
Abstract
Background: It is not known why some patients with underlying chronic nociceptive sources in the neck develop cervicogenic headache (CEH) and why others do not. This quantitative sensory testing (QST) study systematically explores the differences in sensory pain processing in 17 CEH patients with underlying chronic cervical zygapophysial joint pain compared to 10 patients with chronic cervical zygapophysial joint pain but without CEH.
Methods: The QST protocol comprises pressure pain threshold testing, thermal detection threshold testing, electrical pain threshold testing and measurement of descending inhibitory modulation using the conditioned pain modulation (CPM) paradigm.
Results: The main difference between patients with or without CEH was the lateralization of pressure hyperalgesia to the painful side of the head of CEH patients, accompanied by cold as well as warm relative hyperesthesia on the painful side of the head and neck.
Discussion: From this hypothesis-generating study, our results suggest that rostral neuraxial spread of central sensitization, probably to the trigeminal spinal nucleus, plays a major role in the development of CEH.
Keywords
Introduction
Cervicogenic headache (CEH) is pain referred to the head from a source in the cervical spine. Both laboratory and clinical studies have shown that pain from the upper cervical zygapophysial joints and muscles can be referred to the head and face by means of convergence at the trigeminocervical nucleus (1,2). The prevalence of CEH has been estimated at up to 4.1% in the general population and as high as 17.5% among patients with severe headaches. The prevalence is as high as 53% in patients with headache after whiplash (3–5). Currently, no drugs are effective for CEH (1,6,7). Manual therapy was shown in a randomized controlled study to be no more effective than exercise alone (8).
Localized pressure hyperalgesia and bilateral thermal hypoesthesia in the head and face have been observed in patients with CEH when compared to healthy volunteers (9–11). Even when CEH patients were compared to patients with other forms of primary headaches like migraine without aura and tension-type headaches, these differences were still found to be significant (9,10). The pattern of sensory processing in the head in chronic neck pain patients is considered to be a result of pain transmission via the functional interaction of the pars nucleus caudalis of the trigeminal nerve and the upper cervical spinal cord (12,13). This is believed to allow the bidirectional transmission and processing of pain signals between the neck and the trigeminal sensory receptive fields of the face and head (13–19).
In this hypothesis-generating cross-sectional study, we aim to evaluate the differences in sensory pattern in CEH patients with underlying chronic cervical zygapophysial joint pain compared to patients with chronic cervical zygapophysial joint pain without CEH. A multi-modal quantitative sensory testing (QST) measurement battery comprising pressure pain thresholds, thermal detection thresholds, electrical pain detection thresholds, and conditioned pain modulation response (20) testing was used to evaluate the sensory processing in the head and neck.
Methods
Subjects
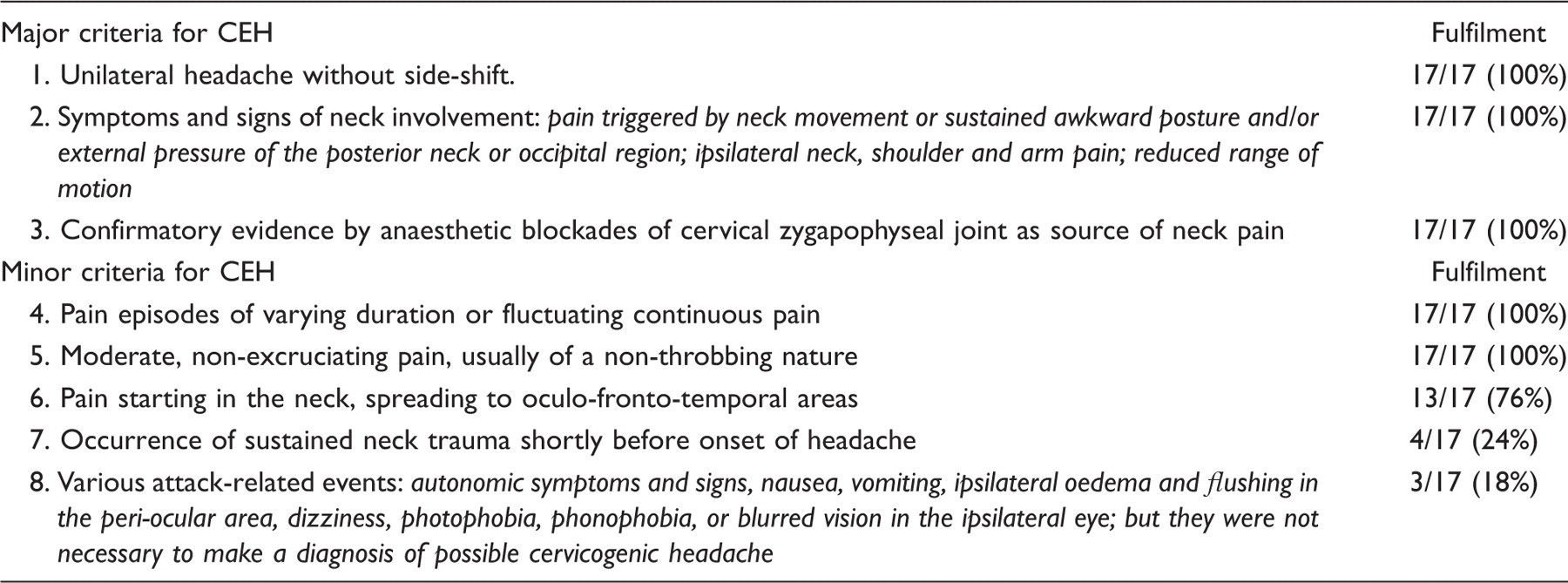
The study was designed as a prospective cross-sectional study. Participants were recruited from a single multidisciplinary pain centre in the Netherlands, between July 2009 and June 2010. Institutional ethics approval for this study was granted by the Central Commission for Human Research for Nijmegen and Arnhem, the Netherlands. Patients aged 18 years or more with chronic neck pain lasting at least 6 months were eligible for inclusion. After informed consent, the patients were screened using a standardized questionnaire and were examined by a pain specialist with special interest in head and neck pain. The recruiting pain specialist had no role in the design of the study, data collection or analysis of the results. Patients with signs and symptoms of cervical zygapophysial joint pain were eligible for inclusion. All patients underwent controlled, comparative diagnostic blocks to confirm the cervical zygapophysial joint pain source (1,21) as described in subsequent paragraphs. Inclusion criteria for the CEH group required fulfilment of all the major criteria from Sjaastad et al. (22) (Table 1). Those with only neck pain and no headache complaints formed the non-CEH group. Exclusion criteria for the study included uncontrolled major depression or serious psychiatric disorders, use of anticoagulant drugs (except low-dose aspirin), pregnancy, acute or uncontrolled medical illness, malignancy or poorly controlled epilepsy, fibromyalgia or painful syndromes associated with diffuse pains, recent history of opioid usage, chronic alcoholism or substance abuse. The procedural workflow is represented in Figure 1.
Patient procedural flow throughout study. CEH, cervicogenic headache. Adapted from the original Sjastaad’s criteria [22]
Procedures
After inclusion, each patient underwent QST measurement. Each QST session lasted for an average of 65 ± 15 minutes. All the tests were conducted by medical personnel certified to perform QST measurements. The QST measurements were performed prior to the diagnostic blocks.
Quantitative sensory tests
The aim of our study was to observe as many aspects of pain processing as possible, while retaining feasibility within the constraints of clinical practice. Our comprehensive QST battery hence consisted of:
Static sensory tests of pain processing for different stimulus modalities [such as pressure pain threshold (PPT) testing, thermal threshold testing and electrical pain threshold (EPT) testing], to demonstrate central sensitization or tonic inhibition. Dynamic testing of descending pain modulation [conditioned pain modulation (CPM) paradigm (5) to test for induction of diffuse noxious inhibitory control (DNIC), a phasic form of descending pain modulation (4)]. Testing of thermal skin sensitivity (cold and warm sensation thresholds) to detect negative or positive sensory signs usually associated with nerve damage or altered central sensory processing (23). Multi-modal quantitative sensory testing (QST) battery. The tests were performed in a clockwise order beginning with pressure algometry. CZJ*, cervical zygapophysial joint; SCM, superior insertion of sternocleidomastoid; GON, greater occipital nerve; TEM, mid-temporal muscle; V1*, ophthalmic division of the trigeminal nerve distribution; WUR, wind-up ratio; CPM, conditioned pain modulation; VAS, visual analogue scale; EPTT, electrical pain tolerance testing. * denotes sites tested with electrical and thermal measurements.
The test sites were measured in a standardized fashion beginning with the non-painful side. The measurement sites are shown in Figure 2 and were chosen to correspond to the most painful sites in the head and face in patients with CEH in previous studies (10,26). The reference site (C, pain-free reference area in the thigh) is as per our institutional QST protocol. PPTs were measured over all five sites and the reference site (C). Thermal detection thresholds and EPTs were measured over sites CZJ, V1 and C.

Pressure pain threshold (PPT) test
PPTs were determined using an algometer (Somedic Production AB, Farsta, Sweden) with a probe area of 1 cm2 that exerts pressure up to a maximum of 2000 kPa. The PPT was determined using ascending stimulus intensities, applied as a slowly increasing ramp of 50 kPa/s.
Thermal detection threshold test
Cold and warm detection thresholds were measured (CDT, WDT) and the mean threshold temperature of three consecutive measurements calculated. All thresholds were obtained with ramped stimuli (1°C/s) that were terminated when the subject pressed a button. The baseline temperature was set at 32°C and the ramp back to baseline was 1°C/s. The contact area of the thermode was 9.0 cm2 and cut-off temperatures were pre-set at −10 and 50°C.
Electrical pain threshold (EPT) test
Each electrical stimulus consisted of tetanic stimulation at 100 Hz (0.2 ms square wave pulses), delivered via two monopolar electrodes with a surface area of 0.3 cm2, 2 cm apart. EPTs were measured in three ascending series with ramping rate of 0.7 mA/s (24). The intensity of stimulation was limited to 50 mA.
Conditioned pain modulation (CPM) response
The test stimulus for the CPM (20) testing was applied on the anterior aspect of the right thigh in the L2 dermatome as well as over the V1 area of the non-painful side (23). Electrical pain tolerance thresholds (EPTTs) were first measured on the anterior aspect of the thigh (C) as well as over the V1 area. The conditioning stimulus was insertion of the dominant hand into an ice-water bucket. The hand was left immersed until a VAS of 80 mm was reached, or until a cut-off time of 180 s (whichever came first). A repeat of the EPT at C and V1 were measured immediately upon hand removal. The CPM response was calculated according to the following formula:
CPM = {(EPTTpost − EPTTpre)/EPTTpre}*100
Controlled comparative diagnostic blocks
Controlled cervical zygapophysial joint medial branch blocks are an established method to diagnose cervical zygapophysial joint pain using two different local anaesthetic agents with different durations of action (21,25–27). All diagnostic blocks were performed under fluoroscopy. Localization of each medial branch was confirmed by sensory stimulation at 50 Hz below 0.5 V and motor stimulation at 2 Hz below 1 V. After localization, 0.5 ml of either 1.0% lignocaine or 0.5% bupivacaine was deposited. The order of the agents was not controlled. The first diagnostic block was performed on the same day as the QST measurement. The second diagnostic block was performed 1–2 weeks later. A positive diagnostic block is defined as pain relief lasting at least 2 hours when lidocaine was used; at least 3 hours when bupivacaine was used, or greater than the duration of relief with lidocaine; and an intensity of relief of 80% or more in the neck.
Statistics
Sample means and standard deviations were applied to continuous baseline characteristics data. Frequency counts were used to summarize categorical data. The normal distribution of samples was tested by the degree of skewness and kurtosis for all baseline characteristics and measured parameters, and subsequently screened using the independent t-test. We randomly selected 27 age- and gender-matched control patients for our healthy control values from our database containing reference values of 118 pain-free healthy volunteers.
A univariate screening analysis was first performed using the independent t-test to compare the reference areas of both groups with healthy control values. The paired t-test was used to compare measurements over the pain-free reference areas as well as CPM measurements over V1 and the pain-free reference area (C) within each group. We compared sides for CDT, WDT and EPT measurements in the neck and face between and within the groups using a paired or unpaired t-test as appropriate. We do not report comparisons between different neck and face sites as no normal values are available for these. When using the independent t-test, equal variances were assumed only when p > 0.05 in Levene’s test for quality of variances. As this was a hypothesis-generating study, we did not perform formal corrections for multiple testing.
Due to the multiple measurements sites compared, multivariate testing using the general linear model was performed for PPT in the head and neck of the CEH and the non-CEH groups. Post hoc analysis (Tukey’s HSD) was applied to interactions that were statistically significant. All statistics were performed using the statistical packages Statistica for Windows (version 7.0; Statsoft Inc., Tulsa, OK, USA). Significance level was set at p < 0.05.
Results
Subjects
Baseline characteristics of patients in the CEH group compared to patients in the non-CEH group

CEH, cervicogenic headache; NRS, numeric rating score; SD, standard deviation.
Mean (± SD) pressure pain thresholds (PPT) in the CEH and non-CEH groups

NP, non-painful; P, painful; PPT, pressure pain threshold; C, Sites of measurement: C, pain-free reference area in the thigh; CZJ, C4/5 zygapophysial joint; SCM, superior insertion of sternocleidomastoid; GON, greater occipital nerve; TEM, mid-temporalis muscle; V1, ophthalmic division of the trigeminal nerve.
Pressure pain thresholds
Reference area (C)
Mean (± SD) of the QST measurements over the pain-free reference areas (C) in the CEH group, the non-CEH group and with healthy control values

(*), randomly selected age- and gender-matched pain-free controls from our database (n = 27). NP, non-painful; P, painful; NS, not significant; PPT, pressure pain threshold; CDT, cold detection threshold; WDT, warm detection threshold; EPT, electrical pain threshold; CPM, conditioned pain modulation (CPM values of both C and V1 are included here).
Head and neck sites
Site effect was significant when the CEH group and the non-CEH group were compared (F = 5.63, p < 0.001). The following interactions were significant: side-group (F = 17.39, p < 0.001) and side-site-group (F = 3.18, p = 0.017). This is represented in Figure 3.
Pressure pain thresholds (PPTs) comparing both sides in the CEH group versus the non-CEH group. CZJ, cervical zygapophysial joint; SCM, superior insertion of sternocleidomastoid; GON, greater occipital nerve; TEM, mid-temporal muscle; V1, ophthalmic division of the trigeminal nerve distribution.
For the side-group interaction, post hoc analysis showed: (i) no significant difference between sides of the CEH compared to the non-CEH group; (ii) no significant difference between sides within the non-CEH group; and (iii) lower PPT in the painful side compared to the non-painful side in the CEH group (p = 0.004).
For the side-site-group interaction, post hoc analysis showed: (i) no significant differences between the CEH and the non-CEH group; (ii) no significant side-to-side differences within the non-CEH group; (iii) a significant side-to-side difference between CZJ and GON PPTs, which were lower for the painful vs non-painful side within the CEH group.
In summary, pertinent PPT findings include pressure hypoalgesia of the pain-free reference areas of both groups compared to healthy control values; lateralization of pressure hyperalgesia to the painful side for CZJ and GON in the CEH group.
Cold detection thresholds (CDTs)
Reference area
There was no significant difference in the CDT over the pain-free reference area (C) between both groups. In the CEH group, CDT was significantly higher in C (28.1°C) on the painful side compared to the non-painful side (24.0°C, p = 0.001) (Table 4).
Head and neck sites
As shown in Figure 4, CDT in V1 on the painful side was significantly higher in the CEH group when compared to the non-CEH group (t = 2.61, p = 0.015) (Table 5).
Cold detection thresholds (CDTs) comparing both sides in the CEH group versus the non-CEH group. CZJ, cervical zygapophysial joint; V1, ophthalmic division of the trigeminal nerve distribution. *p < 0.05 between groups; †p < 0.05, side-side comparison within group; ‡p < 0.05, site-site comparison between groups. Mean (± SD) thermal and electrical QST parameters comparing CEH group versus non-CEH group NP, non-painful; P, painful; PPT, pressure pain threshold; CDT, cold detection threshold; WDT, warm detection threshold; EPT, electrical pain threshold. Sites of measurements (C, pain-free reference area in the thigh; CZJ, C4/5 zygapophysial joint; SCM, superior insertion of sternocleidomastoid; GON, greater occipital nerve; TEM, mid-temporalis muscle; V1, ophthalmic division of the trigeminal nerve).

Within the CEH group, CDT over the CZJ on the painful side was found to be higher compared to the non-painful side (t = −3.45, p = 0.003). These changes were not observed in the non-CEH group.
In summary, relative cold hyperesthesia was detected over V1 on the painful side in the CEH group in comparison to the non-CEH group. Within the CEH group, relative cold hyperesthesia was detected over CZJ on the painful side.
Warm detection thresholds (WDTs)
As shown in Figure 5, WDT in V1 on the painful side was significantly lower in the CEH group when compared to the non-CEH group (t = −2.12, p = 0.044) (Table 5). There were no significant WDT differences detected both between and within groups over the pain-free reference area (C) and the neck (Tables 4 and 5).
Warm detection thresholds (WDTs) comparing both sides in the CEH group versus the non-CEH group. CZJ, cervical zygapophysial joint; V1, ophthalmic division of the trigeminal nerve distribution. *p < 0.05 between groups.
In summary, relative warm hyperesthesia was detected over V1 on the painful side in the CEH group in comparison to the non-CEH group.
Electrical pain thresholds (EPTs)
There were no significant EPT differences detected both between and within groups over the pain-free reference area (C) (Table 4).
Group comparisons showed no significant differences when sides were compared (Table 5).
No significant side-to-side differences were detected within the CEH or the non-CEH group
In summary, no side-to-side differences in electrical hyperalgesia were detected in either group of patients.
Conditioned pain modulation (CDM) response
The CPM response over the pain-free reference area (C) was not significantly different when either group was compared to healthy control values. Also, no differences were detected between groups when CPM in V1 and C were compared. However, within the CEH group, a lower CPM in V1 showed a trend towards significance (p = 0.062) when compared to the CPM response in C (Table 4).
In summary, the lower CPM in V1 compared to C in the CEH group approached significance and may indicate an antagonism of the phasic pain inhibitory response in the face in this group of patients.
Discussion
Findings
This is the first study to systematically evaluate chronic cervical zygapophysial joint pain patients with or without CEH using a multi-modal QST battery. Our findings suggest that the main difference between these patients with and without CEH is the lateralization of pressure hyperalgesia to the painful side of the head and neck. This lateralization of sensitization is accompanied by cold as well as warm relative hyperesthesia on the painful side of the face in patients with CEH. The marked generalized pressure hypoalgesia detected over the non-painful reference areas suggests ongoing descending tonic inhibition in both patient groups. From this hypothesis-generating study, our results suggest that rostral neuraxial spread of central sensitization, probably to the trigeminal spinal nucleus, plays a major role in the development of CEH.
In our endeavours to further elucidate the mechanisms underlying development of CEH, patients with cervical zygapophysial joint pain complicated by CEH were compared to those with only cervical zygapophysial joint pain. Our findings revealed lateralization of pressure hyperalgesia accompanied by distinct cold and warm relative hyperesthesia on the painful side of the face in the CEH group compared to the non-CEH group. This suggests an ongoing central sensitization process in the pathophysiological development of CEH, with hyperalgesia at C2 spinal segment and trigeminal spinal nucleus being interpreted as a sign of rostral neuraxial spread of central sensitization (2).
All current clinical diagnostic criteria describe CEH as a unilateral headache that is side-locked. We describe a unilateral pattern of pressure hyperalgesia in the head and neck that typifies the altered sensory processing in patients with CEH, corresponding to the most painful sites in the head and neck in patients with CEH (10,28). Thus we suggest that pressure algometry may allow objective measure of the degree of lateralization and, more importantly, allows for monitoring of the effect of disease progression and treatment.
Generalized hypoalgesia in a distal unaffected site had been suggested to reflect descending tonic inhibitory modulation (23,29,30), akin to generalized hyperalgesia indicating supraspinal central sensitization (31). This is consistent with the finding that CPM was found to be intact in both the CEH and the non-CEH groups. This indicates that an impairment of descending inhibitory modulation is unlikely to be the mechanism behind the development of CEH. Our findings suggest that rostral spread of central sensitization, e.g. trigeminal sensitization, plays a major role in the development of CEH. In the CEH group, it was interesting to note that the CPM in the trigeminal sensory system did display a trend towards being less effective when compared to the spinal system. Descending inhibitory mechanisms and central sensitization counteract or antagonize each other (32) and our findings probably reflect the physiological antagonism between descending control and central sensitization.
Comparison with literature/available evidence
We have found no studies to date comparing patterns of sensory processing in cervical zygapophysial joint pain in patients with or without CEH. Bovim et al. (10) demonstrated pressure hyperalgesia over cephalic sites in patients with CEH compared to healthy controls and also compared to patients with migraine and tension-type headaches. There were no differences in the PPTs in migraine and tension-type headache compared to healthy controls. Becser et al. (9) compared patients with CEH (n = 20), patients with migraine (n = 17) and healthy volunteers (n = 56) at five cephalic sites and two distal sites in the hand. Bilateral thermal (both cold and warm) hypoesthesia was detected in the frontal, maxillar and mastoid regions as well as in the hands when compared to the healthy volunteers (9).
In comparison to patients with chronic neck pain only, our study, which did not measure neck pain thresholds in healthy volunteers, found unilateral pressure hyperalgesia accompanied by relative thermal hyperesthesia on the painful side in chronic neck pain patients with CEH. The detection of these sensory processing differences was possible only because we compared patients with the same underlying pathology, with and without the complication of CEH (33).
Both groups of patients in our study were in a state of tonic inhibition. In a previous study, Sandrini et al. (34) demonstrated a lack of CPM response in subjects with migraine and tension-type headache, supporting the possibility of impaired pain modulation. This does not appear to be the main mechanism responsible for the development of CEH. The main mechanism from this study is trigeminal sensitization, which antagonizes the effects of descending control. This may explain the lower CPM response in the face compared to the control area in patients with CEH.
Clinical implications
Our findings strongly suggest that the rostral spread of central sensitization is related to the progression of the disease. In this context, QST may not only permit diagnosis and monitoring of rostral spread of central sensitization, it may also allow assessment of the degree of lateralization of sensitization (not pain). If confirmed, we suggest that such measures could in future provide the basis for monitoring disease progression and treatment effects.
Traditionally, the focus of CEH treatment has concentrated on the alleged nociceptive sources in the neck. Such treatments range from conservative programmes with neck exercises with or without manual therapy (8), to minimally invasive interventions such as radiofrequency neurotomy of the upper cervical zygapophysial joints (1), to surgical options such as anterior cervical fusion (35). Detailed discussion of this type of treatment is beyond the scope of this study. Although speculative at this moment, the addition of centrally acting medications that target central sensitization to existing treatment regimes might reduce the intensity or even the rostral spread of central sensitization.
Conclusion
The present study provides evidence for the first time indicating rostral and trigeminal central sensitization as a likely developmental mechanism in chronic cervical zygapophysial joint pain patients with CEH. This insight may be important as it suggests that the treatment of CEH should focus not only on the nociceptive sources in the neck, but also on the central nervous system sensitization spreading to the level of the trigeminal spinal nucleus.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of Conflicting Interests
None.