
Abstract
Background
Short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT) and short-lasting unilateral neuralgiform headache with cranial autonomic symptoms (SUNA) are primary headache syndromes. A growing body of literature has focused on brain magnetic resonance imaging (MRI) evidence of neurovascular compression in these syndromes.
Objective
The objective of this article is to assess whether SUNCT is a subset of SUNA or whether the two are separate syndromes and clarify the role of neurovascular compression.
Method
We describe three new SUNCT cases with MRI findings of neurovascular compression and critically review published SUNCT/SUNA cases.
Results
We identified 222 published SUNCT/SUNA cases. Our three patients with neurovascular compression added to the 34 cases previously described (16.9%). SUNCT and SUNA share the same clinical features and therapeutic options. At present, there is no available abortive treatment for attacks. Lamotrigine was effective in 64% of patients; topiramate and gabapentin in about one-third of cases. Of the 34 cases with neurovascular compression, seven responded to drug therapies, 16 patients underwent microvascular decompression of the trigeminal nerve (MVD) with effectiveness in 75%.
Conclusions
We suggest that SUNCT and SUNA should be considered clinical phenotypes of the same syndrome. Brain MRI should always be performed with a dedicated view to exclude neurovascular compression. The high percentage of remission after MVD supports the pathogenetic role of neurovascular compression.
Introduction
Short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT) is a primary headache syndrome characterized by unilateral stabbing or throbbing orbital or temporal pain. There should be at least 20 attacks, lasting 5–240 seconds, and both ipsilateral conjunctival injection and lacrimation (1). Only one of those symptoms or other cranial autonomic signs, along with a longer duration of attacks (two seconds–10 minutes), characterize short-lasting unilateral neuralgiform headache with cranial autonomic symptoms (SUNA), which is currently classified in the Appendix of the International Classification of Headache Disorders, 2nd edition (ICHD-II) (1). It is not clear whether SUNCT is a subset of SUNA or whether the two are separate entities (1–3). In addition, the growing magnetic resonance imaging (MRI) evidence of neurovascular compression in SUNCT/SUNA cases, commonly detected in the classic trigeminal neuralgia, raises the question of whether it is an incidental finding or a symptomatic cause (2,3). We describe three new SUNCT cases with brain MRI finding of neurovascular compression and critically review published literature on SUNCT/SUNA cases, including therapeutic options.
Methods
We describe three new SUNCT patients with brain MRI finding of neurovascular compression attending our headache center between February 2009 and November 2011. We electronically searched PubMed using the following keywords: trigeminal, autonomic, neuralgia, SUNCT, SUNA, lacrimation, tearing, rhinorrhea, nasal congestion, ptosis, miosis, mydriasis, eyelid edema, facial flushing, sweating, neurovascular compression and microvascular decompression (MVD). We screened the English-language literature to identify SUNCT and SUNA cases, including those with neurovascular compression. We carefully reviewed the reference lists of all the papers found. A few abstracts were included. Secondary SUNCT/SUNA cases were excluded to have a homogeneous group for comparison. However, we were not able to exclude three secondary cases reported in the largest SUNCT/SUNA series (one SUNA patient with multiple sclerosis and two SUNCT patients with pituitary lesions) because they were not reported separately.
Only cases with both conjunctival injection and tearing were classified as SUNCT, according to ICHD-II criteria. We focused on the following clinical items: trigeminal involvement and neurovascular compression, gender, age at onset, laterality of pain, cranial autonomic symptoms, triggers, refractory period, therapeutic options and surgical treatment. Statistical analysis was performed using chi square for categorical data, and unpaired two-tailed t test for continuous variables. A p value < 0.05 was considered significant.
Results
Case 1 (4)
A 55-year-old man with familial thrombocytopenia complained of headache attacks since the age of 46 years. The headache was characterized by severe shock-like burning pain occurring over the right orbital and temporal areas, accompanied by ipsilateral conjunctival injection, ptosis, lacrimation and rhinorrhea. The attacks occurred spontaneously or could be triggered by shaving, chewing or touching the right side of the face. A refractory period after tactile allodynic elicitations was absent. During the attacks the patient was restless and irritable. At onset, he had clusters of attacks with stabs lasting 30–60 seconds that would occur for several minutes (up to 40 minutes), from one to six times a day, mainly during daytime, for nearly a month once a year. Physical and neurological examinations were normal. He was administered gabapentin (600 mg daily) and was rendered asymptomatic. In the last year before our examination the attacks had worsened in frequency, occurring daily and nightly about 15 per hour becoming shorter in duration (seconds). Therapy with pregabalin 300 mg/day and verapamil 240 mg/day proved ineffective. Intravenous corticosteroids (methylprednisolone 500 mg/day) were then administered for three days without efficacy, thus they were discontinued together with the other preventive agents, and indomethacin up to 150 mg/day and carbamazepine (CBZ) up to 1000 mg/day were started. After two days the attacks had dramatically decreased in frequency. Indomethacin was stopped after one month when a complete remission was achieved and maintained with CBZ only. Repeated attempts to stop CBZ led to a recurrence of attacks. A brain MRI performed at the onset of symptoms was interpreted as normal. A second MRI was repeated after the worsening of headache and documented an aberrant loop of the right superior cerebellar artery compressing the ipsilateral trigeminal nerve (Figure 1). The good response to pharmacological treatment and the presence of thrombocytopenia contraindicated surgical MVD.
FSPGR MPR coronal reconstructed image (a) revealed the trigeminal nerve in its cisternal tract, bilaterally (arrows); 3D-TOF MR angiography sequence MPR coronal reconstruction (b) showed the contact between left superior cerebellar artery and the upper surface of the nerve (arrowhead).
Case 2
A 53-year-old woman with a medical history of hypertension and glaucoma presented with a three-year history of headache. She described strictly right-sided episodes of severe electric shock-like pain, occurring on periorbital and temporal areas, accompanied by prominent ipsilateral lacrimation, conjunctival injection, rhinorrhea, miosis and facial flushing. The attacks occurred spontaneously or could be triggered by touching the face, talking, chewing and moving the eyes. The pain usually lasted from two seconds to three minutes, occurring daily and nightly more than 100 times daily, for nearly a month once a year. Brain MRI performed at the onset of symptoms demonstrated hypo-density of the left caudate nucleus, compatible with a lacunar area. Therapy with oxygen, opioid analgesics, anticonvulsants (lamotrigine and valproic acid), and nonsteroidal analgesics, including indomethacin, proved ineffective. The patient came to our attention in February 2011 because of worsening headache. Neurologic examination displayed anisocoria, allodynia and hyperesthesia over the right trigeminal distributions during the attacks. The right corneal reflex could trigger the attacks. A refractory period was absent. A diagnosis of SUNCT was made. A second MRI scan documented right superior cerebellar artery compression on the ipsilateral trigeminal nerve (Figure 2). The patient was administered CBZ (600 mg/day), pregabalin (450 mg/day) and indomethacin (150 mg/day) that maintained her asymptomatic for three months. Following a head trauma in September 2011 the symptoms recurred. The patient was again administered CBZ (600 mg/day), pregabalin (450 mg/day) and indomethacin (150 mg/day) with partial improvement. In March 2012, she finally underwent MVD of the trigeminal nerve, which determined a complete disappearance of symptoms during the following 11 months of observation, without any prophylactic therapy.
FISP MPR coronal reconstructed image (a) revealed the trigeminal nerve in its cisternal tract, bilaterally (arrows); 3D-TOF MR angiography sequence MPR coronal reconstruction (b) and MIP reconstruction (c) showed the contact between right superior cerebellar artery and the upper surface of the nerve (arrowhead).
Case 3
A 47-year-old man with an unremarkable medical history complained of headache attacks since the age of 44 years. At onset, the attacks were characterized by severe shock-like pain occurring on the right orbital area, ear and nose, accompanied by ipsilateral conjunctival injection, ptosis and lacrimation. Usually the headache lasted from 30 to 60 seconds and occurred > 20 times a day. The patient was pain free at nighttime unless he got up. The attacks occurred spontaneously or could be triggered by moving the head, washing or touching the right side of the face, chewing, or wind hitting the face. Initially, the patient was misdiagnosed as having right chronic sinusitis on the basis of sinus computed tomography (CT) scan evidence. Sinusotomy using balloon catheter devices was attempted but after surgery he experienced worsening headache. Brain MRI documented a neurovascular compression. The patient underwent first gamma knife treatment without any improvement and one year later surgery for MVD. During the procedure, the compression of the right superior cerebellar artery and right peritrigeminal vein on the ipsilateral trigeminal nerve was identified and a Teflon sponge was interposed to maintain the separation. After four weeks the attacks returned with the same features previously described, but the patient was now experiencing a continuous burning pain involving all three branches of the right trigeminal nerve. A trial with CBZ (up to 600 mg daily) offered little benefit and was poorly tolerated. Gamma knife and sinusotomy were performed again without any improvement. Therefore, in November 2011, the patient came to our attention and the neurological examination showed only dysesthesia within the right V1-V2-V3 trigeminal areas. Repeat brain MRI with gadolinium documented greater thickness and contrast enhancement of the right trigeminal nerve, compatible with inflammation. The cerebrospinal fluid demonstrated a normal opening pressure (200 mmH20) and no oligoclonal bands, excluding central nervous system (CNS) inflammation. Intravenous corticosteroids were started without lasting benefit. Treatment with indomethacin (150 mg daily) was ineffective. Lamotrigine (up to 450 mg daily), amitriptyline (50 mg daily) and palmitoylethanolamide (600 mg daily) seemed to reduce the lacrimation, but not the frequency or intensity of attacks. Verapamil (240 mg daily) was added without improvement. Oxcarbamazepine (1200 mg daily) plus lamotrigine provided benefit proximally by 50% on both anesthesia dolorosa and SUNCT attacks.
Literature review
We found 222 cases in the literature. Of these, 189 had SUNCT attacks, 31 SUNA (2,3,5–15), two both SUNCT and SUNA (3,5).
Trigeminal involvement and neurovascular compression
Neurovascular compression in SUNCT and SUNA patients.
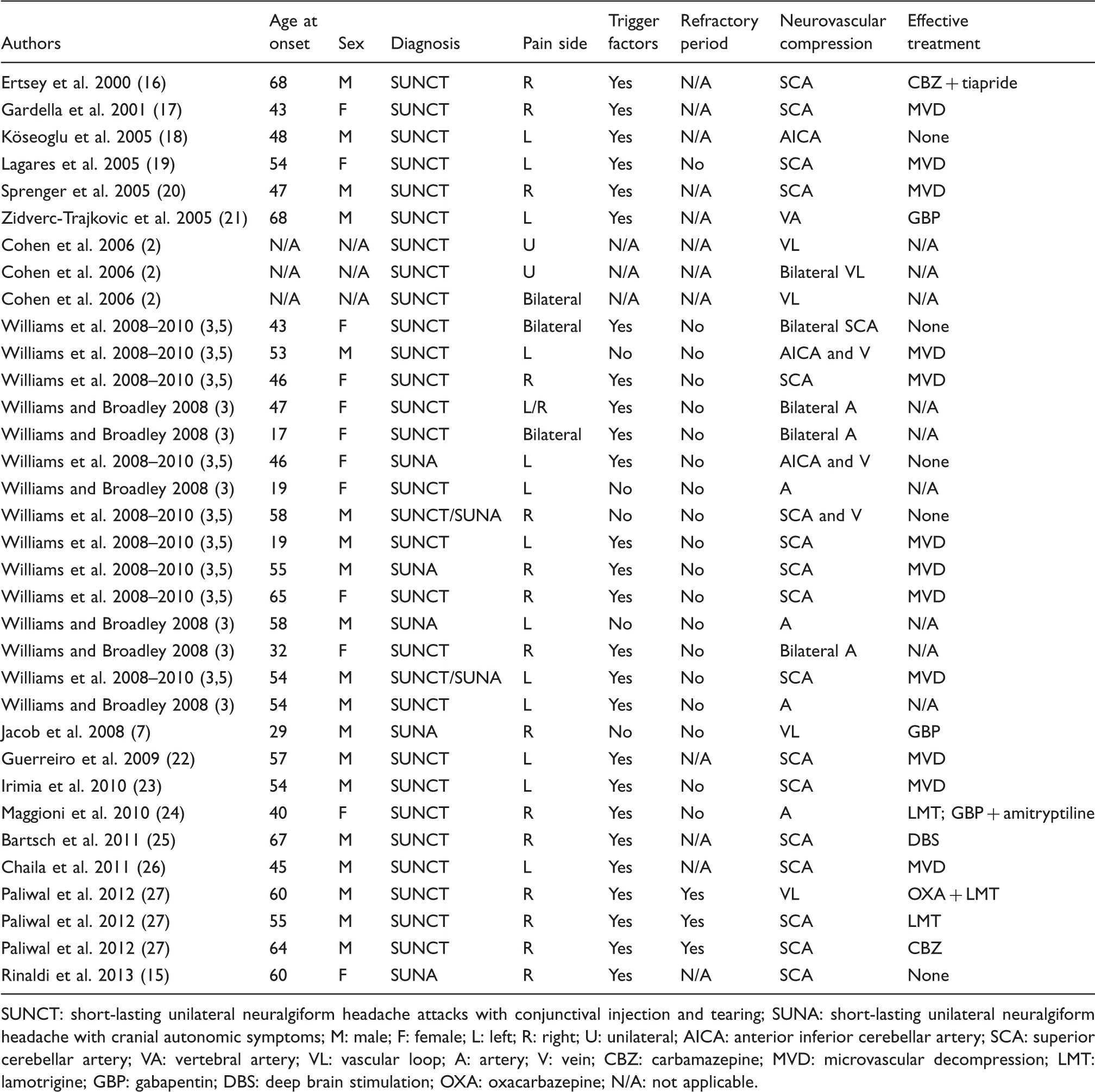
SUNCT: short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing; SUNA: short-lasting unilateral neuralgiform headache with cranial autonomic symptoms; M: male; F: female; L: left; R: right; U: unilateral; AICA: anterior inferior cerebellar artery; SCA: superior cerebellar artery; VA: vertebral artery; VL: vascular loop; A: artery; V: vein; CBZ: carbamazepine; MVD: microvascular decompression; LMT: lamotrigine; GBP: gabapentin; DBS: deep brain stimulation; OXA: oxacarbazepine; N/A: not applicable.
Gender and age at onset
Considering all patients together, information on sex and age at onset were available in 215 (96.8%) and 200 (90.1%) cases, respectively. A total of 109 SUNCT patients were male and 74 female (M:F ratio of 1.5 : 1). Eleven SUNA cases were male and 19 female (M:F ratio of 1 : 1.7). The two cases with both SUNCT and SUNA attacks were male patients, aged 54 and 58 years, respectively (3,5). The mean age at onset was 47.62 ± 17.11 years considering all patients together: 48.30 ± 17.33 years in SUNCT patients and 42.29 ± 15.64 years in SUNA syndrome, with no significant difference (p = 0.131).
Among SUNCT/SUNA patients with MRI evidence of neurovascular compression, 19 were male and 12 female (M:F ratio of 1.6 : 1). Age ranges at onset were available in 31 cases. The mean age at onset was 49.19 ± 14.01 years.
Cranial autonomic symptoms
Autonomic features.

SUNCT: short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing; SUNA: short-lasting unilateral neuralgiform headache with cranial autonomic symptoms; pts: patients.
Laterality of pain
The side of attacks was available in 205 (92.3 %) of 222 patients. Ninety-two (44.8%) had left-sided attacks, 90 (43.9%) right-sided attacks, seven (3.4%) unilateral attacks, but the side was not available; 12 (5.9%) patients had side-shift attacks, four (2%) bilateral attacks.
Among SUNCT/SUNA patients with MRI evidence of a neurovascular compression, 13 (38.2%) patients had left-sided attacks, 15 (44.1%) had right-sided attacks, two (5.9%) had unilateral attacks, but the side was not available; one patient (2.9%) had side-shift attacks and three (8.8%) had bilateral attacks (Table 1).
Triggers
Data on triggers factors were reported in 176 (79.3%) of 222 patients. Triggers such as touching the face, washing, shaving, eating, chewing, brushing teeth, talking, coughing or neck movement were identified in 128 (72.7%) of 176 patients. Conversely, 48 (27.3%) patients had exclusively spontaneous attacks. Of the 34 SUNCT/SUNA patients with neurovascular compression, 26 (76.5%) had triggers, five (14.7%) had only spontaneous attacks and in three cases data were not available (2).
Refractory period
Data on a refractory period were available in 93 (41.9%) of 222 SUNCT/SUNA cases. No refractory period was reported in 84 (90.3%) cases. Nine (9.7%) patients had a preserved refractory period (2,27–30). Three of them had MRI evidence of neurovascular compression (27).
SUNCT/SUNA: Therapeutic options
Lamotrigine alone (up to 400 mg) was effective in 52 of 81 patients (64.2%) (3,10,12,27,31–42), gabapentine (up to 3600 mg) in 24 of 71 (33.8%) (7,31,43–47), topiramate (up to 400 mg) in 14 of 43 (32.6%) (32,48,49), CBZ (200–1200 mg) in 25 of 119 (21%) (3,7,12,27,31,50–53), oxcamazepine in one of seven (14.3%) (54), corticosteroids in seven of 22 (31.8%) (30,40,46,55,56), verapamil in one of 18 (5.5%) (57), zonisamide in one of two (58), and lomerazide hydrochloride in one of two patients (9).
Drug therapies effective in SUNCT/SUNA cases.

SUNCT: short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing; SUNA: short-lasting unilateral neuralgiform headache with cranial autonomic symptoms; pts: patients.
Surgical treatment
MVD
Sixteen of 34 (47.1%) patients with MRI findings of a neurovascular compression underwent MVD of the trigeminal nerve. Twelve were SUNCT patients, two SUNA and two had both SUNCT and SUNA attacks (5,17,19,20,22,23,26). Complete pain relief was achieved in 12 of the 16 patients (75%) lasting up to 32 months after surgery. In addition, three more SUNCT patients with normal MRI studies were unsuccessfully treated with MVD (61,62). Two of them had been previously treated with a trigeminal ablative procedure (61). Data about MRI findings preceding MVD were not available in two SUNCT patients. One of them was asymptomatic for two years following surgery, then the pain recurred (52). The second one experienced a complete resolution of symptoms after three months of follow-up (63) (Table 1).
Local blockades
Blockade of the greater occipital nerve (GON) was performed in 25 patients. Seven SUNCT patients (28%) achieved a good response: five cases with lidocaine and depomedrone (31), one with bupivacaine (64), and another one with an association of triamcinolone, dexamethasone and lidocaine (65). Partial improvement within 72 hours had been reported in another patient treated with a single GON injection of steroids and local anesthetic (40). Three SUNA patients experienced improvement by approximately 50% lasting from two to seven weeks after GON injections (10). Conversely, the treatment was ineffective in 11 patients with SUNCT (10,25,31,37,66,67).
A response to sphenopalatine ganglion and intraorbital phenol blockades was reported in one SUNCT patient, with a benefit up to 12 months (13). Another SUNCT patient experienced headache resolution during the 16-month follow-up period following local opioid blockade of the superior cervical ganglion (68). However, local blockades of the supraorbital nerve (11 patients), infraorbital nerve (eight patients) and orbicularis oculi muscles (two patients) were performed without benefits. Blockades of the lacrimal nerve, gasserian ganglion (13), stellate ganglion, and the retrobulbar region were reported as ineffective in single cases (13,67,69). One patient received local lidocaine injections around the periorbital region with no improvement (65). Recently onabotulinumtoxin A was reported to reduce pain intensity and frequency in a single SUNCT case (70).
No local blockades had been used in any of the SUNCT/SUNA patients with MRI findings of a neurovascular compression.
Glycerol rhizotomy, gamma knife radiosurgery and percutaneous balloon compression
Three of the four patients (three SUNCT and one SUNA) who underwent glycerol rhizotomy achieved complete pain relief lasting from seven months to four years. Two of them were successfully treated twice (13). Conversely, another SUNCT patient underwent glycerol rhizotomy with only two weeks of pain reduction (61). Two SUNCT patients underwent gamma knife targeting both the trigeminal nerve and the sphenopalatine ganglion. The first had complete pain resolution at 39 months follow-up, without medication (71); the second experienced only rare provoked attacks at four months’ follow-up (72). Another two SUNCT patients underwent gamma knife radiosurgery targeting only the trigeminal nerve. The first had near complete pain relief for about two months, then the pain gradually recurred and he suffered from anesthesia dolorosa; the second had no improvement (61).
Two SUNCT patients showed an apparent benefit following radiofrequency thermocoagulation of the trigeminal nerve that lasted for two and three years, respectively (37,62). Another three SUNCT patients were pain free after percutaneous balloon compression of the gasserian ganglion with benefits ranging from 16 months to ten years of follow-up (13,28,73).
No SUNCT/SUNA patients with MRI findings of a neurovascular compression underwent destructive trigeminal nerve procedures.
Neurostimulation
One drug-resistant SUNCT patient with MRI evidence of neurovascular compression underwent successful hypothalamic deep brain stimulation (DBS), although the preoperative oral medication was not suspended because of an increased frequency of attacks on drug reduction. The patient had previously undergone MVD without benefit (25). Another two patients with intractable SUNCT underwent successful DBS (66,74). The first patient experienced an 80% reduction in daily attack frequency without prophylactic therapy after 12 months of stimulation (66). The second achieved a complete response, but lamotrigine treatment was added to eliminate sporadic attacks (74).
Seven refractory patients (six SUNCT, one SUNA) underwent bilateral occipital nerve stimulation (ONS): At a median follow-up of two years four of them achieved an excellent improvement, one moderate, one transient and one no benefit (11).
Discussion
We describe three new SUNCT patients with brain MRI evidence of vascular compression of the trigeminal nerve. These cases of SUNCT raise questions about the role played by neurovascular compression in SUNCT/SUNA manifestations and the best therapeutic approach to these patients.
The first patient we describe achieved a complete remission of symptoms with CBZ, which is the treatment of choice in trigeminal neuralgia (TN). The efficacy of CBZ has already been described in the treatment of SUNCT, including a case with MRI findings of neurovascular compression (27).
It is also likely that the second patient we report is a case of SUNCT secondary to trigeminal neurovascular contact, as suggested by the complete response to MVD and the ineffectiveness of medical treatment.
The third case we describe had a more atypical and complicated clinical course. The patient was initially misdiagnosed as having chronic sinusitis. No medical treatment was tried before he underwent unsuccessful gamma knife, MVD, and a second gamma-knife treatment. Following the MVD the patient started experiencing continuous burning pain involving all three branches of the trigeminal nerve, and exacerbation of SUNCT attacks. The MRI showed greater thickness and contrast enhancement of the right trigeminal nerve that may be compatible with a gamma-knife side effect. We observed only a partial response to an association of oxcamazepine and lamotrigine, and failure of other drugs. The clinical course of this patient is in line with other authors’ hypothesis that a previous trigeminal ablative procedure may explain the ineffectiveness of MVD in some SUNCT patients as occurs in TN (23). In addition, our case suggests that surgery should be attempted only after pharmacological treatment failure.
Clinical features and neurovascular compression
We reviewed the available literature to establish whether SUNCT and SUNA are different entities and to clarify the pathogenetic role played by the vascular loop closest to the trigeminal nerve. Since the last SUNCT syndrome review of medical literature (75), the number of published cases had rapidly increased in parallel with the rising recognition of a neurovascular compression associated with the syndrome, detected in 16.9% of SUNCT/SUNA patients. Taking all patients together, our results confirm a mild male preponderance in SUNCT syndrome, female in SUNA syndrome, and the presence of trigger factors (2,3,75). Conversely, age at onset was not significantly different between SUNCT and SUNA patients. Globally, we observed no side prevalence. Bilateral and side-shift attacks are also reported (2,3,48,76). According to the ICHD-II, all SUNCT patients have both conjunctival injection and lacrimation. In one-third of SUNA cases there is conjunctival injection or alternatively lacrimation. The presence of other autonomic features in SUNA is similar to SUNCT cases. Interestingly, mild autonomic symptoms are also reported in TN series and seem to correlate with a worse prognosis after MVD (77,78), raising the question of whether they should be considered SUNCT/SUNA cases rather than TN with autonomic features. A diagnostic clinical sign able to distinguish SUNCT/SUNA from TN is the absence of a refractory period. However, as in TN, a refractory period is described in a few SUNCT syndrome cases, including three with neurovascular compression (2,27,29,30). Unfortunately many of the previous features may be underreported. Similarly, many subjects were not investigated systematically with dedicated trigeminal views on MRI. The largest previous series reported a vessel closest to the trigeminal nerve in 7% and 88% of patients (2,3). The relevance of neurovascular compression to the pathophysiology of SUNCT/SUNA is unclear. However, the involvement of the trigeminal autonomic reflex in these syndromes is widely acknowledged (79). A vascular compression of the trigeminal nerve has been implicated as a peripheral afferent stimulation to this reflex. The persistent stimulation could lead to central disinhibition of the trigeminal autonomic reflex by hypothalamic activation (5,15). Functional MRI studies have demonstrated ipsilateral, controlateral and bilateral hypothalamic activation in SUNCT and SUNA syndromes (20,31,80). Interestingly, bilateral hypothalamic activation was reported in a SUNCT case with MRI finding of neurovascular compression who underwent successful MDV (20). The high percentage (75%) of SUNCT/SUNA cases who remitted after MVD supported the pathogenetic role of trigeminal neurovascular compression. Conversely, doubts about this assumption are related to the description of one case with unilateral compression of the trigeminal nerve with bilateral pain and two patients with bilateral loops but with unilateral attacks (2,3). It could be argued that these findings are coincidental and not relevant to pain production. In this context, a simple contact between a vessel and the nerve may not cause true nerve compression.
Treatment
Among all cases reviewed, lamotrigine should be considered the treatment of choice, with efficacy reported in 64% of patients when administered alone. Topiramate and gabapentin may be prescribed as an effective preventive medication in one-third of patients treated. SUNCT and SUNA patients have also been reported to respond to CBZ (21%). A variety of other drugs, alone or in combination, have been tried in SUNCT/SUNA syndrome, none with reliable effectiveness. Among acute treatments, triptans, analgesics and opioids have not been consistently effective in SUNCT/SUNA treatment. In particular, indomethacin has been generally found ineffective. Interestingly, intravenous or subcutaneous lidocaine seems highly effective for short-term prevention (2,3). The dramatic improvement in SUNCT and SUNA in response to lidocaine has led some authors to propose this pharmacological test as a diagnostic clinical tool to confirm the diagnosis (60). However, there are no randomized controlled trials because of the rarity of the syndrome.
Trigeminal surgery should be considered only in selected medically intractable patients, in whom MVD should be considered the treatment of choice with an efficacy reported in 75% of subjects with neurovascular compression. On the contrary, limited evidence supports benefits after greater occipital nerve procedures, glycerol rhizotomy, gamma-knife radiosurgery, radiofrequency thermocoagulation, or percutaneous balloon compression. To date, few patients with drug-resistant SUNCT were successfully treated with DBS or ONS, one of them with MRI findings of neurovascular compression, and further reports are needed.
Limits
Our review has some limits. Although every effort was made to include all patients in the literature presenting with SUNCT and SUNA attacks, some reported cases may have been missed, or duplicated, especially in the case of publications from the same research center. Few secondary headaches were included. In addition, much clinical information was reported differently or lacking so it was difficult to make comparisons, particularly on treatment efficacy.
Conclusions
Our three new SUNCT patients with MRI findings of neurovascular compression have been added to the 34 SUNCT/SUNA cases described in the literature. We suggest that brain MRI with a dedicated view of the trigeminal nerve should always be performed to exclude neurovascular compression in SUNCT/SUNA patients. In agreement with Cohen and colleagues (2), we suggest that SUNCT and SUNA should be considered clinical phenotypes of the same spectrum of presentation in the new revision of the international classification for several reasons. First, we confirm these headache syndromes share the same clinical characteristics, except for lacrimation and conjunctival injection. Second, both SUNCT and SUNA attacks are present in the same patients. Third, neurovascular compression is detected in both conditions. Finally, the syndromes respond to the same drug therapies, with lamotrigine as the first-line treatment. For acute treatment, lidocaine should be considered in selected cases. Surgical approaches should be attempted in refractory cases. In particular, as for TN, MVD may represent a treatment option in patients with MRI evidence of neurovascular compression.
Clinical implications
Short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT) and short-lasting unilateral neuralgiform headache with cranial autonomic symptoms (SUNA) should be considered clinical phenotypes of the same syndrome. Brain magnetic resonance imaging (MRI) should always be performed with a dedicated view to exclude neurovascular compression. The high percentage of remittance after microvascular decompression (MVD) supports a pathogenetic role of the neurovascular compression.
Footnotes
Acknowledgments
The authors thank Dr Francesco Toni (Neuroradiology Department, Bellaria Hospital, IRCCS Istituto delle Scienze Neurologiche di Bologna) for reviewing the patients’ MR images with us, and Anne Collins for English editing.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.