
Abstract
Background
While cross-sectional studies have shown associations between migraine and depression, few studies have been able to evaluate the association between migraine and incident depression.
Methods
A prospective cohort study among 36,016 women without a history of depression enrolled in the Women's Health Study who provided information about migraine and headache at baseline. Women were classified as either having nonmigraine headache, migraine with aura, migraine without aura, past history of migraine or no history of headache. Cox proportional hazards models were used to evaluate the association between migraine and headache status and incident depression.
Results
At baseline, 5115 women reported a history of nonmigraine headache, 1805 reported migraine with aura, 2723 reported migraine without aura, and 1896 reported a past history of migraine. During 13.8 mean years of follow-up, 3833 new cases of depression occurred. The adjusted relative risks of incident depression were 1.44 (95% CI: 1.32, 1.56) for nonmigraine headache, 1.53 (95% CI: 1.35, 1.74) for migraine with aura, 1.40 (95% CI: 1.25, 1.56) for migraine without aura, and 1.56 (95% CI: 1.37, 1.77) for past history of migraine compared to no history of headache.
Conclusions
Middle-aged women with migraine or nonmigraine headache are at increased risk of incident depression. Frequent migraine attacks (weekly or daily) were associated with the highest risk for developing depression.
Keywords
Introduction
Migraine and depression are common disorders in the general population and are associated with substantial disability burden (1,2). Studying the association between migraine and depression among women is particularly important because the prevalence of each disorder is more common among women than men (3,4). Several cross-sectional studies have suggested that migraine and depression may be comorbid disorders (5). Since some studies have found evidence of a bidirectional association between migraine and depression (6–9), longitudinal studies are necessary to quantify the risk of incident depression among those with migraine. Additionally, information on whether migraine with aura may exhibit stronger relationships with depression than migraine without aura is limited. One study found that the risk of depression is higher among those who experience migraine with aura compared to those who experience migraine without aura (8).
Based on the hypothesis that migraine may increase the risk of depression through the intense and often long-lasting pain episodes, some studies have also examined whether the presence of nonmigraine headache is associated with an increased risk of depression commensurate with the increase seen in migraine. A cross-sectional and a case-control study found an association between migraine as well as nonmigraine headache and depression compared to no headache, although the association was stronger for migraine than for nonmigraine headache (10,11). However, a prospective study found that severe headache did not result in a significant increase in the risk of developing depression (7).
To further elucidate the associations between migraine, including aura status, as well as nonmigraine headache, and incident depression, we aimed to study these associations in the Women’s Health Study (WHS), an ongoing prospective cohort study.
Methods
The WHS was a large, randomized, placebo-controlled trial designed to test the effects of aspirin and vitamin E on the primary prevention of cardiovascular disease and cancer. The design and main results of the trial have been described previously (12–14). Briefly, at baseline 39,876 United States (US) female health professionals aged 45 years or older were randomized to receive active aspirin, active vitamin E, both active agents, or both placebos according to a two-by-two factorial design. At baseline women were asked about various health and lifestyle characteristics, including information about migraine. Six months after baseline and yearly thereafter, women were again asked about various health conditions and events. Since the end of the trial in 2004, the women continued to be followed on an observational basis.
The WHS was approved by the institutional review board at Brigham and Women’s Hospital and informed consent was obtained from all participants.
Migraine and headache assessment
At baseline the women were asked, “Have you ever had migraine headaches?” and “In the past year, have you had migraine headaches?” Women who experienced migraine headaches within the past year were asked for further details, including, “What is the approximate frequency of your migraines?” with possible response options of daily, weekly, monthly, every other month, and less than six times per year and “Do your migraines have any of the following characteristics? (Mark all that apply.)” The response options included “Aura or any other indication a migraine is coming,” which was used to classify women who experience migraine with aura. Since the baseline questionnaire did not ask about nonmigraine headache, we used information from the six-month questionnaire to assess headache. On the six-month questionnaire, women were asked if they had had any headache since the baseline questionnaire. Using the women’s responses to these questions, we divided them into the following groups: any history of migraine (women who reported ever experiencing migraine headache), history of nonmigraine headache (women who reported experiencing headache but did not report a history of migraine headaches), and no history of headache (women who reported no history of migraine headache or nonmigraine headache). Women with any history of migraine were further divided into the following categories: “migraine with aura” (women who reported migraine within the past year and who reported the presence of aura or any indication that migraine is coming); “migraine without aura”; and “past history of migraine” (women who reported ever having migraines but not within the past year). A previous study in the WHS has shown good agreement between self-reported migraine and classification of migraine without aura based on the second International Classification of Headache Disorders (15) criteria.
Depression assessment
Women were asked if they had ever been diagnosed with depression on the 48-month and 108-month questionnaire. Women who responded affirmatively were asked to provide the month and year of diagnosis. On the 120-month and first observational follow-up questionnaire, women were asked to report newly diagnosed depression within the past year and to include the month and year of diagnosis. Incident diagnosed depression and year of incident diagnosed depression were based on the earliest reported diagnosis date from these four questionnaires. Although depression diagnosis was self-reported, previous research has shown that health professionals report lifestyle characteristics and medical conditions accurately (16–18).
Given the limitations to using self-reported physician diagnoses of depression, we performed sensitivity analyses using three related outcome measures. First, on the 60-month questionnaire, the women were asked questions from the Mental Health Inventory (MHI-5), a five-item subscale of the Short-Form 36 health status survey (19) that measures global psychological distress. The five items ask the participants how much of the time over the past month (all, most, a good bit, some, little or none) they felt nervous, felt so down that nothing could cheer them up, felt calm and peaceful, felt down and blue or felt happy. We categorized the MHI-5 into four groups: 86–100, 76–85, 53–75, and <53 and designated scores <53 as evidence of significant psychological distress, similar to previous studies (20–22). Our second outcome measure was self-reported antidepressant medication use among those reporting depression at the 108-month questionnaire.
Analysis
Of the 39,876 women enrolled in the WHS, we excluded 119 women missing information on migraine status at baseline, 872 women who never provided information on depression status, and 2869 women who reported a history of depression prior to the six-month questionnaire, leaving 36,016 women for this analysis. Using Cox proportional hazards models, we calculated the hazard ratio and 95% confidence intervals (CI) as a measure of the relative risk (RR) of incident depression for women with any history of migraine or a history of nonmigraine headache compared to those without a history of headache. Women contributed person-time from the return date of the sixth-month questionnaire until date of incident depression, death, loss to follow-up or end of study whichever occurred first. We tested the assumption of proportional hazards by including an interaction term between the log transformation of time and headache category and found no significant violation.
We further stratified the group of women reporting any history of migraine into migraine with aura, migraine without aura, and past history of migraine. Additionally, we examined the association between migraine attack frequency and risk of incident depression.
We built age-adjusted and two multivariable-adjusted models. In our first multivariable analysis, we adjusted for the following potential confounders: age (continuous in years), body mass index (BMI; continuous in kg/m2), systolic blood pressure (10 mmHg increments), diastolic blood pressure (<65, 65–74, 75–84, 85–89, 90–94, 95–104, ≥105 mmHg), history of hypertension (yes/no), use of antihypertensive medication (yes/no), menopausal status (premenopausal, postmenopausal, uncertain), ever used oral contraceptives ≥two months (yes/no/not sure), alcohol use (rarely/never, one to three drinks per month, one to six drinks per week, ≥one drink per day), vigorous physical activity (rarely/never, <one time per week, one to three times per week, ≥four times per week), baseline history of diabetes (yes/no), smoking (never, past, smoke <15 cigarettes per day, smoke ≥15 cigarettes per day), postmenopausal hormone use (never/past/current), history of high cholesterol (yes/no), and treatment for high cholesterol (yes/no). We also adjusted for randomized treatment assignments. In our second multivariable-adjusted analysis, we additionally adjusted it for income ($10,000 increments), education (RN, LPN/LVN, Other, MD/MD equivalent, DDS/DMD, DVM) and marital status (single, married, divorced, widowed).
For our sensitivity analyses, we performed logistic regressions adjusting for all covariates listed above in our first multivariable-adjusted model. For the MHI-5 outcome, we excluded women who did not answer all five questions on the MHI-5 (n = 3990). For the antidepressant medication-use outcome, we excluded women who did not return the 108-month questionnaire (n = 8281).
For all models, more than 100 women were missing information on systolic and diastolic blood pressure, income, education, and marital status and were assigned to a separate category. Fewer than 100 women were missing information on all other covariates and were either assigned to the mean value (BMI), the reference category (i.e. lowest exposure category), to the past user category (smoking) or to the unclear exposure category (menopausal status and oral contraceptive use). The highest percentage of missing data was seen for diastolic blood pressure (1.4% of women were missing data on this covariate).
All statistical analyses were performed with the use of SAS 9.1.3. All p values are two tailed and p < 0.05 was considered statistically significant.
Results
Baseline characteristics of women according to headache status in the Women’s Health Study (n = 36,016).

y: years; BMI: body mass index; numbers may not add up to 100% because of rounding or missing data.
Age- and multivariable-adjusted relative risk of depression according to headache status (n = 36,016).
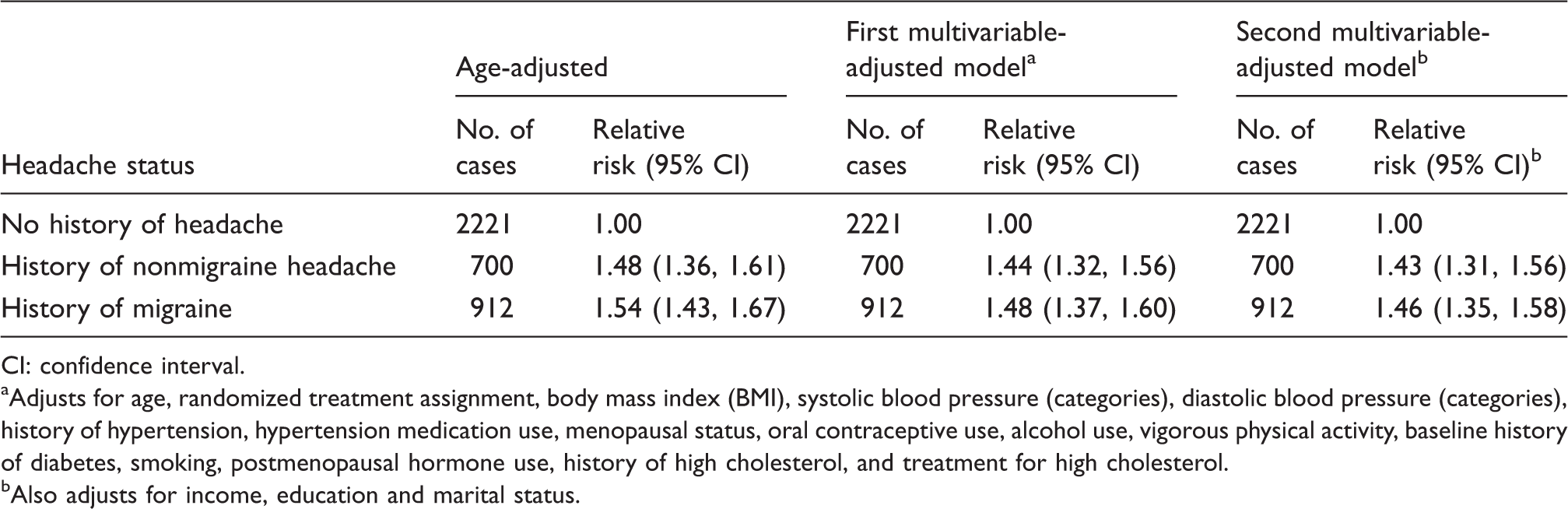
CI: confidence interval. aAdjusts for age, randomized treatment assignment, body mass index (BMI), systolic blood pressure (categories), diastolic blood pressure (categories), history of hypertension, hypertension medication use, menopausal status, oral contraceptive use, alcohol use, vigorous physical activity, baseline history of diabetes, smoking, postmenopausal hormone use, history of high cholesterol, and treatment for high cholesterol. bAlso adjusts for income, education and marital status.
Age- and multivariable-adjusted relative risk of depression according to headache status (n = 36,016).
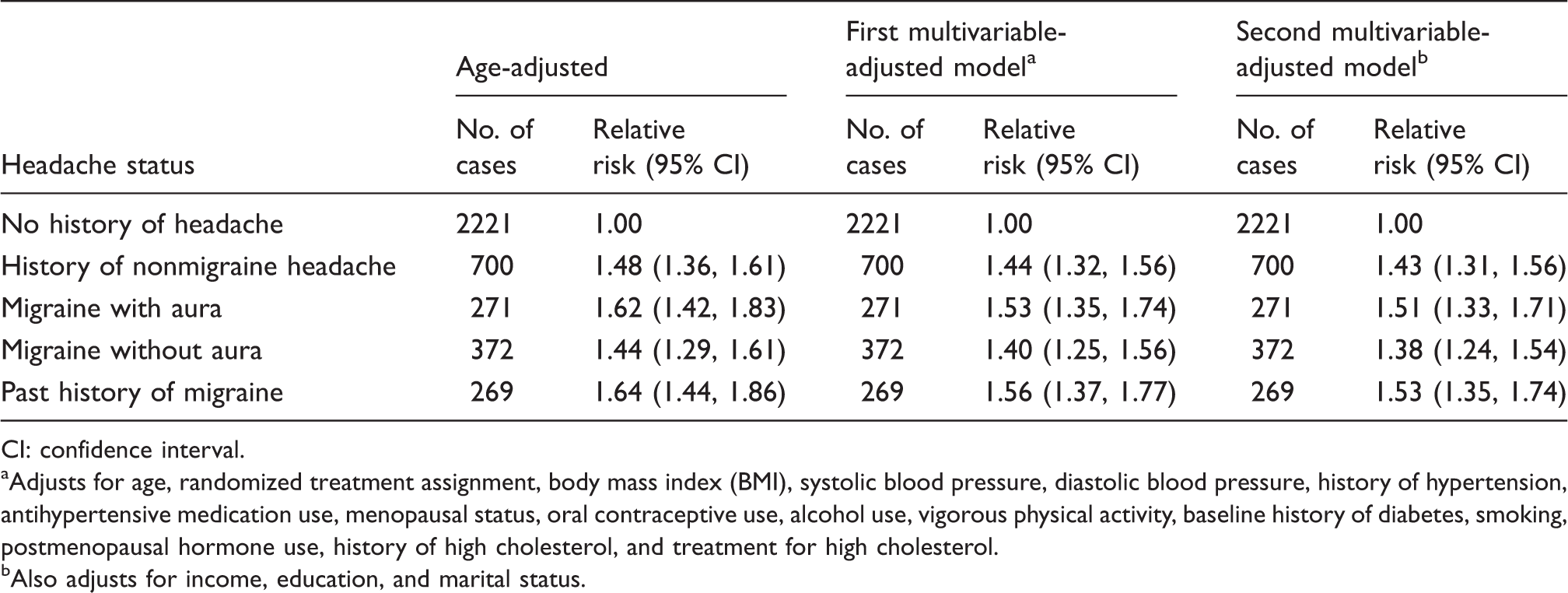
CI: confidence interval. aAdjusts for age, randomized treatment assignment, body mass index (BMI), systolic blood pressure, diastolic blood pressure, history of hypertension, antihypertensive medication use, menopausal status, oral contraceptive use, alcohol use, vigorous physical activity, baseline history of diabetes, smoking, postmenopausal hormone use, history of high cholesterol, and treatment for high cholesterol. bAlso adjusts for income, education, and marital status.
Age- and multivariable-adjusted relative risk of incident depression according to migraine attack frequency (n = 28,949).
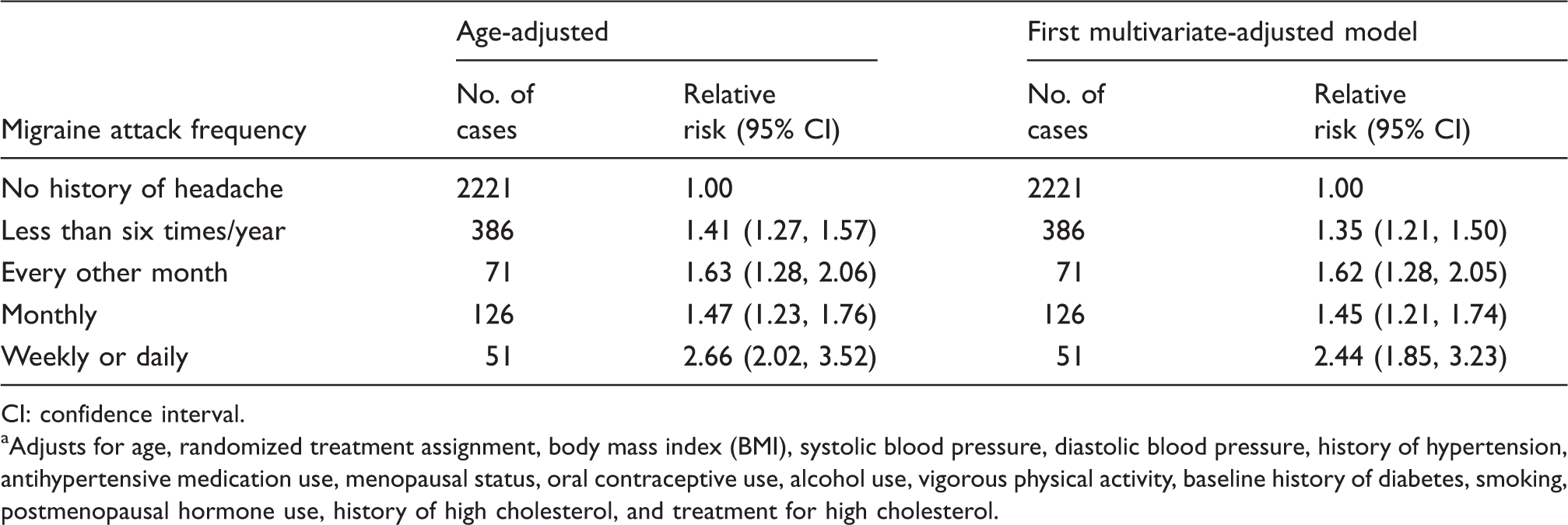
CI: confidence interval. aAdjusts for age, randomized treatment assignment, body mass index (BMI), systolic blood pressure, diastolic blood pressure, history of hypertension, antihypertensive medication use, menopausal status, oral contraceptive use, alcohol use, vigorous physical activity, baseline history of diabetes, smoking, postmenopausal hormone use, history of high cholesterol, and treatment for high cholesterol.
Multivariable-adjusted relative risk of psychological distress as measured by the MHI-5 according to headache status (n = 32,026).

MHI: Mental Health Inventory; CI: confidence interval. aAdjusts for age, randomized treatment assignment, body mass index (BMI), systolic blood pressure, diastolic blood pressure, history of hypertension, antihypertensive medication use, menopausal status, oral contraceptive use, alcohol use, vigorous physical activity, baseline history of diabetes, smoking, postmenopausal hormone use, history of high cholesterol, and treatment for high cholesterol.
Multivariable-adjusted relative risk of significant psychological distress (MHI-5 < 53) and antidepressant medication use according to headache status.

MHI: Mental Health Inventory; CI: confidence interval. aAdjusts for age, randomized treatment assignment, body mass index (BMI), systolic blood pressure, diastolic blood pressure, history of hypertension, antihypertensive medication use, menopausal status, oral contraceptive use, alcohol use, vigorous physical activity, baseline history of diabetes, smoking, postmenopausal hormone use, history of high cholesterol, and treatment for high cholesterol.
Discussion
Results from this large, prospective study among middle-aged women showed that migraine, regardless of migraine subtype, and nonmigraine headache were associated with an increased risk of incident depression compared to individuals with no history of headache. Frequent migraine attacks (weekly or daily) were associated with the highest risk for developing depression.
Few studies have been able to specifically address the direction of the relationship between migraine and depression. Some studies have suggested that migraine and depression may have a bi-directional association (6–9). One study found evidence of a bi-directional association between migraine and depression but was unable to stratify the results by aura status and did not examine the association between nonmigraine headache and depression (6). Another study using data from the Detroit Area Study of Headache followed people with migraine within the past year, people with other severe headache within the last year, and a subset of the remaining sample without migraine or severe headache in their lifetime for the occurrence of migraine, severe headache or depression. The study found that major depression at baseline was associated with the onset of migraine during follow-up (odds ratio (OR) = 3.4, 95% CI: 1.4, 8.7) and that migraine was associated with the onset of depression during follow-up (OR = 5.8, 95% CI: 2.7, 12.3) (7). Given the insignificant associations seen between headache and depression in these analyses, the authors concluded that the association between migraine and depression is most likely due to shared etiologic factors, possibly related to the hormonal or neurotransmitter systems. However, the authors acknowledged that an association between severe headache and depression could not be conclusively ruled out.
Data from the Canadian National Population Health Survey also suggested a bi-directional association between migraine and depression. Those with migraine were 60% more likely to develop major depressive episodes compared to those without migraine while those with a history of major depressive episodes were 40% more likely to develop migraine compared to those without major depressive episodes (9).
While some studies have shown evidence of a bi-directional association between migraine and depression, data from the Baltimore Epidemiologic Catchment Area Follow-up Study did not find evidence of an association between depression and incident migraine (23). However, this study did not examine the association between migraine and incident depression.
While our study confirmed a longitudinal association between migraine and depression, we also found an association between nonmigraine headache and depression. The larger size (36,016 women vs. 1186 women) and the longer follow-up (13.8 years vs. two years) in our study compared to the previous longitudinal study (7) may have resulted in an increased ability to detect a significant association between nonmigraine headache and incident depression.
Most previous studies on migraine and depression could not stratify their results by migraine aura status. The Detroit Area Study of Headache observed an increase in the risk of incident depression for both migraine with aura (RR = 4.90; 95% CI: 3.34, 7.19) and migraine without aura (RR = 3.03; 95% CI: 2.23, 4.11) (8). We also found a slightly higher risk of depression among women who experience migraine with aura than among women who experience migraine without aura, although our effect estimates were lower than those observed in the Detroit Area Study of Headache. There are a few possible explanations for the difference in effect sizes. First, the age ranges of the two cohorts were different. The previous study enrolled people aged 20–55 while our study included only women who were 45 years of age or older. The risk for incident depression among migraineurs may be higher among young adults than middle-aged adults. Additionally, by relying on self-report of physician diagnosis of depression instead of using a structured interview, we may not have captured all cases of depression within our cohort. If this underreporting was nondifferential with respect to our exposure status, we would expect our results to be biased toward the null, which might help to explain why our effect estimates were lower than those seen in the previous study.
Another study followed 379 subjects aged 19 to 20 at first interview for 10 years. Using the Structured Psychopathological Interview and Rating of the Social Consequences for Epidemiology (SPIKE), they found that major depression and recurrent brief depression were more common among the migraine with aura group than among those with migraine without aura, tension-type headache, headache symptoms only or no-headache groups (24).
Three different mechanisms have been proposed to explain why migraine is associated with depression in cross-sectional studies (25). First, psychiatric disorders, like depression, may cause migraine. Second, migraine may cause psychiatric disorders like depression possibly because of the repeated episodes of intense and long-lasting pain associated with migraine or some other migraine-specific mechanism. Finally, migraine and depression may share etiologic factors or common causes.
Our findings that nonmigraine headache in addition to migraine increases the risk for depression favors the concept that the pain aspect of migraine or some pain-related mechanism increases the susceptibility for depression. Two not mutually exclusive scenarios may be envisioned. First, repeated headache attacks (and chronic headache) are debilitating, may obviate social activities, and thus impair quality of life to such an extent that depression develops. Second, headache and depression may share common neuroanatomical circuits, neurotransmitters, and/or genetic susceptibility factors. This agrees with findings from other pain conditions and depression (26–28). If one or both conditions develop as well as when and in which order they manifest may depend on additional factors. Given the increased risk of depression observed among those with migraine or headache, physicians should monitor these patients for the development of depressive symptoms.
The strengths of this study include its prospective, longitudinal design, which allowed us to assess the temporal association between migraine or nonmigraine headache and depression. The large size of the cohort and information on aura status also allowed us to stratify our results based on migraine subtype.
Despite these strengths, there are a few important limitations to this study. First, migraine status and incident depression are self-reported, and misclassification of migraine or depression status is possible. However, previous research has shown that health professionals, similar to those enrolled in our cohort, report lifestyle characteristics and medical conditions accurately (16–18). Additionally, we observed good agreement between self-reported migraine and the classification of migraine without aura according to International Headache Society (IHS) criteria. While some misclassification of migraine status is still possible, this misclassification is more likely nondifferential with respect to our outcome because information on incident depression was collected prospectively. Our sensitivity analysis used related outcomes (the MHI-5, which measures psychological distress, and self-reported antidepressant medication use) and found similar results to our primary analysis. We did not use self-reported antidepressant medication use as our primary outcome because frequent migraine can be treated with antidepressant medication. Other limitations include not having information on the aura status of women who report a prior history of migraine and only crude information on migraine attack frequency. Our study enrolls only middle-aged women, which may impact the generalizability of our findings to other populations. Finally, while we attempted to control for confounding, the potential for unmeasured and residual confounding remains.
Migraine and nonmigraine headache are associated with an increased risk of incident depression in middle-aged women. By incorporating information on the onset of migraine and depression relative to each other and also examining the impact of other pain disorders on the risk of depression, future studies can help to determine if the associations seen between migraine and depression may be causal or due to common etiologic factors.
Clinical implications
Migraine and nonmigraine headache are associated with an increased risk of incident depression in middle-aged women. Given the increased risk of depression observed among those with migraine or headache, physicians should monitor these patients for the development of depressive symptoms.
Footnotes
Funding
The WHS is supported by the National Heart, Lung, and Blood Institute (grants HL-043851, HL-080467, HL-099355) and the National Cancer Institute (grant CA-047988). Dr Rist was funded by a training grant from the National Institute of Aging (AG-00158).
Conflicts of interest
None declared, but the authors report all financial disclosures for the past three years. Dr Rist has received funding from a training grant from the National Institute of Aging (AG-00158), from the Rose Traveling Fellowship Program in Chronic Disease Epidemiology and Biostatistics from the Harvard School of Public Health, and from a travel fund from the Department of Epidemiology at the Harvard School of Public Health. Dr Schürks has received an investigator-initiated research grant from the Migraine Research Foundation and honoraria from LEK Consulting for telephone surveys and from the American Academy of Neurology for educational material. Since August 2011 he is a full-time employee of Bayer HealthCare Germany. Dr Buring has received investigator-initiated research funding and support as principal investigator from the US National Institutes of Health and research support for pills and/or packaging from Bayer Heath Care and the Natural Source Vitamin E Association. Dr Kurth has received investigator-initiated research funding from the French National Research Agency, the US National Institutes of Health, Merck, the Migraine Research Foundation, and the Parkinson’s Disease Foundation. Further, he has received honoraria from Allergan, the American Academy of Neurology, and Merck for educational lectures, from the BMJ for editorial work, and from MAP Pharmaceuticals for participating in a scientific advisory panel.