the age of 50 (mean age 60.4 ± 10.4 years), but some cases in younger adults and even children were reported (12,21,22).
Clinical presentation
Clinical characteristics in adult hypnic headache.
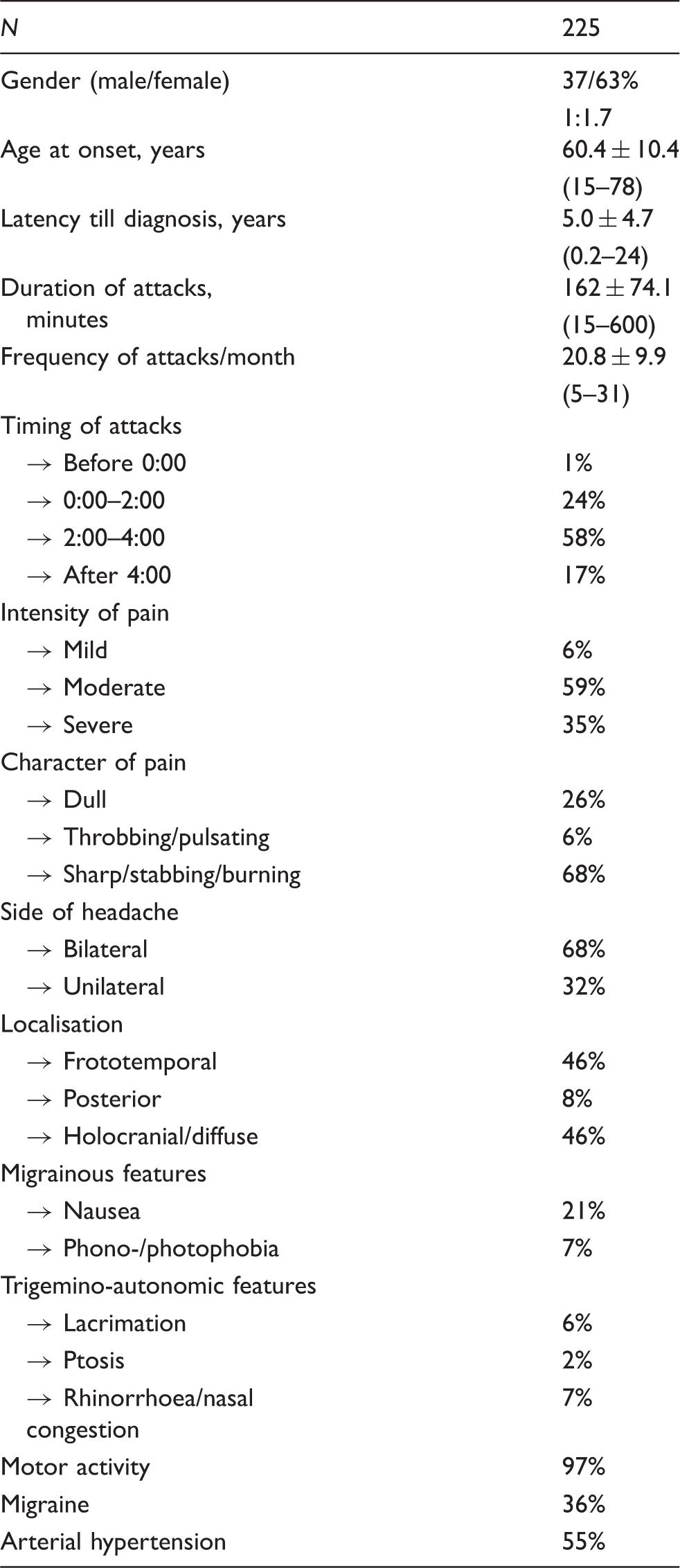
Current International Headache Society (IHS) classification postulates HH pain to be of dull character. However, there is increasing evidence that a large number of patients describe the pain to be rather throbbing, pulsating, sharp, stabbing or even burning in nature. Deviant pain character, therefore, should not lead to rejection of the diagnosis of HH if all other clinical features confirm HH. Initially, HH pain was thought to be rather of mild to moderate intensity, but current data confirm that more than a third of HH patients suffer severe headache attacks. The initially proposed diagnostic criteria in 1997 by Goadsby and Lipton (64) required a bilateral localisation of pain and short attack duration between five and 60 minutes. These criteria had to be broadened as more and more HH patients with unilateral pain localisation and longer pain attacks were reported. The current analysis shows that a third of patients also report unilateral HH attacks. Therefore, the obligation of bilateral headache presentation is not included in the newer diagnostic criteria of HH.
The duration of HH attacks has been intensively discussed in the literature, as more and more case reports were published that documented longer HH headache attacks, even up to 10 hours’ duration (23,24). Sometimes, patients have difficulties reporting the exact end of the headache attack, when a dull background pain persists after the genuine headache attack (15).
Most of the patients describe a frontotemporal or holocranial diffuse pain localisation. Accompanying migranous features are commonly seen in HH. One out of five patients reports nausea. However, these features are predominantly subtle; vomiting has been not been observed in HH. According to the current IHS classification, criteria of HH-associated trigeminal autonomic symptoms such as lacrimation, ptosis, rhinorrhoea and nasal congestion contradict the diagnosis of HH, but newer data suggest that at least light autonomic features might occur (3,15,17).
The natural course of disease remains unknown. Most studies and case reports did not investigate the course of disease. Liang et al. reported that most of their Taiwanese patients (52.9%; n = 9) showed an episodic clinical course with an attack period lasting seven to 365 days with sustained remission after treatment (18). In contrast, other patients showed an episodic relapsing remitting course of disease (18,25,26).
One study looked for clinical differences between female and male patients suffering from HH, analysing 24 patients (15 females) (9). No significant gender-related differences in clinical presentation were observed, but pain was rated to be more intense by male HH patients.
Pathophysiology
The underlying pathophysiology of HH is still enigmatic. The circadian rhythmicity of headache attacks is the most striking pathognomonic feature of HH and suggests possible hypothalamic involvement.
Voxel-based morphometry (VBM) can be used to analyse structural alterations between different groups. This method was used to compare brains of 14 HH patients with 14 age- and gender-matched healthy controls (27). Alongside the decrease of grey matter (GM) within areas of known cerebral pain processing areas (formerly called pain matrix) (e.g. cingulate cortex, frontal lobe, inferior temporal gyrus), which can often be detected in chronic pain disorders, significant GM decrease within the posterior hypothalamus of HH patients was detected. This observation was the first pathophysiological correlate of hypothalamic dysfunction in this condition. Interestingly, this anatomic hypothalamic area was also found to be altered in narcoleptic patients, underlying its association with sleep pathology (28).
Up to now only one study has been published addressing functional electrophysiological changes in HH. Trigeminal pain processing was investigated in 15 HH patients and 15 age- and gender-matched healthy controls using the nociceptive blink reflex and trigeminal pain-related-evoked potentials (29). No significant differences and no habituation deficit could be observed in the patient group compared with healthy controls.
Sleep and polysomnography
Polysomnographic (PSG) data on HH patients are sparse and mainly based on single-patient studies. Initial case reports seemed to clearly show a strict rapid eye movement (REM) sleep dependency of HH attacks (26,30–35). Newer data, however, contradict this hypothesis, showing a large part of HH attacks rising from nonrapid eye movement (NREM) sleep stages (18,36–39). A total of 58 HH attacks were recorded in 37 different patients and reported in the literature (7,18,26,30–40). Forty-seven per cent of HH attacks occurred during REM sleep, 53% occurred during NREM sleep stages, mainly during sleep stage 2 (38%) (Figure 1). An REM or NREM subtype cannot be differentiated, as REM- and NREM-associated headache attacks occur in the same patient and even during the same night (39).

Capuano et al. performed a macro- and microstructural analysis of sleep and actigraphy in a single HH patient over 12 consecutive nights who was successfully treated with amitriptyline (40). Before starting medication a quantitative reduction of REM sleep could be observed, which increased after starting amitriptyline. Additionally, the cyclic alternating pattern (CAP), which reflects disturbing factors and drug manipulation as well as subjective quality of sleep, was analysed (41,42). Contrary to expectations, the CAP rate increased after treatment. Therefore, the authors suggested that nocturnal hypoarousal might play an important role in the underlying pathophysiology in HH, which has already been suggested in migraine (43–45).
Obstructive sleep apnoea syndrome (OSAS) is commonly observed in HH patients, but PSG-recorded HH attacks do not temporally correlate with observed oxygen desaturation in most of the cases (18,30,31,37–39). Only one case report describes an HH patient who is affected by severe OSAS and improved significantly after treatment with nasal continuous positive airway pressure and supplemental oxygen (34). The observed high prevalence of OSAS in HH patients seems to be rather due to the elderly patient population than causally associated with HH. Therefore, OSAS has to be ruled out only in HH patients who show additional symptoms such as excessive daytime sleepiness, unrefreshing sleep, fatigue and unintentional sleep episodes during wakefulness.
Headache comorbidities
In many HH patients other primary headache disorders were reported. More than a third of patients report having suffered from migraine at some point in life. The relevance of this observation has not yet been clarified. Most of the elderly patients do not report actual migraine attacks in the period of time when the HH occurred. This might be due to the decrease of migraine attacks after menopause.
One patient suffered from an associated primary sexual headache (46). When treated with indomethacin, both headache entities disappeared.
Diagnostic approach and differential diagnosis in HH
The diagnosis of HH can be made only after excluding secondary causes (Figure 2). Therefore, cerebral neuroimaging is always warranted in HH as several symptomatic cases have been described in the literature. One patient with typical HH presentation had a haemangioblastoma of the cerebellum (47), the other ones had a nonfunctioning pituitary macroadenoma (48), a growth hormone-secreting pituitary tumour (49), a posterior fossa meningioma (50) or a brainstem lesion (51).
Diagnostic and therapeutic algorithm in hypnic headache patients.
Besides cerebral lesions, nocturnal arterial hypertension as another major medical condition should be ruled out by diagnostic work-up (Figure 2). Single-case reports showed that treatment of this condition can terminate HH attacks (16,52). Some authors concluded that HH in general might be caused by nocturnal arterial hypertension and cannot be considered a primary headache disorder (16). This hypothesis was supported by the high comorbidity rates of arterial hypertension in HH. However, arterial hypertension is treated well in most patients and treatment does not lead to attack termination in the vast majority of patients.
Additionally, drug-induced HH has been described in single-case reports. Transient HH symptoms were described after withdrawal of long-term lithium treatment (53). In contrast, HH attacks stopped after withdrawal of angiotensin-converting enzyme (ACE) inhibitor medication (54). HH might also occur because of medication overuse; however, literature in this regard is very limited (55).
Other primary headache disorders presenting with sleep-related headache attacks
HH can be diagnosed only when other primary headache disorders that may also present with sleep-related headache attacks are ruled out. The International Classification of Sleep Disorders classifies besides HH a few other primary headaches as so-called sleep-related headaches, which are cluster headache, chronic paroxysmal hemicrania and migraine (56). The circadian rhythmicity of cluster headache attacks occurring always at the same time has been reported often in the literature. Sleep-related headache attacks can often be observed in cluster headache (for review, see Barloese et al. (57)). Some studies even suggested cluster headache to be a REM sleep disorder, but previous studies showed that cluster headache attacks also occur during NREM sleep stages. Additionally, sleep-independent headache attacks also occur in most cluster headache patients, which helps to differentiate HH from cluster headache. Other clinical features for differentiation are distinct trigemino-autonomic features and headache-accompanied restlessness that can be observed only in cluster headache. Chronic paroxysmal hemicrania is another trigemino-autonomic cephalgia that might display sleep-related headache attacks. Despite ipsilateral trigemino-autonomic symptoms in regard to the headache side, duration of headache is usually shorter than in HH attacks (i.e. two to 30 minutes) (2). Headache frequencies above five per day are typically seen in chronic paroxysmal hemicrania. It is a common clinical observation that migraine attacks often occur during night sleep and upon awakening. Especially in older patients over the age of 60 years, up to two-thirds of headache attacks may develop during sleep (58).
If a patient has headache attacks fulfilling IHS criteria or probable IHS criteria for other primary headaches such as cluster headache, chronic paroxysmal hemicrania and migraine, these headache entities should be considered first before diagnosing a patient with HH, because these headache disorders are much more common than HH.
Therapeutic options
Treatment options in hypnic headache.

P: prophylactic medication; A: acute medication; d: day.
Prophylactic treatment options
Only three drugs have shown relevant efficacy in preventing HH attacks in a significant number of patients and should be considered as treatment options in HH: a) lithium carbonate, b) caffeine and c) indomethacin.
Lithium carbonate is the most often used prophylactic drug in HH (1,16–18,24,30,32,36,59–69). It has been shown to be effective in about two-thirds of patients. However, because of frequent side effects especially in this older patient population, therapy is often discontinued. Additionally, contraindications such as heart and kidney failure, psoriasis, cardiovascular disease, electrolyte disturbance and hypothyroidism have to be considered before starting therapy. Caffeine in terms of a cup of coffee seems to be effective as prophylactic treatment as well as acute medication of the individual attack (15,19,24,31,59,70–74). Patients are often afraid of sleep disturbances as side effects and do not try this treatment option. Case reports indicate that this only seldom occurs in this patient population. Indomethacin was evaluated in 22 documented patients and was effective in about 70% of them (6,15,16,19,24–26,33,36,67,70,72–78). Moreover, it was suggested that indomethacin shows distinct efficacy in patients with unilateral localisation of HH (70). However, side effects led to a large discontinuation rate. Topiramate was used in 12 patients as a prophylactic agent and was effective in eight of them (15,61,65). Other substances such as oxetorone (17) or sodium ferulate (100 or 50 mg, 3 times/day, two or three months) (7) showed good therapeutic responses but were tried in only a few patients (n = 8, n = 2, respectively). Melatonin, which was always suggested as a therapeutic option in HH, showed a rather poor response rate (15,70,74). Many other drugs were not effective or have shown only anecdotal effects such as β-blockers (19,30,34,61), verapamil (24,30,31,70), flunarizine (18,24,30,31,60,61,63,79,80), prednisone (19,24,34,59,65,81), benzodiazepines (30,34), gabapentin (24,36,74), antidepressants other than tricyclics (25,34,71,77), valproate (25,30,61) and azolamide (76).
One HH patient was successfully treated with botulinum toxin type A (71). In total 75 U BOTOX® was injected in the corrugator muscle, splenius capitis muscle, semispinalis muscle and trapezius muscle. In one patient occipital nerve stimulation was reported to be effective (10). The stimulator was started at 11:00 at night and was turned off in the morning. The headache frequency was decreased to one to three per month. Furthermore, headache intensity was decreased to 1–2/10. After lead disconnection, pain reoccurred, but ceased again after revision.
Acute treatment options
In addition to genuine caffeine intake in the form of a cup of coffee, efficacy of caffeine-containing analgesics was shown in some patients (15,19). However, daily intake of mixed analgesics should be avoided to prevent secondary side effects (e.g. medication-overuse headache, ulcers, etc.). Many other drugs were not effective or have shown only anecdotal effects such as triptans (19,24,25,30,31,61,70,71), nonsteroidal anti-inflammatory drugs (5,10,15,24,25,31,71,82), acetaminophen (15,21,30,61,62), oxygen inhalation (15,21,45,56,) metamizole (15), opioids (15), nimesulid (24,30,61,81) and ergotamine (62).
HH in children
HH starting at paediatric age is a very rare phenomenon. Only five cases have been reported in the literature so far (12,21,22). These five cases do not meet the current IHS criteria and therefore have to be considered as atypical presentations of HH. However, in other primary headache disorders such as migraine, it is a well-known observation that clinical presentation in childhood might be quite different from that in adulthood. In paediatric HH more girls than boys were affected (gender ratio male/female 1:1.5). The children were between 7 and 11 years old (mean age 9 ± 1.6 years) and attack duration was rather short compared to adult patients (mean duration 26.6 ± 11.3 minutes). Mean attack frequency was rather small (9.6 ± 8.6). One patient even had only one attack per month (21). Based on this low number of patients, typical clinical characteristics of paediatric HH are difficult to determine. However, one should have in mind that HH can also occur in younger patients.
Additionally, two adult patients were described who reported an onset of HH attacks at the age of 15 (13,25). Paediatric subtype might persist into adulthood at least in some patients.
Conclusion
This review on all currently reported HH cases in the available literature shows that although current IHS classification reflects a majority of HH patients, some clinical features may be overlooked. Motor behaviour during the HH attacks seems to be performed by almost all patients and might be helpful for making the right diagnosis. Additionally, some patients may show mild trigeminal autonomic symptoms, which should not exclude the diagnosis of HH. Cerebral magnetic resonance imaging (cMRI) and 24-hour blood pressure monitoring should be performed in the diagnostic work-up of HH. Secondary causes as well as other primary headache disorders should be ruled out before diagnosing HH. Especially, cluster headache and migraine often present with sleep-related headache attacks and have a much higher prevalence compared to HH. As controlled treatment trials are missing in HH, recommendations are based only on anecdotal case reports and uncontrolled trials in smaller case series. Caffeine taken as a cup of strong coffee seems to be the best acute and prophylactic treatment option. Alternatively, lithium carbonate and indomethacin can be used as prophylactic agents to reduce attack frequency. Although both drugs show good efficacy, high discontinuation rates were reported because of side effects. To improve treatment of HH in the future, randomised controlled trials are urgently needed. Additionally, studies on the pathophysiology of HH are warranted for a better understanding of the disease. Future studies should strictly include patients according to the new upcoming ICDH-III criteria to avoid distortion of the study data. However, further clinical observations have to demonstrate whether the new upcoming ICDH-III criteria sufficiently depict the HH population.
Clinical implications
Almost all patients display a distinct motor activity during hypnic headache (HH) attacks. Cerebral magnetic resonance imaging (cMRI) and 24-hour blood pressure should be performed to rule out symptomatic subtypes of HH. Other primary headache disorders such as migraine and cluster headache may also present with sleep-related headache attacks and should be considered first in nocturnal headache attacks. Rapid eye movement (REM) and nonrapid eye movement (NREM) sleep-associated headache attacks can be observed in HH patients, even in the same night. Treatment recommendations are based only on anecdotal case reports and uncontrolled trials in small case series. Caffeine taken as a cup of strong coffee seems to be the best acute and prophylactic treatment option in HH.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.