
Abstract
Objectives: To study the frequency and significance of distal hyperintense vessels (HVs) on fluid-attenuated inversion recovery (FLAIR) imaging in patients with reversible cerebral vasoconstriction syndrome (RCVS).
Methods: Patients with RCVS were recruited during 2002 through 2009. Prominence and location of HVs on FLAIR images during the acute and recovery stages were documented. Clinical profiles, vasoconstriction scores, mean flow velocities of the middle cerebral artery (VMCA) and posterior cerebral artery (VPCA), and the Lindegaard index (LI) were collected for analysis.
Results: Ninety-five patients with RCVS (11M/84F, mean age 47.8 ± 10.9 years) were recruited. Twenty-one (22.1%) had FLAIR HVs, which were noted at a mean of 14.3 ± 12.7 days and resolved by 44.9 ± 18.8 days. Compared with patients without HVs, patients with this finding had higher vasoconstriction scores for all arterial segments; higher VMCA (121.0 ± 39.5 cm/s vs. 93.3 ± 27.8, p = 0.002), VPCA (73.3 ± 35.0 vs. 50.5 ± 17.8 cm/s, p = 0.010), and LI (2.8 ± 1.2 vs. 1.9 ± 0.5, p = 0.018), and complications such as posterior reversible encephalopathy syndrome (PRES) [8/21 (38%) vs. 0/74 (0%), p < 0.001] or ischemic stroke [5/21 (24%) vs. 1/74 (1%), p = 0.002].
Conclusions: HVs in patients with RCVS might be attributed to the failure of cerebrospinal fluid (CSF) signal nulling on FLAIR imaging due to severe cerebral hemodynamic derangements and were associated with more frequent ischemic complications.
Keywords
Introduction
Reversible cerebral vasoconstriction syndrome (RCVS) comprises a group of disorders characterized by recurrent, acute-onset severe headaches (usually thunderclap headaches) and reversible cerebral vasoconstriction (1). RCVS is more common than previously thought and is important in the differential diagnosis of aneurysmal subarachnoid hemorrhage (SAH). The clinical features of RCVS have been well characterized in recent years (2,3). RCVS tends to be self-limiting and dissipates within 3 months; however, RCVS in some patients can be complicated by posterior reversible encephalopathy syndrome (PRES), ischemic strokes over watershed zones, cortical SAH, or intracerebral hemorrhage (ICH) (2–5). Vasoconstrictions in RCVS are pervasive and outlast headache resolution. The severity of the vasoconstrictions, especially those in the middle cerebral arteries (MCAs) revealed by transcranial color-coded sonographic studies (TCCS) or magnetic resonance angiography (MRA), is associated with ischemic complications (6,7).
Fluid-attenuated inversion recovery (FLAIR) imaging is a highly sensitive magnetic resonance (MR) technique for the detection of parenchymal or sulcal signal changes (8–12). Cumulative evidence indicates that FLAIR sequence is also sensitive in detecting hyperintense vessels (HVs) in diseases with severe stenosis or occlusion of major cerebral arteries (13,14). HVs are hypothesized to result from abnormal blood flow kinetics in small arteries, veins, or collateral vessels (14). In a case-control study, HVs were found in 13 of 19 symptomatic patients with multiple intracerebral arterial stenoses (68%), but in only one of their age-matched controls (5.2%) (15). Eight out of the 19 patients had a diagnosis of reversible angiopathy (i.e. RCVS) and all eight patients (100%) had HVs on FLAIR imaging (15). However, the small sample size makes it difficult to draw a definitive conclusion from these observed associations. Furthermore, this paper does not provide relevant hemodynamic and clinical data in correlation with the occurrence or extent of HVs. The significance of HVs in patients with RCVS remains unclear. Therefore, we investigated the frequency and significance of HVs on FLAIR images in consecutive RCVS patients.
Methods
Subjects
We prospectively recruited consecutive patients presenting to the headache clinic at the Taipei Veterans General Hospital (TVGH) with recurrent thunderclap headaches and RCVS between 2002 and 2009. The diagnosis of RCVS required fulfillment of the following criteria:
At least one acute-onset severe headache (thunderclap headache) with or without focal neurological deficits; Vasoconstrictions demonstrated on MRA; Reversibility of vasoconstrictions demonstrated by at least one follow-up MRA within 3 months; SAH or other intracranial disorders ruled out by appropriate investigations.
The diagnostic criteria was based on the criteria ‘benign (or reversible) angiopathy of the central nervous system’ proposed by the International Classification of Headache Disorders, 2nd Edition (ICHD-2; code 6.7.3), with the exception of the duration criterion D (16), and also fulfilled the essential diagnostic elements of RCVS proposed by Calabrese et al. (1), except for cerebrospinal fluid (CSF) studies. Clinical profiles including demographic information and headache characteristics were constructed. Lumbar puncture with CSF analysis was performed to exclude SAH if the patient gave consent. The study protocol was approved by the TVGH Institutional Review Board. All patients provided informed consent before entering the study.
Neuroimaging studies
Brain MRI
All subjects underwent sequential brain MRI with adequate sequences to exclude intracranial lesions, using a procedure that has been reported elsewhere (6,7). For each image series, 20 slices covering the entire brain (matrix 240–256 × 256–320; field of view 22–24 cm; slice thickness 4–5 mm; interslice gap 1 mm) were obtained. The presence of HVs on FLAIR imaging was carefully evaluated in every subject. This targeted image finding was interpreted by an experienced neuroradiologist (JFL) who was blinded to the clinical data. A HV was defined as a linear, serpentine, or dot-appearing, high-intensity signal along the cortical sulci and subarachnoid space on at least two contiguous axial slices. The vascular distribution of HVs in different vascular territories [i.e. anterior cerebral artery (ACA), middle cerebral artery (MCA), or posterior cerebral artery (PCA)] was also recorded. The extent of the HV was graded as 1) absent, 2) subtle, or 3) prominent, which was adopted from a previous study that rated the extent of distal HVs in the perfusion lesions in acute ischemic strokes (14). In brief, subtle HV was defined as the presence of HVs in less than or equal to one-third of the cortical sulci of the corresponding vascular distribution. The presence of HVs in more than one-third of the cortical sulci was defined as prominent (Figure 1). Gradient echo T2-weighted MRI was used to evaluate whether these hyperintense signals on FLAIR sequence represented blood (8,11,17).
Hyperintense vessels and their resolution on FLAIR images in patients with RCVS. (A) Subtle and prominent hyperintense vessels over the territory of the middle cerebral artery (indicated by arrows). (B) Subtle and prominent hyperintense vessels over the territory of the posterior cerebral artery (indicated by arrows). FLAIR, fluid-attenuated inversion recovery; RCVS, reversible cerebral vasoconstriction syndrome.
PRES and ischemic stroke were identified through the comparison of FLAIR images with diffusion-weighted images (DWIs) and apparent diffusion coefficient mapping on sequential MR studies. HVs located immediately along the infarcted cortices or PRES lesions were recorded as uninterpretable. This study also recorded the presence or absence of white matter hyperintense lesions (WMHLs) in addition to PRES and ischemic stroke. WMHLs had to be hyperintense both on T2-weighted fast spin-echo MR and FLAIR imaging; when signal alteration was >3 mm and present on two or more contiguous slices, it was recorded as a single lesion. On the basis of signal characteristics, shape, and location, Virchow–Robin spaces were identified and excluded. The number of WMHLs was calculated and their distribution according to arterial territories was recorded.
MRA was obtained using a 3D time-of-flight (TOF) MR technique with multi-slab reconstruction and maximum intensity projection (MIP) post-processing to evaluate for cerebral vasoconstrictions and their reversibility. The basilar artery (BA) and the first and second segments of the ACA (A1 and A2), MCA (M1 and M2), and PCA (P1 and P2) were evaluated. The vasoconstriction severity was graded on a five-point scale: 0 (<10%), 1 (10 to < 25%), 2 (25 to < 50%), 3 (50 to < 75%), and 4 (≥75%), and designated as the ‘vasoconstriction score’ for each arterial segment for further analysis. For arterial segments with the same designations, such as bilateral M1, M2, A1, A2, P1, and P2, the bilateral vasoconstriction scores were averaged to derive a mean score.
MRA follow-up
Sequential MRAs were performed in all subjects to determine whether the focal narrowing of cerebral arteries was reversible or attributable to congenital hypoplasia, atherosclerosis, or dissection. Reversibility was considered present if the vasoconstriction score of ≥ one arterial segment returned from higher scores (i.e. 2–4) to scores of 1 or 0. The follow-up intervals depended on the clinical conditions of patients and the availability of MR scanners; the follow-up MRA examinations were conducted until normalization of vasoconstrictions or within 3 months after disease onset.
Brain computed tomography (CT)
The brain CT imaging that some patients received prior to the MR studies was reviewed, if available, to evaluate whether there was a corresponding hyperdense lesion along the cortical sulci with HVs on FLAIR imaging.
Transcranial color-coded sonographic studies
Patients recruited after October 2003 also received TCCS. A detailed protocol has been previously described (6). The mean flow velocity of the MCA (VMCA) and PCA (VPCA) and the Lindegaard index (LI), which were calculated by dividing the VMCA by the mean flow velocity of the ipsilateral distal extracranial internal carotid artery (ICA) obtained within one day of MRA performance, were used to correlate with the presence or absence of HVs. To analyze the relationship of headache laterality and location with HVs, the bilateral cerebral arteries (MCAs or PCAs) in a single patient were treated as independent vessels since they were not always symmetrical. To calculate the hemodynamic differences between patients with or without HVs, the worse one of the bilateral cerebral arteries in a single patient was selected.
Statistics
Descriptive statistics were presented as median, mean ± SD, or percentages. The Shapiro–Wilk test was used to test for normality. Parametric tests were employed when the variables to be compared did not deviate from a normal distribution. Means were compared using the unpaired t-test or one-way analysis of variance (ANOVA), and proportions were compared using the chi-square test or Fisher’s exact test when appropriate. All calculated p values were two-tailed, and statistical significance was defined as p < 0.05.
Results
Demographics
We reviewed the brain MRIs of 95 consecutive patients with RCVS [11 males and 84 females, mean age 47.8 ± 10.9 years (range 10–76)]. Each patient had a mean of 2.1 (range 1–8) follow-up MRI/MRA studies in this study. Reversibility of vasoconstrictions on MRA was demonstrated in all patients. Twenty-three patients (24.2%) had a history of hypertension and 39 (41.1%) experienced a blood pressure (BP) surge during headache attacks. The mean maximal systolic BP during the headache attacks was 155.3 ± 30.4 mmHg (range 101–220 mmHg). Six subjects (6.3%) had type 2 diabetes mellitus, 22 (23.2%) had a history of migraine headaches, and one (1.1%) had coronary artery disease. Among the 84 female patients, 39 (46.4%) were postmenopausal and 15 (17.9%) were taking hormone therapy at disease onset. Six of the recruited patients had some possible secondary causes of RCVS or associated conditions, including the use of a selective serotonin reuptake inhibitor (n = 1) or pseudoephedrine (n = 1), an unruptured aneurysm of the intracranial ICA, left distal vertebral artery (VA) dissection, post-partum state, and microangiopathic hemolytic anemia (7). None of the patients had objective neck stiffness. On average, the patients had 6.7 ± 6.4 (median 4, range 2–45) thunderclap headache attacks in a mean period of 18.0 ± 10.6 (median 15, range 5–45) days. Triggers such as exertion, defection, sexual activity, bathing, etc. were identifiable in 78 (83.0%) patients.
MRI findings
Distribution and severity of hyperintense vessels
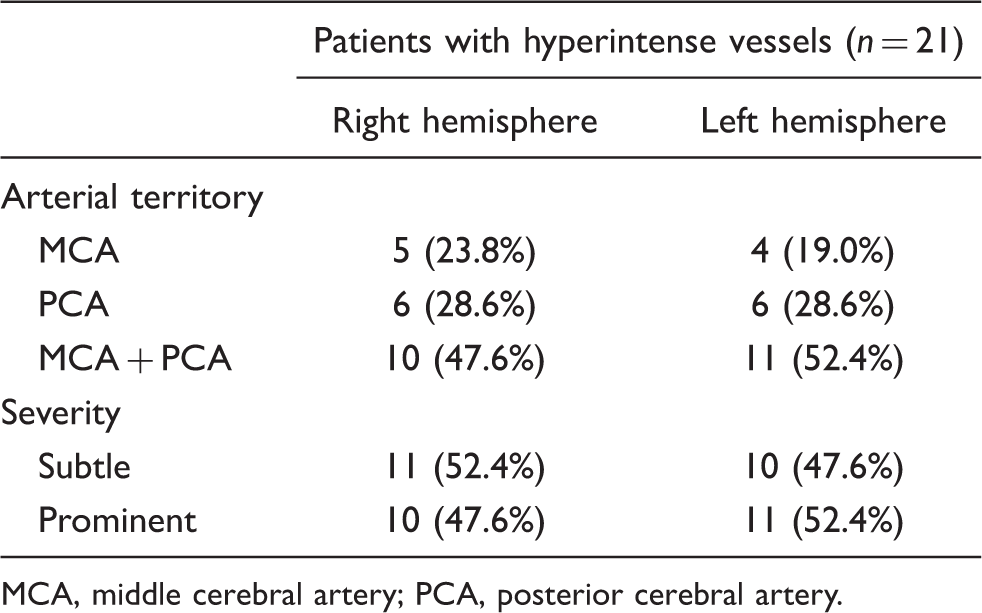
MCA, middle cerebral artery; PCA, posterior cerebral artery.
None of these HVs demonstrated hypointensity on gradient echo, T2-weighted MRI, which excluded the possibility of bleeding. The HV was found at a mean of 14.3 ± 12.7 (range 1–45) days after headache onset and disappeared on 44.9 ± 18.8 (range 7–70) days. Eight patients (8.4%) developed PRES. Six patients (6.3%) developed ischemic strokes; four of them occurred concomitantly with PRES. The PRES were located predominately over the posterior border zone (100%), with six purely in the posterior border zone and two having additional involvement over the anterior and internal border zones. The ischemic infarct lesions involved the posterior border zone in five patients (83%) and were multifocal without restriction to a specific arterial territory in one patient (7).
WMHLs on FLAIR imaging were noted in 43 (45.3%) of the subjects. These WMHLs were located in the ACA territory in 26 patients (60.5%), the MCA territory in 42 patients (97.7%), and the PCA territory in 11 patients (25.6%). The median number of WMHLs was 5.0 (range 1–102). None of the 95 patients had hemorrhagic complications or other intracranial lesions.
Brain CT findings
Twenty-six of our patients had received a brain CT prior to their MR studies, including eight with HVs. However, none of the brain CTs demonstrated comparable hyperdense lesions over the cortical sulci.
CSF studies
CSF studies were undertaken in 15 (15.9 %) patients. Five out of the 21 patients (24%) with HVs had undergone lumbar puncture. In each case, their CSF was clear and colorless, and pressure, cell counts, metabolic and immunological analyses were normal.
Correlation between clinical parameters and FLAIR HVs
Patients with HVs had a higher maximum BP (178.5 ± 28.1 vs. 147.8 ± 27.4 mmHg, p < 0.001) than those without HVs. Patients whose headache was occipital in location were more likely to have HVs than those with headaches in other locations (55.6% vs. 22.6%, p = 0.009). Parameters that did not differ significantly between patients with and without HVs included: gender; menopausal status; history of hypertension; diabetes mellitus; migraine; coronary artery disease; hormone therapy; headache-associated symptoms; BP surge; the types and numbers of triggers; headache duration; and the total number of thunderclap headache attacks (data not shown). In addition, the laterality of the headaches or their localization outside the occipital region was not associated with the anatomical distribution of HVs.
Correlation between HVs and the severity of vasoconstriction
The mean vasoconstriction scores of all major arterial segments in patients with HVs were higher than those without HVs (Table 2). Among all subjects, five had no TCCS studies and 12 had bilateral trans-temporal window thickening. Consequently, 78 patients had measurements available for the VMCA and LI. Among them, those with HVs (n = 15) had a higher corresponding VMCA (121.0 ± 39.5 vs. 93.3 ± 27.8 cm/s, p = 0.002), VPCA (73.3 ± 35.0 vs. 50.5 ± 17.8 cm/s, p = 0.010), and LI (2.8 ± 1.2 vs. 1.9 ± 0.5, p = 0.018) than those without (n = 63). The comparison of these sonographic parameters between those with prominent (n = 9), subtle (n = 6), and no HVs were as follows:
VMCA: 126.8 ± 40.5 vs. 112.3 ± 39.9 vs. 93.3 ± 27.8 cm/s, p = 0.003; VPCA: 82.8 ± 29.4 vs. 65.5 ± 38.7 vs. 50.5 ± 17.8 cm/s, p < 0.001; LI: 3.1 ± 1.4 vs. 2.5 ± 0.8 vs. 1.9 ± 0.5, p < 0.001 (ANOVA). Comparison of the mean vasoconstriction scores between patients with and without hyperintense vessels on FLAIR imaging M1, first segment of middle cerebral artery; M2, second segment of the middle cerebral artery; A1, first segment of the anterior cerebral artery; A2, second segment of the anterior cerebral artery; P1, first segment of the posterior cerebral artery; P2, second segment of the posterior cerebral artery. FLAIR, fluid-attenuated inversion recovery; HV, hyperintense vessel.

Relationship between HVs and complications
Patients with HVs were more likely to have PRES [8/21 (38%) vs. 0/74 (0%), p < 0.001], ischemic stroke [5/21 (24%) vs. 1/74 (1%), p = 0.002], or WMHLs [14/21 (66.7%) vs. 29/74 (39.2%), p = 0.026] than those without. Except for one patient who had an HV prior to the development of an ischemic stroke (Figure 2), all the other patients with PRES or ischemic stroke had an HV on the same MR scan.
Hyperintense vessel predating ischemic stroke. (A) Hyperintense vessel (indicated by an arrow) noted 14 days after headache onset. (B and C) Acute ischemic stroke developed over the bilateral thalamus and the right parieto-occipital area on day 17.
Discussion
This study demonstrates that HVs on FLAIR imaging could be found in one-fifth of patients with RCVS. These HVs were transient, noted on around day 14 after headache onset, and lasted for approximately 6 weeks. The presence of HVs indicated more severe disease, as demonstrated by measurements of more severe cerebral vasoconstriction and a higher incidence of ischemic complications including PRES, ischemic stroke, or WMHLs.
HVs observed in our patients were likely contributed by very low flow velocities of the distal branches of the cerebral arteries or their leptomeningeal anastomotic collateral vessels, as observed in Moyamoya syndrome or acute ischemic stroke (13,14). The vasoconstrictions in RCVS, when severe enough, could alter the hemodynamics of distal arterioles and leptomeningeal networks, which in turn would lead to the failure of nulling the normal CSF signal within the sulcal space on the MRI FLAIR imaging. Our finding that HVs were associated with more severe hemodynamic derangement in proximal cerebral arteries was supportive of this hypothesis. One study reported that up to 22% of the RCVS patients had cortical SAH (3), which was almost the same as the frequency of HVs identified in our study subjects (22.1%). However, we do not consider the HVs we observed to be cortical SAH because the well-circumscribed dot- or tubular-like appearance of hyperintense lesions running through the sulci (Figures 1 and 2) was dissimilar to the hyperintensities of SAH which were usually diffuse and occupied the entire sulcus (18). Besides, gradient echo T2-weighted MRI, though not the gold standard technique, did not find hypointensity over the corresponding cortical sulci (11, 17). In addition, in eight patients who had brain CT scans, none demonstrated hyperdense lesions over the cortical sulci.
The vascular territorial distribution of HVs in patients with RCVS was MCA, PCA, or a combination of the two. Because the frequency of HVs in patients with PRES or ischemic stroke was much higher than in those without, we hypothesized that a HV was a consequence of compromised cerebral perfusion resulting from more severe vasoconstrictions within the MCA and PCA territories (7). In addition, our study demonstrated that patients with HVs had an initial maximum VMCA of up to 121.0 ± 39.5 cm/s and an LI of up to 2.8 ± 1.2, which was in proximity to the cut-off criteria for predicting PRES or ischemic stroke (VMCA > 120 cm/s and LI > 3) (6). Hence, the existence of HVs might be considered a surrogate marker for disease severity. Patients with headaches over the occipital area were more likely to have HVs. Whether these hyperintense and perhaps more engorged vessels could facilitate the activation of perivascular nociceptors and contribute to the anatomical distribution of pain requires further study. WMHLs, though more prevalent in patients with HVs, were predilectionally distributed over the anterior circulation. The nature and pathogenesis of WMHLs in patients with RCVS requires further exploration.
Because most patients with PRES or ischemic stroke had HVs on the same scan, we were unable to evaluate whether HVs could be predictive of PRES or ischemic stroke. However, one of our patients did have a HV prior to his ischemic stroke. One recent report also demonstrated the presence of FLAIR HV and leptomeningeal gadolinium enhancement 4 days prior to the development of characteristic PRES in a patient with eclampsia (19). Considering the overlapping clinical features and radiological findings of eclampsia and post-partum angiopathy (20), it is plausible that the presence of HVs in an ultra-early MR study in patients with RCVS could herald the occurrence of PRES or ischemic stroke. Nonetheless, more studies which utilize neuroimaging at an earlier stage of the disease course are required to validate this speculation.
Our study had some limitations. First, in the case of HV prior to ischemic stroke, arterial distribution between initial HV sign and the subsequent stroke was not exactly the same. The HV was located over the right MCA territory, whereas the stroke lesions were located over the PCA and MCA–PCA watershed zones. We do not know the exact reason for this mismatch but provide the following possible explanations:
Vasoconstrictions are usually pervasive and can evolve over time in patients with RCVS (3,7); Since there might be individual variation of intracranial anastomotic networks, HVs might not have an exact localizing value for vasoconstrictions. The presence of a HV in the right MCA territory might not directly be resulted from altered hemodynamics of the right MCA, but could be a consequence of both the right MCA and PCA; The vulnerability (or threshold) to ischemic lesions is different between different brain regions. In the exemplified case, the presence of a HV may be taken as a marker for compromised hemodynamics rather than a direct localizing indicator of ischemic stroke.
Secondly, we could not completely prove or disprove the possibility that a HV is of arterial or venous origin because of the limitations of current MR sequences. Prospective MR studies using a higher magnetic field (such as 3 Tesla MR), more thin-layered cuts, and multi-sequences, including pre- and post-contrast images, might be of help to differentiate the nature of this imaging finding in some patients.
Thirdly, a low percentage of our patients had CSF studies, because in Taiwan patients generally have a negative impression of lumbar puncture. Although, during the long-term follow-up, none of our RCVS patients without CSF studies developed SAH, the importance of obtaining CSF to rule out other conditions should not be overlooked.
Finally, though the patients were prospectively recruited, the timing with which they entered the study was inevitably varied depending on the nature of disease and timing of medical help seeking. Therefore, we were unable to determine the exact timing for the appearance of a HV and could not confirm its predictability for complications. Nonetheless, this study showed that regardless of the timing of MR, the appearance of HVs was correlated with more severe hemodynamic disturbances. The presence of HVs might be an important reminder for clinicians to be vigilant about disease severity.
Footnotes
Funding
This study was supported in part by grants from Taiwan National Science Council [97-2628-B-010-007-MY3 & 99-2314-B-075-036-MY3], Taipei Veterans General Hospital [VGHUST100-G7-1-1, V100C-087], NSC support for Centre for Dynamical Biomarkers and Translational Medicine, National Central University, Taiwan [NSC 99-2911-I-008-100] and Brain Research Center, National Yang-Ming University and a grant from Ministry of Education, Aim for the Top University Plan.
Conflict of interest declaration
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.