
Abstract
Background: Oculomotor ophthalmoplegic migraine (O-OPM) occurs in many children, and in some cases MRI shows a small mass in the root exit zone (REZ) of the oculomotor nerve. This mass is considered to result from nerve hypertrophy caused by repeated demyelination.
Case results: A 51-year-old man has been on oral medication for O-OPM, which he had from 6 years of age. However, the frequency and intensity of his migraine attacks have gradually increased. Brain magnetic resonance imaging (MRI) revealed a small nodular mass in the REZ of the oculomotor nerve. The mass was initially diagnosed as oculomotor schwannoma and tumor resection was attempted. However, as the mass was tightly adhered to the oculomotor nerve and hemorrhagic, biopsy was performed. The pathological diagnosis was neuromuscular hamartoma.
Conclusion: The small nodular mass in the REZ of the oculomotor nerve may be a hamartoma associated with congenital factors and may possibly be the primary pathology of O-OPM in this case.
Keywords
Introduction
The International Headache Society defines ophthalmoplegic migraine (OPM) as recurrent attacks of headache with migrainous characteristics associated with paresis of one or more ocular cranial nerves (commonly the oculomotor nerve) with no demonstrable intracranial lesions other than changes within the affected nerve on magnetic resonance imaging (MRI) (1). Based on these characteristics, OPM is diagnosed when at least two attacks with migraine-like headaches are accompanied or followed within 4 days of onset by paresis of one or more of the third, fourth or sixth oculomotor cranial nerve.
OPM is very rare, with an estimated prevalence rate of 0.7 per million (2). Such a limited number of reported cases make it difficult to analyse its unique pathological state characterized by neuralgia preceded by migraine. Recently, Carlow (3) has reported six pediatric cases of oculomotor ophthalmoplegic migraine (O-OPM) with symptoms limited to the oculomotor nerve. MRI abnormalities were detected in all of these cases at the root exit zone (REZ) of the oculomotor nerve, suggesting that a focal pathological process underlies O-OPM (3).
In this article, we report a patient who has been an O-OPM sufferer for 45 years. MRI revealed nodular enhancement in the REZ of the oculomotor nerve and neuromuscular hamartoma (NMH) was diagnosed histopathologically.
Case presentation
The patient was a 51-year-old man who has suffered recurrent headache attacks over the past 45 years. There were no findings suggesting neurofibromatosis and no family history of migraine. A left outer strabismus was noted at birth. From around 6 years of age, he had left retrobulbar pain once or twice a month. Following detailed examinations at several hospitals, O-OPM was diagnosed. Symptomatic treatment was started with single-use non-steroidal anti-inflammatory drugs (NSAIDs). The frequency of O-OPM attacks was initially once or twice a month but this increased to once a week with greater intensity from around 39 years of age. His condition improved with the addition of a single-use steroid (prednisolone, 20 mg/day) to the NSAIDs. However, the control of his headaches deteriorated from 2007, and he started to have headaches at least once every 2 to 3 days. In addition, he gradually developed ptosis and left mydriasis. Brain MRI revealed an enhanced nodular mass in the REZ of the left oculomotor nerve. Although he had clear consciousness, his left pupil was dilated, and there was no direct or indirect pupillary light reflex. The left eye was completely turned outward, showing incomplete ptosis. Thin-slice imaging using 3-Tesla MRI showed an intensely and homogeneously enhanced lesion in the REZ of the inner upper part of the left oculomotor nerve (Figure 1A). Oculomotor nerve schwannoma was suspected.
Preoperative 3-Tesla brain MR images and intraoperative findings. (A) Gadolinium-enhanced brain magnetic resonance imaging (MRI): sagittal T1-weighted MRI images show an enhanced nodular mass at the root exit zone (REZ) of the oculomotor nerve. (B) An operative field view under a rigid endoscope. A swollen oculomotor nerve and a white, elastic hard mass were confirmed (asterisk: oculomotor nerve, arrow: mass).
A left frontotemporal craniotomy was performed using the trans-sylvian approach to the oculomotor nerve. Under a surgical microscope, the mass was white, elastic and made of slightly hard tissue adhering to and wrapped around the REZ of the oculomotor nerve. When this area was observed using a rigid-type endoscope, a lesion was found wrapped around the entire circumference of the REZ of the oculomotor nerve, and the nerve appeared to be swollen (Figure 1B). Separation of the mass from the oculomotor nerve was attempted, but this caused severe hemorrhage. The surgical procedure was therefore terminated after obtaining a biopsy tissue specimen sufficient for pathological diagnosis. The biopsied tissue consisted of several strips of peripheral nerve bundles and interstitial tissue. The interstitium under the epineurium contained a large number of 50 - to 100 -µm-thick strongly eosinophilic fibrous tissues. Being positive for smooth muscle actin (SMA), desmin and the muscle-actin-specific antibody HHF35, this tissue was considered to be smooth muscle tissue (Figure 2A, B). Although neurofilament protein (NFP)-positive axons and S100-positive Schwann cells remained, SMA-positive and HHF35-positive smooth muscle tissues were also found in the nerve bundles. In addition, Schwann cell proliferation was observed, and the axonal structure showed slight edematous swelling (Figure 2C).
Photomicrographs of the resected tissue. (A) Hematoxylin and eosin (HE) staining (original magnification × 40). Several strips of peripheral nerve bundles can be observed, with strongly eosinophilic fibrous structures (arrow) in some areas of the interstitium. (B) Immunohistochemical staining (anti-alpha-smooth muscle actin × 40). The fibrous structures in the interstitium were confirmed to be smooth muscle structures, strongly positive for alpha-smooth muscle actin (arrow). (C) Immunohistochemical staining (anti-alpha-smooth muscle actin, original magnification × 400). Neurofilament-positive nerve bundles were covered with S100-positive myelin sheaths, and smooth muscle structures were positive for alpha-smooth muscle actin and HHF35, indicating features of neuromuscular hamartoma.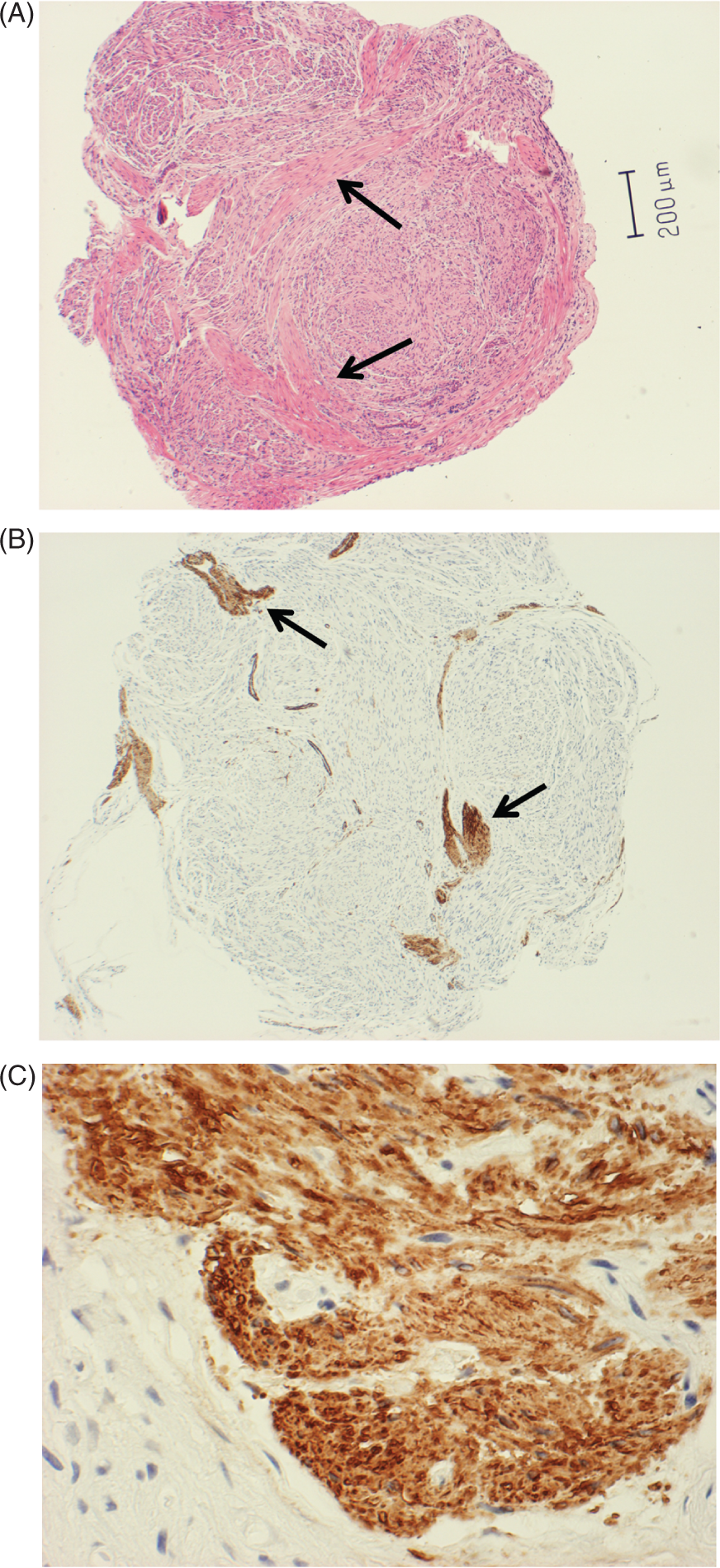
NMH was diagnosed, and the frequency and intensity of his O-OPM markedly improved postoperatively. Although the patient suffered mild retrobulbar pain once every 2 to 3 months, it was immediately alleviated by NSAIDs. However, there has been no improvement in his left oculomotor nerve palsy. In addition, brain MRI findings obtained 2 years postoperatively showed no changes in the lesion in the REZ of the oculomotor nerve.
Discussion
This rare non-neoplastic mass lesion consists of mature skeletal muscle and peripheral nerves, the myocytes being closely associated with nerve fibers and encompassed by the perineurium. The precise nature of this extremely rare lesion remains unclear, but some reports have suggested the possibility of the neuroectoderm undergoing mesenchymal differentiation (ectomesenchyme), and the possible occurrence of skeletal muscle heterotopias within normal peripheral nerves (4,5). Twenty-eight cases of NMH developing in the central nervous system have been reported (6). The optic nerve was the most common site of NMH development, followed by the trigeminal nerve, and then the facial and acoustic nerves. NMH of the oculomotor nerve is extremely rare (6) and only two histologically verified cases have been reported thus far (7,8). Together with the present case, all three cases had repeated episodes of typical O-OPM symptoms over a reasonably long period, and therefore the patients have received long-term treatment with NSAIDs and steroids. Imaging findings in all cases showed a nodular lesion several millimeters in size and with intense enhancement, occurring near the REZ of the oculomotor nerve. All three patients underwent surgical intervention after a preoperative diagnosis of oculomotor nerve schwannoma. Oculomotor nerve schwannoma is fundamentally a painless mass that is not limited to the REZ but often extends from the cistern to the cavernous sinus (9). T2-weighted imaging showed high signal intensity in contrast to the low signal intensity of NMH, and contrast enhancement was often heterogeneous, reflecting intratumoral cyst formation and hemorrhagic changes. There are only two previous reports of oculomotor nerve schwannoma that developed in patients with O-OPM (10,11). However, neither case had a histologically confirmed diagnosis. In particular, the images reported by Bisdorff and Wildanger (10) show a nodular lesion homogeneously enhanced in the REZ. In both cases, the symptoms slightly improved with steroid therapy, and the lesion did not enlarge for a considerable time (10,11). Therefore, we believe that these two cases were highly likely to have been NMH.
The pathophysiology of O-OPM has not yet been fully clarified. We speculate that one possible explanation for this condition may be based on the trigeminovascular theory (3) proposed by Carlow. In all the six child patients reported by Carlow, the observed nodular lesion with a trapezoidal configuration in the REZ might have been NMH. Carlow described that the focal nerve enlargement was due to repeated demyelination and remyelination, and therefore the nerve edema improved upon restoration of the blood-nerve barrier during periods of headache remission, resulting in a decrease in the contrast enhancement of the lesion. Carlow considers the mechanism to be equivalent to the contrast enhancement in the nerve root hypertrophy observed in Guillain-Barre syndrome and chronic inflammatory demyelinating polyneuropathy (3,12–15). During the chronic phase, nerve hypertrophy leads to scar formation, possibly resulting in irreversible oculomotor palsy (3,12–15). However, these six cases were children with a mean age of 3.7 years. During the interictal migraine phase, nodules were present, although the degree of contrast enhancement in the lesion was reduced. Moreover, because the number of migraine episodes was limited (about 1 to 2), these cases are unlikely to have a prolonged course leading to secondary nerve hypertrophy due to repeated neuritis.
In the present case, oculomotor nerve axons were preserved, although slight edematous swelling was observed. There were no obvious findings of inflammatory cell infiltration or demyelination and thus the strong contrast enhancement of the oculomotor nerve was not changed throughout. The nerve bundles were surrounded by smooth muscle tissue intermingled with slightly proliferated Schwann cells (5,16). We can therefore speculate that the trigeminovascular stimulation-induced dilatation of the blood vessels that supply the oculomotor nerve (3,17) could cause contraction of the muscle structure of the NMH (5), and the resulting strangulation of the oculomotor nerve axons may cause ophthalmoplegia. If these mechanisms occur repeatedly over a long period of time, progression of axonal damage may occur, leading to permanent ophthalmoplegia. The NMH mass in the present case was separated from the surrounding structures by surgical intervention, and biopsy was performed following the partial application of electric cautery. Given that there was no evidence of dilatation of vessels supplying the oculomotor nerve, we speculate that these procedures may have reduced the vascular supply to the muscle structures involved, leading to an improvement in the frequency and intensity of the O-OPM in this case.
Conclusion
Even though the extent of applicability of these findings is limited as a brief report, we describe an extremely rare case of a patient who had a long history of O-OPM due to NMH developing in the oculomotor nerve. Although the primary cause of O-OPM has been considered to be chronically repeated demyelinative change, the presence of NMH in this case is highly likely to be involved in the etiology of the O-OPM.
Footnotes
Acknowledgements
We are indebted to Roderick J. Turner, Edward F. Barroga and J. Patrick Barron for editing and reviewing the English manuscript.