
Abstract
Aims: The main purpose of the study was to evaluate the impact of weather, and especially sun exposure, on migraine.
Methods: Data from a previous prospective 12-month diary study was compared with meteorological data. We retrospectively evaluated 1250 migraine attacks recorded by a group of 40 women with a mean age of 37.1 years who fulfilled the IHS criteria for migraine with and without aura.
Results: The patients reported more sun-induced migraine attacks on sunny days, but the total distribution of migraine attacks was constant throughout the year. Also, no seasonal variation of migraine, nor any relationships between weather parameters and onset of migraine attacks, were found. An analysis of a subgroup of patients with ‘sun-induced’ migraine showed a significant increase in frequency of migraine attacks in the summer compared to the winter (p = 0.04).
Conclusion: This study confirms that sunlight might be a trigger for migraine, but a risk for increased impact of light on the total ailment of migraine headache should be searched for in a subgroup of sensitive migraineurs.
Introduction
The prevalence of migraine approximates 10% and is one of the most common causes of disability in adult populations (1). Knowledge about how to reduce the influence of trigger factors is probably an important strategy to reduce the ailment of migraine. A majority of patients, especially those who experience aura, report that trigger factors often precipitate migraine attacks (2,3). Menstruation, sleep disturbance, light exposure, stress, smoke, and alcohol are some common triggers reported by patients (3).
Almost the entire region of 460,000 inhabitants in North Norway is located north of the Arctic Circle. During the winter there is a long period with little sun, and the sun does not rise above the horizon from about 20 November until 20 January in the city of Tromsø at latitude between 69° and 70° north. Equivalent to this dark season, there are several months with bright daylight (light season) even at midnight in the summer period. It is a clinical experience that exposure to bright sunlight may trigger migraine attacks in some patients. Both the variation and the intensity of the light may be the precipitating cause (4), but the neural mechanism for this is not known. Modulation of dura-sensitive thalamocortical neurons by non-image-forming retinal pathways has been proposed as a possible mechanism by Noseda et al. (5). Previous questionnaire and diary studies in our area have shown an increase in migraine attacks during the summer (6), especially in those with aura (7,8). Consequently, migraine patients in North Norway reporting sunlight as a trigger for migraine seem to be a problem mainly in migraine with aura and possibly confined to a subgroup of migraineurs. Studies including groups of non-selected patients may therefore fail to detect seasonal variation of migraine.
We studied seasonal variation of migraine headache in a population of women living north of the Arctic Circle and the impact of migraine attacks induced by sunlight on the distribution of migraine attacks throughout the year. We also evaluated associations between migraine attacks and barometric pressure, temperature, and humidity. Finally, we studied seasonal variation of migraine in a subgroup of migraineurs experiencing light-sensitive migraine more regularly.
Methods
Patients
The study population was part of a larger population described previously (7,8). Forty female migraineours, living between 68° and 71° north, recorded in detail every migraine attack experienced from 23 March 2004 throughout 12 months; i.e. equivalent to the equinox. They were all interviewed by experienced neurologists (KBA, SB), given a lifetime diagnosis according to the ICHD-2 criteria (9), and they were all healthy except for their migraine. Patients who were not able to distinguish between migraine and other types of headache were excluded. A complete list of inclusion criteria are described elsewhere (7). Based on their diary recordings patients were reclassified according to their predominant active migraine; those with aura in ≥50% of the attacks were classified as migraine with aura (MA), and the others as migraine without aura (MO).
Data collection
From the diary, frequency of aura prior to migraine attacks, character of the headache (‘throbbing’, ‘pressing’, or ‘other’), intensity of pain on a visual analogue scale from 0–10, additional symptoms (nausea, photophobia, etc.), use of medication, the effect of the treatment, and reduced period of sleep during the night before onset of migraine were recorded. We used HIT-6 to assess the impact of migraine headache (10). Attacks triggered by the sun, as self-defined by the patients, were classified as light-induced attacks (LIA). In the subgroup-analyses, we defined patients as having sun-induced migraine (SIM) when they reported ≥10% frequency of LIAs. When attacks occurred on day 1 ± 2 relative to onset of menstruation, attacks were classified as menstruation-related (MRM) (9). In general, migraine attacks were defined and counted as new only when they were separated from previous attacks by at least a 24-hour pain free interval (11). Meterological data were provided through a public meteorological database (12) with assistance from Tromsø weather station (70° N). Due to a widespread population, and local variations in weather, only patients living within 1.5° latitude distance from the weather station, i.e. between 68° and 71° north with reliable data, were included from the original study (8). This compromise was decided after discussions with meteorologists working at the weather station, which is the only one in North Norway providing a complete meteorological data set.
Statistical analysis
Data were analysed with SPSS software (version 12.0 for Windows). The statistical analyses and evaluation of the reliability of the patient’s diaries were performed by professional statisticians (KH, FG). Descriptive data are presented as mean and standard deviation (SD). Most of the data were ordinal and categorical. To compare frequencies, χ2 test were performed. Independent t-test was used for comparison of means between the groups.
A change in weather conditions, from the day before an attack to the day with the onset of the attack (Δ), and meteorological observations on the day the migraine attacks started were used in the statistical model. A gliding average of the number of migraine attacks per day was used for comparison of SIM (red curves) and non-SIM (blue curves) in any interval throughout the year. The summed value is 1 for both red and blue curves respectively. In the subgroup analyses of migraineurs reporting ≥10% LIA, the periods between 23 September and 22 March (winter) was compared with the period between 23 March and 22 September (summer). For a better visualization of the data, we presented a 31-day average centered on each day in the period. The level of significance was set at 5%.
Ethics
The regional ethical committee of Northern Norway reviewed the protocol and approved the protocol.
Results
Baseline characteristics in women with sun-induced migraine (SIM) and non-SIM attacks
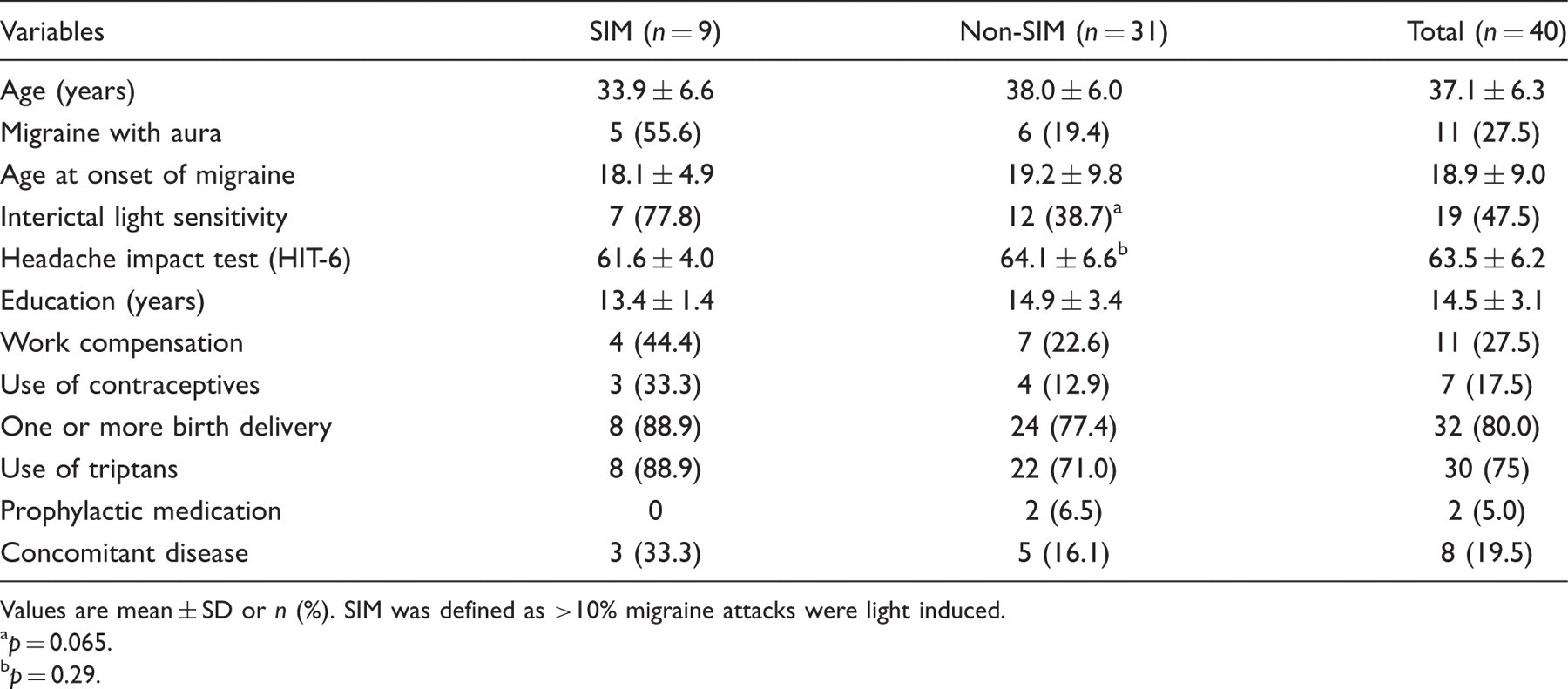
Values are mean ± SD or n (%). SIM was defined as >10% migraine attacks were light induced. a p = 0.065. b p = 0.29.
Migraine characteristics in women with sun-induced migraine (SIM) and non-SIM attacks
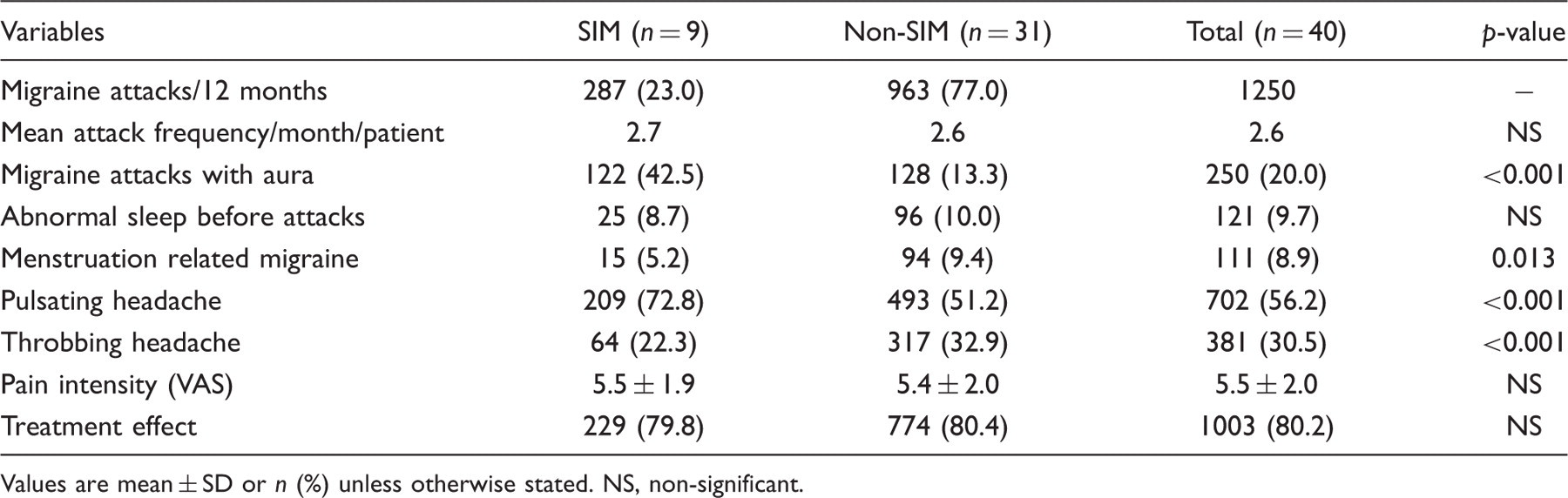
Values are mean ± SD or n (%) unless otherwise stated. NS, non-significant.
Figure 1 shows a cumulative distribution of migraine attacks during 12 months (blue line). LIAs decreased towards the beginning of the arctic dark season and increased again at the end of the period (red line, Figure 1). As expected, almost no LIAs were registered in the dark season (November−January) (Figure 1). The last LIA was registered on 18 November while LIA appeared the next year at 8 January for the first time. Both sleep-deprivation attacks and MRM attacks were equally distributed throughout the year; i.e. by removing MRM or sleep-related attacks and finally removing both variables from the statistical model, the curve reflecting average number of attacks remained similar but at a lower level (Figure 2). In the LIA group, the patients reported 25 sleep-deprivation migraine attacks; 25/298 = 8.4% compared to 99/1001 attacks in the non-LIA-group (9.9%, not statistically significant). No evidence of the confounding effect of MRM or sleep-related migraine attacks was detected.
Cumulative distribution of light-induced migraine attacks (LIA) and total migraine attacks in 40 women with migraine living between 68° and 71° north. Moving average of daily number of migraine attacks with a 31-day window of all migraine attacks and all migraine attacks minus those which are reported to be caused by either lack of sleep or menstruation.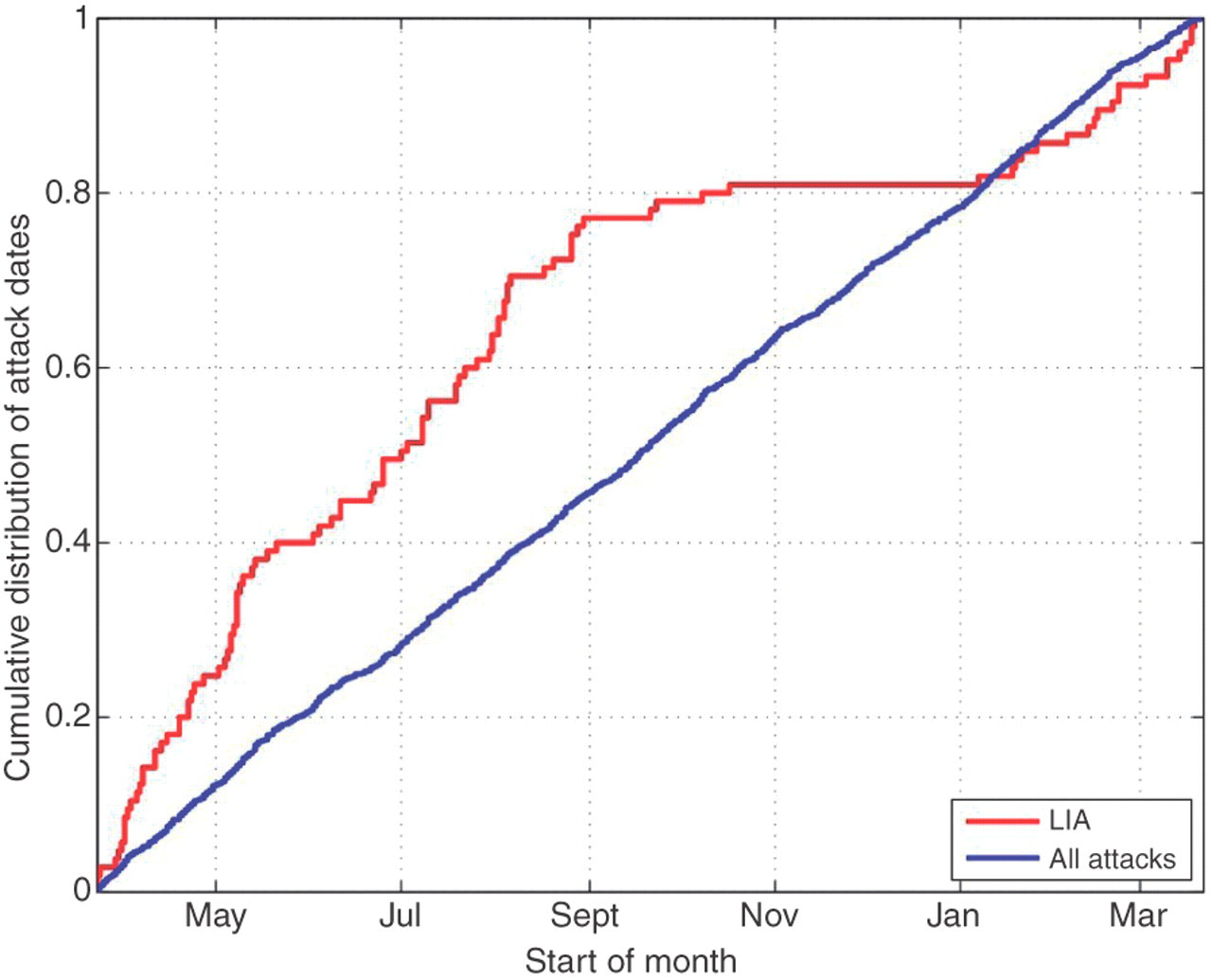

Association between self-reported sun-induced migraine attacks and number of hours with sun on the day of migraine onset (attacks in the ‘dark season’ are excluded)

LIA, light-induced migraine attacks.
The nine patients with SIM recorded 287 migraine attacks, of those 77 (26.8%) were sun-induced. These patients had significant more migraine attacks in the summer (163 attacks) compared to the winter (124 attacks, p = 0.04). The difference in distribution of migraine attacks in SIM and non-SIM throughout the year is shown in Figure 3. The mean number of migraine attacks was 31.3 (1250/40) while mean number of attacks in those with SIM was 31.9 (287/9; not significantly different). Also, the total number of migraine attacks was not significantly different in the periods with complete darkness and periods with midnight sun (SIM: 44 attacks in dark season vs. 40 attacks in the midnight summer period corresponding to non-SIM: 157 attacks in dark season and 174 in the arctic light season).
Normalized moving average of daily number of migraine attacks with a 31-day window of all migraine attacks in the sun-induced migraine (SIM) group and all migraine attacks in the non-SIM group. The SIM group had significantly more migraine attacks in the summer compared to the winter (p = 0.04).
The subjects with SIM had more often aura and reported presence of interictal light-hypersensitivity in the majority of the cases and were typically of pulsating character (Tables 1 and 2). In the SIM group, 5.2% of the attacks were related to menstruation and 9.4% in the non-SIM group (p = 0.013; Table 2). The proportion of MRM attacks in SIM attacks was 7.14 (total SIM minus 77 LIA = 15/(287–77)). The corresponding result for non-SIM was 10.05 (total non-SIM minus 28 LIA = 94/(963–28); p = 0.09). No linear correlation was found between any weather variations, neither registrations performed the day of migraine onset nor the previous day, and number of migraine attacks.
Discussion
We aimed to study the impact of exposure to external light on migraine for the following reasons: (i) we have previously reported increased frequency of migraine attacks in the arctic summer season (6–8), but the variation diminished after correction for insomnia (13); (ii) the huge variation of weather conditions provide a good opportunity for chronobiological studies in conditions like migraine; and (iii) a possible variation of migraine attacks dependent on sun exposure may guide to better prophylactic studies and hopefully, improving treatment for the patients.
We could not demonstrate any seasonal variation of migraine by analysing the total number of migraine attacks in 40 women living within a defined area from a weather station in North Norway who reported 1250 migraine attacks thoroughly in a 12-month diary. However, in the subgroup analysis in a limited number of patients reporting sun or reflection from the sun as a trigger for migraine attacks regularly (≥10% of the attacks), significantly more migraine attacks in the summer compared to the winter were observed. These attacks were more often precipitated by aura, less frequently related to menstruation, and usually of pulsating character. The majority of these patients with sun-induced migraine reported interictal light sensitivity to be a problem, although not significantly, possibly due to a limited sample size.
The role of weather as trigger factor for migraine is difficult to interpret from the literature. Among several factors, exposure to sunlight was a consistent migraine trigger in a recent report (3). Frequency of weather as a trigger for migraine attacks was found in more than half of the patients in retrospective analyses from an American headache centre (2). In contrast, 91% of 200 migraine patients visiting a clinic reported some kind of migraine trigger, but weather was not listed among expected trigger factors (14). Decreased temperature and humidity (15), lower barometric pressure, and sunshine >3 hours (16) are some reported associations between meteorological parameters and migraine attacks. Self-reported data may overestimate the influence of weather on migraine headache and may be one explanation for the divergence in the ‘weather studies’ (17). In a recent prospective cohort of 238 patients fulfilling a 90-day diary, no associations between weather parameters and migraine attacks were detected after controlling for multiple statistical analyses (18). This finding corresponds well to the overall findings from our population. No previous studies have tried to identify subgroups of migraineurs with increased sensitivity to sun exposure or other weather variables. Although, the present study was not primarily designed for evaluating sensitivity for trigger factors in certain predisposed individuals, previous studies also indicate that such research should be completed (6–8). It is an interesting finding that a limited number of patients with a certain degree of light-induced migraine attacks seem to have seasonal variation of migraine with significantly less frequent attacks in the winter compared to the summer (Figure 3). Another finding that may question treatment strategies is that the increased proportion of LIAs was associated with number of hours with sun in the same geographical area (Table 3). A well-designed prophylactic study selecting patients with frequent LIAs performed in the summer period should be considered.
Sleep insufficiency is an important variable to control for in studies of migraine variation. We have previously shown that insomnia may explain seasonal variation of migraine, especially in migraineurs with aura (13). In this material, migraine attacks occurring the day after a reduced amount of sleep did not change the circannual distribution of migraine. Similarly to MRM attacks, the sleep-related attacks were not confined to any period of the year, and are therefore less likely being confounders.
Strength and shortcomings of the study
Controlling for important confounding variables such as MRM and sleep deprivation, a thorough review of all patient diaries performed by professional statisticians excluding those with incomplete data and recruiting patients from the general population via newspaper announcement providing a representative group of patients are the main advantages of the study.
Lack of coordinated registrations of migraine onset and weather variables may provide some uncertainty to the results. Another drawback is lack of information about patient location at onset of migraine attacks. An obvious limitation to the study is the small sample, especially in the subgroup analyses. The results should therefore be interpretated cautiously and mainly be used as hypothesis for future studies. A possible confounding effect by use of prophylactic drugs in two of the non-SIM patients cannot be excluded. Finally, we cannot exclude the risk of overestimating headache episodes by the patients, although participation in the study required that they were able to separate migraine headache from other headaches.
In conclusion, sun exposure may be regarded as an important precipitating factor in some migraineurs. The role of other weather phenomena as trigger factors is dubious.
Footnotes
Acknowledgement
We thank the meteorologist Stein-Erik Øines for professional advice in defining the geographical cut-off and for assisting us in providing correct weather variables for the study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.