
Abstract
Background: Headache is often associated with physical trauma and psychological stress. The aim of this study is to evaluate the impact of headache on personnel deployed in war zones and to identify factors associated with return to duty (RTD).
Methods: Outcome data were prospectively collected on 985 personnel medically evacuated out of Operations Iraqi and Enduring Freedom for a primary diagnosis of headache between 2004 and 2009. Electronic medical records were reviewed to examine clinical and treatment patterns and the effect that myriad factors had on RTD.
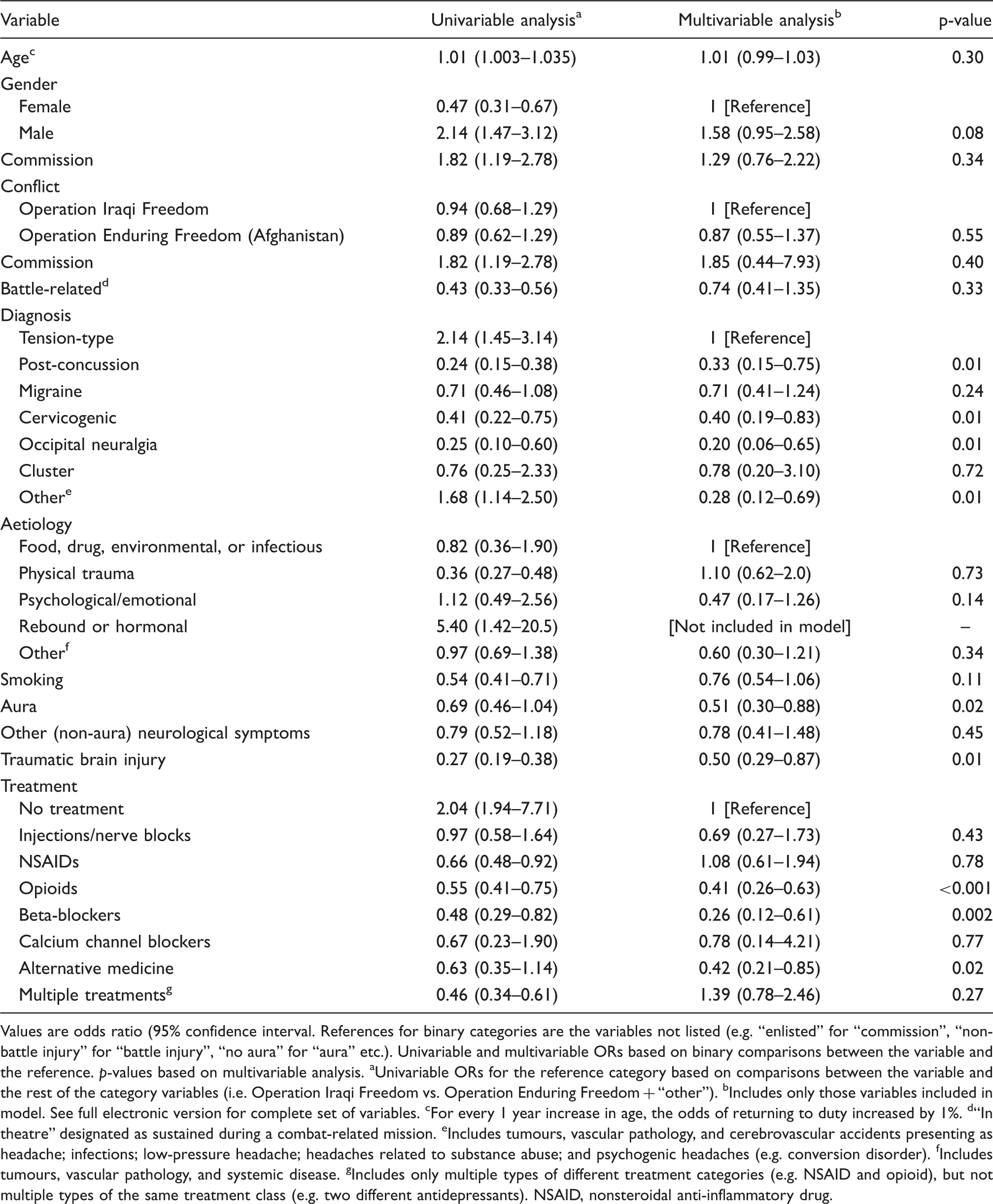
Results: 33.6% of evacuees returned to duty. The most common headaches were post-concussion (34.1%) and migraine (30.0%). Headaches typically associated with trauma such as post-concussion (18.7%), occipital neuralgia (23.1%), and cervicogenic headache (29.7%) had the lowest RTD rates, whereas tension headache (49.6%) was associated with the best outcome. Other variables associated with negative outcome included presence of aura (OR 0.51, 95% CI 0.30–0.88; p = 0.02), traumatic brain injury (OR 0.50, 95% CI 0.29–0.87; p = 0.01), opioid (OR 0.41, 95% CI 0.26–0.63; p < 0.001), and beta-blocker (OR 0.26, 95% CI 0.12–0.61; p = 0.002) use, and co-existing psychopathology (p < 0.001 in univariable analysis).
Conclusion: Headaches represent a significant cause of unit attrition in personnel deployed in military operations, with physical trauma and co-existing psychopathology associated with poorer outcomes.
Keywords
Introduction
In modern warfare, the main causes of unit attrition have never been combat injuries, but rather the same types of ailments that plague and derail non-service members. In World Wars I and II, the top two causes of hospitalization were respiratory and infectious disorders, with neurological disorders, including headache, ranking fifth. By Vietnam, non-battle injuries had surpassed all other disease categories as the leading cause of unit declension, with neurological conditions ranking tenth (1). In Operations Iraqi Freedom (OIF) and Enduring Freedom (OEF), non-battle musculoskeletal injuries continue to account for more injuries than any other injury classification, but neurological illness has risen to the second leading cause of non-combat-related loss of unit strength. Perhaps more concerning, except for psychiatric morbidity, the rise in medical evacuations for neurological injuries over the course of the prolonged conflicts was greater than that observed for any other disease category (2).
Headache is the most common neurological symptom across all demographic and geographic groups. According to some estimates, over 70% of the population suffers from headaches (3,4), with over 45% having an active diagnosis (5,6). Headaches are one of the top 10 causes of disability (5) and missed work days (7), with an economic cost approaching US$ 50 billion per year in the USA (6). In civilian and “in garrison” (non-deployed) military cohorts, the two most frequent categories of headache are tension and migraine, which collectively account for over 90% of cases (8,9).
Recent studies suggest a higher prevalence of these headache types in recently deployed service members and those subjected to severe physical and psychosocial stressors (9–12). During combat operations, traumatic brain injury, which typically manifests as a constellation of neuropsychiatric symptoms that includes post-concussive headache, comprises a significant portion of the neurological disease burden, though the long-term ramifications are still being quantified (13). To date, the epidemiological impact of headache on unit strength has never been studied during wartime. This is surprising, since such an undertaking might affect how valuable resources are allocated, which patients are treated in theatre, and who requires evacuation for more sophisticated evaluation and treatment. Therefore, the main objectives of this cohort study are to estimate the prevalence of the various subcategories of headache during war; provide an overview of treatment; and determine which demographic and clinical variables affect outcome, which is henceforth defined as “return to duty” (RTD).
Patients and methods
This performance improvement protocol was approved for publication by the Walter Reed Army Medical Center Internal Review Board. Permission to conduct this study was granted by the Landstuhl Regional Medical Center and the Deployed Warrior Medical Management Center (DWMMC). The DWMMC was established in November 2002 to coordinate air evacuation missions from OIF and OEF to Landstuhl, Germany, and to orchestrate the management of wounded personnel. Since 2004, DWMMC has served the additional role of being the main database for injured personnel. It is estimated that this prospectively maintained database contains identifying information on over 98% of medically evacuated service members and a significant percentage of redeploying non-service personnel.
A list containing identifying information on service and non-service members medically evacuated out of OIF and OEF between 2004 and 2009 for medical conditions pertaining to “headache” was obtained from DWMMC in January 2010. Preliminary diagnoses used to garner patient data were conferred by a treating physician in theatre and recorded based on the International Statistical Classification of Diseases and Related Health Problems (ICD-9-CM codes) (14) (e.g. 346 for “migraine”, 307.81 for tension headache; see Appendix for full set of ICD-9 surveillance). For personnel with multiple diagnoses, only the primary one is coded; thus, each patient carries a single diagnosis related to headache. Patients who experienced headache consequent to another ICD-9-CM code diagnosed in theatre (e.g. cervical spondylosis, brain tumour) were hence systematically excluded. Other data contemporaneously collected in the DWMMC database include age, gender, rank, service component, date of evacuation, whether the injury was battle or non-battle related, deployment mission (i.e. OIF, OEF or “other”), and disposition (i.e. RTD or transfer to a military treatment facility in the continental USA). A positive outcome was defined as RTD “in theatre”, whereas further evacuation to either a military treatment facility or the service member's base unit was considered a negative outcome. In over 90% of cases, the duration of treatment and disposition from Germany was determined in less than 2 weeks. In the few patients found on record review to have returned to duty after further evacuation to the USA, the ultimate disposition superseded the initial designation.
Record review
Electronic medical records were subsequently reviewed to obtain data on variables related to the nature of the headache, treatment, and those suspected of influencing RTD. These included final diagnosis, aetiology, family history, previous pain complaints, co-existing psychiatric conditions, smoking history, aura and other associated symptoms, and pharmacological and non-pharmacological therapies. For these variables, standardized instruments were only used to screen for psychiatric disorders (e.g. PTSD Checklist- Military Version for PTSD, Hamilton Depression Scale and Beck Depression Inventory for depression).
The operation in which the injury occurred (e.g. OIF, OEF, or “other”) was garnered directly from the database, whose source was the subject's deployment orders. In addition to the primary mission in Afghanistan and neighbouring countries, OEF also included support operations in Kyrgyzstan, Horn of Africa, Trans-Sahara, Philippines, and Western Europe. Along with deployments to Iraq, the designation OIF included missions involving deployment to the Arabian Peninsula, Djibouti, Turkey, and the Republic of Georgia. The category “other” included soldiers deployed to places such as Lebanon and Eastern Europe.
Rank was separated into senior and junior levels based on pay grade, which was considered a surrogate means to gauge time in service. Senior level for enlisted was designated as a non-commissioned officer in the pay grade of E5 and above (e.g. sergeant in the army or marines, and petty officer‐2nd class in the navy). For commissioned officers, senior level was considered to be a field grade or general officer (e.g. major or above in Army or Marines, and lieutenant commander and above in the Navy). The categorization of an injury as battle or non-battle-related was based on information prospectively recorded in the DWMMC database. This designation was based on whether or not the injury was sustained during a combat mission.
Diagnosis and treatment
Headache diagnosis was classified into the following seven categories, based on patient consultation with a neurologist in over 90% of cases: tension-type, migraine, cluster, post-traumatic, cervicogenic, occipital neuralgia, cluster, and other (e.g. brain tumour, prolonged postdural puncture, substance abuse, etc.). Frequently, this diagnosis differed from the preliminary, more general diagnosis conferred in theatre. Disorders wherein facial pain was the primary complaint (e.g. trigeminal neuralgia) were not considered for the purposes of this study. Etiological categories were annotated as physical trauma (e.g. traumatic brain injury); psychological or emotional trauma; food, drug, infectious, or environmental exposure; rebound or hormonal; or other (e.g. infectious, tumour). Previous pain was broken down into prior headache or other (e.g. back pain). Co-existing psychiatric illnesses were divided into affective disorder, anxiety disorder, substance abuse, or combat stress. The headache frequency was delineated as either constant or episodic. Brain imaging abnormalities (computed tomography or magnetic resonance imaging), for which the results were available in 89% of individuals, were loosely defined as any finding that could possibly explain symptoms (e.g. arteriovenous malformations, white matter hyperintensities, calcifications). Treatment was separated into injections, alternative treatments, and pharmacological, which was further subcategorized as antidepressant, anticonvulsant, non-steroidal anti-inflammatory drug, opioid, and beta/calcium channel blockers. For analgesic therapy, it was not always possible to discern when treatment was initiated in relation to final disposition.
Statistical analysis
Statistical analyses were performed using STATA version 11.1 software (StataCorp, College Station, Texas). Exploratory data analysis and summary statistics were calculated with chi-squared testing for categorical variables, and two-tailed t-tests or the Kruskal‐Wallis equality of populations rank test, depending on whether continuous data was distributed parametrically or non-parametrically. Potential explanatory variables were identified a priori for inclusion in a logistic regression model. A logistic regression model was selected to identify associations with potential explanatory variables and the binary outcome of RTD. Explanatory variables were selected for the final model using backwards stepwise logistic regression, and variables with p < 0.20 were included in the final model. Additionally, several non-significant, but potentially clinically relevant variables (commission source, smoking status, and combination therapies) were re-introduced into the model because these factors were deemed clinically relevant. Unadjusted univariable analyses were performed, followed by multivariable logistic regression. A p-value<0.05 was considered statistically significant. Measures of leverage and influence were calculated, and a residual analysis was performed to test the assumptions of the logistic regression model. Additionally, goodness-of-fit testing and deviance testing confirmed that the required assumptions for the model were met.
Results
Subject analysis
The DWMMC database contained a total of 1139 patients with a primary diagnosis of “headache”. Of these, 154 were excluded from analysis, 77 because the presence of headache could not be confirmed as the primary condition based on record review, 58 because no notes were available, 13 because of incorrect identifying information (i.e. miscoding), three because they were <17 years of age, and three because they were repeat evacuations within one tour of duty (in which case only the final evacuation data was tabulated). A majority of excluded subjects were evacuated in 2004 and 2005, before the military electronic medical record system was fully implemented in Iraq and Afghanistan. This left data on 985 subjects for analysis.
Demographic, clinical and treatment data
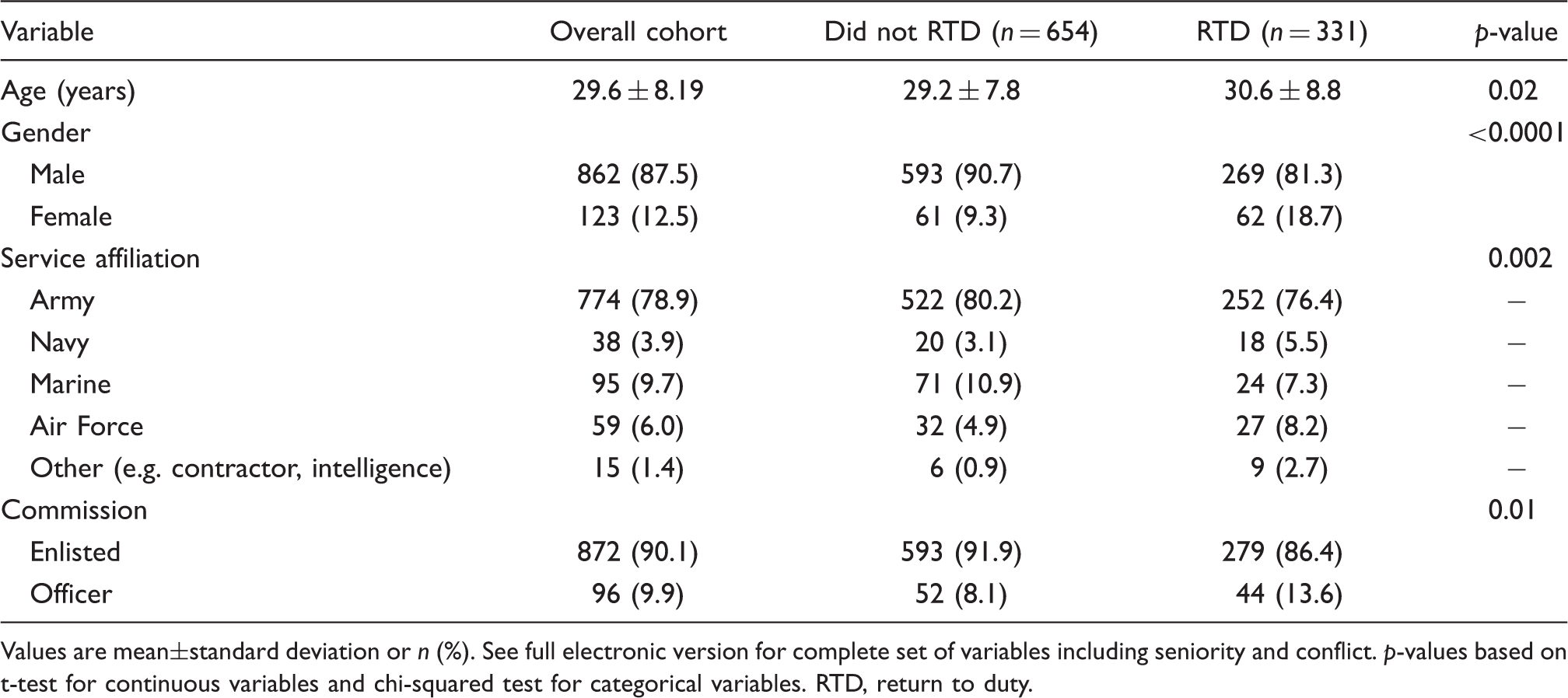
The demographic and clinical data are presented in Tables 1 and 2. The mean age of subjects was 29.6 years (SD 8.19, range 18–63), with 87.5% being male. Over the course of the study, 33.6% returned to duty. Peak evacuations were in 2007 (n = 327), with the nadir occurring in 2004 (n = 56; Figure 1). Overall, 81.3% of evacuations were from OIF, which is roughly commensurate with the proportion of service members deployed in that operation. The most common diagnoses were post-concussive (34.1%), migraine (30.0%), and tension-type (11.4%) headache. When noted, the most frequent inciting event by far was physical trauma (47.6%). Slightly over half (51.9%) of the headaches were episodic. Small proportions noted a positive family history of headache (12.6%) or had brain imaging abnormalities (13.7%). Co-existing psychiatric illness was present in 333 (33.8%) individuals.
Personnel evacuated from Operations Iraqi and Enduring Freedom broken down by year and return-to-duty rate. RTD, return to duty. Demographic variables stratified by outcome Values are mean±standard deviation or n (%). See full electronic version for complete set of variables including seniority and conflict. p-values based on t-test for continuous variables and chi-squared test for categorical variables. RTD, return to duty. Clinical variables stratified by outcome Values are n (%). See full electronic version for complete set of variables including battle or non-battle related injury, presence of brain imaging abnormalities, and presence of non-aura neurological symptoms. p-values based on chi-squared testing between RTD and not RTD. aIncludes tumours, vascular pathology, and cerebrovascular accidents presenting as headache; infections; low-pressure headache; headaches related to substance abuse; and psychogenic headaches (e.g. conversion disorder). bIncludes tumours, vascular pathology, and systemic disease. cRefers to headache history in first-degree relatives. RTD, return to duty. Treatment variables stratified by outcome Values are n (%). P values based on chi-squared testing between RTD and not RTD. aIncludes only multiple types of different treatment categories (e.g. NSAID and opioid), but not multiple types of the same treatment class (e.g. two different antidepressants). NSAID, nonsteroidal anti-inflammatory drug; RTD, return to duty; SNRI, serotonin and norepinephrine reuptake inhibitor; SSRI, selective serotonin reuptake inhibitor; TCA, tricyclic antidepressant. Factors associated with return-to-duty in multivariable analysis Values are odds ratio (95% confidence interval. References for binary categories are the variables not listed (e.g. “enlisted” for “commission”, “non-battle injury” for “battle injury”, “no aura” for “aura” etc.). Univariable and multivariable ORs based on binary comparisons between the variable and the reference. p-values based on multivariable analysis. aUnivariable ORs for the reference category based on comparisons between the variable and the rest of the category variables (i.e. Operation Iraqi Freedom vs. Operation Enduring Freedom + “other”). bIncludes only those variables included in model. See full electronic version for complete set of variables. cFor every 1 year increase in age, the odds of returning to duty increased by 1%. d“In theatre” designated as sustained during a combat-related mission. eIncludes tumours, vascular pathology, and cerebrovascular accidents presenting as headache; infections; low-pressure headache; headaches related to substance abuse; and psychogenic headaches (e.g. conversion disorder). fIncludes tumours, vascular pathology, and systemic disease. gIncludes only multiple types of different treatment categories (e.g. NSAID and opioid), but not multiple types of the same treatment class (e.g. two different antidepressants). NSAID, nonsteroidal anti-inflammatory drug.


The treatment data are shown in Table 3. Over 95% received multiple pharmacological treatments, with nonsteroidal anti-inflammatory drugs prescribed most frequently. Using the total number of deployments in support of OIF and OEF over the 6-year study period as the denominator (15), the overall incidence of evacuation for headache was just under 1 in 1000 (0.10%).
Univariable correlates of return to duty
Factors associated with RTD are outlined in Tables 1–3. Subjects who returned to duty were significantly older (mean age 30.6 vs. 29.2 years; p = 0.015) and more likely to be female (p < 0.0001) than those who did not. Broken down by service affiliation, the lowest RTD rate was found in the Marines (25.3%), while non-service members (60.0%) were most likely to return to duty.
Headaches often associated with trauma (i.e. post-concussive and occipital neuralgia) were significantly correlated with negative outcomes, with only 18.7% and 23.1% of each category RTD, respectively. For patients with occipital neuralgia, 46.2% (n = 24) cited physical trauma as the inciting event, with 11.5% being diagnosed with traumatic brain injury. The presence of constant, rather than episodic, headache symptoms, also predicted a negative result. Similarly, other factors suggestive of disease burden (e.g. presence of aura and brain imaging abnormalities) were weakly associated with not returning to duty. Both smoking and the presence of comorbid psychiatric illness strongly portended a negative outcome. Among the various therapies implemented, patients not receiving treatment were most likely to return to duty (64.9%), whereas the use of opioids (24.9%), beta-blockers (21.5%), and multiple modalities (23.1%) were associated with the lowest RTD rates.
Multivariable analysis
In the multivariable statistical model, most factors associated with outcome in univariable analysis fell shy of statistical significance when confounding factors were controlled for (Table 4). This was attributed to significant colinearity amongst several explanatory variables. Smoking history decreased the likelihood of a service member returning to duty by 24%, but this result did not reach statistical significance (OR 0.76, 95% CI, 0.54–1.06; p = 0.11). Officers were more likely to return to duty than enlisted service members (45.8% vs. 32%), but this fell shy of statistical significance in multivariable analysis (OR 1.29 95% CI 76–2.22; p = 0.34) Battle-related injuries, of which 36.7% (n = 389) consisted of either post-concussion headache (n = 337; 31.8 %) or occipital neuralgia (n = 52; 4.9%), were associated with a non-statistically significant 26% decreased likelihood of a positive outcome (OR 0.74, 95% CI, 0.41–1.35; p = 0.33). However, carrying a diagnosis of occipital neuralgia increased the risk of a poor outcome by 80% (OR 0.20, 95% CI, 0.06–0.65; p = 0.008), as did the diagnoses of post-concussion headache (OR 0.33, 95% CI, 0.15–0.75; p = 0.008) and cervicogenic headache (OR 0.40, 95% CI, 0.19–0.83; p = 0.01). On a related note, the presence of co-existing traumatic brain injury, which occurred in 77.1% of post-concussion headaches (n = 249), reduced the chance of an evacuee returning to duty by 50% (OR 0.50, 95% CI, 0.29–0.87; p = 0.01). Amongst the various therapies, the use of opioids and beta-blockers were associated with a 59% and 74% increased risk of treatment failure, respectively. When interaction variables were added to the model to assess effect modification, no statistically significant interactions were found (p > 0.20).
Discussion
The key finding in this study is that a deployed person medically evacuated from theatre with a primary diagnosis of headache was nearly twice as likely to continue treatment in garrison as they were to return to duty with their unit. Among the various subtypes, the highest RTD rate was associated with tension headache (49.6%), while the lowest rates were observed for post-concussion headache (18.7%) and occipital neuralgia (23.1%). Other factors found to strongly correlate with outcome were frequency (e.g. episodic or constant headache), inciting event, treatment, and co-existing psychiatric diagnosis.
In univariable analysis, perhaps the greatest augur of a poor outcome was a battle-related injury, which correlated with the presence of comorbid traumatic brain injury (r=−0.22; p = 0.0001) and a physical traumatic inciting event (r=−0.23; p = 0.0001). In a recent study comparing RTD rates in military and non-service members, the main divider separating personnel who returned to duty and those who did not was whether or not the nature of injury could be directly attributed to war (16). Whereas nearly 95% of war-related injuries resulted in a negative outcome, over two-thirds of individuals who suffered a disease or non-battle-related injury returned to their unit (16). Headache classifications often associated with physical trauma, such as post-concussion, occipital neuralgia, and cervicogenic headaches (17–23), were collectively associated with a 21.3 % RTD rate, compared to 46.5 % positive outcomes in other subtypes (i.e. tension, cluster, and other). Migraines, which most typically occur without a physical inciting event but are more likely to be associated with trauma than tension-type or other headaches (24,25), were intermediate in RTD rates (40.9%).
For the most part, our findings are consistent with the literature on headaches and war injuries. Officers may be more likely to return to duty than enlisted personnel because of different motivations (i.e. unlike lower enlisted personnel, many commanders volunteer for their duty slots) and job descriptions (i.e. less likely to experience physical trauma on the frontlines). The latter reason may also explain why females, who occupy almost exclusively non-combat positions, had higher RTD rates than males, and marines had the lowest RTD rates. Service members serving in non-combat roles are less likely to suffer battle-related injuries and may be more likely to be able to return to work in a less physical or mentally stressful capacity. Although the numbers were small, non-service members were found to have the highest RTD rates, a phenomenon that may be partially explained by their different roles (i.e. non-combat) and the strong economic incentives they have to remain in duty. Previous studies have found an inverse association between financial remuneration and disability for pain conditions (26) and between headaches and socioeconomic status (27).
Smoking was found to correlate with poor outcome in this study, which is consistent with some studies showing an association with headache (28), but not with others (29). Across the spectrum of psychopathology, having a comorbid psychiatric illness significantly reduced the chance that a service member would return to duty, which is consistent with findings in civilian cohorts (30) and in studies conducted in military personnel with other pain conditions (31–33). The observation that opioids and beta-blockers were associated with a greater likelihood of not returning to duty likely reflects the fact that they tended to be utilized in the most recalcitrant cases. Many experts and guidelines discourage the use of opioid therapy in otherwise healthy patients with refractory, chronic daily headaches (34).
There are several limitations to our study that need to be addressed in order to place our results in context. The principal one is that our population reflects only those individuals who were already evacuated from theatre for headache, so that the true denominator, and consequent overarching RTD rate among all headache sufferers, remains unknown. The second downside is that the individuals in this study constitute a somewhat unique group of individuals subject to exceptional circumstances. Hence, their generalizability to a non-military population, and even service members “in garrison”, is limited.
In conclusion, headaches comprise a significant burden to units and healthcare providers deployed to combat zones. The overall RTD rate of 33.6% is one of the lowest among all injury types, and to some degree reflects the observation that a large percentage of headaches were incurred during combat operations. Although the ability of interventions to return this subset of individuals back to their unit will likely be limited, better guidelines for the management of headache are needed in theatre and post-evacuation.
Footnotes
Funding
This work was supported in part by a Congressional Grant from the John P Murtha Neuroscience and Pain Institute, the US Army, and the Army Regional Anesthesia and Pain Medicine Initiative.
Declaration
The opinions or assertions contained herein are the private views of the authors and are not to be construed as official or as reflecting the views of the Department of the Army or the Department of Defense.
Presentation
This work was presented at Association of University Anesthesiologists 58th Annual Meeting, May 12–14, 2011, Philadelphia, PA, USA.