
Abstract
The aim of the investigation was to study the impact of headache on quality of life (QOL) in adolescents in a population-based sample (N = 1047, aged between 13 and 17 years). QOL was assessed using the KINDL-R (Revidierter Kinder Lebensqualitätsfragebogen) questionnaire with its six dimensions. In order to assess potential differences in the impact on QOL according to the type of headache, a stratified analysis was performed. QOL differences compared to the ‘no headache’ group are presented with adjustment for socio-demographic confounders. Headache at least once per month was reported in 48% of the adolescents and accounted for a small but significant reduction of 2.5 points in the total KINDL-R score, which was mainly caused by a reduction in physical wellbeing by 6.8 points. Adolescents with migraine reported higher reductions in physical wellbeing and total QOL than subjects with tension-type headache (TTH). The size of the reduction in QOL scores was small but similar to that observed for other chronic conditions in adolescents. Headache prevention programs might therefore have an impact on QOL in adolescents.
Introduction
Headaches are among the most important health problems worldwide (1) in terms of both economic and non-economic impact on sufferers (2). Epidemiological studies in adults demonstrate that headache, especially migraine, is associated with reduced (QOL) (3–9). In contrast, only a few studies have investigated the general impact of headache on QOL in adolescents, particularly with regard to different types of headache, although it is known that approximately 10% of adolescents suffer from migraine and 15%–20% suffer from TTH (10–13). Some studies (14)–(19) reported a reduced QOL related to headache. However, most of the studies focused on adolescents with migraine only (14),(17)–(19), while others yielded inconsistent results with respect to school-related QOL (14),(16),(18),(19). To our knowledge there is only one recent (hospital-based) study which systematically addresses the impact of different types of headache on QOL in a small study group of adolescents, yielding no differences in QOL dimensions depending on the type of headache (20).
We, therefore, performed a population-based study using the KINDL-R questionnaire to assess QOL in adolescents with different types of primary headache. The self-administered KINDL-R questionnaire is a German-language tool designed to study health-related QOL in children and adolescents by evaluating the following dimensions: physical wellbeing, emotional wellbeing, self-esteem, family-, friend- and school-related QOL (21,22). In addition to dimension-specific scores, a total QOL score can be calculated.
The aim of our study was to compare differences in total QOL score as well as dimension-specific differences in QOL between adolescents with migraine and/or TTH and adolescents without headache, with adjustment for socio-demographic confounders. The following questions were addressed: (1) How greatly is QOL reduced in adolescents with headache, and which dimensions are affected? (2) Does the impact of headache on QOL vary depending on the type of headache?
Methods
The present study was a spin-off of the MobilEe project, an epidemiologic investigation of possible acute health effects of electromagnetic fields from mobile phone networks, conducted in four cities in Bavaria, Germany (23). A population-based sample of adolescents was interviewed about a broad spectrum of health conditions, including answering a screening question on prevalent headache during the last 6 months. Adolescents who indicated at least one episode of headache per month during the last 6 months were invited to fill in an additional questionnaire for a more detailed investigation of headache.
Participants
Within the MobilEe project, 6386 children and adolescents, randomly drawn from population registries in the four cities, were contacted to participate (see Figure 1); 516 could not be approached and 2848 refused to participate (23). Of the 3022 participants with completed interviews, 1498 were children younger than 13 years and, therefore, not eligible for the present study on headache in adolescents; 1524 were aged between 13 and 17 years. For 388 of the adolescents, inclusion in the headache study was not possible, because they had been recruited prior to the conception of the headache study, leaving 1136 adolescents for our study. Of these, 547 reported no headache episodes during the last six months, while 589 subjects reported headache and were, therefore, invited to complete the headache questionnaires. Of these, 508 completed the questionnaire, but 8 had to be excluded because of inconclusive information. This leaves a final study population of 1047 subjects: 500 with valid headache questionnaires (‘any headache’ group) and the above-mentioned 547 subjects without any headache (‘no headache’ group) (shaded parts in Figure 1).
Flow diagram of subject participation. Subjects included in the headache study are marked as shaded. † Excluded for logistical reasons: In Munich, recruitment had been started before the concept of the headache study had been finalized.
Data assessment
Written informed consent was obtained from the participants’ parents and—if they were older than 14 years—from the adolescents themselves as well. Computer-assisted personal interviews were performed in public buildings and took between 15 and 25 minutes to complete. Thereafter, participants reporting at least one headache episode per month during the last six months were asked to complete the headache questionnaire in the waiting room or at home.
The interview included questions on socio-demographic status, health behaviour and QOL; questions on socio-demographic status (age, sex, family status, siblings, school type, parents’ employment status) were taken from the German Health Interview and Examination Survey for Children and Adolescents (24). Age was dichotomized into the two age groups ‘14 years and younger’ and ‘15 years and older’. Family status was considered as ‘complete’ if the subject indicated that he or she was living together with both parents; otherwise, it was considered as ‘incomplete’. School type was considered as ‘grammar school’ if the subject indicated that he or she attended a ‘Gymnasium’; otherwise, as ‘no grammar school’. Parents’ employment status was considered as ‘full-time’ if so indicated; otherwise, as ‘not full-time’.
The KINDL-R, a recently developed German tool designed to study health-related QOL in adolescents, was used to measure QOL in the following dimensions: physical wellbeing, emotional wellbeing, self-esteem, family-, friend- and school-related QOL (21,22). Each of these six dimensions consists of four items that are each rated on a 5-point Likert scale. Mean scores for each dimension and a total KINDL-R score are calculated and then linearly transformed to values between 0 and 100, with higher values corresponding to better/higher QOL. The instrument has been psychometrically tested with good reliability (Cronbach alpha 0.63–0.76 for the different dimensions; 0.84 for the total KINDL-R score) and convergent and discriminant validity (21,22).
Sixty-four subjects who had already finished school did not answer items on school-related QOL. One additional subject did not answer enough items concerning friend-related QOL, so that there was not sufficient information to calculate this dimension score. For these 65 subjects, no total KINDL-R score could be calculated either.
Headache questionnaire
The headache-screening question in the interview (‘How often did you experience headache within the last six months?’) was taken from the Health Behaviour in School-aged Children symptom checklist (25). Subjects who indicated that they suffered from headache at least once per month answered a detailed questionnaire on the type of headache, based on the German translation of the second edition of the International Headache Society (IHS) classification (26).
The classification of any type of migraine included the subtypes migraine (with or without aura) and probable migraine according to the strict criteria for adults. Furthermore, probable migraine was classified according to a modified criterion for children with a shorter duration of headache (i.e., attacks lasting between 30 minutes and 72 hours). This criterion was chosen for the sake of comparability with another German study on adolescent headache (13), although it does not quite match the conventional IHS criterion for children, which requires attack duration of at least one hour and up to 72 hours (26). The classification of TTH included the following subtypes: infrequent episodic TTH, frequent episodic TTH, chronic TTH, probable infrequent episodic TTH, probable frequent episodic TTH and probable chronic TTH. A classification of combined ‘migraine plus TTH’ could arise in subjects fulfilling the criteria for both probable migraine and probable TTH, which require compliance with all but one of the respective criteria for migraine or TTH. All other subjects with a headache that did not match any of these classifications for primary headache were considered to have miscellaneous headache (MH).
Statistical analyses
Associations between categorical variables were tested using Chi-square statistics. For continuous variables, means and standard deviations were reported. Multiple linear regression models for any headache (with ‘no headache’ vs. ‘any headache’), migraine (with ‘no headache’ vs. ‘pure migraine’), TTH (with ‘no headache’ vs. ‘pure TTH’), migraine plus TTH (with ‘no headache’ vs. ‘any migraine + any TTH’) and MH (with ‘no headache’ vs. ‘MH’) were used to quantify the difference in the KINDL-R scores between adolescents with and without headache, with adjustment for age group, sex and family status as potential confounding co-variables. p values <. 05 were considered to indicate a significant difference. The statistical analyses were performed with the SAS software package (version 9.1, SAS Institute, Cary, NC, USA).
Results
Prevalence of different types of headache
Six-month prevalence of migraine, tension-type headache and miscellaneous headache

aTension-type headache; bMiscellaneous headache.
Distribution of selected socio-demographic characteristics in subjects with and without headache

Significant p values of Chi-square tests:
a p < .05; b p < .01; c p < .001.
Headache and QOL
Mean scores and standard deviations of the KINDL-R dimensions for no headache, any headache and type of headache

aTension-type headache; bMiscellaneous headache.
Prediction of each KINDL-R dimension score and the total KINDL-R score for any headache (N = 475) compared to no headache (N = 501) and confounding co-variables: results of the multiple linear regression analysis
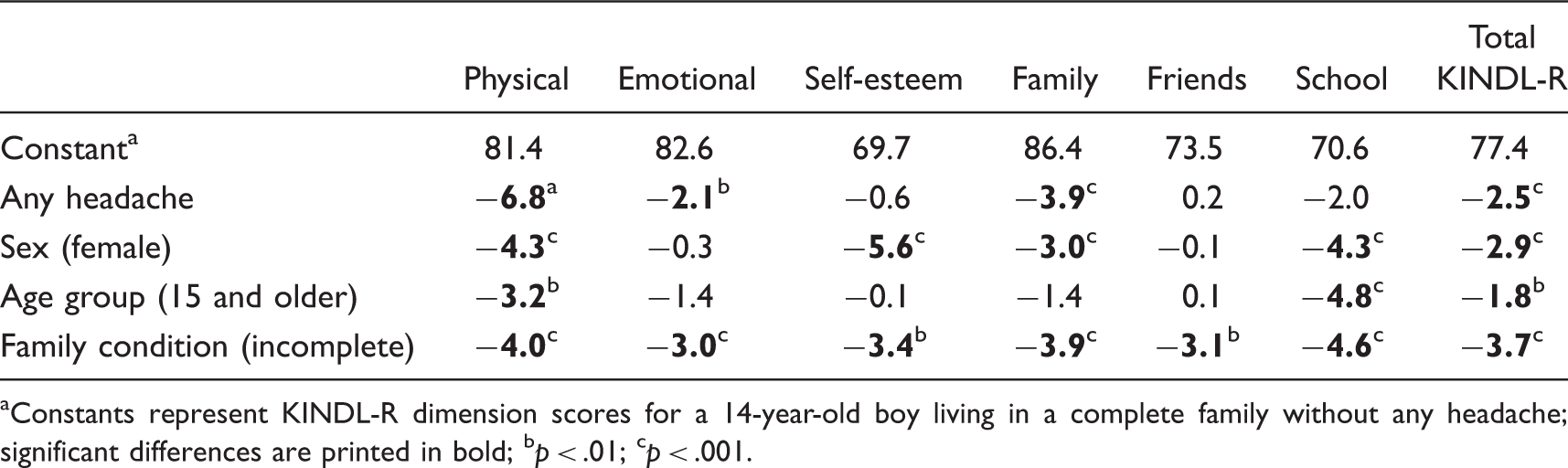
aConstants represent KINDL-R dimension scores for a 14-year-old boy living in a complete family without any headache; significant differences are printed in bold; b p < .01; c p < .001.
Headache-type specific quality of life
Prediction of each KINDL-R dimension score and the total KINDL-R score for type of headache compared to no headache: results of the multiple linear regression analyses a

aConstants and effect estimates for confounders are not shown in this table to allow for better reading; bsignificant differences are printed in bold; b p > .05; c p > .01; d p > .001.
Discussion
The aim of the present investigation was to study the impact of headache on QOL in a population-based sample of adolescents. Prevalent headache was associated with lower overall QOL scores. Physical and emotional wellbeing as well as family- and school-related QOL were the contributing dimensions to the lower overall QOL in adolescents with headache. The strength of the effect, however, appeared small, accounting for a reduction of the total KINDL-R score by 2.5 points and a reduction in the physical wellbeing score by 6.8 points. Subjects suffering from migraine and migraine plus TTH appeared to be most affected in terms of total reduction of QOL scores, whereas subjects suffering from MH and TTH reported more dimensions of QOL with lower scores.
These findings are in accordance with other studies in adolescents where it was shown that headache was associated with reduced QOL (14)–(19), with the greatest impact in the areas of physical wellbeing for all types of headache. In contrast to other studies (16–19), we did not find reductions in mental, social and school functioning in adolescents with migraine after adjusting for relevant socio-demographic variables.
Likewise, our models did not reveal reductions in emotional functioning and mood in subjects with TTH, as reported by Talarska (27), but rather reduced family-related QOL. Subjects suffering from MH appeared to be most impaired, with significantly reduced scores in physical and emotional wellbeing, family- and school-related QOL. Another study of the present sample revealed that subjects with MH reported a broad spectrum of psychopathological abnormalities (28). These findings raise the question whether MH might rather be a marker of a more generalized problem characterized by higher psychosocial impairments involving a broad spectrum of wellbeing. In this sense, MH reflects not only a primary headache, but rather a general response to the challenges of adolescence, and therefore accounts for a comparatively large number of cases (11%) who reported suffering from headache at least once per month during the last 6 months but did not fit the classification of migraine and/or TTH.
There is an ongoing debate whether migraine and TTH might phenomenologically co-exist or whether TTH attacks in migraineurs might actually be mild migraine attacks (29). Some authors report combined migraine plus TTH cases as a separate classification category (13,30,31). The results of our present study support the view that the combined classification might be close to migraine, as reductions in QOL observed in subjects with migraine plus TTH were similar to those in subjects with pure migraine.
Although the impact of headache on QOL appeared to be small, the size of the effect was higher than that observed for other chronic conditions in children, such as spina bifida, myelomeningocele, type 1 diabetes, hemophilia or asthma (32–37) and comparable to the effect size observed for obesity and attention deficit hyperactivity disorder (37), all assessed with the same instrument (KINDL-R). More importantly, the social relevance on a population level of reduction of QOL due to headache is high, as many adolescents (48%) are affected by headache.
Strengths and limitations
The major strength of this study is its population-based data collection, with enrollment of adolescents from different urban and rural areas as well as different types of schools (secondary schools, grammar schools) and those already in the workforce. Furthermore, with the application of multiple regression models adjusting for relevant socio-demographic factors, we were able to determine the adjusted estimates of the effect of (special types of) headache on QOL.
Frequencies of migraine and TTH in the present study correspond satisfactorily with prevalence estimates in other recent studies on adolescent headache in Europe (10,11) and especially in Germany (12,13).
One major weakness of the study is that headache classification was based on only a self-administered questionnaire. However, a number of studies report reasonable sensitivity, specificity and predictive values for a number of migraine screening questionnaires based on a few simple items for adults (38–44) and adolescents (45–47). In the present study, the items of the headache questionnaire were those used in a recent epidemiological study in Germany (13) and similar to recently published IHS criteria (26).
Differences between the sub-sample eligible for the headache study and the total study sample constitute a potential source of bias. The only significant difference between the sub-sample and the total study group, however, pertained to the number of subjects attending grammar schools. Because ‘attending a grammar school’ was not associated with the prevalence of headache or with QOL measures in our data, sampling bias appears unlikely.
Conclusions
A small but significant reduction of QOL due to headache was observed in adolescents, which could not be explained by confounding variables. The impact on QOL was more pronounced than that seen in many chronic conditions studied in adolescence and similar to that observed for obesity and attention deficit hyperactivity disorder. Many forms of headache in adolescents may be either prevented or treated by psychological interventions (see Trautmann et al. (48) for meta-analysis) and QOL may improve with decreasing headache intensity and frequency (49). Prevention of headache might help to improve QOL in adolescents, while psychological treatment—although improving recurrent pain—may not improve QOL to a similar extent (50).
Footnotes
Funding
This study is part of the project MobilEe: Mobilfunk – Exposition und Befinden (“Mobile Phone Exposure and Wellbeing in Children and Adolescents), which was funded by the Federal Office for Radiation Protection (BfS Oberschleißheim/Munich) as part of the German Mobile Telecommunication Research Programme. The authors report no conflicts of interest.
Acknowledgements
The authors would like to thank the field workers for their invaluable engagement in data collection. We thank all participants for their time and efforts. Further, we thank the participating towns for their support and the provision of space to run the data collection. The authors gratefully acknowledge the editorial assisstance of Katie Ogston in the preparation of this manuscript.