
Abstract
Introduction: Benign paroxysmal vertigo (BPV) is characterized by recurrent attacks of dizziness in a healthy child. Complete recovery typically takes place during childhood, and an epidemiological link with migraine has been pointed out. Nevertheless, data concerning long-term patient outcome are scarce.
Subjects and methods: We analyzed the clinical data of 17 patients diagnosed with BPV between 1991 and 2008 in our neuropediatric department; we particularly focused on family medical history and long-term patient outcome by reviewing their medical files and by interviewing the families with a standardized questionnaire administered by phone.
Results: Thirteen families responded to the questionnaire, performed 1.1 to 24.5 years after onset. Among 10 patients older than 11 years of age, five continue to suffer attacks of vertigo. Median age at recovery was six years. Nine subjects exhibited migraine, including all six aged 15 years or older. There was a first-degree history of migraine in eight out of 13 children.
Conclusion: BPV may not be a homogeneous condition, as some children have a poorer prognosis than others. The strong link with migraine, already noticed by previous authors, led us to discuss the pathophysiology of this condition.
Introduction
A complaint of vertigo is unusual among children. Benign paroxysmal vertigo (BPV) was first described in the 1960s and is characterized by recurrent attacks of dizziness, with onset between two and five years of age—often accompanied by neurovegetative signs and ataxia—in otherwise healthy children. Results of clinical and paraclinical investigations remain negative (1–3).
So far, only small series of patients have been reported (4–10). Although a higher incidence of behavioral or emotional symptoms in childhood BPV has recently been suggested (11), there is a lack of data about the long-term outcomes of these children, even if this affliction is classically considered to be “benign” with a complete recovery during childhood (7–9).
The physiopathology of this disorder is a matter of debate. Some authors have pointed out an epidemiological link with migraine (4,6,12), leading the International Headache Society (IHS) to include this entity in its first International Classification of Headache Disorders under the chapter “Childhood periodic syndromes that are commonly precursors of migraine” (1.3.3), without modification in the second edition of the classification (13). In this retrospective study, we describe a group of 17 patients with BPV and report their long-term outcomes. Our series of patients led us to discuss the pathology of BPV of childhood.
Subjects and methods
International Headache Society criteria for Benign Paroxysmal Vertigo (13)

All of these patients had been examined by an experienced child neurologist. Electroencephalogram, audio-vestibular investigation and brain imaging were normal for all of our patients.
We collected data from the medical files concerning the clinical characteristics of attacks: age of onset, triggering factors, duration, frequency and associated neurovegetative signs (photophobia, nausea, vomiting). Data concerning the past medical history and the psychomotor development of the patients were also collected.
Each family was then contacted by telephone and the parents were interviewed using a standardized questionnaire. This questionnaire was designed to assess patient follow-up, specific to the age at last episode; persistence or improvement of the attacks; occurrence of migraine using IHS criteria (type of migraine, frequency); occurrence of other types of periodic phenomena, such as benign paroxysmal torticollis (BPT), abdominal migraine and cyclical vomiting; and the occurrence of any other relevant co-morbidity. The questionnaire also focused on family history, especially in terms of the occurrence of migraine and other neurological paroxysmal manifestations.
Results
Clinical features of our patients
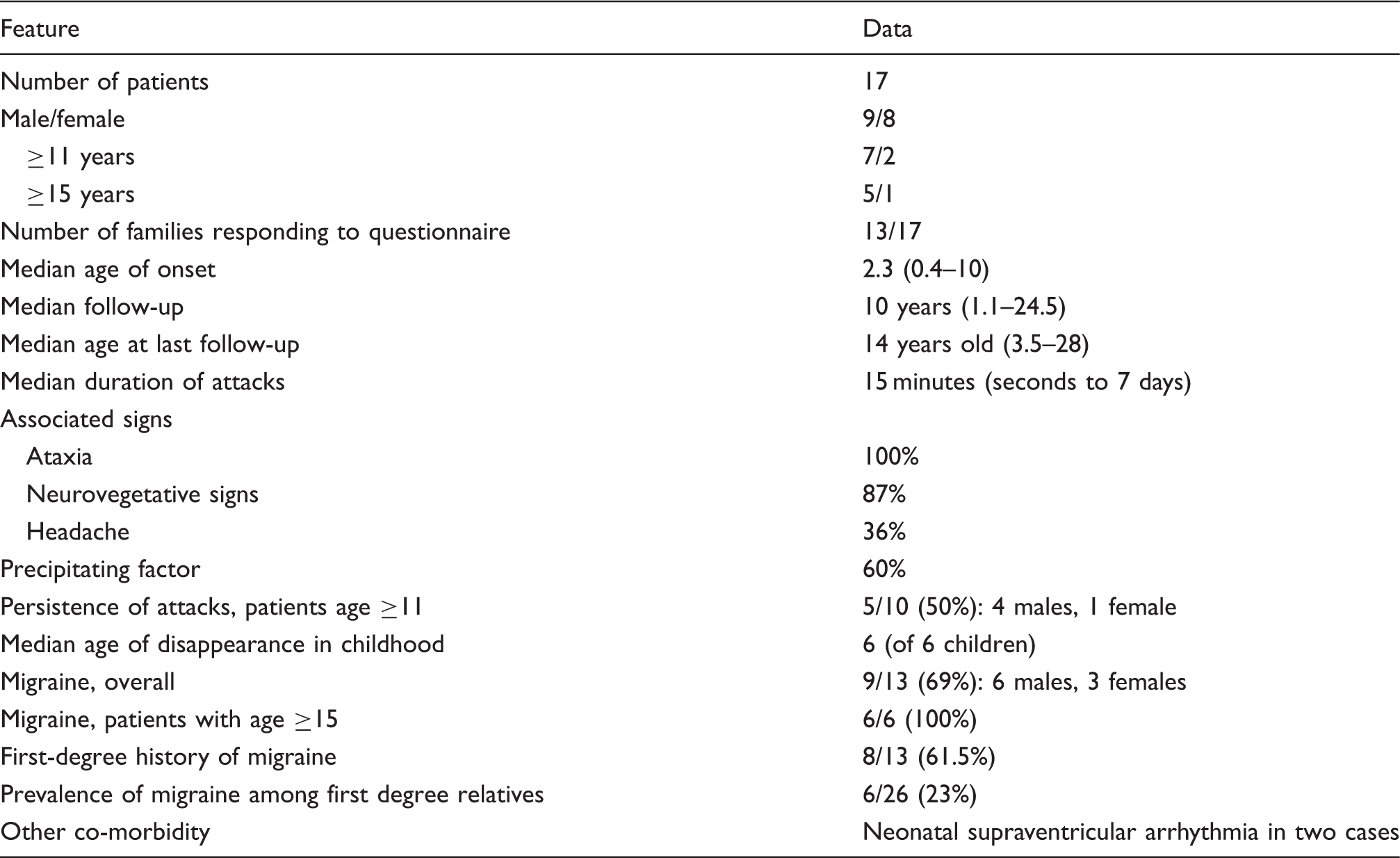
Seventeen patients were included in this study, nine boys and eight girls. Thirteen families were contacted by phone. They all agreed to participate in the study. Four families were lost to follow-up.
The median age of the patients at the time of the study was 14 years (3.5–28) and median time period since the first attack was 10 years (1.1–24.5). Median age at first attack was 2.3 years (0.4–10). The onset of attacks was always abrupt. Their duration varied between seconds to several days (up to seven), with a median of 15 minutes. The more frequent signs associated with attacks were ataxia (100% of cases), neurovegetative signs (87%) and headache (36%). A triggering factor was found in 60% of cases. Psychological trauma, fever, a car trip and fatigue were the most commonly reported triggering factors.
Follow-up
Attacks had disappeared for more than two years in six of 13 children whose families were contacted. The median age of disappearance of attacks for these children was six years (2–12). Attacks became progressively less intense before complete disappearance in five of these six children.
Five of 10 children (50%) continued to suffer attacks after 11 years of age. For two of these children, the attacks relapsed during their teens, after an attack-free period of seven and 10 years, respectively. Furthermore, the severity and frequency of the episodes were notably increased in one patient after a prolonged free interval. Our oldest patient still exhibits attacks of vertigo at age 28.
Association with migraine
Among the 13 children whose families were contacted, nine reported recurrent headaches, including all six subjects older than 15 at the time of the study. Five of the nine cephalalgic patients fulfilled IHS criteria for migraine without aura, and four fulfilled the criteria of probable migraine without aura. None presented migraine with aura or tension-type headache. Four patients among the nine aged above 11 years suffer from both migraine and vertigo.
Two children developed paroxysmal manifestations concordant with “childhood periodic syndrome that is commonly precursor of migraine” (IHS classification): BPT for one child and abdominal migraine for the other child.
First-degree familial history of migraine was found in eight of 13 children: the mothers of seven patients and both parents of one patient. In most cases it was migraine without aura (four cases); otherwise, migraine with visual aura (two cases, including one father) or probable migraine without aura (two cases). Certain migraine was suffered by six of 26 first-degree relatives, resulting in a prevalence of 23% among this population.
Associated co-morbidity
Two children presented neonatal cardiac supraventricular arrhythmia. One girl was diagnosed with an atrial flutter, and a multifocal atrial tachycardia was diagnosed in a boy. Echocardiograms were normal in both cases. Amiodarone treatment resulted in a rapid and complete improvement.
Family history was otherwise unremarkable.
Discussion
We report a new series of children presenting with BPV. Despite its small size (comparable to those reported before), it provides new information because of (i) the 10-year follow-up of our patients and (ii) the systematic long-term reevaluation of personal and familial history of migraine. No other study has reported such a long follow-up period except for Lindskog’s (8), which reported on the 15-year outcome of a cohort of 19 children.
The clinical characteristics of the attacks in our group of patients are very similar to those previously reported: onset occurs during early childhood, vertigo is accompanied by ataxia and neurovegetative signs in nearly every case, headache is frequent during attacks and most often, a precipitating factor can be found (4,5,7,8,10).
Another interesting finding of our study is the wide range of attack duration, from a few seconds to seven days. The duration of attacks was quite consistent for a given child; nevertheless, two patients presented classical short-lasting attacks associated with recurrent attacks lasting two to seven days. One of these patients was free of attacks after age 12, whereas the other continues suffering episodes of vertigo at 11.
Persistence of the attacks in adolescence in 50% of cases is an important finding of our study. Although persistence until adulthood has been occasionally reported in the literature, a favorable outcome during childhood is commonly seen: total recovery in 80% of the 33 patients in Dunn’s study (10), and in all patients in Lindskog’s study (19 children) (8) and in Simoncelli’s (10 patients) (9). This difference can be partly explained by our long-term follow-up. Moreover, our study is the first to use IHS criteria to select patients; as previous studies did not use these criteria but rather various definitions for BPV, the selected groups of patients might differ. Our sample is too small to analyze the effect of gender upon persistence of attacks.
Nevertheless, our results do suggest that some children who fulfill IHS criteria for BPV do not have such a benign evolution. One may also hypothesize that two distinct groups of children suffering BPV might be delineated: a group with a neuro-developmental anomaly that recovers spontaneously, and a second group with a functional chronic neurological disease. Except for differences in long-term outcome, no other characteristic distinguishes these two groups. However, our sample is small. Furthermore, the possibility of a hormonal influence on the severity or recurrence of BPV attacks at puberty, similar to the well-known hormonal influence on migraine at puberty, might also be suggested.
Another interesting finding of our study is the high prevalence of migraine among our patients (100% after age 15); previous studies reported prevalence around 10–21%. Prevalence of migraine among first-degree relatives (23%) is also slightly higher than the 9.7% found in our region’s general population per the FRAMIG-3 study (14). This finding supports the epidemiological link between BPV and migraine, and suggests common physiopathological mechanisms. The implication of genetic factors in the physiopathology of migraine with and without aura has already been demonstrated (15,16). Interestingly, mutations of CACNA1A have been reported in two patients with BPV associated with BPT or hemiplegic migraine (17,18). The CACNA1A gene codes for the alpha subunit of voltage-dependent calcium channel type P/Q and is implicated in familial hemiplegic migraine (FHM) type 1 and episodic ataxia type 2 (19). Until now, CACNA1A mutations have not been reported in children with isolated BPV, but literature data are scarce. In adult patients suffering from recurrent vertigo, large population screenings have been carried out but sequencing of different genes coding for ion channels did not reveal any deleterious abnormalities (20–22).
Two children from our cohort presented with cardiac supraventricular arrhythmia during the neonatal period. We cannot conclude whether this association is coincidental. Nevertheless, such cardiologic manifestations share several features with BPV: abruptness of onset, lack of anomaly in clinical and para-clinical investigations and complete recovery usually observed during childhood. Interestingly, mutations in genes coding for voltage-dependent ion channel have recently been described in forms of familial atrial fibrillation, the physiopathology of which is close to those of the cardiac abnormalities seen in our children (23). Whether these clinical manifestations (vertigo and cardiac manifestation) are related to a common ionic channelopathy is unclear.
Despite the small size of our cohort, our study provides new findings on BPV. The concept of benignity usually associated with this disorder is put into question by the findings of the long-term follow-up of our patients, with persistence of attacks in half of the patients older than 11 years. The high prevalence of migraine among our patients and their relatives provides further evidence for a close link with migraine, although the shared physiopathological mechanisms remain to be identified.
Footnotes
Conflict of interest statement
The authors declare that they have no conflict of interest.